

Examining the Role of Vitamin D in Caries Susceptibility in Children’s Deciduous Teeth: A Systematic Review
Abstract
:1. Introduction
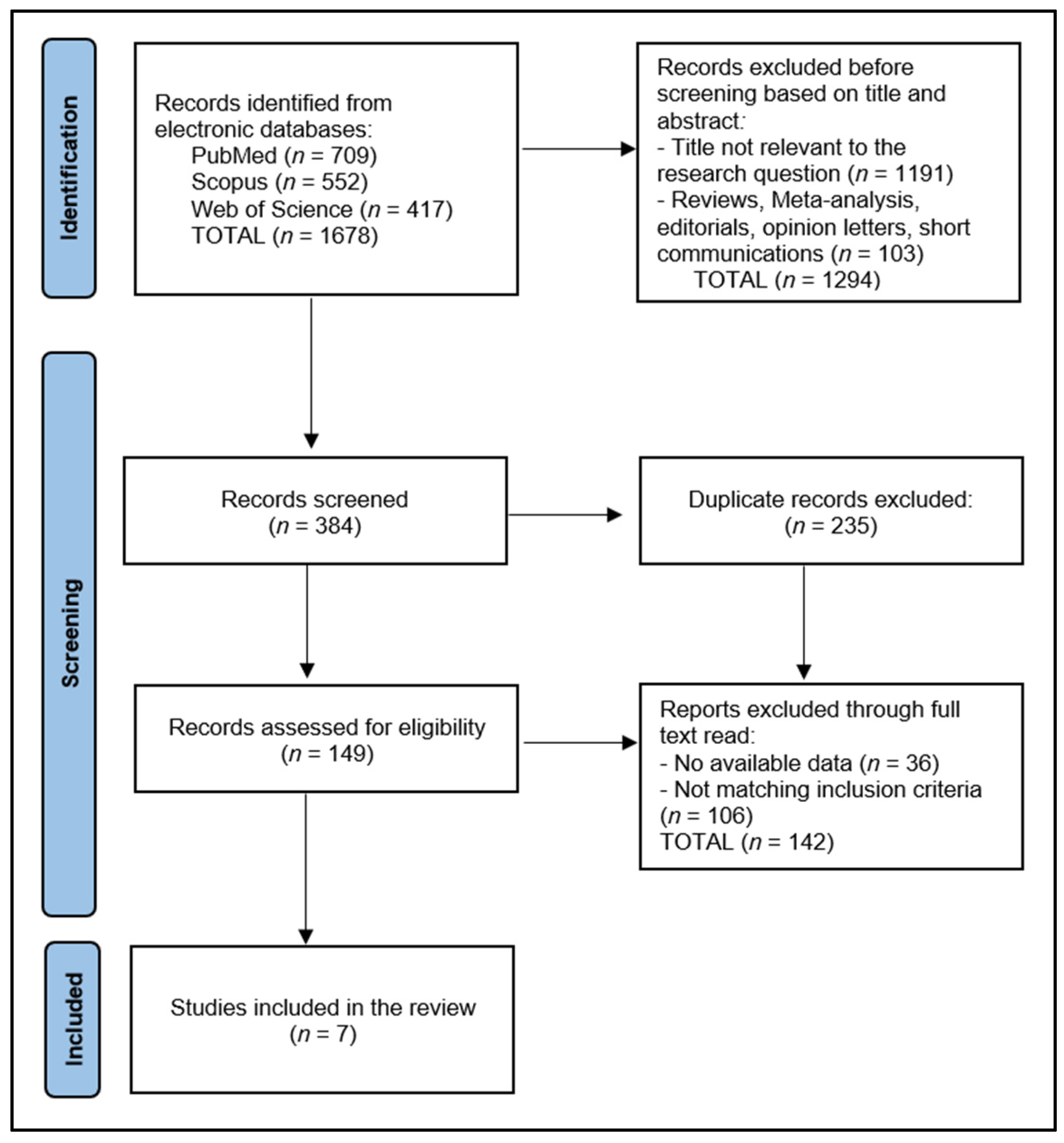
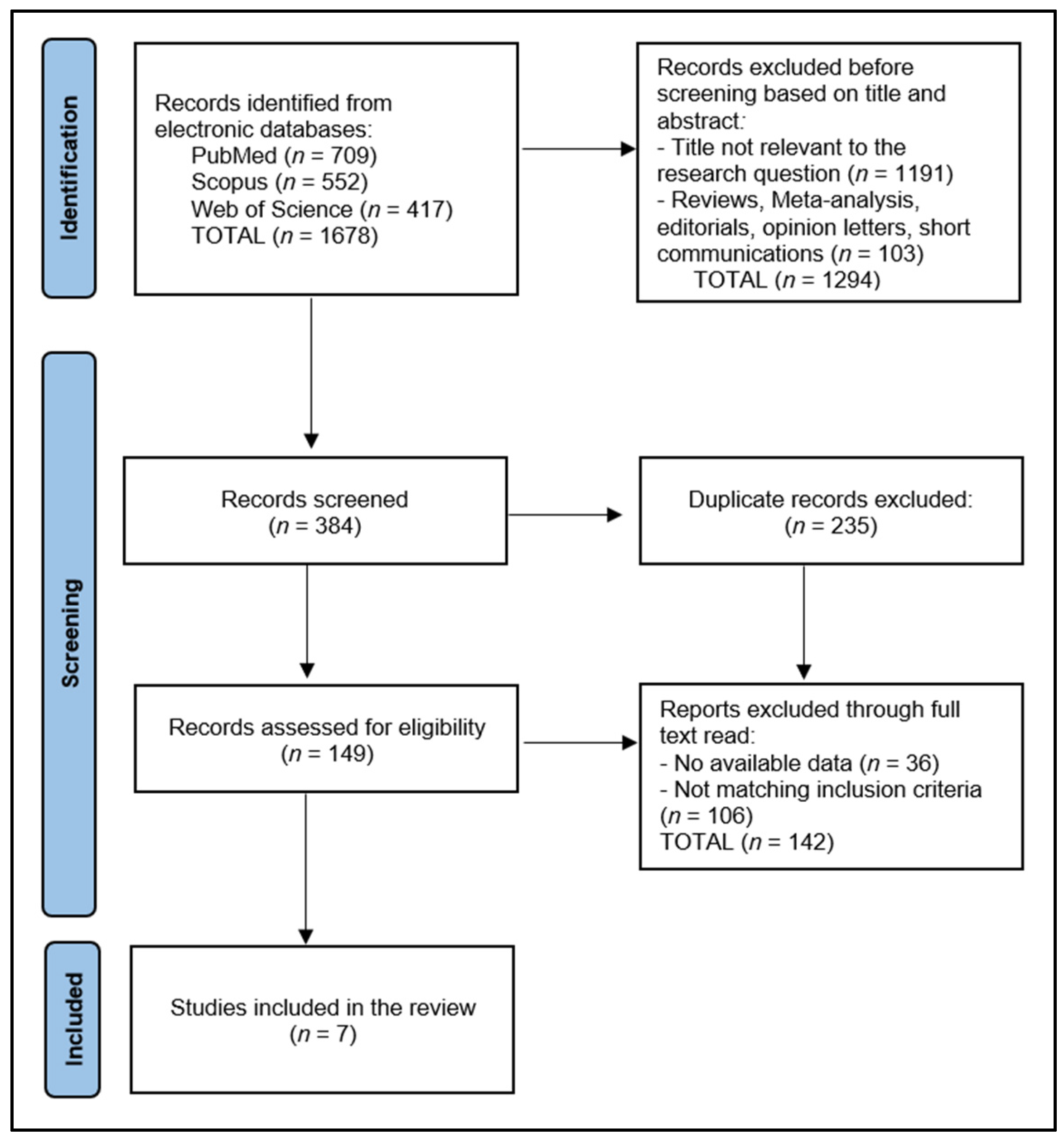
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Data Collection Process
2.4. Risk of Bias
3. Results
3.1. Study Characteristics
3.2. Children’s Characteristics
3.3. Children’s Habits
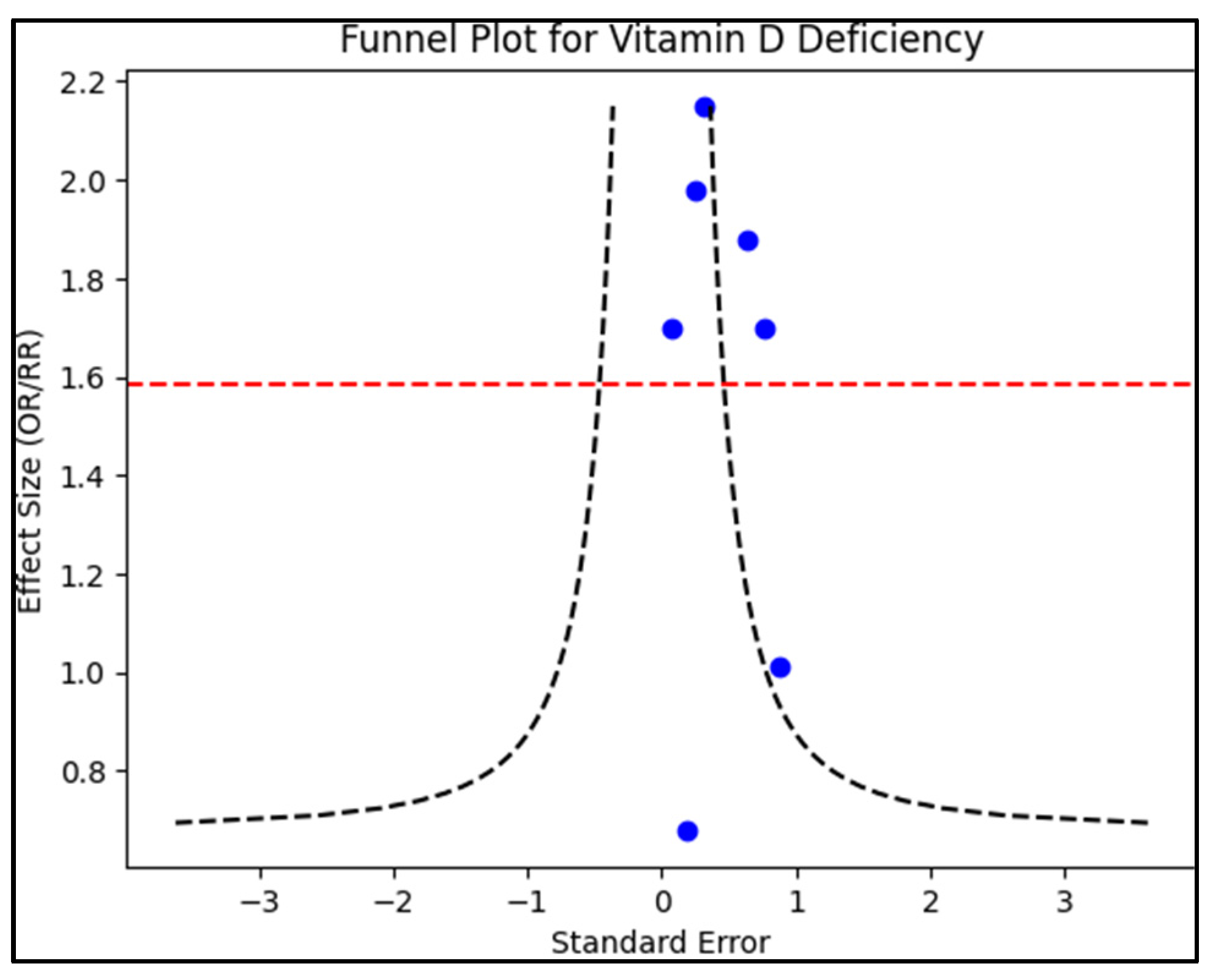
3.4. Risk Factors for Caries in Primary Teeth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colak, H.; Dülgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef] [PubMed]
- Prasai Dixit, L.; Shakya, A.; Shrestha, M.; Shrestha, A. Dental caries prevalence, oral health knowledge and practice among indigenous Chepang school children of Nepal. BMC Oral Health 2013, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Shi, W. Salivary biomarkers for caries risk assessment. J. Calif. Dent. Assoc. 2013, 41, 107–109; 112–118. [Google Scholar] [CrossRef]
- Nyvad, B.; Takahashi, N. Integrated hypothesis of dental caries and periodontal diseases. J. Oral Microbiol. 2020, 12, 1710953. [Google Scholar] [CrossRef]
- Chen, X.; Daliri, E.B.; Kim, N.; Kim, J.R.; Yoo, D.; Oh, D.H. Microbial Etiology and Prevention of Dental Caries: Exploiting Natural Products to Inhibit Cariogenic Biofilms. Pathogens 2020, 9, 569. [Google Scholar] [CrossRef]
- Banga, K.S.; Rastogi, S.; Mistry, S. Profile of Dental Caries in Teenagers in Mumbai City Visiting Nair Hospital Dental College. Contemp. Clin. Dent. 2018, 9, 223–230. [Google Scholar] [CrossRef]
- Zou, J.; Du, Q.; Ge, L.; Wang, J.; Wang, X.; Li, Y.; Song, G.; Zhao, W.; Chen, X.; Jiang, B.; et al. Expert consensus on early childhood caries management. Int. J. Oral Sci. 2022, 14, 35. [Google Scholar] [CrossRef]
- Laird, E.; Ward, M.; McSorley, E.; Strain, J.J.; Wallace, J. Vitamin D and bone health: Potential mechanisms. Nutrients 2010, 2, 693–724. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D and bone. Curr. Osteoporos. Rep. 2012, 10, 151–159. [Google Scholar] [CrossRef]
- Pike, J.W.; Christakos, S. Biology and Mechanisms of Action of the Vitamin D Hormone. Endocrinol. Metab. Clin. N. Am. 2017, 46, 815–843. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Incalzi, R.A.; Zamboni, V.; Pahor, M. Vitamin D hormone: A multitude of actions potentially influencing the physical function decline in older persons. Geriatr. Gerontol. Int. 2011, 11, 133–142. [Google Scholar] [CrossRef]
- Costantini, E.; Sinjari, B.; Piscopo, F.; Porreca, A.; Reale, M.; Caputi, S.; Murmura, G. Evaluation of Salivary Cytokines and Vitamin D Levels in Periodontopathic Patients. Int. J. Mol. Sci. 2020, 21, 2669. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proença, L.; Delgado, A.S.; Mendes, J.J. Vitamin D Deficiency and Oral Health: A Comprehensive Review. Nutrients 2020, 12, 1471. [Google Scholar] [CrossRef] [PubMed]
- Diachkova, E.; Trifonova, D.; Morozova, E.; Runova, G.; Ashurko, I.; Ibadulaeva, M.; Fadeev, V.; Tarasenko, S. Vitamin D and Its Role in Oral Diseases Development. Scoping Rev. Dent. J. 2021, 9, 129. [Google Scholar] [CrossRef]
- Al-Jubori, S.H.; Al-Murad, M.A.; Al-Mashhadane, F.A. Effect of Oral Vitamin D3 on Dental Caries: An In-Vivo and In-Vitro Study. Cureus 2022, 14, e25360. [Google Scholar] [CrossRef]
- Kalia, G.; Tandon, S.; Bhupali, N.R.; Rathore, A.; Mathur, R.; Rathore, K. Speech evaluation in children with missing anterior teeth and after prosthetic rehabilitation with fixed functional space maintainer. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 391–395. [Google Scholar] [CrossRef]
- Bommangoudar, J.S.; Chandrashekhar, S.; Shetty, S.; Sidral, S. Pedodontist’s Role in Managing Speech Impairments Due to Structural Imperfections and Oral Habits: A Literature Review. Int. J. Clin. Pediatr. Dent. 2020, 13, 85–90. [Google Scholar] [CrossRef]
- Singh, S.; Talmale, P. Impact of dental caries and nutritional status on oral health related quality of life in young Indian adolescents. J. Oral Biol. Craniofac. Res. 2023, 13, 506–510. [Google Scholar] [CrossRef]
- Madhusudhan, K.S.; Khargekar, N. Nutritional Status and its Relationship with Dental Caries among 3-6-year-old Anganwadi Children. Int. J. Clin. Pediatr. Dent. 2020, 13, 6–10. [Google Scholar] [CrossRef]
- Beckett, D.M.; Broadbent, J.M.; Loch, C.; Mahoney, E.K.; Drummond, B.K.; Wheeler, B.J. Dental Consequences of Vitamin D Deficiency during Pregnancy and Early Infancy-An Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 1932. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Calleja, C.; Aza-Morera, J.; Iglesias-Cabo, T.; Tardón, A. Vitamin D, pregnancy and caries in children in the INMA-Asturias birth cohort. BMC Pediatr. 2021, 21, 380. [Google Scholar] [CrossRef] [PubMed]
- Dhamo, B.; Miliku, K.; Voortman, T.; Tiemeier, H.; Jaddoe, V.W.; Wolvius, E.B.; Ongkosuwito, E.M. The Associations of Maternal and Neonatal Vitamin D with Dental Development in Childhood. Curr. Dev. Nutr. 2019, 3, nzy100. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Kostiuk, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef]
- Chawłowska, E.; Karasiewicz, M.; Lipiak, A.; Cofta, M.; Fechner, B.; Lewicka-Rabska, A.; Pruciak, A.; Gerreth, K. Exploring the Relationships between Children’s Oral Health and Parents’ Oral Health Knowledge, Literacy, Behaviours and Adherence to Recommendations: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 11288. [Google Scholar] [CrossRef]
- Azizi, Z. The prevalence of dental caries in primary dentition in 4- to 5-year-old preschool children in northern palestine. Int. J. Dent. 2014, 2014, 839419. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. Ed. 2021, 372, n71. [Google Scholar] [CrossRef]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Song, J.W.; Chung, K.C. Observational studies: Cohort and case-control studies. Plast. Reconstr. Surg. 2010, 126, 2234–2242. [Google Scholar] [CrossRef]
- Schroth, R.J.; Rabbani, R.; Loewen, G.; Moffatt, M.E. Vitamin D and Dental Caries in Children. J. Dent. Res. 2016, 95, 173–179. [Google Scholar] [CrossRef]
- Wagner, Y.; Heinrich-Weltzien, R. Evaluation of an interdisciplinary preventive programme for early childhood caries: Findings of a regional German birth cohort study. Clin. Oral Investig. 2016, 20, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Seminario, A.L.; Jumani, K.; Velan, E.; Scott, J.M.; Latimer, J.; Schroth, R.J. Suboptimal Serum Vitamin D Associated with Early Childhood Caries in Special Health Care Needs Children. J. Dent. Child. 2018, 85, 93–101. [Google Scholar]
- Schroth, R.J.; Levi, J.A.; Sellers, E.A.; Friel, J.; Kliewer, E.; Moffatt, M.E. Vitamin D status of children with severe early childhood caries: A case-control study. BMC Pediatr. 2013, 13, 174. [Google Scholar] [CrossRef] [PubMed]
- Navarro, C.L.A.; Grgic, O.; Trajanoska, K.; van der Tas, J.T.; Rivadeneira, F.; Wolvius, E.B.; Voortman, T.; Kragt, L. Associations Between Prenatal, Perinatal, and Early Childhood Vitamin D Status and Risk of Dental Caries at 6 Years. J. Nutr. 2021, 151, 1993–2000. [Google Scholar] [CrossRef]
- Schroth, R.J.; Jeal, N.S.; Kliewer, E.; Sellers, E.A. The relationship between vitamin D and severe early childhood caries: A pilot study. International journal for vitamin and nutrition research. Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung. J. Int. Vitaminol. Nutr. 2012, 82, 53–62. [Google Scholar] [CrossRef]
- El Shiekh, M.A.; Hanafy, R.M.H. Relationship between vitamin D status and caries experience in a group of Egyptian children: A cross-sectional study. BMC Oral Health 2023, 23, 374. [Google Scholar] [CrossRef]
- Bertoldo, F.; Cianferotti, L.; Di Monaco, M.; Falchetti, A.; Fassio, A.; Gatti, D.; Gennari, L.; Giannini, S.; Girasole, G.; Gonnelli, S.; et al. Definition, Assessment, and Management of Vitamin D Inadequacy: Suggestions, Recommendations, and Warnings from the Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS). Nutrients 2022, 14, 4148. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0, an update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Grant, W.B. The role of geographical ecological studies in identifying diseases linked to UVB exposure and/or vitamin D. Derm.-Endocrinol. 2016, 8, e1137400. [Google Scholar] [CrossRef]
- Uwitonze, A.M.; Murererehe, J.; Ineza, M.C.; Harelimana, E.I.; Nsabimana, U.; Uwambaye, P.; Gatarayiha, A.; Haq, A.; Razzaque, M.S. Effects of vitamin D status on oral health. J. Steroid Biochem. Mol. Biol. 2018, 175, 190–194. [Google Scholar] [CrossRef]
- Li, Z.; Wei, X.; Shao, Z.; Liu, H.; Bai, S. Correlation between vitamin D levels in serum and the risk of dental caries in children: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 768. [Google Scholar] [CrossRef] [PubMed]
- Spodzieja, K.; Olczak-Kowalczyk, D. Premature Loss of Deciduous Teeth as a Symptom of Systemic Disease: A Narrative Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 3386. [Google Scholar] [CrossRef] [PubMed]
- Kapil, D.; Saraf, B.G.; Sheoran, N.; Srivastava, P.; Singh, S.; Singh, R. To Assess the Prevalence of Dental Caries and Its Association with Body Mass Index, Socioeconomic Status, Dietary Habits, and Oral Hygiene among 6-12-year-old Children in Faridabad. Int. J. Clin. Pediatr. Dent. 2023, 16, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Reddy, E.R.; Rani, S.T.; Manjula, M.; Kumar, L.V.; Mohan, T.A.; Radhika, E. Assessment of caries status among schoolchildren according to decayed-missing-filled teeth/decayed-extract-filled teeth index, International Caries Detection and Assessment System, and Caries Assessment Spectrum and Treatment criteria. Indian J. Dent. Res. 2017, 28, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Moradi, G.; Mohamadi Bolbanabad, A.; Moinafshar, A.; Adabi, H.; Sharafi, M.; Zareie, B. Evaluation of Oral Health Status Based on the Decayed, Missing and Filled Teeth (DMFT) Index. Iran. J. Public Health 2019, 48, 2050–2057. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Li, Q.; Deng, C.; Yao, G.; Bai, X.; Tan, X.; Zhang, X. Prevalence and Clinical Correlation of Decayed, Missing, and Filled Teeth in Elderly Inpatients with Schizophrenia. Front. Psychiatry 2021, 12, 728971. [Google Scholar] [CrossRef]
- Macey, R.; Walsh, T.; Riley, P.; Glenny, A.M.; Worthington, H.V.; Clarkson, J.E.; Ricketts, D. Tests to detect and inform the diagnosis of caries. Cochrane Database Syst. Rev. 2018, 2018, CD013215. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study & Author | Country | Study Year | Study Design | Study Quality | |
|---|---|---|---|---|---|
| 1 | Schroth et al. [30] | Canada | 2016 | Cross-sectional | Excellent |
| 2 | Wagner et al. [31] | Germany | 2016 | Cohort | Excellent |
| 3 | Seminario et al. [32] | USA | 2018 | Cross-sectional | Good |
| 4 | Schroth et al. [33] | Canada | 2013 | Case-control | Good |
| 5 | Navarro et al. [34] | Netherlands | 2021 | Cohort | Excellent |
| 6 | Schroth et al. [35] | Canada | 2012 | Cohort | Good |
| 7 | El Shiekh et al. [36] | Egypt | 2023 | Cross-sectional | Fair |
| Study Number | Number of Participants | Study Groups (Vitamin D Levels) | Age | Region (Latitude Range) | Sun Exposure (UV Index) | |
|---|---|---|---|---|---|---|
| 1 | Schroth et al. 2016 [30] | 1017 | Insufficient (127) vs. Normal (890) | 6–11 years | Manitoba—Canada (49° N–60° N) | Winter: UV 0–1 (Low), Summer: UV 4–7 (Moderate to High) |
| 2 | Wagner et al. 2016 [31] | 755 | Insufficient (60) vs. Normal (695) | 3–4 years | Thuringia—Germany (50° N–52° N) | Winter: UV 0–1 (Low), Summer: UV 5–7 (Moderate to High) |
| 3 | Seminario et al. 2018 [32] | 276 | Insufficient (138) vs. Normal (138) | 1–6 years | Washington—USA (45° N–49° N) | Winter: UV 0–2 (Low), Summer: UV 5–8 (Moderate to Very High) |
| 4 | Schroth et al. 2013 [33] | 261 | Insufficient (43) vs. Normal (218) | 3–5 years | Manitoba—Canada (49° N–60° N) | Winter: UV 0–1 (Low), Summer: UV 4–7 (Moderate to High) |
| 5 | Navarro et al. 2021 [34] | 5257 | Insufficient (2620) vs. Normal (2637) | 6 years | South Holland—Netherlands (51° N–52° N) | Winter: UV 0–1 (Low), Summer: UV 5–7 (Moderate to High) |
| 6 | Schroth et al. 2012 [35] | 38 | Insufficient (32) vs. Normal (6) | 1–6 years | All regions—Canada (41° N–83° N) | Varies widely |
| 7 | El Shiekh et al. 2023 [36] | 51 | Insufficient (34) vs. Normal (17) | 3–5 years | Cairo—Egypt (30° N) | Winter: UV 3–5 (Moderate), Summer: UV 9–11+ (Very High to Extreme) |
| Study Number | Brushing | Hygiene | Food | Supplements | |
|---|---|---|---|---|---|
| 1 | Schroth et al. [30] | 2 times/day—70.9% | Visits the dentist at least once a year—94.0% | Drink milk 1/day—64.0%; Sugary drinks 1/day—64.0% | Vitamin D—100% Fluoride—37.3% |
| 2 | Wagner et al. [31] | Daily brushing—94.2% | Visits the dentist at least once a year—64.1% | Sugary drinks/food > 3 times daily—2.3% | Vitamin D—92.1% |
| 3 | Seminario et al. [32] | NR | NR | NR | Vitamin D—100% |
| 4 | Schroth et al. [33] | 1–2 times/day | Visits the dentist at least once a year | Breast-fed—78.2% | Multivitamins—54.8% |
| 5 | Navarro et al. [34] | ≥2 times/day—51.2% | NR | NR | NR |
| 6 | Schroth et al. [35] | Daily brushing—45.5% | Visits the dentist at least once a year—46.7% | Drink milk 1/day—50.0% | Multivitamins—44.4% |
| 7 | El Shiekh et al. [36] | Daily brushing—60.9% | Visits the dentist at least once a year—78.5% | Snacking—53.5% | Fluoride—63.3% |
| Risk Factors (OR/RR) | Vitamin D Deficiency | Daily Brushing | Yearly Dental Visits | Snacking/Sugary Foods | Vitamin Supplements | Adjusted Factors in Analysis | |
|---|---|---|---|---|---|---|---|
| 1 | Schroth et al. [30] | 0.68 (0.40–1.14) | 0.51 * (0.33–0.79) | 1.90 (0.82–4.41) | 1.09 (0.78–1.54) | Fluoride 1.01 (0.58–1.75) | Daily brushing, Yearly dental visits, Snacking |
| 2 | Wagner et al. [31] | 1.88 (0.99–3.51) | 0.71 (0.38–1.32) | 4.51 (3.82–5.34) | 0.30 (0.10–0.92) | NR | Daily brushing, Yearly dental visits |
| 3 | Seminario et al. [32] | 2.15 * (1.61–2.86) | NR | NR | NR | NR | None (Unadjusted) |
| 4 | Schroth et al. [33] | 1.98 * (1.55–2.53) | 0.97 (0.94–1.01) | NR | NR | Vitamin D drops 1.51 (0.81–2.82) | Daily brushing |
| 5 | Navarro et al. [34] | 1.70 * (1.57–1.85) | NR | NR | NR | 0.96 (0.95–0.97) | None (Unadjusted) |
| 6 | Schroth et al. [35] | 1.70 (0.75–3.83) | 0.21 (NR) | NR | NR | 0.65 (NR) | Daily brushing |
| 7 | El Shiekh et al. [36] | 1.01 (−0.74–2.76) | −2.21 * (−4.14–−0.28) | −1.43 (−3.09–−0.23) | −1.18 (2.42–0.89) | Fluoride drops/tablets 2.19 (−1.25–5.63) | Daily brushing, Yearly dental visits, Snacking |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bumbu, B.A.; Luca, M.M.; Buzatu, R. Examining the Role of Vitamin D in Caries Susceptibility in Children’s Deciduous Teeth: A Systematic Review. Nutrients 2023, 15, 4826. https://doi.org/10.3390/nu15224826
Bumbu BA, Luca MM, Buzatu R. Examining the Role of Vitamin D in Caries Susceptibility in Children’s Deciduous Teeth: A Systematic Review. Nutrients. 2023; 15(22):4826. https://doi.org/10.3390/nu15224826
Chicago/Turabian StyleBumbu, Bogdan Andrei, Magda Mihaela Luca, and Roxana Buzatu. 2023. "Examining the Role of Vitamin D in Caries Susceptibility in Children’s Deciduous Teeth: A Systematic Review" Nutrients 15, no. 22: 4826. https://doi.org/10.3390/nu15224826
APA StyleBumbu, B. A., Luca, M. M., & Buzatu, R. (2023). Examining the Role of Vitamin D in Caries Susceptibility in Children’s Deciduous Teeth: A Systematic Review. Nutrients, 15(22), 4826. https://doi.org/10.3390/nu15224826