

The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review


Abstract
:1. Introduction
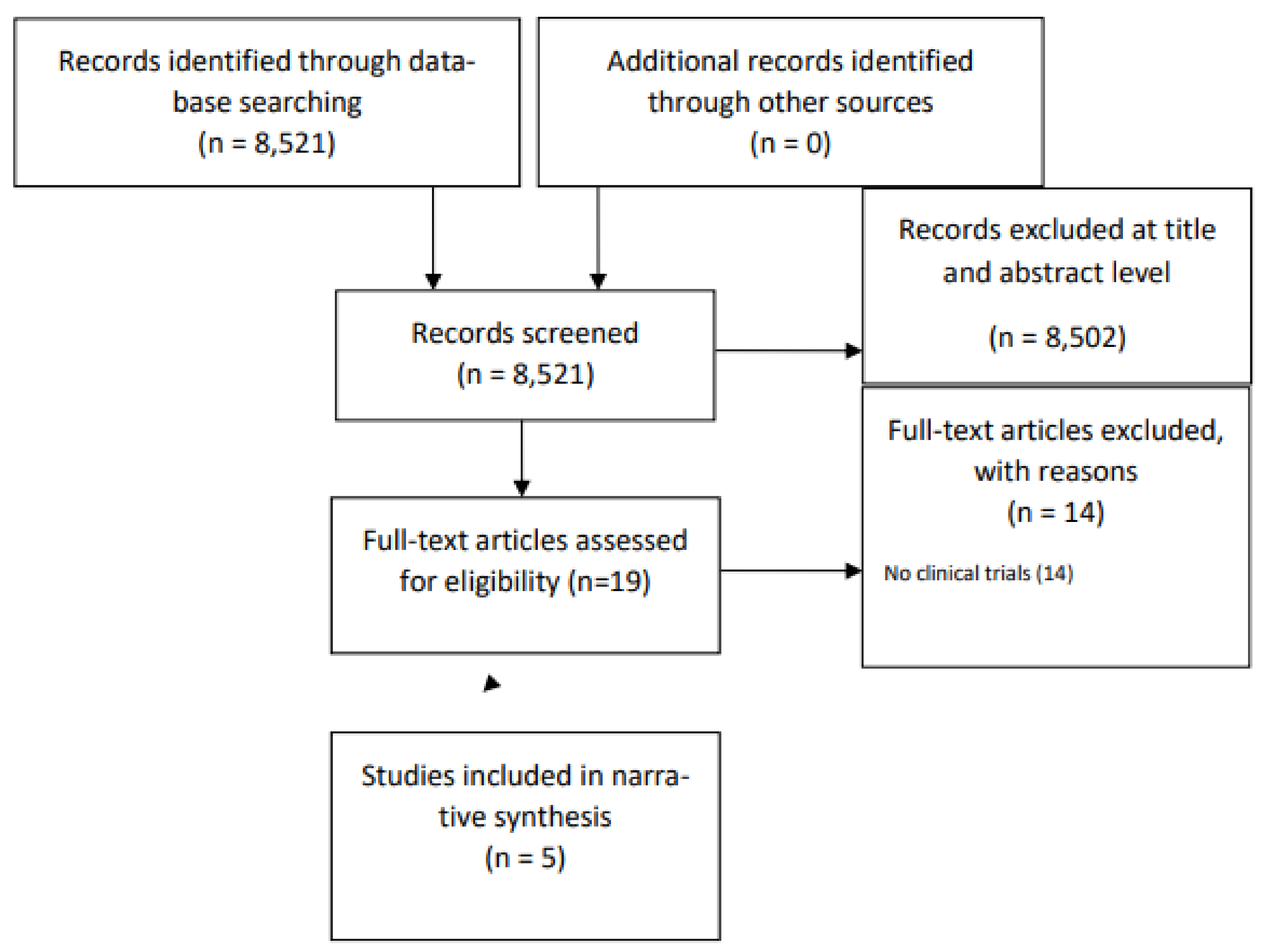
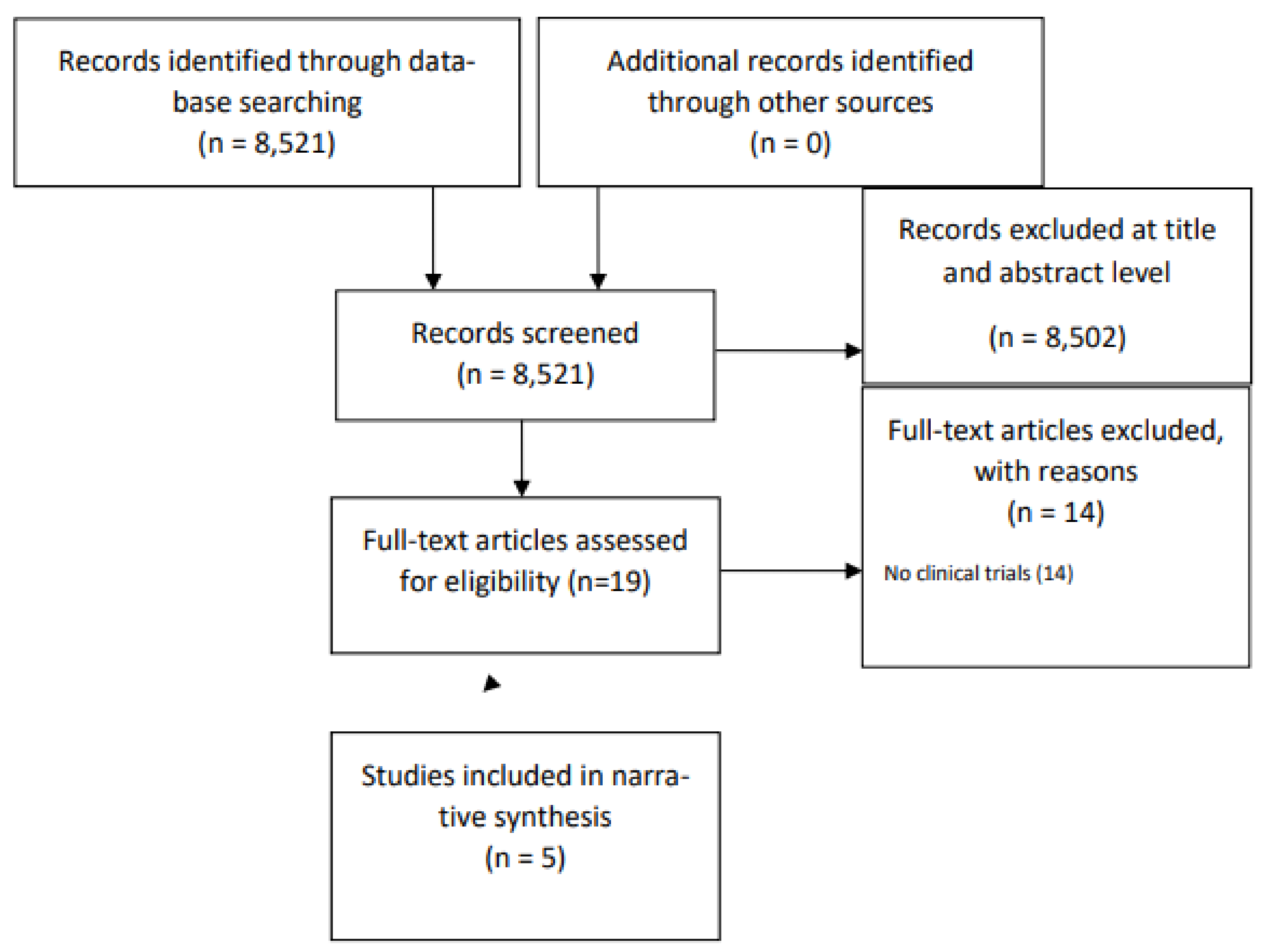
2. Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection Criteria
3. Results
3.1. Summary of Included Studies
3.2. Technical Aspects of tDCS in AN and Safety
3.3. Effects on Psychopathology and Eating Behaviour
3.4. Effects on AN Symptoms
3.5. Effects on Depressive Symptoms
3.6. Effects on Anxiety
3.7. Effects on BMI
3.8. Effects on Other Measurements
3.9. Durability of tDCS Effects
4. Discussion
4.1. General Findings
4.2. Impact on AN Symptoms, Psychopathology, and Eating Behaviours
4.3. Impact on BMI
4.4. Impact on Depression
4.5. Mechanisms of Action
4.6. Safety and Acceptance
4.7. Ethical Issues
4.8. Review Limitations and Risk of Bias
4.9. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, J. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, X.; Wang, J.; Chen, J.; Guo, Q.; Li, C.; Enck, P. Processing of food, body and emotional stimuli in anorexia nervosa: A systematic review and meta-analysis of functional magnetic resonance imaging studies. Eur. Eat. Disord. Rev. 2012, 20, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Fudge, J.L.; Paulus, M. New insights into symptoms and neurocircuit function of anorexia nervosa. Nat. Rev. Neurosci. 2009, 10, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.G.; Cohen, P.; Kasen, S.; Brook, J.S. Personality disorder traits evident by early adulthood and risk for eating and weight problems during middle adulthood. Int. J. Eat. Disord. 2006, 39, 184–192. [Google Scholar] [CrossRef]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology, course, and outcome of eating disorders. Curr. Opin. Psychiatry 2013, 26, 543–548. [Google Scholar] [CrossRef]
- Su, T.; Gong, J.; Tang, G.; Qiu, S.; Chen, P.; Chen, G.; Wang, J.; Huang, L.; Wang, Y. Structural and functional brain alterations in anorexia nervosa: A multimodal meta-analysis of neuroimaging studies. Hum. Brain Mapp. 2021, 42, 5154–5169. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Harrison, P.J. Eating disorders. Lancet 2003, 361, 407–416. [Google Scholar] [CrossRef]
- van Eeden, A.E.; van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef]
- Murray, S.B.; Nagata, J.M.; Griffiths, S.; Calzo, J.P.; Brown, T.A.; Mitchison, D.; Blashill, A.J.; Mond, J.M. The enigma of male eating disorders: A critical review and synthesis. Clin. Psychol. Rev. 2017, 57, 1–11. [Google Scholar] [CrossRef]
- Esposito, R.; Cieri, F.; di Giannantonio, M.; Tartaro, A. The role of body image and self-perception in anorexia nervosa: The neuroimaging perspective. J. Neuropsychol. 2018, 12, 41–52. [Google Scholar] [CrossRef]
- Schorr, M.; Miller, K.K. The endocrine manifestations of anorexia nervosa: Mechanisms and management. Nat. Rev. Endocrinol. 2017, 13, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia nervosa: Aetiology, assessment, and treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, A.; Svensson, M.; Jacobi, F.; Allgulander, C.; Alonso, J.; Beghi, E.; Dodel, R.; Ekman, M.; Faravelli, C.; Fratiglioni, L.; et al. Cost of disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 718–779. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.; Desmond, M.; Desai, J.; Lockert, J. The disconnect between treatment outcome data and reimbursement for the treatment of anorexia nervosa. Int. J. Physiatry 2016, 2, 1–6. [Google Scholar] [CrossRef]
- Steinhausen, H.C. The outcome of anorexia nervosa in the 20th century. Am. J. Psychiatry 2002, 159, 1284–1293. [Google Scholar] [CrossRef]
- Zipfel, S.; Lowe, B.; Reas, D.L.; Deter, H.C.; Herzog, W. Long-term prognosis in anorexia nervosa: Lessons from a 21-year follow-up study. Lancet 2000, 355, 721–722. [Google Scholar] [CrossRef]
- Sullivan, P.F. Mortality in anorexia nervosa. Am. J. Psychiatry 1995, 152, 1073–1074. [Google Scholar]
- Phillipou, A.; Rossell, S.L.; Castle, D.J. The neurobiology of anorexia nervosa: A systematic review. Aust. N. Z. J. Psychiatry 2014, 48, 128–152. [Google Scholar] [CrossRef]
- Murao, E.; Sugihara, G.; Isobe, M.; Noda, T.; Kawabata, M.; Matsukawa, N.; Takahashi, H.; Murai, T.; Noma, S. Differences in neural responses to reward and punishment processing between anorexia nervosa subtypes: An fMRI study. Psychiatry Clin. Neurosci. 2017, 71, 647–658. [Google Scholar] [CrossRef]
- Cassin, S.E.; von Ranson, K.M. Personality and eating disorders: A decade in review. Clin. Psychol. Rev. 2005, 25, 895–916. [Google Scholar] [CrossRef] [PubMed]
- Herzog, D.B.; Keller, M.B.; Sacks, N.R.; Yeh, C.J.; Lavori, P.W. Psychiatric comorbidity in treatment-seeking anorexics and bulimics. J. Am. Acad. Child Adolesc. Psychiatry 1992, 31, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Fouladi, F.; Mitchell, J.E.; Crosby, R.D.; Engel, S.G.; Crow, S.; Hill, L.; Le Grange, D.; Powers, P.; Steffen, K.J. Prevalence of Alcohol and Other Substance Use in Patients with Eating Disorders. Eur. Eat. Disord. Rev. 2015, 23, 531–536. [Google Scholar] [CrossRef]
- Nagata, T.; Kawarada, Y.; Kiriike, N.; Iketani, T. Multi-impulsivity of Japanese patients with eating disorders: Primary and secondary impulsivity. Psychiatry Res. 2000, 94, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Marsa, M.; Carrasco, J.L.; Saiz, J. A study of temperament and personality in anorexia and bulimia nervosa. J. Personal. Disord. 2000, 14, 352–359. [Google Scholar] [CrossRef]
- Kaye, W.H. Neurobiology of anorexia and bulimia nervosa. Physiol. Behav. 2008, 94, 121–135. [Google Scholar] [CrossRef]
- Frank, G.; Bailer, U.F.; Henry, S.; Drevets, W.; Meltzer, C.C.; Price, J.C.; Mathis, C.A.; Wagner, A.; Hoge, J.; Ziolko, S.; et al. Increased dopamine D2/D3 receptor binding after recovery from anorexia nervosa measured by positron emission tomography and [11C]ralopride. Biol. Psychiatry 2005, 58, 908–912. [Google Scholar] [CrossRef]
- Higgins, A. The Neurobiology of Anorexia Nervosa. In Anorexia and Bulimia Nervosa; IntechOpen: London, UK, 2019. [Google Scholar]
- Avena, N.M.; Bocarsly, M.E. Dysregulation of brain reward systems in eating disorders: Neurochemical information from animal models of binge eating, bulimia nervosa, and anorexia nervosa. Neuropharmacology 2012, 63, 87–96. [Google Scholar] [CrossRef]
- Riva, G. Neurobiology of Anorexia Nervosa: Serotonin Dysfunctions Link Self-Starvation with Body Image Disturbances through an Impaired Body Memory. Front. Hum. Neurosci. 2016, 10, 600. [Google Scholar] [CrossRef]
- Jenkins, T.A.; Nguyen, J.C.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef]
- Yabut, J.M.; Crane, J.D.; Green, A.E.; Keating, D.J.; Khan, W.I.; Steinberg, G.R. Emerging Roles for Serotonin in Regulating Metabolism: New Implications for an Ancient Molecule. Endocr. Rev. 2019, 40, 1092–1107. [Google Scholar] [CrossRef] [PubMed]
- Calati, R.; De Ronchi, D.; Bellini, M.; Serretti, A. The 5-HTTLPR polymorphism and eating disorders: A meta-analysis. Int. J. Eat. Disord. 2011, 44, 191–199. [Google Scholar] [CrossRef]
- Haleem, D.J. Serotonin neurotransmission in anorexia nervosa. Behav. Pharmacol. 2012, 23, 478–495. [Google Scholar] [CrossRef] [PubMed]
- Isingrini, E.; Perret, L.; Rainer, Q.; Amilhon, B.; Guma, E.; Tanti, A.; Martin, G.; Robinson, J.; Moquin, L.; Marti, F.; et al. Resilience to chronic stress is mediated by noradrenergic regulation of dopamine neurons. Nat. Neurosci. 2016, 19, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Delvenne, V.; Lotstra, F.; Goldman, S.; Biver, F.; De Maertelaer, V.; Appelboom-Fondu, J.; Schoutens, A.; Bidaut, L.M.; Luxen, A.; Mendelwicz, J. Brain hypometabolism of glucose in anorexia nervosa: A PET scan study. Biol. Psychiatry 1995, 37, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Kojima, S.; Nagai, N.; Nakabeppu, Y.; Muranaga, T.; Deguchi, D.; Nakajo, M.; Masuda, A.; Nozoe, S.I.; Naruo, T. Comparison of regional cerebral blood flow in patients with anorexia nervosa before and after weight gain. Psychiatry Res. 2005, 140, 251–258. [Google Scholar] [CrossRef]
- Naruo, T.; Nakabeppu, Y.; Deguchi, D.; Nagai, N.; Tsutsui, J.; Nakajo, M.; Nozoe, S.I. Decreases in blood perfusion of the anterior cingulate gyri in anorexia nervosa restricters assessed by SPECT image analysis. BMC Psychiatry 2001, 1, 2. [Google Scholar] [CrossRef]
- Takano, A.; Shiga, T.; Kitagawa, N.; Koyama, T.; Katoh, C.; Tsukamoto, E.; Tamaki, N. Abnormal neuronal network in anorexia nervosa studied with I-123-IMP SPECT. Psychiatry Res. 2001, 107, 45–50. [Google Scholar] [CrossRef]
- Frank, G.K.; Bailer, U.F.; Meltzer, C.C.; Price, J.C.; Mathis, C.A.; Wagner, A.; Becker, C.; Kaye, W.H. Regional cerebral blood flow after recovery from anorexia or bulimia nervosa. Int. J. Eat. Disord. 2007, 40, 488–492. [Google Scholar] [CrossRef]
- Yonezawa, H.; Otagaki, Y.; Miyake, Y.; Okamoto, Y.; Yamawaki, S. No differences are seen in the regional cerebral blood flow in the restricting type of anorexia nervosa compared with the binge eating/purging type. Psychiatry Clin. Neurosci. 2008, 62, 26–33. [Google Scholar] [CrossRef]
- Beato-Fernández, L.; Rodríguez-Cano, T.; García-Vilches, I.; García-Vicente, A.; Poblete-García, V.; Castrejon, A.S.; Toro, J. Changes in regional cerebral blood flow after body image exposure in eating disorders. Psychiatry Res. 2009, 171, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Ruf, M.; Braus, D.F.; Schmidt, M.H. Neuronal activity changes and body image distortion in anorexia nervosa. Neuroreport 2003, 14, 2193–2197. [Google Scholar] [CrossRef] [PubMed]
- Kuruoglu, A.C.; Kapucu, O.; Atasever, T.; Arikan, Z.; Işik, E.; Unlü, M. Technetium-99m-HMPAO brain SPECT in anorexia nervosa. J. Nucl. Med. 1998, 39, 304–306. [Google Scholar]
- Pietrini, F.; Castellini, G.; Ricca, V.; Polito, C.; Pupi, A.; Faravelli, C. Functional neuroimaging in anorexia nervosa: A clinical approach. Eur. Psychiatry 2011, 26, 176–182. [Google Scholar] [CrossRef]
- Been, G.; Ngo, T.T.; Miller, S.M.; Fitzgerald, P.B. The use of tDCS and CVS as methods of non-invasive brain stimulation. Brain Res. Rev. 2007, 56, 346–361. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Wilfurth, S.; Landgrebe, M.; Eichhammer, P.; Hajak, G.; Langguth, B. Anodal skin lesions after treatment with transcranial direct current stimulation. Brain Stimul. 2010, 3, 58–59. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Lang, N.; Siebner, H.R.; Ward, N.S.; Lee, L.; Nitsche, M.A.; Paulus, W.; Rothwell, J.C.; Lemon, R.N.; Frackowiak, R.S. How does transcranial DC stimulation of the primary motor cortex alter regional neuronal activity in the human brain? Eur. J. Neurosci. 2005, 22, 495–504. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Doemkes, S.; Karaköse, T.; Antal, A.; Liebetanz, D.; Lang, N.; Tergau, F.; Paulus, W. Shaping the effects of transcranial direct current stimulation of the human motor cortex. J. Neurophysiol. 2007, 97, 3109–3117. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Koschack, J.; Pohlers, H.; Hullemann, S.; Paulus, W.; Happe, S. Effects of frontal transcranial direct current stimulation on emotional state and processing in healthy humans. Front. Psychol. 2012, 3, 58. [Google Scholar] [CrossRef]
- Fritsch, B.; Reis, J.; Martinowich, K.; Schambra, H.M.; Ji, Y.; Cohen, L.G.; Lu, B. Direct current stimulation promotes BDNF-dependent synaptic plasticity: Potential implications for motor learning. Neuron 2010, 66, 198–204. [Google Scholar] [CrossRef]
- Kronberg, G.; Bridi, M.; Abel, T.; Bikson, M.; Parra, L.C. Direct current stimulation modulates LTP and LTD: Activity dependence and dendritic effects. Brain Stimul. 2017, 10, 51–58. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Liebetanz, D.; Schlitterlau, A.; Henschke, U.; Fricke, K.; Frommann, K.; Lang, N.; Henning, S.; Paulus, W.; Tergau, F. GABAergic modulation of DC stimulation-induced motor cortex excitability shifts in humans. Eur. J. Neurosci. 2004, 19, 2720–2726. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Seeber, A.; Frommann, K.; Klein, C.C.; Rochford, C.; Nitsche, M.S.; Fricke, K.; Liebetanz, D.; Lang, N.; Antal, A.; et al. Modulating parameters of excitability during and after transcranial direct current stimulationof the human motor cortex. J. Physiol. 2005, 568 Pt 1, 291–303. [Google Scholar] [CrossRef]
- Stagg, C.J.; Best, J.G.; Stephenson, M.C.; O’Shea, J.; Wylezinska, M.; Kincses, Z.T.; Morris, P.G.; Matthews, P.M.; Johansen-Berg, H. Polarity-sensitive modulation of cortical neurotransmitters by transcranial stimulation. J. Neurosci. 2009, 29, 5202–5206. [Google Scholar] [CrossRef]
- Reed, T.; Cohen Kadosh, R. Transcranial electrical stimulation (tES) mechanisms and its effects on cortical excitability and connectivity. J. Inherit. Metab. Dis. 2018, 41, 1123–1130. [Google Scholar] [CrossRef]
- Lisman, J.E. Three Ca2+ levels affect plasticity differently: The LTP zone, the LTD zone and no man’s land. J. Physiol. 2001, 532 Pt 2, 28. [Google Scholar] [CrossRef]
- Sousa, B.; Martins, J.; Castelo-Branco, M.; Gonçalves, J. Transcranial Direct Current Stimulation as an Approach to Mitigate Neurodevelopmental Disorders Affecting Excitation/Inhibition Balance: Focus on Autism Spectrum Disorder, Schizophrenia, and Attention Deficit/Hyperactivity Disorder. J. Clin. Med. 2022, 11, 2839. [Google Scholar] [CrossRef]
- Duriez, P.; Bou Khalil, R.; Chamoun, Y.; Maatoug, R.; Strumila, R.; Seneque, M.; Gorwood, P.; Courtet, P.; Guillaume, S. Brain Stimulation in Eating Disorders: State of the Art and Future Perspectives. J. Clin. Med. 2020, 9, 2358. [Google Scholar] [CrossRef]
- Beaumont, J.D.; Smith, N.C.; Starr, D.; Davis, D.; Dalton, M.; Nowicky, A.; Russell, M.; Barwood, M.J. Modulating eating behavior with transcranial direct current stimulation (tDCS): A systematic literature review on the impact of eating behavior traits. Obes. Rev. 2022, 23, e13364. [Google Scholar] [CrossRef] [PubMed]
- Gallop, L.; Flynn, M.; Campbell, I.C.; Schmidt, U. Neuromodulation and Eating Disorders. Curr. Psychiatry Rep. 2022, 24, 61–69. [Google Scholar] [CrossRef]
- Dalton, B.; Bartholdy, S.; Campbell, I.C.; Schmidt, U. Neurostimulation in Clinical and Sub-clinical Eating Disorders: A Systematic Update of the Literature. Curr. Neuropharmacol. 2018, 16, 1174–1192. [Google Scholar] [CrossRef]
- Hall, P.A.; Vincent, C.M.; Burhan, A.M. Non-invasive brain stimulation for food cravings, consumption, and disorders of eating: A review of methods, findings and controversies. Appetite 2018, 124, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Elfetoh, N.A.; Ali, A.M.; Noamany, M. Anodal transcranial direct current stimulation over the dorsolateral prefrontal cortex improves anorexia nervosa: A pilot study. Restor. Neurol. Neurosci. 2014, 32, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Baumann, S.; Mareš, T.; Albrecht, J.; Anders, M.; Vochosková, K.; Hill, M.; Bulant, J.; Yamamotová, A.; Štastný, O.; Novák, T.; et al. Effects of Transcranial Direct Current Stimulation Treatment for Anorexia Nervosa. Front. Psychiatry 2021, 12, 717255. [Google Scholar] [CrossRef]
- Costanzo, F.; Menghini, D.; Maritato, A.; Castiglioni, M.C.; Mereu, A.; Varuzza, C.; Zanna, V.; Vicari, S. New Treatment Perspectives in Adolescents with Anorexia Nervosa: The Efficacy of Non-invasive Brain-Directed Treatment. Front. Behav. Neurosci. 2018, 12, 133. [Google Scholar] [CrossRef] [PubMed]
- Strumila, R.; Thiebaut, S.; Jaussent, I.; Seneque, M.; Attal, J.; Courtet, P.; Guillaume, S. Safety and efficacy of transcranial direct current stimulation (tDCS) in the treatment of Anorexia Nervosa. The open-label STAR study. Brain Stimul. 2019, 12, 1325–1327. [Google Scholar] [CrossRef]
- Rząd, Z.; Szewczyk, P.; Rog, J.; Karakula-Juchnowicz, H. Efficiency of Transcranial Direct Current Stimulation (tDCS) in Anorexia Nervosa Treatment-Case Report. Curr. Probl. Psychiatry 2022, 23, 111–117. [Google Scholar] [CrossRef]
- Thair, H.; Holloway, A.L.; Newport, R.; Smith, A.D. Transcranial Direct Current Stimulation (tDCS): A Beginner’s Guide for Design and Implementation. Front. Neurosci. 2017, 11, 641. [Google Scholar] [CrossRef]
- Grunwald, M.; Weiss, T.; Assmann, B.; Ettrich, C. Stable asymmetric interhemispheric theta power in patients with anorexia nervosa during haptic perception even after weight gain: A longitudinal study. J. Clin. Exp. Neuropsychol. 2004, 26, 608–620. [Google Scholar] [CrossRef] [PubMed]
- Galusca, B.; Costes, N.; Zito, N.G.; Peyron, R.; Bossu, C.; Lang, F.; Estour, B. Organic background of restrictive-type anorexia nervosa suggested by increased serotonin1A receptor binding in right frontotemporal cortex of both lean and recovered patients:18F. MPPF PET scan study. Biol. Psychiatry 2008, 64, 1009–1013. [Google Scholar] [CrossRef]
- Pellón Mendoza, A.R.; Castaño Castaño, S. Application of Direct Transcranial Current as Non-Invasive Therapy in Eating Disorders: An Intervention Proposal. MLS Psychol. Res. 2020, 3, 79–98. [Google Scholar] [CrossRef]
- Taghva, A.; Corrigan, J.D.; Rezai, A.R. Obesity and brain addiction circuitry: Implications for deep brain stimulation. Neurosurgery 2012, 71, 224–238. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Wierenga, C.E.; Bailer, U.F.; Simmons, A.N.; Wagner, A.; Bischoff-Grethe, A. Does a shared neurobiology for foods and drugs of abuse contribute to extremes of food ingestion in anorexia and bulimia nervosa? Biol. Psychiatry 2013, 73, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Aizenstein, H.; Venkatraman, V.K.; Fudge, J.; May, J.C.; Mazurkewicz, L.; Carter, C. Altered reward processing in women recovered from anorexia nervosa. Am. J. Psychiatry 2007, 164, 1842–1849. [Google Scholar] [CrossRef]
- Tanaka, T.; Takano, Y.; Tanaka, S.; Hironaka, N.; Kobayashi, K.; Hanakawa, T.; Watanabe, K.; Honda, M. Transcranial direct-current stimulation increasesextracellular dopamine levels in the rat striatum. Front. Syst. Neurosci. 2013, 7, 6. [Google Scholar] [CrossRef]
- Fonteneau, C.; Redoute, J.; Haesebaert, F.; Le Bars, D.; Costes, N.; Suaud-Chagny, M.F.; Brunelin, J. Frontal Transcranial Direct Current Stimulation Induces Dopamine Release in the Ventral Striatum in Human. Cereb. Cortex 2018, 28, 2636–2646. [Google Scholar] [CrossRef]
- Casper, R.C. The “drive for activity” and “restlessness” in anorexia nervosa: Potential pathways. J. Affect. Disord. 2006, 92, 99–107. [Google Scholar] [CrossRef]
- Alcaro, A.; Huber, R.; Panksepp, J. Behavioral functions of the mesolimbic dopaminergic system: An affective neuroethological perspective. Brain Res. Rev. 2007, 56, 283–321. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Hasan, A.; Strube, W.; Padberg, F. tDCS for the treatment of depression: A comprehensive review. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 681–694. [Google Scholar] [CrossRef]
- Woodham, R.; Rimmer, R.M.; Mutz, J.; Fu, C.H.Y. Is tDCS a potential first line treatment for major depression? Int. Rev. Psychiatry 2021, 33, 250–265. [Google Scholar] [CrossRef] [PubMed]
- Pizzagalli, D.A.; Roberts, A.C. Prefrontal cortex and depression. Neuropsychopharmacology 2022, 47, 225–246. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.P.; Siemer, M.; Gotlib, I.H. Amygdala volume in major depressive disorder: A meta-analysis of magnetic resonance imaging studies. Mol. Psychiatry 2008, 13, 993–1000. [Google Scholar] [CrossRef]
- Sheline, Y.I. Depression and the hippocampus: Cause or effect? Biol. Psychiatry 2011, 70, 308–309. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Ferrucci, R.; Fregni, F.; Boggio, P.S.; Priori, A. Transcranial direct current stimulation for the treatment of major depressive disorder: A summary of preclinical, clinical and translational findings. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2012, 39, 9–16. [Google Scholar] [CrossRef]
- Fukai, M.; Bunai, T.; Hirosawa, T.; Kikuchi, M.; Ito, S.; Minabe, Y.; Ouchi, Y. Endogenous dopamine release under transcranial direct-current stimulation governs enhanced attention: A study with positron emission tomography. Transl. Psychiatry 2019, 9, 115. [Google Scholar] [CrossRef]
- Bunai, T.; Hirosawa, T.; Kikuchi, M.; Fukai, M.; Yokokura, M.; Ito, S.; Takata, Y.; Terada, T.; Ouchi, Y. tDCS-induced modulation of GABA concentration and dopamine release in the human brain: A combination study of magnetic resonance spectroscopy and positron emission tomography. Brain Stimul. 2021, 14, 154–160. [Google Scholar] [CrossRef]
- Dunlop, B.W.; Nemeroff, C.B. The role of dopamine in the pathophysiology of depression. Arch. Gen. Psychiatry 2007, 64, 327–337. [Google Scholar] [CrossRef]
- Belujon, P.; Grace, A.A. Dopamine System Dysregulation in Major Depressive Disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Delva, N.C.; Stanwood, G.D. Dysregulation of brain dopamine systems in major depressive disorder. Exp. Biol. Med. 2021, 246, 1084–1093. [Google Scholar] [CrossRef]
- Maslen, H.; Pugh, J.; Savulescu, J. The ethics of deep brain stimulation for the treatment of anorexia nervosa. Neuroethics 2015, 8, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Koivuniemi, A.; Otto, K. When “altering brain function” becomes “mind control”. Front. Syst. Neurosci. 2014, 8, 202. [Google Scholar] [CrossRef] [PubMed]
- Normann, C.; Schmitz, D.; Fürmaier, A.; Döing, C.; Bach, M. Long-term plasticity of visually evoked potentials in humans is altered in major depression. Biol. Psychiatry 2007, 62, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Kuo, M.F.; Ralf Karrasch, R.; Wächter, B.; Liebetanz, D.; Paulus, W. Serotonin affects transcranial direct current-induced neuroplasticity in humans. Biol. Psychiatry 2009, 66, 503–508. [Google Scholar] [CrossRef]
- Monte-Silva, K.; Kuo, M.F.; Thirugnanasambandam, N.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Dose-dependent inverted U-shaped effect of dopamine (D2-like) receptor activation on focal and nonfocal plasticity in humans. J. Neurosci. 2009, 29, 6124–6131. [Google Scholar] [CrossRef]
- Tuplin, E.W.; Holahan, M.R. Aripiprazole, A Drug that Displays Partial Agonism and Functional Selectivity. Curr. Neuropharmacol. 2017, 15, 1192–1207. [Google Scholar] [CrossRef]
- Hamamura, T.; Harada, T. Unique pharmacological profile of aripiprazole as the phasic component buster. Psychopharmacology 2007, 191, 741–743. [Google Scholar] [CrossRef]
- Blanchet, C.; Guillaume, S.; Bat-Pitault, F.; Carles, M.E.; Clarke, J.; Dodin, V.; Duriez, P.; Gerardin, P.; Hanachi-Guidoum, M.; Iceta, S.; et al. Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews. J. Clin. Med. 2019, 8, 278. [Google Scholar] [CrossRef]
- Burton, C.Z.; Garnett, E.O.; Capellari, E.; Chang, S.E.; Tso, I.F.; Hampstead, B.M.; Taylor, S.F. Combined Cognitive Training and Transcranial Direct Current Stimulation in Neuropsychiatric Disorders: A Systematic Review and Meta-analysis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2023, 8, 151–161. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author, Citation | Population | Technical Specifications | Outcome Measurment | Main Results (Primary Outcomes Are Bolded) |
|---|---|---|---|---|
| Khedr et al. [67] | 7 patients with AN (n = 7). | Anodal tDCS (2 mA) over the left dorsolateral prefrontal cortex (DLPFC) for 10 consecutive days (5 session/week), anodal tDCS for 25 min. | Eating Attitude Test (EAT), Eating Disorder Inventory (EDI) and Beck Depression Inventory (BDI). Pre-tDCS, post-tDCS, and one month later. | 3 patients improved in all three rating scales post tDCS and after 1 month; 1 patient improved only in the BDI; 2 patients showed improvement at the end of session but returned to the baseline after one month. The 7th patient had no changes. |
| Baumann et al. [68] | 43 inpatients with AN, active (n = 22) or sham (n = 21) tDCS. | 2 mA anodal stimulation over the left DLPFC with the cathode over the right orbitofrontal region, 10–30 min sessions. | Eating Disorder Examination Questionnaire (EDE-Q), Zung Self-Rating Depression Scale (ZUNG), BMI; pre-tDCS, post-tDCS, and one month later. | No significant effect on complex psychopathology and weight recovery in patients with AN. |
| Costanzo et al. [69] | 23 adolescents with AN, tDCS + therapy as usual (tDCS + (AU) n = 11) or a family-based therapy (FBT + AU n = 12). | 1 mA, anodal electrode positioned over the left DLPFC and cathodal electrode over the right DLPFC; 20 min, 3 times a week for 6 weeks. | EDI-3, Bulimia (B), Global Psychological Maladjustment (GPM), Interpersonal Problems, BMI. Pre-, post-, one month, and 6 weeks after tDCS. | After 4 and 6 weeks, BMI increased in the tDCS group; in this group, a medium negative correlation was found between improvements in BMI, B and GPM. |
| Strumila et al. [70] | 9 female patients with AN (n = 9). | Anodal 2 mA stimulation, anode on the left DLPFC, and cathode on the right DLPFC, 2 times per day for 25 min, 2 weeks. | Eating Disorder Inventory (EDI), Eating Disorder Examination Questionnaire (EDE-Q), Body Shape Questionnaire (BSQ-34), Beck Depression Inventory (BDI). Pre-, post-, and one month after tDCS. | Depression symptoms significantly decreased post and after 1 month. EDI decreased significantly post and 1 month after stimulation, EDE-Q questionnaire at 1 month was significantly lower. |
| Rząd et al. [71] | 1 patient with AN (n = 1). | Anodal 2 mA stimulation, anode on the left DLPFC, and cathode on the right DLPFC, twice daily for 25 min for 2 weeks. | Fasting venous blood; Eating Attitudes Test, Rosenberg Self-Esteem scale, BDI, EDE-Q, Body Esteem Scale, Perceived Stress Scale. Pre-, post-, and 2 weeks after tDCS. | Improvement in anthropometric measurement, some blood parameters (e.g., ferritin), symptoms of depression and stress, and self-body image after two weeks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chmiel, J.; Gladka, A.; Leszek, J. The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review. Nutrients 2023, 15, 4455. https://doi.org/10.3390/nu15204455
Chmiel J, Gladka A, Leszek J. The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review. Nutrients. 2023; 15(20):4455. https://doi.org/10.3390/nu15204455
Chicago/Turabian StyleChmiel, James, Anna Gladka, and Jerzy Leszek. 2023. "The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review" Nutrients 15, no. 20: 4455. https://doi.org/10.3390/nu15204455
APA StyleChmiel, J., Gladka, A., & Leszek, J. (2023). The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review. Nutrients, 15(20), 4455. https://doi.org/10.3390/nu15204455