

Diet Quality and Consumption of Healthy and Unhealthy Foods Measured via the Global Diet Quality Score in Relation to Cardiometabolic Outcomes in Apparently Healthy Adults from the Mediterranean Region: The ATTICA Epidemiological Cohort Study (2002–2022)




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
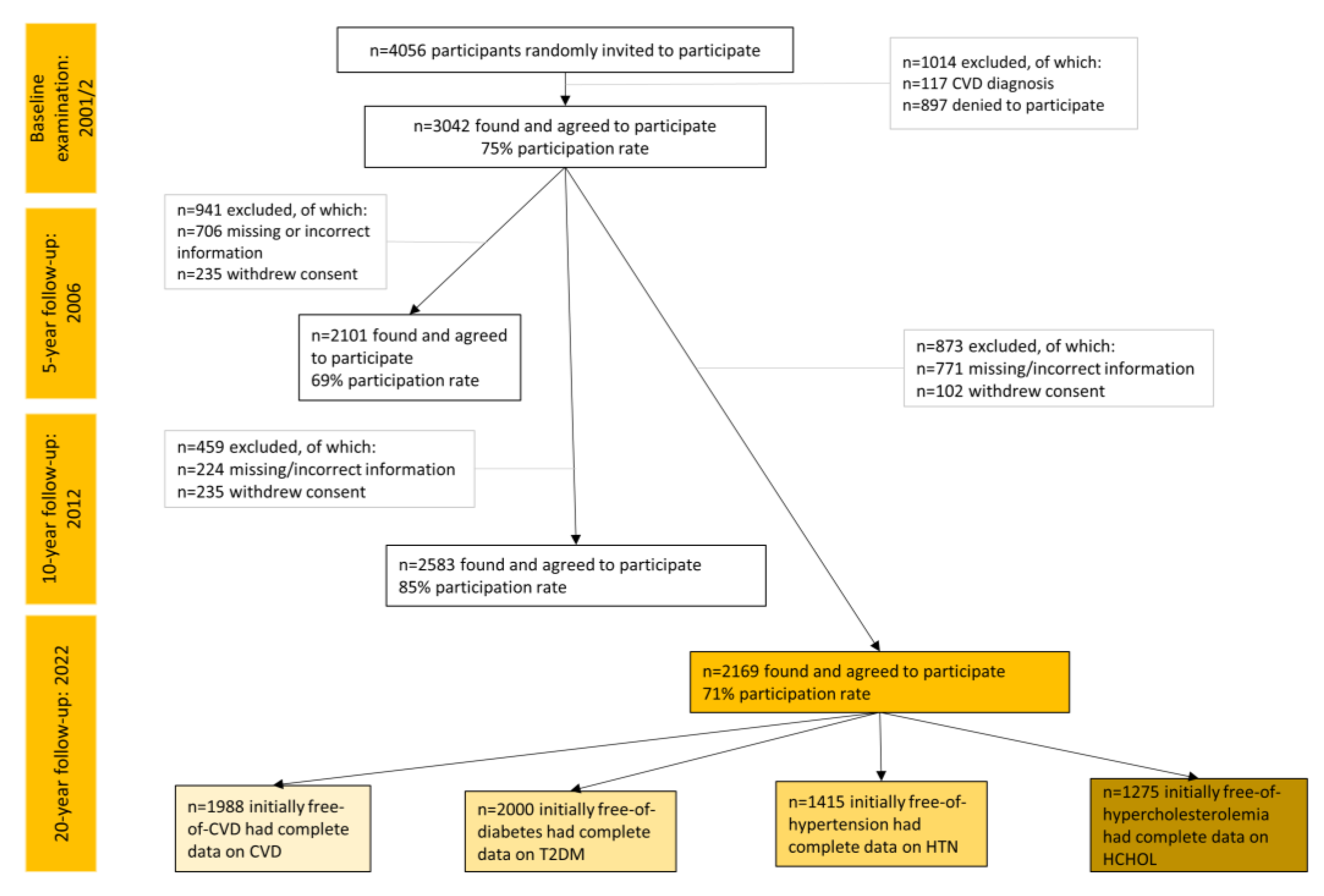
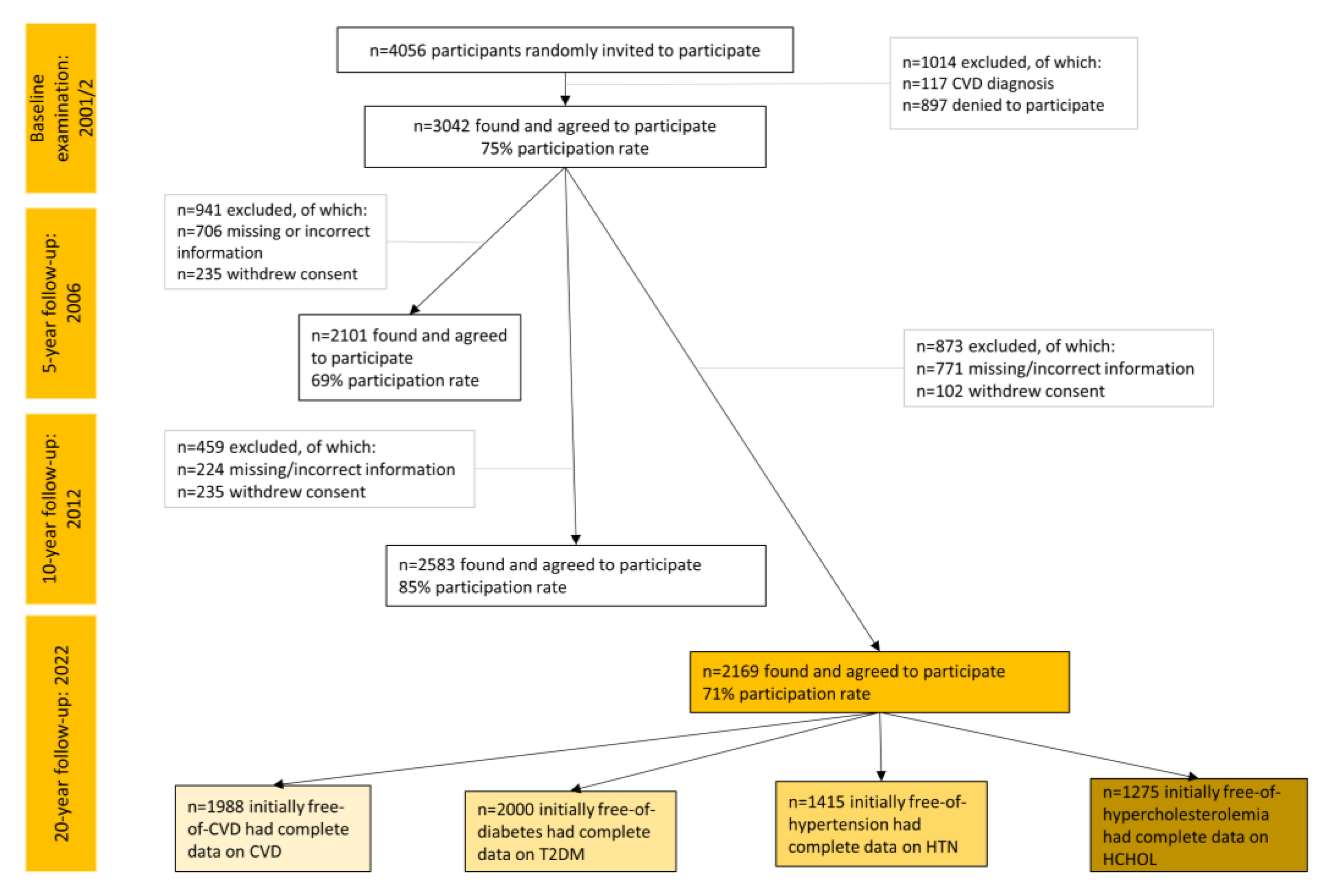
2.2. Setting and Participants
2.3. Variables and Measurements at Baseline Examination
2.3.1. Sociodemographic Parameters
2.3.2. Clinical, Biochemical, and Anthropometric Parameters
2.3.3. Lifestyle Habits
2.3.4. Dietary Habits
2.4. Variables and Measurements at Follow-Up Examinations
2.5. Sample Size
2.6. Statistical Analysis
3. Results
3.1. Baseline Sample Characteristics
3.2. Baseline Diet Quality Measured by GDQS and Its Submetrics in Relation to Long-Term Trajectories of Mediterranean Diet Adherence
3.3. Incidence of Cardiometabolic Outcomes by GDQS Tertiles
3.4. Diet Quality and Incidence of Cardiometabolic Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willett, W.C.; Stampfer, M.J. Current Evidence on Healthy Eating. Annu. Rev. Public Health 2013, 34, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Martínez-González, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food Based Dietary Patterns and Chronic Disease Prevention. BMJ 2018, 361, k2396. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Shulkin, M.L.; Peñalvo, J.L.; Khatibzadeh, S.; Singh, G.M.; Rao, M.; Fahimi, S.; Powles, J.; Mozaffarian, D. Etiologic Effects and Optimal Intakes of Foods and Nutrients for Risk of Cardiovascular Diseases and Diabetes: Systematic Reviews and Meta-Analyses from the Nutrition and Chronic Diseases Expert Group (NutriCoDE). PLoS ONE 2017, 12, e0175149. [Google Scholar] [CrossRef]
- GBD 2017 Diet Collaborators. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.; Diamond, J.; Vieco, A.; Chaudhuri, S.; Shinnar, E.; Cromer, S.; Perel, P.; Mensah, G.A.; Narula, J.; Johnson, C.O.; et al. Global Atlas of Cardiovascular Disease 2000-2016: The Path to Prevention and Control. Glob. Heart 2018, 13, 143–163. [Google Scholar] [CrossRef] [PubMed]
- Global Cardiovascular Risk Consortium; Magnussen, C.; Ojeda, F.M.; Leong, D.P.; Alegre-Diaz, J.; Amouyel, P.; Aviles-Santa, L.; De Bacquer, D.; Ballantyne, C.M.; Bernabé-Ortiz, A.; et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N. Engl. J. Med. 2023, 389, 1273–1285. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J.; et al. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef]
- Song, Y.; Lobene, A.J.; Wang, Y.; Hill Gallant, K.M. The DASH Diet and Cardiometabolic Health and Chronic Kidney Disease: A Narrative Review of the Evidence in East Asian Countries. Nutrients 2021, 13, 984. [Google Scholar] [CrossRef]
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the Double Burden of Malnutrition and the Changing Nutrition Reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Bromage, S.; Batis, C.; Bhupathiraju, S.N.; Fawzi, W.W.; Fung, T.T.; Li, Y.; Deitchler, M.; Angulo, E.; Birk, N.; Castellanos-Gutiérrez, A.; et al. Development and Validation of a Novel Food-Based Global Diet Quality Score (GDQS). J. Nutr. 2021, 151, 75S–92S. [Google Scholar] [CrossRef]
- Bromage, S.; Zhang, Y.; Holmes, M.D.; Sachs, S.E.; Fanzo, J.; Remans, R.; Sachs, J.D.; Batis, C.; Bhupathiraju, S.N.; Fung, T.T.; et al. The Global Diet Quality Score Is Inversely Associated with Nutrient Inadequacy, Low Midupper Arm Circumference, and Anemia in Rural Adults in Ten Sub-Saharan African Countries. J. Nutr. 2021, 151, 119S–129S. [Google Scholar] [CrossRef]
- Moursi, M.; Bromage, S.; Fung, T.T.; Isanaka, S.; Matsuzaki, M.; Batis, C.; Castellanos-Gutiérrez, A.; Angulo, E.; Birk, N.; Bhupathiraju, S.N.; et al. There’s an App for That: Development of an Application to Operationalize the Global Diet Quality Score. J. Nutr. 2021, 151, 176S–184S. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Li, Y.; Bromage, S.; Bhupathiraju, S.N.; Batis, C.; Fawzi, W.; Holmes, M.D.; Stampfer, M.; Hu, F.B.; Deitchler, M.; et al. Higher Global Diet Quality Score Is Associated with Less 4-Year Weight Gain in US Women. J. Nutr. 2021, 151, 162S–167S. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Fang, Y.; Bromage, S.; Fung, T.T.; Bhupathiraju, S.N.; Batis, C.; Deitchler, M.; Fawzi, W.; Stampfer, M.J.; Hu, F.B.; et al. Application of the Global Diet Quality Score in Chinese Adults to Evaluate the Double Burden of Nutrient Inadequacy and Metabolic Syndrome. J. Nutr. 2021, 151, 93S–100S. [Google Scholar] [CrossRef]
- Angulo, E.; Stern, D.; Castellanos-Gutiérrez, A.; Monge, A.; Lajous, M.; Bromage, S.; Fung, T.T.; Li, Y.; Bhupathiraju, S.N.; Deitchler, M.; et al. Changes in the Global Diet Quality Score, Weight, and Waist Circumference in Mexican Women. J. Nutr. 2021, 151, 152S–161S. [Google Scholar] [CrossRef] [PubMed]
- Yaregal, Z.; Baye, K. The Global Diet Quality Score Predicts Diet Quality of Women of Reproductive Age in Addis Ababa, Ethiopia. Br. J. Nutr. 2023, 130, 1573–1579. [Google Scholar] [CrossRef]
- Castellanos-Gutiérrez, A.; Rodríguez-Ramírez, S.; Bromage, S.; Fung, T.T.; Li, Y.; Bhupathiraju, S.N.; Deitchler, M.; Willett, W.; Batis, C. Performance of the Global Diet Quality Score with Nutrition and Health Outcomes in Mexico with 24-h Recall and FFQ Data. J. Nutr. 2021, 151, 143S–151S. [Google Scholar] [CrossRef]
- Birk, N.; Matsuzaki, M.; Fung, T.T.; Li, Y.; Batis, C.; Stampfer, M.J.; Deitchler, M.; Willett, W.C.; Fawzi, W.W.; Bromage, S.; et al. Exploration of Machine Learning and Statistical Techniques in Development of a Low-Cost Screening Method Featuring the Global Diet Quality Score for Detecting Prediabetes in Rural India. J. Nutr. 2021, 151, 110S–118S. [Google Scholar] [CrossRef]
- Cliffer, I.; Darling, A.M.; Madzorera, I.; Wang, D.; Perumal, N.; Wang, M.; Liu, E.; Pembe, A.B.; Urassa, W.; Fawzi, W.W. Associations of Diet Quality, Socioeconomic Factors, and Nutritional Status with Gestational Weight Gain among Pregnant Women in Dar Es Salaam, Tanzania. Curr. Dev. Nutr. 2023, 7, 100041. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Chrysohoou, C.; Stefanadis, C. Epidemiology of Cardiovascular Risk Factors in Greece: Aims, Design and Baseline Characteristics of the ATTICA Study. BMC Public Health 2003, 3, 32. [Google Scholar] [CrossRef] [PubMed]
- Damigou, E.; Kouvari, M.; Chrysohoou, C.; Barkas, F.; Kravvariti, E.; Pitsavos, C.; Skoumas, J.; Michelis, E.; Liberopoulos, E.; Tsioufis, C.; et al. Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022). Life 2023, 13, 1142. [Google Scholar] [CrossRef]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- Katsouyanni, K.; Rimm, E.B.; Gnardellis, C.; Trichopoulos, D.; Polychronopoulos, E.; Trichopoulou, A. Reproducibility and Relative Validity of an Extensive Semi-Quantitative Food Frequency Questionnaire Using Dietary Records and Biochemical Markers among Greek Schoolteachers. Int. J. Epidemiol. 1997, 26, S118. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and Vegetable Intake and the Risk of Cardiovascular Disease, Total Cancer and All-Cause Mortality-a Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wu, X.; Zhuang, W.; Xia, L.; Chen, Y.; Wang, Y.; Wu, C.; Rao, Z.; Du, L.; Zhao, R.; et al. Green Leafy Vegetable and Lutein Intake and Multiple Health Outcomes. Food Chem. 2021, 360, 130145. [Google Scholar] [CrossRef] [PubMed]
- Alissa, E.M.; Ferns, G.A. Dietary Fruits and Vegetables and Cardiovascular Diseases Risk. Crit. Rev. Food Sci. Nutr. 2017, 57, 1950–1962. [Google Scholar] [CrossRef]
- Slavin, J.L.; Lloyd, B. Health Benefits of Fruits and Vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef]
- De Souza, R.G.M.; Schincaglia, R.M.; Pimentel, G.D.; Mota, J.F. Nuts and Human Health Outcomes: A Systematic Review. Nutrients 2017, 9, 1311. [Google Scholar] [CrossRef] [PubMed]
- Casas-Agustench, P.; Bulló, M.; Salas-Salvadó, J. Nuts, Inflammation and Insulin Resistance. Asia Pac. J. Clin. Nutr. 2010, 19, 124–130. [Google Scholar] [PubMed]
- Jiang, L.; Wang, J.; Xiong, K.; Xu, L.; Zhang, B.; Ma, A. Intake of Fish and Marine N-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 2342. [Google Scholar] [CrossRef]
- Chen, G.-C.; Koh, W.-P.; Yuan, J.-M.; Qin, L.-Q.; van Dam, R.M. Green Leafy and Cruciferous Vegetable Consumption and Risk of Type 2 Diabetes: Results from the Singapore Chinese Health Study and Meta-Analysis. Br. J. Nutr. 2018, 119, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.J.; Mori, T.A. Dietary Patterns, Dietary Nutrients and Cardiovascular Disease. Rev. Cardiovasc. Med. 2022, 23, 17. [Google Scholar] [CrossRef]
- Chen, G.-C.; Chai, J.C.; Xing, J.; Moon, J.-Y.; Shan, Z.; Yu, B.; Mossavar-Rahman, Y.; Sotres-Alvarez, D.; Li, J.; Mattei, J.; et al. Healthful Eating Patterns, Serum Metabolite Profile and Risk of Diabetes in a Population-Based Prospective Study of US Hispanics/Latinos. Diabetologia 2022, 65, 1133–1144. [Google Scholar] [CrossRef]
- Chen, G.-C.; Koh, W.-P.; Neelakantan, N.; Yuan, J.-M.; Qin, L.-Q.; van Dam, R.M. Diet Quality Indices and Risk of Type 2 Diabetes Mellitus: The Singapore Chinese Health Study. Am. J. Epidemiol. 2018, 187, 2651–2661. [Google Scholar] [CrossRef]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- Chen, X.; Chu, J.; Hu, W.; Sun, N.; He, Q.; Liu, S.; Feng, Z.; Li, T.; Han, Q.; Shen, Y. Associations of Ultra-Processed Food Consumption with Cardiovascular Disease and All-Cause Mortality: UK Biobank. Eur. J. Public Health 2022, 32, 779–785. [Google Scholar] [CrossRef]
- Kieneker, L.M.; Eisenga, M.F.; Gansevoort, R.T.; de Boer, R.A.; Navis, G.; Dullaart, R.P.F.; Joosten, M.M.; Bakker, S.J.L. Association of Low Urinary Sodium Excretion With Increased Risk of Stroke. Mayo Clin. Proc. 2018, 93, 1803–1809. [Google Scholar] [CrossRef]
- Stolarz-Skrzypek, K.; Kuznetsova, T.; Thijs, L.; Tikhonoff, V.; Seidlerová, J.; Richart, T.; Jin, Y.; Olszanecka, A.; Malyutina, S.; Casiglia, E.; et al. Fatal and Nonfatal Outcomes, Incidence of Hypertension, and Blood Pressure Changes in Relation to Urinary Sodium Excretion. JAMA 2011, 305, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Tsirimiagkou, C.; Karatzi, K.; Argyris, A.; Chalkidou, F.; Tzelefa, V.; Sfikakis, P.P.; Yannakoulia, M.; Protogerou, A.D. Levels of Dietary Sodium Intake: Diverging Associations with Arterial Stiffness and Atheromatosis. Hell. J. Cardiol. 2021, 62, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Argyris, A.; Tsirimiagkou, C.; Karatzi, K.; Ntouska, K.; Sfikakis, P.; Protogerou, A. Dietary Sugars and Subclinical Vascular Damage. Atherosclerosis 2021, 331, e53. [Google Scholar] [CrossRef]
- Neelakantan, N.; Park, S.H.; Chen, G.-C.; van Dam, R.M. Sugar-Sweetened Beverage Consumption, Weight Gain, and Risk of Type 2 Diabetes and Cardiovascular Diseases in Asia: A Systematic Review. Nutr. Rev. 2021, 80, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Damigou, E.; Kosti, R.I.; Panagiotakos, D.B. White Meat Consumption and Cardiometabolic Risk Factors: A Review of Recent Prospective Cohort Studies. Nutrients 2022, 14, 5213. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dairy Foods, Obesity, and Metabolic Health: The Role of the Food Matrix Compared with Single Nutrients. Adv. Nutr. 2019, 10, 917S–923S. [Google Scholar] [CrossRef]
- Bhupathi, V.; Mazariegos, M.; Cruz Rodriguez, J.B.; Deoker, A. Dairy Intake and Risk of Cardiovascular Disease. Curr. Cardiol. Rep. 2020, 22, 11. [Google Scholar] [CrossRef]
- Kouvari, M.; Damigou, E.; Florentin, M.; Kosti, R.I.; Chrysohoou, C.; Pitsavos, C.S.; Panagiotakos, D.B. Egg Consumption, Cardiovascular Disease and Cardiometabolic Risk Factors: The Interaction with Saturated Fatty Acids. Results from the ATTICA Cohort Study (2002–2012). Nutrients 2022, 14, 5291. [Google Scholar] [CrossRef]
- Mathieu, J. What Should You Know about Mindful and Intuitive Eating? J. Am. Diet. Assoc. 2009, 109, 1982–1987. [Google Scholar] [CrossRef]
- Warren, J.M.; Smith, N.; Ashwell, M. A Structured Literature Review on the Role of Mindfulness, Mindful Eating and Intuitive Eating in Changing Eating Behaviours: Effectiveness and Associated Potential Mechanisms. Nutr. Res. Rev. 2017, 30, 272–283. [Google Scholar] [CrossRef]
- Van Dyke, N.; Drinkwater, E.J. Relationships between Intuitive Eating and Health Indicators: Literature Review. Public Health Nutr. 2014, 17, 1757–1766. [Google Scholar] [CrossRef]
- Katcher, J.A.; Suminski, R.R.; Pacanowski, C.R. Impact of an Intuitive Eating Intervention on Disordered Eating Risk Factors in Female-Identifying Undergraduates: A Randomized Waitlist-Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 12049. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.K.; Kristeller, J.L.; Headings, A.; Nagaraja, H.; Miser, W.F. Comparative Effectiveness of a Mindful Eating Intervention to a Diabetes Self-Management Intervention among Adults with Type 2 Diabetes: A Pilot Study. J. Acad. Nutr. Diet. 2012, 112, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.B. Mindful Eating: The Art of Presence While You Eat. Diabetes Spectr. 2017, 30, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Webster, P. Canada’s Updated Food Guide Promotes Mindful Eating. Lancet 2019, 393, e5. [Google Scholar] [CrossRef] [PubMed]
- Tapper, K. Mindful Eating: What We Know so Far. Nutr. Bull. 2022, 47, 168–185. [Google Scholar] [CrossRef] [PubMed]
- Canada, H. Canada’s Dietary Guidelines. Available online: https://food-guide.canada.ca/en/guidelines/ (accessed on 6 July 2023).
- Pfinder, M.; Heise, T.L.; Hilton Boon, M.; Pega, F.; Fenton, C.; Griebler, U.; Gartlehner, G.; Sommer, I.; Katikireddi, S.V.; Lhachimi, S.K. Taxation of Unprocessed Sugar or Sugar-Added Foods for Reducing Their Consumption and Preventing Obesity or Other Adverse Health Outcomes. Cochrane Database Syst. Rev. 2020, 4, CD012333. [Google Scholar] [CrossRef] [PubMed]
- Smed, S.; Scarborough, P.; Rayner, M.; Jensen, J.D. The Effects of the Danish Saturated Fat Tax on Food and Nutrient Intake and Modelled Health Outcomes: An Econometric and Comparative Risk Assessment Evaluation. Eur. J. Clin. Nutr. 2016, 70, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Lhachimi, S.K.; Pega, F.; Heise, T.L.; Fenton, C.; Gartlehner, G.; Griebler, U.; Sommer, I.; Bombana, M.; Katikireddi, S.V. Taxation of the Fat Content of Foods for Reducing Their Consumption and Preventing Obesity or Other Adverse Health Outcomes. Cochrane Database Syst. Rev. 2020, 9, CD012415. [Google Scholar] [CrossRef]
- Jensen, J.D.; Smed, S. State-of-the-Art for Food Taxes to Promote Public Health. Proc. Nutr. Soc. 2018, 77, 100–105. [Google Scholar] [CrossRef]
- Wright, A.; Smith, K.E.; Hellowell, M. Policy Lessons from Health Taxes: A Systematic Review of Empirical Studies. BMC Public Health 2017, 17, 583. [Google Scholar] [CrossRef] [PubMed]
- Food Is Medicine Initiative. Available online: https://www.heart.org/en/professional/food-is-medicine-initiative (accessed on 8 October 2023).
- Food Is Medicine. The Rockefeller Foundation. Available online: https://www.rockefellerfoundation.org/initiative/food-is-medicine/ (accessed on 8 October 2023).

{kind=link}
| GDQS | Food Group | Median | Interquartile Range |
|---|---|---|---|
| GDQS+ | Healthy | ||
| Citrus fruits | 90 | 45 | |
| Deep orange fruits | 86 | 46 | |
| Other fruits | 130 | 50 | |
| Dark green leafy vegetables | 129 | 50 | |
| Cruciferous vegetables | 108 | 25 | |
| Deep orange vegetables | 88 | 18 | |
| Other vegetables | 138 | 50 | |
| Legumes | 50 | 25 | |
| Deep orange tubers | 36 | 5 | |
| Nuts and seeds | 4 | 2 | |
| Whole grains | 5 | 10 | |
| Liquid oils | 60 | 5 | |
| Fish and shellfish | 21 | 21 | |
| Poultry and game meat | 39 | 19 | |
| Low-fat dairy | 29 | 100 | |
| Eggs | 17 | 9 | |
| GDQS− | Unhealthy in excessive amounts | ||
| High-fat dairy | 30 | 230 | |
| Red meat | 34 | 17 | |
| Unhealthy | |||
| Processed meat | 4 | 6 | |
| Refined grains and baked goods | 55 | 10 | |
| Sweets and ice cream | 12 | 37 | |
| Sugar-sweetened beverages | 94 | 141 | |
| Juice | 143 | 86 | |
| White roots and tubers | 34 | 17 | |
| Purchased deep fried foods | 26 | 13 |
| Baseline Characteristics | Global Diet Quality Score (GDQS) Tertiles | |||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Value | |
| N | 804 | 969 | 396 | - |
| Sociodemographic factors | ||||
| Age, years | 50 (14) | 43 (11) | 40 (17) | <0.001 |
| Men, % | 58 | 48 | 38 | <0.001 |
| Education, years in school | 12 (7) | 12 (4) | 12 (4) | 0.004 |
| Clinical factors | ||||
| History of hypercholesterolemia, % | 45 | 41 | 26 | <0.001 |
| History of hypertension, % | 40 | 25 | 24 | <0.001 |
| History of diabetes mellitus, % | 12 | 4 | 6 | <0.001 |
| Family history of cardiovascular disease, % | 37 | 35 | 36 | 0.309 |
| Anthropometric factors | ||||
| Body mass index, kg/m2 | 28 (4.6) | 26 (3.2) | 26 (6.4) | <0.001 |
| Waist circumference, cm | 94 (15) | 88 (13) | 86 (19) | <0.001 |
| Lifestyle factors | ||||
| MedDietScore, range 0–55 | 25 (12) | 27 (1.7) | 29 (6.2) | <0.001 |
| Global Diet Quality Score, 0–49 | 19 (12) | 37 (0) | 42 (10) | <0.001 |
| Global Diet Quality Score+, 0–32 | 11 (10) | 31 (0) | 31 (1) | <0.001 |
| Global Diet Quality Score−, 0–17 | 6 (2) | 6 (0) | 10 (11) | <0.001 |
| Physical activity, %yes | 34 | 34 | 39 | 0.137 |
| Smoking habits, % | ||||
| Never smoked (2002–2012) | 40 | 37 | 39 | 0.002 |
| Started smoking during follow-up (2012) | 22 | 17 | 23 | |
| Stopped smoking during follow-up (2012) | 17 | 23 | 19 | |
| Always smoked (2002–2012) | 21 | 23 | 20 | |
| Pack-years of cigarette smoking | 450 (608) | 340 (456) | 278 (520) | <0.001 |
| Mediterranean Diet Trajectories | p-Value | ||||
|---|---|---|---|---|---|
| Always Away (2002–2012) from the Mediterranean Diet | From Away (2002) to Close (2012) to the Mediterranean Diet | From Close (2002) to Away (2012) from the Mediterranean Diet | Always Close (2002–2012) to the Mediterranean Diet | ||
| Global Diet Quality Score, 0–49 | 27 (14) | 30 (13) * | 33 (8.5) * | 35 (7) * | <0.001 |
| Global Diet Quality Score+, 0–32 | 20 (12) | 20 (11) | 27 (8) * | 28 (7) * | <0.001 |
| Global Diet Quality Score-, 0–17 | 8 (5.6) | 11 (5.6) * | 6 (1.4) * | 6 (1.1) * | <0.001 |
| 20-Year Endpoint, % | Global Diet Quality Score Tertiles | p-Value | ||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | ||
| Fatal/nonfatal cardiovascular disease event | 61 | 22 * | 21 * | <0.001 |
| Hypercholesterolemia | 80 | 73 * | 59 *, ** | <0.001 |
| Hypertension | 62 | 43 * | 35 *, ** | <0.001 |
| Diabetes mellitus | 38 | 26 * | 25 * | <0.001 |
| CVD | Hypertension | Hypercholesterolemia | Type 2 Diabetes Mellitus | ||
|---|---|---|---|---|---|
| N (total), n (new cases) | 1988, 718 | 1415, 314 | 1275, 694 | 2000, 526 | |
| HR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | Models adjusted for | |
| GDQS, per 1/49 | 0.93 (0.92, 0.94) | 0.99 (0.98, 1.00) | 0.99 (0.98, 1.00) | 0.98 (0.97, 0.99) | Model 1: Age, sex |
| GDQS+, per 1/32 | 0.92 (0.90, 0.93) | 0.99 (0.98, 1.00) | 0.98 (0.98, 1.01) | 0.98 (0.97, 0.99) | |
| GDQS−, per 1/17 | 1.01 (0.96, 1.05) | 1.02 (0.99, 1.05) | 0.99 (0.95, 1.02) | 1.00 (0.97, 1.03) | |
| GDQS Tertiles | |||||
| Tertile 1 | Ref | Ref | Ref | Ref | |
| Tertile 2 | 0.24 (0.17, 0.33) | 0.72 (0.58, 0.89) | 1.01 (0.79, 1.28) | 0.74 (0.59, 0.93) | |
| Tertile 3 | 0.39 (0.23, 0.67) | 0.83 (0.61, 1.13) | 0.82 (0.60, 1.13) | 0.79 (0.57, 1.11) | |
| GDQS, per 1/49 | 0.92 (0.91, 0.94) | 0.99 (0.98, 1.00) | 0.99 (0.98, 1.00) | 0.98 (0.97, 0.99) | Model 2: Model 1 plus body mass index, physical activity, smoking habits (2002–2012), and MedDietScore |
| GDQS+, per 1/32 | 0.91 (0.90, 0.93) | 0.99 (0.98, 1.00) | 0.99 (0.98, 1.01) | 0.98 (0.97, 0.99) | |
| GDQS−, per 1/17 | 1.01 (0.96, 1.06) | 0.99 (0.96, 1.02) | 0.98 (0.94, 1.01) | 1.00 (0.97, 1.03) | |
| GDQS Tertiles | |||||
| Tertile 1 | Ref | Ref | Ref | Ref | |
| Tertile 2 | 0.23 (0.16, 0.33) | 0.82 (0.66, 1.03) | 1.02 (0.79, 1.31) | 0.74 (0.59, 0.93) | |
| Tertile 3 | 0.31 (0.16, 0.59) | 0.87 (0.60, 1.24) | 0.84 (0.59, 1.19) | 0.79 (0.57, 1.11) | |
| GDQS, per 1/49 | 0.92 (0.91, 0.94) | 0.99 (0.98, 1.00) | 0.99 (0.98, 1.00) | 0.98 (0.97, 0.99) | Model 3: Model 2 plus history of (hypertension, hypercholesterolemia, and diabetes mellitus), family history of CVD, and education status |
| GDQS+, per 1/32 | 0.91 (0.89, 0.93) | 0.99 (0.98, 1.00) | 0.99 (0.98, 1.01) | 0.98 (0.97, 0.99) | |
| GDQS−, per 1/17 | 1.02 (0.96, 1.07) | 0.99 (0.95, 1.03) | 0.98 (0.94, 1.02) | 1.00 (0.97, 1.04) | |
| GDQS Tertiles | |||||
| Tertile 1 | Ref | Ref | Ref | Ref | |
| Tertile 2 | 0.22 (0.14, 0.34) | 0.77 (0.56, 1.12) | 0.96 (0.74, 1.31) | 0.78 (0.60, 1.03) | |
| Tertile 3 | 0.35 (0.17, 0.73) | 0.72 (0.42, 1.26) | 0.84 (0.59, 1.32) | 0.78 (0.53, 1.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damigou, E.; Kouvari, M.; Chrysohoou, C.; Barkas, F.; Kravvariti, E.; Dalmyras, D.; Koutsogianni, A.D.; Tsioufis, C.; Pitsavos, C.; Liberopoulos, E.; et al. Diet Quality and Consumption of Healthy and Unhealthy Foods Measured via the Global Diet Quality Score in Relation to Cardiometabolic Outcomes in Apparently Healthy Adults from the Mediterranean Region: The ATTICA Epidemiological Cohort Study (2002–2022). Nutrients 2023, 15, 4428. https://doi.org/10.3390/nu15204428
Damigou E, Kouvari M, Chrysohoou C, Barkas F, Kravvariti E, Dalmyras D, Koutsogianni AD, Tsioufis C, Pitsavos C, Liberopoulos E, et al. Diet Quality and Consumption of Healthy and Unhealthy Foods Measured via the Global Diet Quality Score in Relation to Cardiometabolic Outcomes in Apparently Healthy Adults from the Mediterranean Region: The ATTICA Epidemiological Cohort Study (2002–2022). Nutrients. 2023; 15(20):4428. https://doi.org/10.3390/nu15204428
Chicago/Turabian StyleDamigou, Evangelia, Matina Kouvari, Christina Chrysohoou, Fotios Barkas, Evrydiki Kravvariti, Dimitrios Dalmyras, Amalia D. Koutsogianni, Costas Tsioufis, Christos Pitsavos, Evangelos Liberopoulos, and et al. 2023. "Diet Quality and Consumption of Healthy and Unhealthy Foods Measured via the Global Diet Quality Score in Relation to Cardiometabolic Outcomes in Apparently Healthy Adults from the Mediterranean Region: The ATTICA Epidemiological Cohort Study (2002–2022)" Nutrients 15, no. 20: 4428. https://doi.org/10.3390/nu15204428
APA StyleDamigou, E., Kouvari, M., Chrysohoou, C., Barkas, F., Kravvariti, E., Dalmyras, D., Koutsogianni, A. D., Tsioufis, C., Pitsavos, C., Liberopoulos, E., Sfikakis, P. P., & Panagiotakos, D. (2023). Diet Quality and Consumption of Healthy and Unhealthy Foods Measured via the Global Diet Quality Score in Relation to Cardiometabolic Outcomes in Apparently Healthy Adults from the Mediterranean Region: The ATTICA Epidemiological Cohort Study (2002–2022). Nutrients, 15(20), 4428. https://doi.org/10.3390/nu15204428