


Long-Term Consumption of Green Tea Can Reduce the Degree of Depression in Postmenopausal Women by Increasing Estradiol
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Recruiting
2.2. Variables
2.2.1. Basic Socio-Demographic Information
2.2.2. Sleep Patterns and Depression Levels
2.2.3. Hormone Levels and Inflammatory Markers
2.3. Statistical Analyses
3. Results
3.1. The Characteristics and Differences of Two Groups on Different Variables
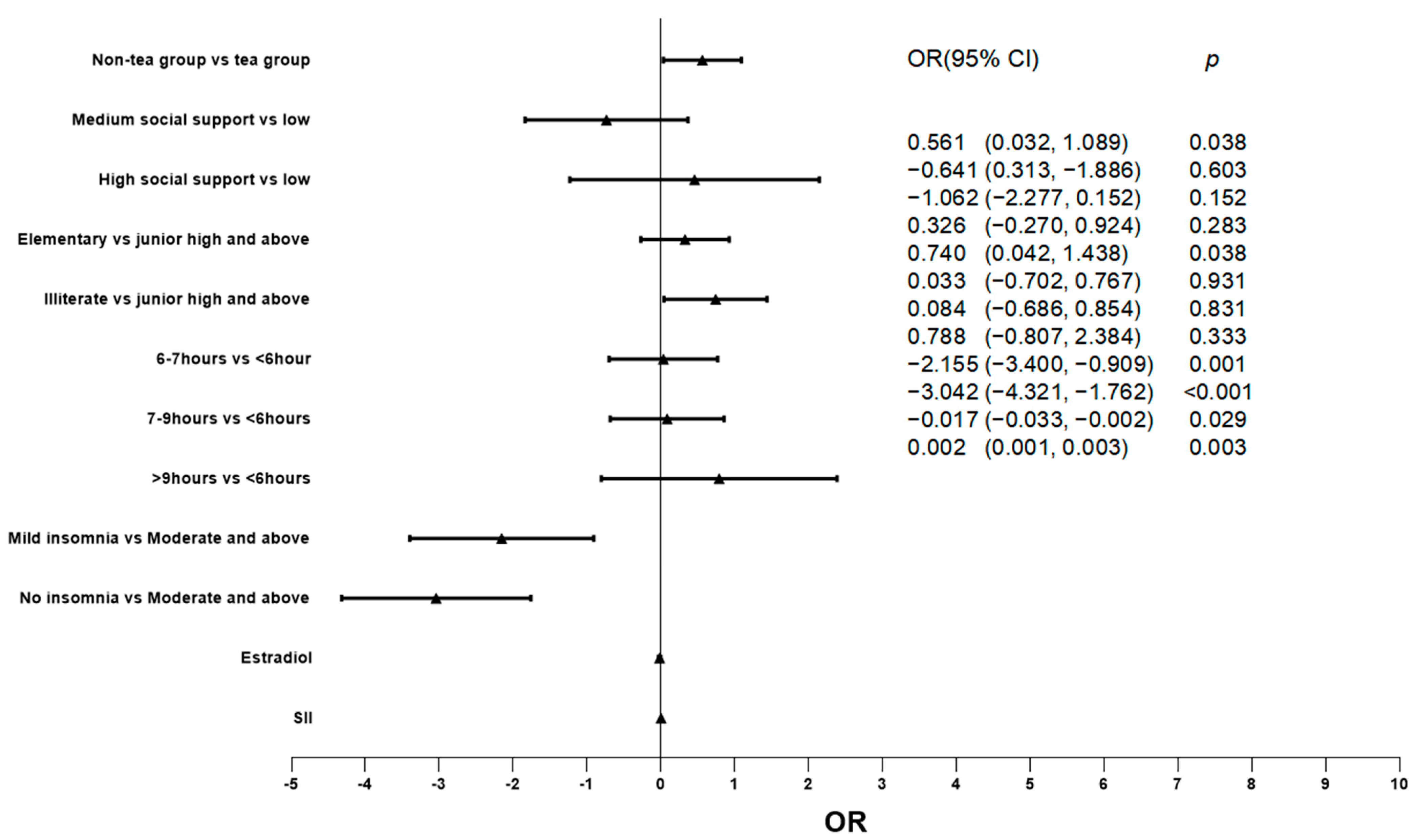
3.2. Relationship between Two Groups and Degree of Depression
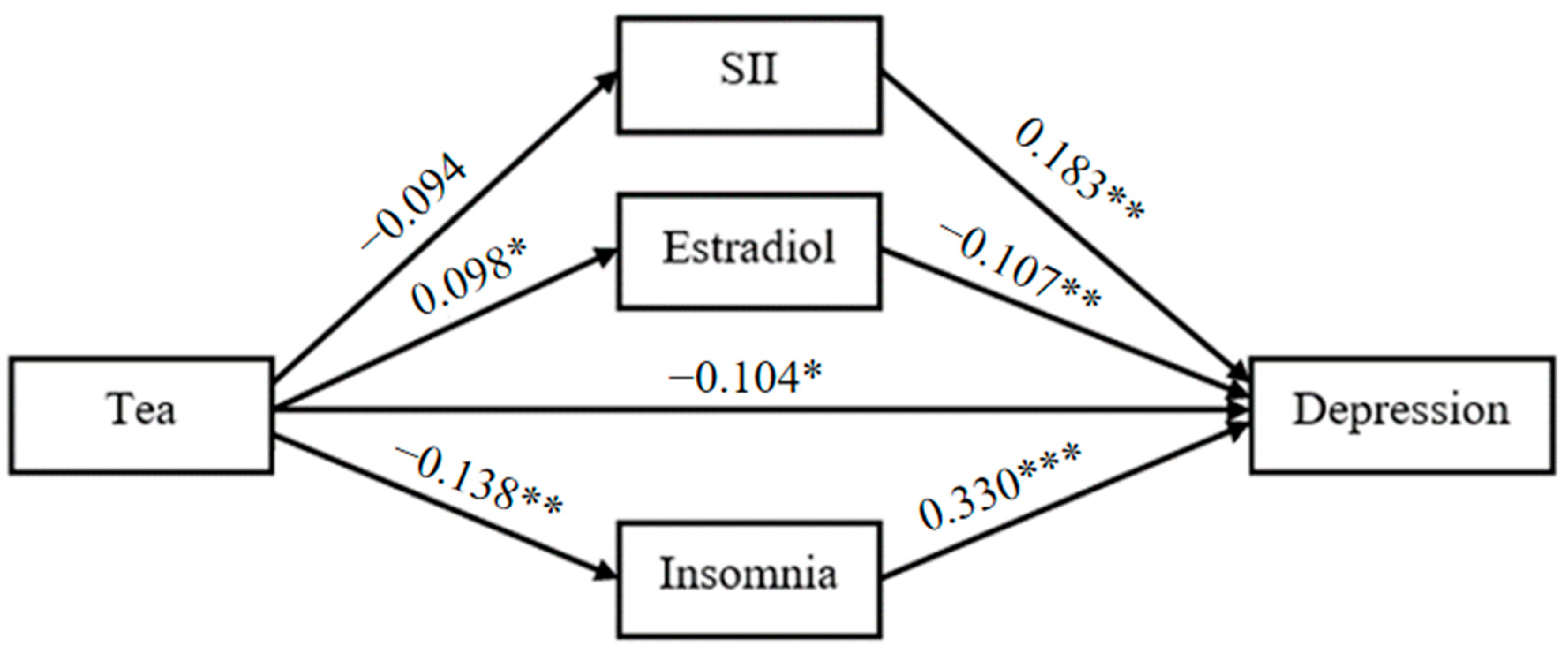
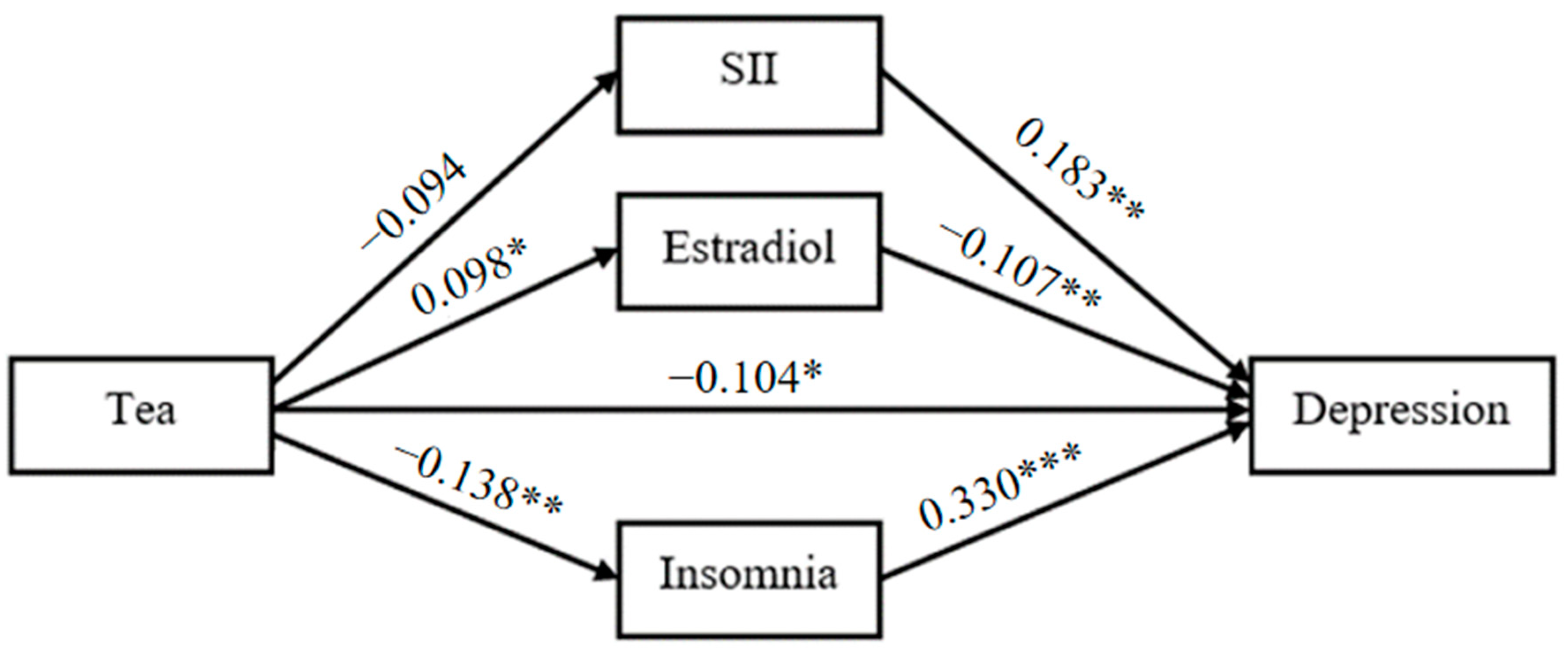
3.3. Path Analysis Model
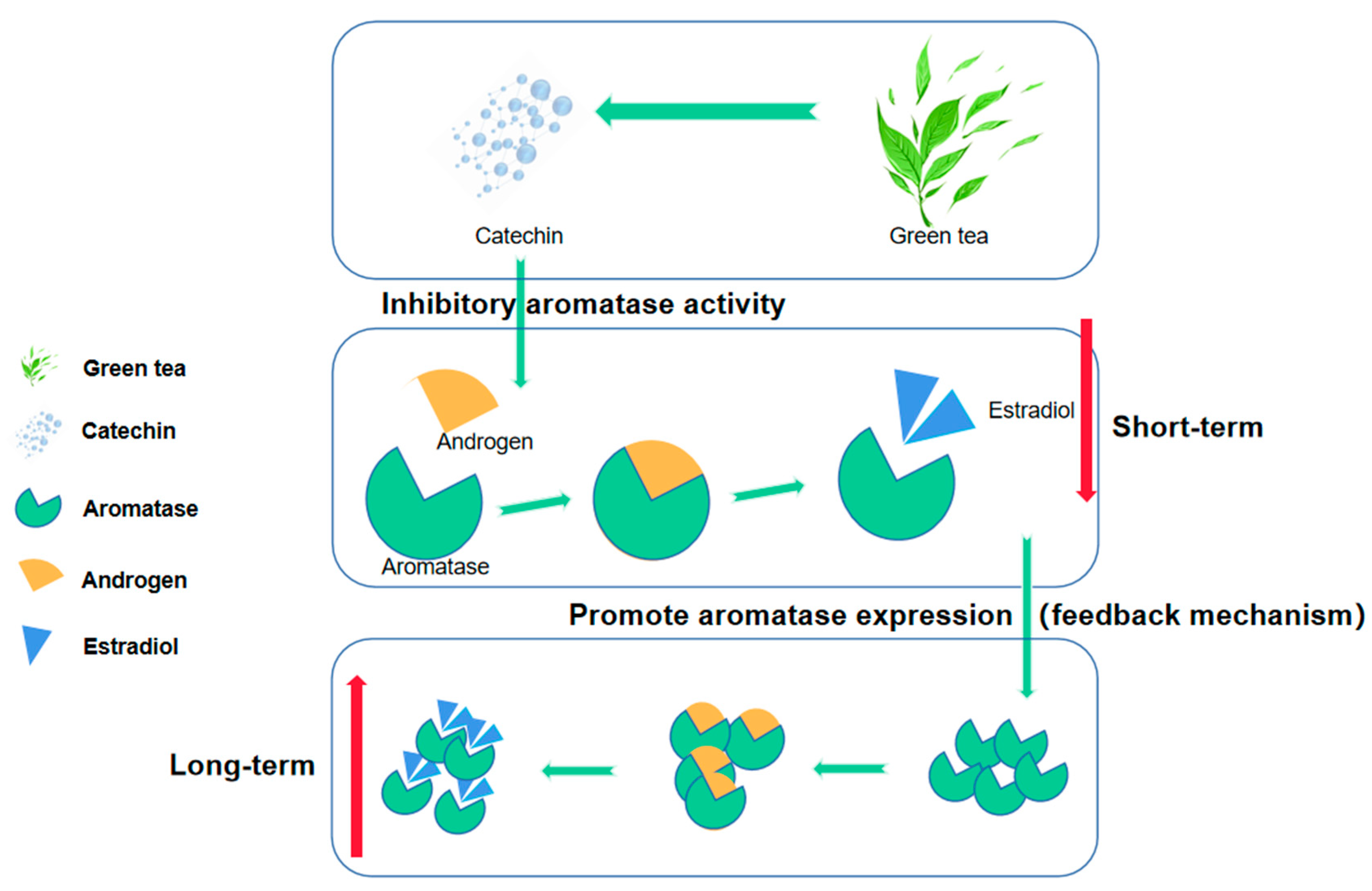
4. Discussion
5. Advantage and Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Herrman, H.; Patel, V.; Kieling, C.; Berk, M.; Buchweitz, C.; Cuijpers, P.; Furukawa, T.A.; Kessler, R.C.; Kohrt, B.A.; Maj, M.; et al. Time for united action on depression: A Lancet–World Psychiatric Association Commission. Lancet 2022, 399, 957–1022. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.E.; Jo, M.-W.; Shin, Y.-W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef] [PubMed]
- Aziz, R.; Steffens, D.C. What Are the Causes of Late-Life Depression? Psychiatr. Clin. N. Am. 2013, 36, 497–516. [Google Scholar] [CrossRef]
- Uher, R.; McGuffin, P. The moderation by the serotonin transporter gene of environmental adversity in the etiology of depression: 2009 update. Mol. Psychiatry 2009, 15, 18–22. [Google Scholar] [CrossRef]
- Caspi, A.; Sugden, K.; Moffitt, T.E.; Taylor, A.; Craig, I.W.; Harrington, H.; McClay, J.; Mill, J.; Martin, J.; Braithwaite, A.; et al. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 2003, 301, 386–389. [Google Scholar] [CrossRef]
- Kupfer, D.J.; Frank, E.; Phillips, M.L. Major depressive disorder: New clinical, neurobiological, and treatment perspectives. Lancet 2012, 379, 1045–1055. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Luo, M.; Li, J.; Peng, Y.; Wang, Y.; Liu, B.; Liu, G.; Wang, Y.; Lin, S.; Chen, R. Symptoms of anxiety and depression among Chinese women transitioning through menopause: Findings from a prospective community-based cohort study. Fertil. Steril. 2019, 112, 1160–1171. [Google Scholar] [CrossRef]
- Tangen, T.; Mykletun, A. Depression and anxiety through the climacteric period: An epidemiological study (HUNT-II). J. Psychosom. Obstet. Gynecol. 2008, 29, 125–131. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Prasanth, M.I.; Sivamaruthi, B.S.; Chaiyasut, C.; Tencomnao, T. A Review of the Role of Green Tea (Camellia sinensis) in Antiphotoaging, Stress Resistance, Neuroprotection, and Autophagy. Nutrients 2019, 11, 474. [Google Scholar] [CrossRef]
- Yang, X.; Dai, H.; Deng, R.; Zhang, Z.; Quan, Y.; Giri, M.; Shen, J. Association between tea consumption and prevention of coronary artery disease: A systematic review and dose-response meta-analysis. Front. Nutr. 2022, 9, 1021405. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Zhang, Z.; Zheng, T.-Z.; Bassig, B.A.; Mao, C.; Liu, X.; Zhu, Y.; Shi, K.; Ge, J.; Yang, Y.-J.; et al. Green tea consumption and risk of cardiovascular and ischemic related diseases: A meta-analysis. Int. J. Cardiol. 2016, 202, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Mendilaharsu, M.; De Stefani, E.; Deneo-Pellegrini, H.; Carzoglio, J.C.; Ronco, A. Consumption of tea and coffee and the risk of lung cancer in cigarette-smoking men: A case-control study in Uruguay. Lung Cancer 1998, 19, 101–107. [Google Scholar] [CrossRef]
- Hakim, I.A.; Harris, R.B.; Weisgerber, U.M. Tea intake and squamous cell carcinoma of the skin: Influence of type of tea beverages. Cancer Epidemiol. Biomark. Prev. 2000, 9, 727–731. [Google Scholar]
- Nakachi, K.; Suemasu, K.; Suga, K.; Takeo, T.; Imai, K.; Higashi, Y. Influence of drinking green tea on breast cancer malignancy among Japanese patients. Jpn. J. Cancer Res. 1998, 89, 254–261. [Google Scholar] [CrossRef]
- Gao, Y.T.; McLaughlin, J.K.; Blot, W.J.; Ji, B.T.; Dai, Q.; Fraumeni, J.F., Jr. Reduced risk of esophageal cancer associated with green tea consumption. J. Natl. Cancer Inst. 1994, 86, 855–858. [Google Scholar] [CrossRef]
- Wang, Z.Y.; Khan, W.A.; Bickers, D.R.; Mukhtar, H. Protection against polycyclic aromatic hydrocarbon-induced skin tumor initiation in mice by green tea polyphenols. Carcinogenesis 1989, 10, 411–415. [Google Scholar] [CrossRef]
- Dong, X.; Yang, C.; Cao, S.; Gan, Y.; Sun, H.; Gong, Y.; Yang, H.; Yin, X.; Lu, Z. Tea consumption and the risk of depression: A meta-analysis of observational studies. Aust. N. Z. J. Psychiatry 2015, 49, 334–345. [Google Scholar] [CrossRef]
- Ruusunen, A.; Lehto, S.M.; Tolmunen, T.; Mursu, J.; Kaplan, G.A.; Voutilainen, S. Coffee, tea and caffeine intake and the risk of severe depression in middle-aged Finnish men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Public Health Nutr. 2010, 13, 1215–1220. [Google Scholar] [CrossRef]
- Li, F.-D.; He, F.; Ye, X.-J.; Shen, W.; Wu, Y.-P.; Zhai, Y.-J.; Wang, X.-Y.; Lin, J.-F. Tea consumption is inversely associated with depressive symptoms in the elderly: A cross-sectional study in eastern China. J. Affect. Disord. 2016, 199, 157–162. [Google Scholar] [CrossRef]
- Stefanescu, C.; Ciobica, A. The relevance of oxidative stress status in first episode and recurrent depression. J. Affect. Disord. 2012, 143, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Crespy, V.; Williamson, G. A review of the health effects of green tea catechins in in vivo animal models. J. Nutr. 2004, 134 (Suppl. S12), 3431S–3440S. [Google Scholar] [CrossRef] [PubMed]
- Cavet, M.E.; Harrington, K.L.; Vollmer, T.R.; Ward, K.W.; Zhang, J.-Z. Anti-inflammatory and anti-oxidative effects of the green tea polyphenol epigallocatechin gallate in human corneal epithelial cells. Mol. Vis. 2011, 17, 533–542. [Google Scholar] [PubMed]
- Wu, Z.; Huang, S.; Li, T.; Li, N.; Han, D.; Zhang, B.; Xu, Z.Z.; Zhang, S.; Pang, J.; Wang, S.; et al. Gut microbiota from green tea polyphenol-dosed mice improves intestinal epithelial homeostasis and ameliorates experimental colitis. Microbiome 2021, 9, 184. [Google Scholar] [CrossRef]
- Sun, Q.; Cheng, L.; Zhang, X.; Wu, Z.; Weng, P. The interaction between tea polyphenols and host intestinal microorganisms: An effective way to prevent psychiatric disorders. Food Funct. 2021, 12, 952–962. [Google Scholar] [CrossRef]
- Zhu, W.-L.; Shi, H.-S.; Wei, Y.-M.; Wang, S.-J.; Sun, C.-Y.; Ding, Z.-B.; Lu, L. Green tea polyphenols produce antidepressant-like effects in adult mice. Pharmacol. Res. 2012, 65, 74–80. [Google Scholar] [CrossRef]
- Niu, K.; Hozawa, A.; Kuriyama, S.; Ebihara, S.; Guo, H.; Nakaya, N.; Ohmori-Matsuda, K.; Takahashi, H.; Masamune, Y.; Asada, M.; et al. Green tea consumption is associated with depressive symptoms in the elderly. Am. J. Clin. Nutr. 2009, 90, 1615–1622. [Google Scholar] [CrossRef]
- Kim, J.; Kim, J. Green Tea, Coffee, and Caffeine Consumption Are Inversely Associated with Self-Report Lifetime Depression in the Korean Population. Nutrients 2018, 10, 1201. [Google Scholar] [CrossRef]
- Nanri, A.; Eguchi, M.; Kochi, T.; Kabe, I.; Mizoue, T. Green Tea Consumption and Depressive Symptoms among Japanese Workers: The Furukawa Nutrition and Health Study. Nutrients 2021, 14, 167. [Google Scholar] [CrossRef]
- Kimura, Y.; Suga, H.; Kobayashi, S.; Sasaki, S.; The Three-Generation Study of Women on Diets and Health Study Group. Intake of Coffee Associated with Decreased Depressive Symptoms among Elderly Japanese Women: A Multi-Center Cross-Sectional Study. J. Epidemiol. 2020, 30, 338–344. [Google Scholar] [CrossRef]
- Sites, C.K.; Toth, M.J.; Cushman, M.; L’hommedieu, G.D.; Tchernof, A.; Tracy, R.P.; Poehlman, E.T. Menopause-related differences in inflammation markers and their relationship to body fat distribution and insulin-stimulated glucose disposal. Fertil. Steril. 2002, 77, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Malutan, A.M.; Dan, M.; Nicolae, C.; Carmen, M. Proinflammatory and anti-inflammatory cytokine changes related to menopause. Prz. Menopauzalny 2014, 3, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.-L. Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Pers. Individ. Differ. 2000, 28, 299–307. [Google Scholar] [CrossRef]
- Thorndike, F.P.; Ritterband, L.M.; Saylor, D.K.; Magee, J.C.; Gonder-Frederick, L.A.; Morin, C.M. Validation of the insomnia severity index as a web-based measure. Behav. Sleep Med. 2011, 9, 216–223. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Wheaton, A.G.; Olsen, E.O.; Miller, G.F.; Croft, J.B. Sleep Duration and Injury-Related Risk Behaviors Among High School Students—United States, 2007–2013. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 337–341. [Google Scholar] [CrossRef]
- Thacher, P.V.; Onyper, S.V. Longitudinal Outcomes of Start Time Delay on Sleep, Behavior, and Achievement in High School. Sleep 2016, 39, 271–281. [Google Scholar] [CrossRef]
- Mazza, M.G.; Palladini, M.; De Lorenzo, R.; Magnaghi, C.; Poletti, S.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; Benedetti, F. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: Effect of inflammatory biomarkers at three-month follow-up. Brain Behav. Immun. 2021, 94, 138–147. [Google Scholar] [CrossRef]
- Tian, T.; Lu, J.; Zhao, W.; Wang, Z.; Xu, H.; Ding, Y.; Guo, W.; Qin, P.; Zhu, W.; Song, C.; et al. Associations of systemic inflammation markers with identification of pulmonary nodule and incident lung cancer in Chinese population. Cancer Med. 2022, 11, 2482–2491. [Google Scholar] [CrossRef]
- Zhang, F.; Niu, M.; Wang, L.; Liu, Y.; Shi, L.; Cao, J.; Mi, W.; Ma, Y.; Liu, J. Systemic-Immune-Inflammation Index as a Promising Biomarker for Predicting Perioperative Ischemic Stroke in Older Patients Who Underwent Non-cardiac Surgery. Front. Aging Neurosci. 2022, 14, 865244. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-W.; Huang, S.-M. Tea consumption affects the absorption of levothyroxine. Front. Endocrinol. 2022, 13, 943775. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.K.; De, N. Goitrogenic/antithyroidal potential of green tea extract in relation to catechin in rats. Food Chem. Toxicol. 2010, 48, 2304–2311. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.K.; De, N. Catechin induced modulation in the activities of thyroid hormone synthesizing enzymes leading to hypothyroidism. Mol. Cell. Biochem. 2013, 374, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Arakawa, K.; Stanczyk, F.Z.; Berg, D.V.D.; Koh, W.-P.; Yu, M.C. Tea and circulating estrogen levels in postmenopausal Chinese women in Singapore. Carcinogenesis 2005, 26, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Kabuto, M.; Shimizu, H. Association of coffee, green tea, and caffeine intakes with serum concentrations of estradiol and sex hormone-binding globulin in premenopausal Japanese women. Nutr. Cancer 1998, 30, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Spicer, D.; Stanczyk, F.Z.; Tseng, C.-C.; Yang, C.S.; Pike, M.C. Effect of 2-month controlled green tea intervention on lipoprotein cholesterol, glucose, and hormone levels in healthy postmenopausal women. Cancer Prev. Res. 2012, 5, 393–402. [Google Scholar] [CrossRef]
- Monteiro, R.; Assuncao, M.; Andrade, J.P.; Neves, D.; Calhau, C.; Azevedo, I. Chronic green tea consumption decreases body mass, induces aromatase expression, and changes proliferation and apoptosis in adult male rat adipose tissue. J. Nutr. 2008, 138, 2156–2163. [Google Scholar] [CrossRef]
- Shen, C.-L.; Wang, P.; Guerrieri, J.; Yeh, J.K.; Wang, J.-S. Protective effect of green tea polyphenols on bone loss in middle-aged female rats. Osteoporos. Int. 2008, 19, 979–990. [Google Scholar] [CrossRef]
- Satoh, K.; Sakamoto, Y.; Ogata, A.; Nagai, F.; Mikuriya, H.; Numazawa, M.; Yamada, K.; Aoki, N. Inhibition of aromatase activity by green tea extract catechins and their endocrinological effects of oral administration in rats. Food Chem. Toxicol. 2002, 40, 925–933. [Google Scholar] [CrossRef]
- Figueiroa, M.S.; Vieira, J.S.B.C.; Leite, D.S.; Filho, R.C.O.A.; Ferreira, F.; Gouveia, P.S.; Udrisar, D.P.; Wanderley, M.I.I. Green tea polyphenols inhibit testosterone production in rat Leydig cells. Asian J. Androl. 2009, 11, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.-L.; Pu, H.-F.; Chen, S.-Y.; Wang, S.-W.; Wang, P.S. Effects of catechin, epicatechin and epigallocatechin gallate on testosterone production in rat leydig cells. J. Cell. Biochem. 2010, 110, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Han, B.; Hu, H.; Liu, J.; Liu, Y.; Lee, W.; Lee, S.Y.; Son, Y.-J.; Yun, J.-M.; Yoon, L.; et al. Epigallocatechin-3-O-Gallate Protects Against Hepatic Damage and Testicular Toxicity in Male Mice Exposed to Di-(2-Ethylhexyl) Phthalate. J. Med. Food 2015, 18, 753–761. [Google Scholar] [CrossRef]
- Harada, N.; Hatano, O. Inhibitors of aromatase prevent degradation of the enzyme in cultured human tumour cells. Br. J. Cancer 1998, 77, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Do Rego, J.L.; Seong, J.Y.; Burel, D.; Leprince, J.; Luu-The, V.; Tsutsui, K.; Tonon, M.-C.; Pelletier, G.; Vaudry, H. Neurosteroid biosynthesis: Enzymatic pathways and neuroendocrine regulation by neurotransmitters and neuropeptides. Front. Neuroendocrinol. 2009, 30, 259–301. [Google Scholar] [CrossRef] [PubMed]
- Ano, Y.; Ohya, R.; Kita, M.; Taniguchi, Y.; Kondo, K. Theaflavins Improve Memory Impairment and Depression-Like Behavior by Regulating Microglial Activation. Molecules 2019, 24, 467. [Google Scholar] [CrossRef]
- Wang, J.; Li, P.; Qin, T.; Sun, D.; Zhao, X.; Zhang, B. Protective effect of epigallocatechin-3-gallate against neuroinflammation and anxiety-like behavior in a rat model of myocardial infarction. Brain Behav. 2020, 10, e01633. [Google Scholar] [CrossRef]
- Smith, R.E. The Effects of Dietary Supplements that Overactivate the Nrf2/ARE System. Curr. Med. Chem. 2020, 27, 2077–2094. [Google Scholar] [CrossRef]
- Yang, C.S.; Zhang, J.; Zhang, L.; Huang, J.; Wang, Y. Mechanisms of body weight reduction and metabolic syndrome alleviation by tea. Mol. Nutr. Food Res. 2016, 60, 160–174. [Google Scholar] [CrossRef]
- Zhou, J.-R.; Li, L.; Pan, W. Dietary soy and tea combinations for prevention of breast and prostate cancers by targeting metabolic syndrome elements in mice. Am. J. Clin. Nutr. 2007, 86, 882S–888S. [Google Scholar] [CrossRef]
- Liu, W.; Wan, C.; Huang, Y.; Li, M. Effects of tea consumption on metabolic syndrome: A systematic review and meta-analysis of randomized clinical trials. Phytother. Res. 2020, 34, 2857–2866. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tang, N.; Xia, W.; Seraj, S.S.; Pereira, M.; Velu, P.; Zhou, H.; Yang, H.; Du, G. The effect of green tea supplementation on the anthropometric outcomes in overweight and obese women: A time and dose-response meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kleiser, C.; Wawro, N.; Stelmach-Mardas, M.; Boeing, H.; Gedrich, K.; Himmerich, H.; Linseisen, J. Are sleep duration, midpoint of sleep and sleep quality associated with dietary intake among Bavarian adults? Eur. J. Clin. Nutr. 2017, 71, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.J.; Banks, S.; Coates, A.M.; Kohler, M.J. The Relationship Between Caffeine, Sleep, and Behavior in Children. J. Clin. Sleep Med. 2017, 13, 533–543. [Google Scholar] [CrossRef]
- Wei, Y.; Xu, J.; Miao, S.; Wei, K.; Peng, L.; Wang, Y.; Wei, X. Recent advances in the utilization of tea active ingredients to regulate sleep through neuroendocrine pathway, immune system and intestinal microbiota. Crit. Rev. Food Sci. Nutr. 2022, 63, 7598–7626. [Google Scholar] [CrossRef]
- Türközü, D.; Şanlier, N. L-theanine, unique amino acid of tea, and its metabolism, health effects, and safety. Crit. Rev. Food Sci. Nutr. 2017, 57, 1681–1687. [Google Scholar] [CrossRef]
- Ng, T.P.; Gao, Q.; Gwee, X.; Chua, D.Q.L. Tea Consumption and Depression from Follow Up in the Singapore Longitudinal Ageing Study. J. Nutr. Health Aging 2021, 25, 295–301. [Google Scholar] [CrossRef]
- Riemann, D.; Berger, M.; Voderholzer, U. Sleep and depression—Results from psychobiological studies: An overview. Biol. Psychol. 2001, 57, 67–103. [Google Scholar] [CrossRef]
- Plante, D.T. The Evolving Nexus of Sleep and Depression. Am. J. Psychiatry 2021, 178, 896–902. [Google Scholar] [CrossRef]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Shelton, R.C.; Claiborne, J.; Sidoryk-Wegrzynowicz, M.; Reddy, R.; Aschner, M.; Lewis, D.A.; Mirnics, K. Altered expression of genes involved in inflammation and apoptosis in frontal cortex in major depression. Mol. Psychiatry 2011, 16, 751–762. [Google Scholar] [CrossRef] [PubMed]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.L.; Rubinow, D.R.; Eisenlohr-Moul, T.A.; Xia, K.; Schmidt, P.J.; Girdler, S.S. Efficacy of Transdermal Estradiol and Micronized Progesterone in the Prevention of Depressive Symptoms in the Menopause Transition: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.S.; Soares, C.N.; Poitras, J.R.; Prouty, J.; Alexander, A.B.; Shifren, J.L. Short-term use of estradiol for depression in perimenopausal and postmenopausal women: A preliminary report. Am. J. Psychiatry 2003, 160, 1519–1522. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variables | Non-Tea Group 165 (42.7%) | Tea Group 221 (57.3%) | p |
|---|---|---|---|
| Only child | 0.647 | ||
| Yes | 155 (93.9%) | 205 (92.8%) | |
| No | 10 (6.1%) | 16 (7.2%) | |
| Educational level | 0.781 | ||
| Illiterate | 33 (20.0%) | 38 (17.2%) | |
| elementary | 67 (40.6%) | 93 (42.1%) | |
| junior high and above | 65 (39.4%) | 90 (40.7% | |
| Annual income ($) | 0.740 | ||
| <1369 | 79(47.9%) | 101 (45.7%) | |
| 1369–4100 | 61 (37.0%) | 90 (40.7%) | |
| >4100 | 25(15.2%) | 30 (13.6%) | |
| Live alone | 0.511 | ||
| Yes | 11 (6.7%) | 11 (5.0%) | |
| No | 154 (93.3%) | 210 (95.0%) | |
| Type of work | 0.336 | ||
| Peasant | 117 (70.9%) | 171 (77.4%) | |
| Housewife | 34 (18.8%) | 34 (14.9%) | |
| Retired group | 14 (8.5%) | 16 (7.2%) | |
| Sleep duration | 0.992 | ||
| >9 h | 3.0% (5) | 3.2% (7) | |
| 7–9 h | 33.9% (56) | 34.8% (77) | |
| 6–7 h | 30.3% (50) | 30.8% (68) | |
| <6 h | 32.7% (54) | 31.2% (69) | |
| Degree of insomnia | 0.003 | ||
| None | 119 (72.1%) | 189 (85.5%) | |
| Mild | 40 (24.2%) | 25 (11.3%) | |
| Moderate and above | 6 (3.6%) | 7 (3.2%) | |
| Degree of social support | 0.187 | ||
| High | 94 (57.0%) | 146 (66.1%) | |
| medium | 65 (39.4%) | 68 (30.8%) | |
| low | 6 (3.6%) | 7 (3.2%) | |
| Degree of depression | 0.002 | ||
| None | 113 (68.5%) | 185 (83.7%) | |
| Mild | 30 (18.2%) | 21 (9.5%) | |
| Moderate and above | 22 (13.3%) | 15 (6.8%) |
| Variables | Non-Tea Group 165 (42.7%) | Tea Group 221 (57.3%) | Z | p |
|---|---|---|---|---|
| Age | 61.94 (57–67) | 61.93 (56–68) | −0.053 | 0.958 |
| Heart rate | 75.12 (69–80) | 74.24 (68–81) | −0.730 | 0.465 |
| Systolic | 123.02 (111.0–133.5) | 124.83 (109.5–137.0) | −0.873 | 0.383 |
| Diastolic | 77.32 (68.0–84.0) | 78.84 (69.0–87.0) | −0.592 | 0.554 |
| BMI | 24.78 (22.89–26.64) | 23.23 (21.23–25.10) | −5.140 | <0.001 |
| TSH(mIU/L) | 3.79 (2.16–3.84) | 4.13 (1.69–4.36) | −0.263 | 0.792 |
| FT4(pmol/L) | 17.70 (14.32–18.58) | 17.23 (14.58–18.45) | −0.02 | 0.984 |
| FT3(pmol/L) | 4.85 (4.51–5.14) | 4.84 (4.57–5.24) | −1.229 | 0.219 |
| SII | 427.02 (281.31–526.07) | 387.65 (249.77–485.59) | −2.132 | 0.033 |
| Estradiol(pg/mL) | 27.35 (13.45–30.61) | 33.57 (18.63–29.81) | −3.710 | <0.001 |
| Testosterone(ng/dL) | 15.47 (7.95–15.30) | 16.85 (8.28–15.81) | −1.044 | 0.297 |
| DOD | Age | EL | AI | HR | SBP | DBP | TSH | FT4 | FT3 | BMI | SII | E2 | T | DOI | DOSS | SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DOD | 1.000 | ||||||||||||||||
| age | −0.006 | 1.000 | |||||||||||||||
| EL | −0.127 * | −0.256 *** | 1.000 | ||||||||||||||
| AI | −0.064 | −0.225 *** | 0.186 *** | 1.000 | |||||||||||||
| HR | 0.060 | −0.163 ** | 0.038 | 0.045 | 1.000 | ||||||||||||
| SBP | −0.055 | 0.026 | 0.062 | 0.047 | 0.259 *** | 1.000 | |||||||||||
| DBP | −0.042 | −0.119 * | 0.089 | 0.053 | 0.287 ** | 0.658 ** | 1.000 | ||||||||||
| TSH | −0.048 | −0.053 | 0.050 | 0.037 | −0.071 | 0.012 | −0.027 | 1.000 | |||||||||
| FT4 | 0.022 | 0.082 | 0.005 | −0.025 | 0.153 ** | 0.099 | 0.083 | −0.238 *** | 1.000 | ||||||||
| FT3 | 0.071 | −0.070 | 0.032 | −0.054 | 0.020 | −0.023 | 0.057 | −0.077 | 0.205 *** | 1.000 | |||||||
| BMI | −0.000 | −0.025 | 0.092 | 0.111 * | 0.071 | 0.112 * | 0.076 | 0.032 | −0.041 | 0.053 | 1.000 | ||||||
| SII | 0.149 ** | 0.026 | −0.006 | 0.011 | 0.053 | 0.084 | 0.078 | −0.064 | 0.053 | −0.084 | 0.041 | 1.000 | |||||
| E2 | −0.324 *** | −0.095 | 0.005 | −0.032 | −0.078 | −0.092 | 0.000 | 0.032 | −0.001 | −0.009 | 0.009 | −0.050 | 1.000 | ||||
| T | −0.087 | −0.070 | 0.025 | 0.037 | 0.046 | 0.000 | 0.026 | 0.066 | −0.033 | 0.005 | 0.021 | −0.059 | 0.161 ** | 1.000 | |||
| DOI | 0.294 *** | 0.073 ** | −0.089 | −0.086 | 0.003 | −0.031 | 0.019 | −0.067 | 0.016 | 0.022 | 0.070 | 0.053 | −0.155 * | −0.143 ** | 1.000 | ||
| DOSS | 0.159 ** | 0.023 | 0.023 | −0.025 | −0.013 | −0.063 | −0.036 | 0.010 | 0.006 | 0.035 | 0.024 | 0.009 | 0.009 | −0.002 ** | 0.132 ** | 1.000 | |
| SD | 0.129 * | 0.157 ** | −0.087 | −0.097 | −0.037 | −0.003 | −0.020 | −0.043 | −0.009 | −0.59 | 0.010 | 0.049 | −0.116 * | −0.034 | 0.502 ** | 0.011 | 1.000 |
| Mediating Effect Path | Effect Value | Boot SE | Boot LLCI | Boot ULCI | Relative Mediation Effect |
|---|---|---|---|---|---|
| Total indirect effect | −0.094 * | 0.030 | −0.160 | −0.043 | 45.2% |
| Tea→SII→Depression | −0.022 * | 0.012 | −0.055 | −0.003 | 10.3% |
| Tea→Estradiol→Depression | −0.014 * | 0.008 | −0.032 | −0.001 | 6.7% |
| Tea→Insomnia→Depression | −0.059 * | 0.025 | −0.118 | −0.018 | 28.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wan, Z.; Qin, X.; Tian, Y.; Ouyang, F.; Wang, G.; Wan, Q. Long-Term Consumption of Green Tea Can Reduce the Degree of Depression in Postmenopausal Women by Increasing Estradiol. Nutrients 2023, 15, 4514. https://doi.org/10.3390/nu15214514
Wan Z, Qin X, Tian Y, Ouyang F, Wang G, Wan Q. Long-Term Consumption of Green Tea Can Reduce the Degree of Depression in Postmenopausal Women by Increasing Estradiol. Nutrients. 2023; 15(21):4514. https://doi.org/10.3390/nu15214514
Chicago/Turabian StyleWan, Zhenyu, Xucong Qin, Yuling Tian, Fangcheng Ouyang, Gaohua Wang, and Qirong Wan. 2023. "Long-Term Consumption of Green Tea Can Reduce the Degree of Depression in Postmenopausal Women by Increasing Estradiol" Nutrients 15, no. 21: 4514. https://doi.org/10.3390/nu15214514
APA StyleWan, Z., Qin, X., Tian, Y., Ouyang, F., Wang, G., & Wan, Q. (2023). Long-Term Consumption of Green Tea Can Reduce the Degree of Depression in Postmenopausal Women by Increasing Estradiol. Nutrients, 15(21), 4514. https://doi.org/10.3390/nu15214514