
Cholesterol Levels, Hormone Replacement Therapy, and Incident Dementia among Older Adult Women

Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnosis of Non-Dementia and Dementia in the HAICDDS Database
2.2. Definition of Conversion
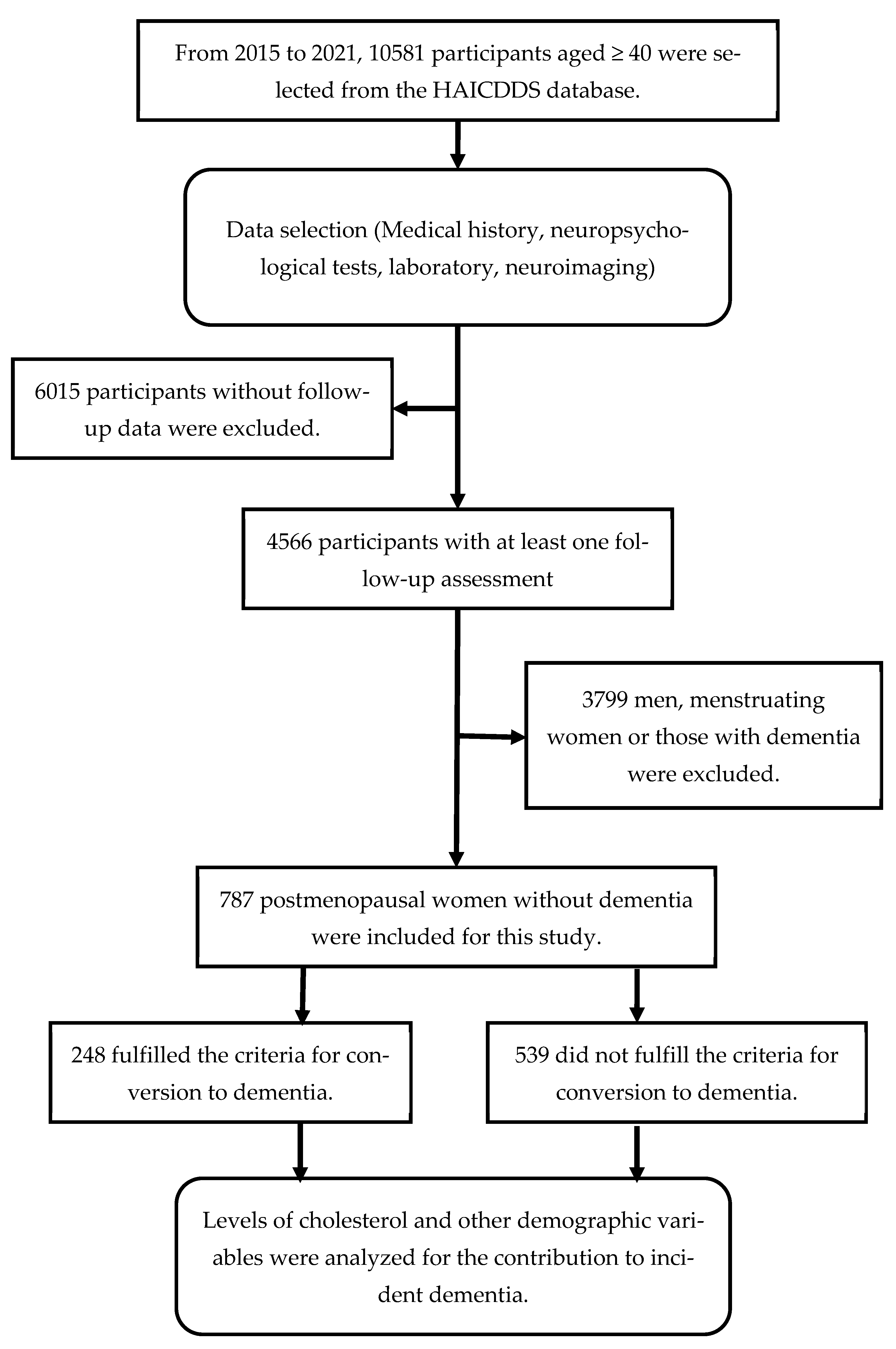
2.3. Study Procedure
2.4. Statistics
2.5. Ethical Consideration
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raz, L.; Knoefel, J.; Bhaskar, K. The neuropathology and cerebrovascular mechanisms of dementia. J. Cereb. Blood Flow Metab. 2016, 36, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Hyman, B.T.; Phelps, C.H.; Beach, T.G.; Bigio, E.H.; Cairns, N.J.; Carrillo, M.C.; Dickson, D.W.; Duyckaerts, C.; Frosch, M.P.; Masliah, E.; et al. National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers. Dement. 2012, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Barker, W.W.; Luis, C.A.; Kashuba, A.; Luis, M.; Harwood, D.G.; Loewenstein, D.; Waters, C.; Jimison, P.; Shepherd, E.; Sevush, S.; et al. Relative frequencies of Alzheimer disease, Lewy body, vascular and frontotemporal dementia, and hippocampal sclerosis in the State of Florida Brain Bank. Alzheimer Dis. Assoc. Disord. 2002, 16, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Spillantini, M.G.; Schmidt, M.L.; Lee, V.M.; Trojanowski, J.Q.; Jakes, R.; Goedert, M. Alpha-synuclein in Lewy bodies. Nature 1997, 388, 839–840. [Google Scholar] [CrossRef] [PubMed]
- Pertesi, S.; Coughlan, G.; Puthusseryppady, V.; Morris, E.; Hornberger, M. Menopause, cognition and dementia—A review. Post Reprod. Health 2019, 25, 200–206. [Google Scholar] [CrossRef]
- Hogervorst, E.; Bandelow, S. Brain and cognition. Is there any case for improving cognitive function in menopausal women using estrogen treatment? Minerva Ginecol. 2009, 61, 499–515. [Google Scholar]
- Langer, R.D.; Hodis, H.N.; Lobo, R.A.; Allison, M.A. Hormone replacement therapy—Where are we now? Climacteric 2021, 24, 3–10. [Google Scholar] [CrossRef]
- Flores, V.A.; Pal, L.; Manson, J.E. Hormone Therapy in Menopause: Concepts, Controversies, and Approach to Treatment. Endocr. Rev. 2021, 42, 720–752. [Google Scholar] [CrossRef]
- Stute, P.; Wienges, J.; Koller, A.S.; Giese, C.; Wesemuller, W.; Janka, H.; Baumgartner, S. Cognitive health after menopause: Does menopausal hormone therapy affect it? Best Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101565. [Google Scholar] [CrossRef]
- Pourhadi, N.; Morch, L.S.; Holm, E.A.; Torp-Pedersen, C.; Meaidi, A. Menopausal hormone therapy and dementia: Nationwide, nested case-control study. BMJ 2023, 381, e072770. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; Wright, L.; McFadden, E.; Griffin, J.; Thomas, D.; Hemming, J.; Wright, K.; Ashworth, A.; Swerdlow, A.J. Menopausal hormone therapy and breast cancer: What is the true size of the increased risk? Br. J. Cancer 2016, 115, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Johansson, T.; Fowler, P.; Ek, W.E.; Skalkidou, A.; Karlsson, T.; Johansson, A. Oral Contraceptives, Hormone Replacement Therapy, and Stroke Risk. Stroke 2022, 53, 3107–3115. [Google Scholar] [CrossRef] [PubMed]
- Strothmann, A.; Schneider, H.P. Hormone therapy: The European women’s perspective. Climacteric 2003, 6, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.; Kivipelto, M.; Wolozin, B.; Zhou, J.; Whitmer, R.A. Midlife serum cholesterol and increased risk of Alzheimer’s and vascular dementia three decades later. Dement. Geriatr. Cogn. Disord. 2009, 28, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.; White, L.R.; Xue, Q.L.; Launer, L.J. Twenty-six-year change in total cholesterol levels and incident dementia: The Honolulu-Asia Aging Study. Arch. Neurol. 2007, 64, 103–107. [Google Scholar] [CrossRef]
- Mielke, M.M.; Zandi, P.P.; Sjogren, M.; Gustafson, D.; Ostling, S.; Steen, B.; Skoog, I. High total cholesterol levels in late life associated with a reduced risk of dementia. Neurology 2005, 64, 1689–1695. [Google Scholar] [CrossRef]
- Ding, D.; Zhou, F.; Cao, Y.; Liang, X.; Wu, W.; Xiao, Z.; Zhao, Q.; Deng, W. Cholesterol profiles and incident cognitive decline among older adults: The Shanghai Aging Study. Age Ageing 2021, 50, 472–479. [Google Scholar] [CrossRef]
- Moroney, J.T.; Tang, M.X.; Berglund, L.; Small, S.; Merchant, C.; Bell, K.; Stern, Y.; Mayeux, R. Low-density lipoprotein cholesterol and the risk of dementia with stroke. JAMA 1999, 282, 254–260. [Google Scholar] [CrossRef]
- Marin, R.; Fabelo, N.; Martin, V.; Garcia-Esparcia, P.; Ferrer, I.; Quinto-Alemany, D.; Diaz, M. Anomalies occurring in lipid profiles and protein distribution in frontal cortex lipid rafts in dementia with Lewy bodies disclose neurochemical traits partially shared by Alzheimer’s and Parkinson’s diseases. Neurobiol. Aging 2017, 49, 52–59. [Google Scholar] [CrossRef]
- Reitz, C. Dyslipidemia and dementia: Current epidemiology, genetic evidence, and mechanisms behind the associations. J. Alzheimers Dis. 2012, 30 (Suppl. S2), S127–S145. [Google Scholar] [CrossRef]
- Schengrund, C.L. Lipid rafts: Keys to neurodegeneration. Brain Res. Bull. 2010, 82, 7–17. [Google Scholar] [CrossRef]
- Michel, V.; Bakovic, M. Lipid rafts in health and disease. Biol. Cell 2007, 99, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Moll, T.; Marshall, J.N.G.; Soni, N.; Zhang, S.; Cooper-Knock, J.; Shaw, P.J. Membrane lipid raft homeostasis is directly linked to neurodegeneration. Essays Biochem. 2021, 65, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.; Khan, S. Plasma Lipids as Biomarkers for Alzheimer’s Disease: A Systematic Review. Cureus 2020, 12, e12008. [Google Scholar] [CrossRef]
- Suryadevara, V.; Storey, S.G.; Aronow, W.S.; Ahn, C. Association of abnormal serum lipids in elderly persons with atherosclerotic vascular disease and dementia, atherosclerotic vascular disease without dementia, dementia without atherosclerotic vascular disease, and no dementia or atherosclerotic vascular disease. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, M859–M861. [Google Scholar] [CrossRef] [PubMed]
- Ban, Y.; Watanabe, T.; Miyazaki, A.; Nakano, Y.; Tobe, T.; Idei, T.; Iguchi, T.; Ban, Y.; Katagiri, T. Impact of increased plasma serotonin levels and carotid atherosclerosis on vascular dementia. Atherosclerosis 2007, 195, 153–159. [Google Scholar] [CrossRef]
- Zandi, P.P.; Sparks, D.L.; Khachaturian, A.S.; Tschanz, J.; Norton, M.; Steinberg, M.; Welsh-Bohmer, K.A.; Breitner, J.C.; Cache County Study Investigators. Do statins reduce risk of incident dementia and Alzheimer disease? The Cache County Study. Arch. Gen. Psychiatry 2005, 62, 217–224. [Google Scholar] [CrossRef]
- Hung, C.H.; Hung, G.U.; Wei, C.Y.; Tzeng, R.C.; Chiu, P.Y. Function-based dementia severity assessment for vascular cognitive impairment. J. Formos. Med. Assoc. 2021, 120, 533–541. [Google Scholar] [CrossRef]
- Yang, Y.W.; Hsu, K.C.; Wei, C.Y.; Tzeng, R.C.; Chiu, P.Y. Operational Determination of Subjective Cognitive Decline, Mild Cognitive Impairment, and Dementia Using Sum of Boxes of the Clinical Dementia Rating Scale. Front. Aging Neurosci. 2021, 13, 705782. [Google Scholar] [CrossRef]
- Wang, T.Y.; Chang, W.L.; Wei, C.Y.; Liu, C.H.; Tzeng, R.C.; Chiu, P.Y. Cholesterol Paradox in Older People with Type 2 Diabetes Mellitus Regardless of Lipid-Lowering Drug Use: A Cross-Sectional Cohort Study. Nutrients 2023, 15, 3270. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.N.; Wang, P.N.; Liu, C.Y.; Chen, W.T.; Lee, Y.C.; Liu, H.C. Cutoff scores of the cognitive abilities screening instrument, Chinese version in screening of dementia. Dement. Geriatr. Cogn. Disord. 2002, 14, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Cummings, J.L. The Neuropsychiatric Inventory: Assessing psychopathology in dementia patients. Neurology 1997, 48, S10–S16. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Lacritz, L.H.; Hall, J.; Waring, S.C.; Chan, W.; Khodr, Z.G.; Massman, P.J.; Hobson, V.; Cullum, C.M. Validation of the new interpretive guidelines for the clinical dementia rating scale sum of boxes score in the national Alzheimer’s coordinating center database. Arch. Neurol. 2010, 67, 746–749. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Waring, S.C.; Cullum, C.M.; Hall, J.; Lacritz, L.; Massman, P.J.; Lupo, P.J.; Reisch, J.S.; Doody, R.; Texas Alzheimer’s Research, C. Staging dementia using Clinical Dementia Rating Scale Sum of Boxes scores: A Texas Alzheimer’s research consortium study. Arch. Neurol. 2008, 65, 1091–1095. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, R.C.; Yang, Y.W.; Hsu, K.C.; Chang, H.T.; Chiu, P.Y. Sum of boxes of the clinical dementia rating scale highly predicts conversion or reversion in predementia stages. Front. Aging Neurosci. 2022, 14, 1021792. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- Simons, K.; Toomre, D. Lipid rafts and signal transduction. Nat. Rev. Mol. Cell Biol. 2000, 1, 31–39. [Google Scholar] [CrossRef]
- Jacobson, K.; Mouritsen, O.G.; Anderson, R.G. Lipid rafts: At a crossroad between cell biology and physics. Nat. Cell Biol. 2007, 9, 7–14. [Google Scholar] [CrossRef]
- Lingwood, D.; Simons, K. Lipid rafts as a membrane-organizing principle. Science 2010, 327, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Tsui-Pierchala, B.A.; Encinas, M.; Milbrandt, J.; Johnson, E.M., Jr. Lipid rafts in neuronal signaling and function. Trends Neurosci. 2002, 25, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.Y.; McLaurin, J. Mechanisms of amyloid-Beta Peptide uptake by neurons: The role of lipid rafts and lipid raft-associated proteins. Int. J. Alzheimers Dis. 2010, 2011, 548380. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, M.; Honda, A.; Kawasaki, A.; Nozumi, M. Neuronal Signaling Involved in Neuronal Polarization and Growth: Lipid Rafts and Phosphorylation. Front. Mol. Neurosci. 2020, 13, 150. [Google Scholar] [CrossRef]
- Frank, C.; Rufini, S.; Tancredi, V.; Forcina, R.; Grossi, D.; D’Arcangelo, G. Cholesterol depletion inhibits synaptic transmission and synaptic plasticity in rat hippocampus. Exp. Neurol. 2008, 212, 407–414. [Google Scholar] [CrossRef]
- Krivoi, I.I.; Petrov, A.M. Cholesterol and the Safety Factor for Neuromuscular Transmission. Int. J. Mol. Sci. 2019, 20, 1046. [Google Scholar] [CrossRef]
- Saher, G.; Brugger, B.; Lappe-Siefke, C.; Mobius, W.; Tozawa, R.; Wehr, M.C.; Wieland, F.; Ishibashi, S.; Nave, K.A. High cholesterol level is essential for myelin membrane growth. Nat. Neurosci. 2005, 8, 468–475. [Google Scholar] [CrossRef]
- Berghoff, S.A.; Spieth, L.; Sun, T.; Hosang, L.; Depp, C.; Sasmita, A.O.; Vasileva, M.H.; Scholz, P.; Zhao, Y.; Krueger-Burg, D.; et al. Neuronal cholesterol synthesis is essential for repair of chronically demyelinated lesions in mice. Cell. Rep. 2021, 37, 109889. [Google Scholar] [CrossRef]
- Langa, K.M.; Larson, E.B.; Crimmins, E.M.; Faul, J.D.; Levine, D.A.; Kabeto, M.U.; Weir, D.R. A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012. JAMA Intern. Med. 2017, 177, 51–58. [Google Scholar] [CrossRef]
- Sun, Y.; Lee, H.J.; Yang, S.C.; Chen, T.F.; Lin, K.N.; Lin, C.C.; Wang, P.N.; Tang, L.Y.; Chiu, M.J. A nationwide survey of mild cognitive impairment and dementia, including very mild dementia, in Taiwan. PLoS ONE 2014, 9, e100303. [Google Scholar] [CrossRef]
- Gray, S.L.; Anderson, M.L.; Hubbard, R.A.; LaCroix, A.; Crane, P.K.; McCormick, W.; Bowen, J.D.; McCurry, S.M.; Larson, E.B. Frailty and incident dementia. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.; Xue, Q.L.; Masaki, K.; Petrovitch, H.; Ross, G.W.; White, L.R.; Launer, L.J. Change in blood pressure and incident dementia: A 32-year prospective study. Hypertension 2009, 54, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.; Launer, L.J.; Dewey, M.E.; Letenneur, L.; Ott, A.; Copeland, J.R.; Dartigues, J.F.; Kragh-Sorensen, P.; Baldereschi, M.; Brayne, C.; et al. Gender differences in the incidence of AD and vascular dementia: The EURODEM Studies. EURODEM Incidence Research Group. Neurology 1999, 53, 1992–1997. [Google Scholar] [CrossRef] [PubMed]
- Azad, N.A.; Al Bugami, M.; Loy-English, I. Gender differences in dementia risk factors. Gend. Med. 2007, 4, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Dufouil, C.; Richard, F.; Fievet, N.; Dartigues, J.F.; Ritchie, K.; Tzourio, C.; Amouyel, P.; Alperovitch, A. APOE genotype, cholesterol level, lipid-lowering treatment, and dementia: The Three-City Study. Neurology 2005, 64, 1531–1538. [Google Scholar] [CrossRef]
- Hogervorst, E.; Williams, J.; Budge, M.; Riedel, W.; Jolles, J. The nature of the effect of female gonadal hormone replacement therapy on cognitive function in post-menopausal women: A meta-analysis. Neuroscience 2000, 101, 485–512. [Google Scholar] [CrossRef]
- Lin, S.K.; Tsai, Y.T.; Lai, J.N.; Wu, C.T. Demographic and medication characteristics of traditional Chinese medicine users among dementia patients in Taiwan: A nationwide database study. J. Ethnopharmacol. 2015, 161, 108–115. [Google Scholar] [CrossRef]
- Lee, C.Y.; Sun, Y.; Lee, H.J.; Chen, T.F.; Wang, P.N.; Lin, K.N.; Tang, L.Y.; Lin, C.C.; Chiu, M.J. Modest Overweight and Healthy Dietary Habits Reduce Risk of Dementia: A Nationwide Survey in Taiwan. J. Prev. Alzheimers Dis. 2017, 4, 37–43. [Google Scholar] [CrossRef]
- Ho, W.M.; Wu, Y.Y.; Chen, Y.C. Genetic Variants behind Cardiovascular Diseases and Dementia. Genes 2020, 11, 1514. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Non-Converters Mean (SD) | Converters Mean (SD) | p-Value | |
|---|---|---|---|
| N | 539 | 248 | |
| Age, year | 70.3 (8.8) | 77.0 (7.2) | <0.001 |
| Education, year | 5.2 (4.4) | 4.1 (3.8) | <0.001 |
| Follow-up, year | 2.9 (1.5) | 3.3 (1.6) | <0.001 |
| CDR-SB | 1.3 (1.1) | 2.2 (1.2) | <0.001 |
| CASI | 76.2 (12.4) | 67.7 (11.1) | <0.001 |
| MoCA | 17.2 (6.4) | 12.6 (4.9) | <0.001 |
| HAIADL | 3.2 (2.4) | 5.0 (2.8) | <0.001 |
| NPI | 4.4 (6.3) | 4.6 (5.5) | NS |
| Cerebrovascular disease, N (%) | 106 (19.7) | 64 (25.8) | NS |
| Hypertension, N (%) | 378 (70.1) | 189 (76.2) | NS |
| Diabetes, N (%) | 192 (35.6) | 108 (43.5) | 0.040 |
| Dyslipidemia, N (%) | 348 (64.6) | 133 (53.6) | 0.005 |
| Coronary artery disease, N (%) | 52 (9.6) | 33 (13.3) | NS |
| Atrial fibrillation, N (%) | 70 (13.0) | 48 (19.4) | 0.024 |
| Congestive heart failure, N (%) | 42 (7.8) | 32 (12.9) | 0.026 |
| Regular exercise, N (%) | 288 (53.4) | 83 (33.5) | <0.001 |
| Hormone replacement therapy, N (%) | 68 (12.6) | 28 (11.3) | NS |
| Anti-Hypertensive, N (%) | 378 (70.1) | 189 (76.2) | NS |
| Anti-Diabetes, N (%) | 192 (35.6) | 108 (43.5) | 0.021 |
| Lipid-lowering drugs, N (%) | 348 (64.6) | 133 (53.6) | NS |
| Total Cholesterol | 182.9 (35.8) | 170.5 (39.6) | <0.001 |
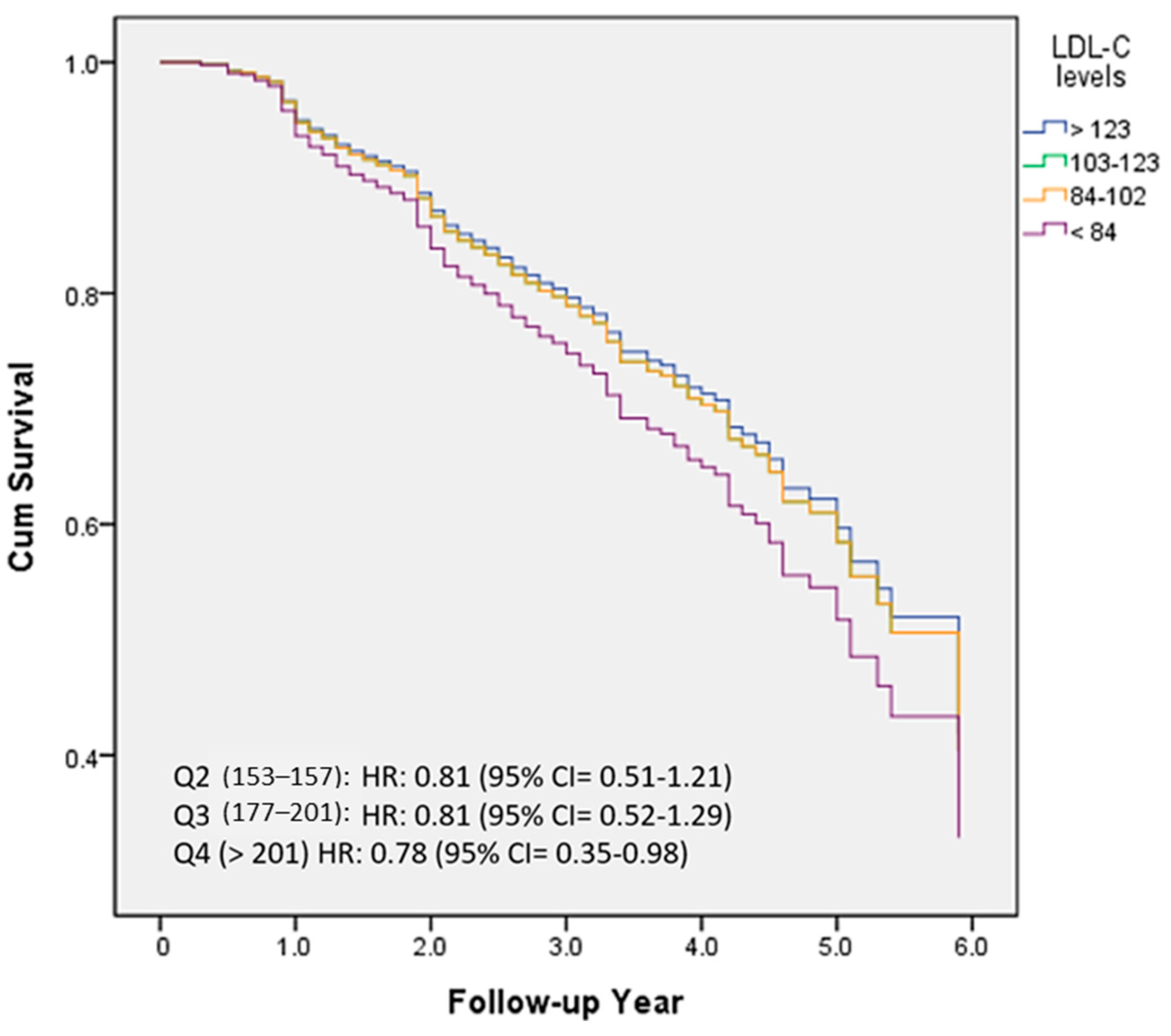
| Low-density lipoprotein cholesterol | 109.4 (32.2) | 98.8 (33.1) | <0.001 |
| High-density lipoprotein cholesterol | 54.8 (15.1) | 53.4 (17.4) | NS |
| Triglyceride | 129.7 (80.1) | 129.8 (87.2) | NS |
| Systolic blood pressure | 134.0 (18.3) | 135.9 (18.2) | NS |
| Ac glucose | 112.6 (36.0) | 119.0 (41.3) | 0.047 |
| Body mass index | 24.8 (3.1) | 24.0 (3.7) | NS |
| Creatinine | 0.8 (0.4) | 1.0 (0.6) | 0.002 |
| Variables | B | Wald | Sig | Exp | 95% Confidence Interval for Exp |
|---|---|---|---|---|---|
| Cholesterol | |||||
| Q1 (<153) | 0 | ||||
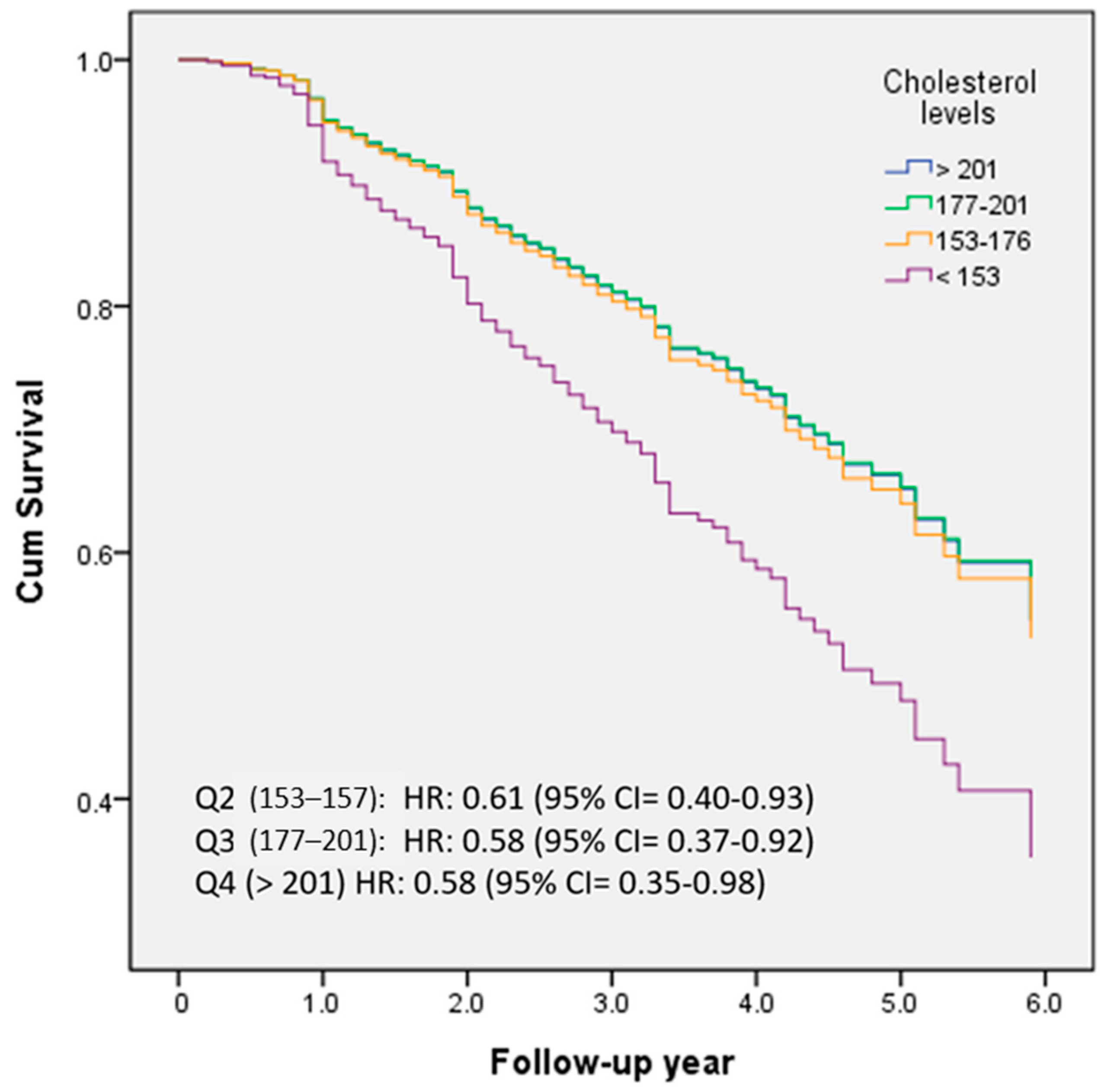
| Q2 (153–176) | −0.54 | 4.10 | 0.043 | 0.58 | 0.35–0.98 |
| Q3 (177–201) | −0.55 | 5.39 | 0.020 | 0.58 | 0.37–0.92 |
| Q4 (>201) | −0.50 | 5.28 | 0.022 | 0.61 | 0.70–0.93 |
| Age | 0.07 | 30.42 | <0.001 | 1.09 | 1.05–1.10 |
| Education | 0.09 | 12.28 | <0.001 | 1.09 | 1.04–1.14 |
| CASI | −0.03 | 6.74 | 0.009 | 0.98 | 0.96–0.99 |
| HAIADL | 0.11 | 10.64 | 0.001 | 1.11 | 1.04–1.19 |
| NPI | 0.03 | 3.62 | 0.057 | 1.03 | 1.00–1.05 |
| CVD | 0.14 | 0.53 | 0.465 | 1.15 | 0.79–1.67 |
| diabetes | −0.00 | 0.00 | 0.996 | 1.00 | 0.52–1.93 |
| hypertension | 0.06 | 0.02 | 0.888 | 1.06 | 0.49–2.27 |
| dyslipidemia | −0.01 | 0.00 | 0.973 | 0.99 | 0.65–1.52 |
| CAD | 0.32 | 1.89 | 0.169 | 1.38 | 0.87–2.17 |
| CHD | 0.40 | 2.66 | 0.103 | 1.49 | 0.92–2.42 |
| No exercise | 0.24 | 6.66 | 0.010 | 1.27 | 1.06–1.53 |
| Hormone replacement therapy | 0.24 | 0.79 | 0.375 | 1.26 | 0.75–2.13 |
| Antihypertensives | −0.04 | 0.01 | 0.928 | 0.97 | 0.45–2.06 |
| Anti-diabetes | 0.09 | 0.06 | 0.803 | 1.09 | 0.55–2.17 |
| Lipid-lowering drugs | −0.15 | 0.52 | 0.470 | 0.86 | 0.58–1.29 |
| SBP | 0.01 | 0.39 | 0.048 | 1.01 | 1.00–1.02 |
| Fasting glucose | 0.00 | 0.53 | 0.468 | 1.00 | 1.00–1.01 |
| Creatinine | 0.11 | 0.67 | 0.413 | 1.12 | 0.86–1.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, H.-Y.; Chang, H.-T.; Chan, P.-C.; Chiu, P.-Y. Cholesterol Levels, Hormone Replacement Therapy, and Incident Dementia among Older Adult Women. Nutrients 2023, 15, 4481. https://doi.org/10.3390/nu15204481
Chiu H-Y, Chang H-T, Chan P-C, Chiu P-Y. Cholesterol Levels, Hormone Replacement Therapy, and Incident Dementia among Older Adult Women. Nutrients. 2023; 15(20):4481. https://doi.org/10.3390/nu15204481
Chicago/Turabian StyleChiu, Huei-Ying, Hsin-Te Chang, Po-Chi Chan, and Pai-Yi Chiu. 2023. "Cholesterol Levels, Hormone Replacement Therapy, and Incident Dementia among Older Adult Women" Nutrients 15, no. 20: 4481. https://doi.org/10.3390/nu15204481
APA StyleChiu, H.-Y., Chang, H.-T., Chan, P.-C., & Chiu, P.-Y. (2023). Cholesterol Levels, Hormone Replacement Therapy, and Incident Dementia among Older Adult Women. Nutrients, 15(20), 4481. https://doi.org/10.3390/nu15204481