
Is the Consumption of Added Sugar from Common Beverages Associated with the Presence of Attention Deficit Hyperactivity Disorder Symptoms in Thai Medical Students?

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Study Determinant
2.4. Study Endpoint
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thapar, A.; Cooper, M. Attention Deficit Hyperactivity Disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef]
- Magnus, W.; Nazir, S.; Anilkumar, A.C.; Shaban, K. Attention Deficit Hyperactivity Disorder. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Howard, A.L.; Strickland, N.J.; Murray, D.W.; Tamm, L.; Swanson, J.M.; Hinshaw, S.P.; Arnold, L.E.; Molina, B.S.G. Progression of Impairment in Adolescents with Attention-Deficit/Hyperactivity Disorder through the Transition out of High School: Contributions of Parent Involvement and College Attendance. J. Abnorm. Psychol. 2016, 125, 233–247. [Google Scholar] [CrossRef]
- Agnew-Blais, J.C.; Polanczyk, G.V.; Danese, A.; Wertz, J.; Moffitt, T.E.; Arseneault, L. Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry 2016, 73, 713–720. [Google Scholar] [CrossRef]
- Rivas-Vazquez, R.A.; Diaz, S.G.; Visser, M.M.; Rivas-Vazquez, A.A. Adult ADHD: Underdiagnosis of a Treatable Condition. J. Health Serv. Psychol. 2023, 49, 11–19. [Google Scholar] [CrossRef]
- Meeks, L.M.; Case, B.; Herzer, K.; Plegue, M.; Swenor, B.K. Change in Prevalence of Disabilities and Accommodation Practices Among US Medical Schools, 2016 vs 2019. JAMA 2019, 322, 2022–2024. [Google Scholar] [CrossRef]
- Karawekpanyawong, N.; Wongpakaran, T.; Wongpakaran, N.; Boonnag, C.; Siritikul, S.; Chalanunt, S.; Kuntawong, P. Impact of Perceived Social Support on the Relationship between ADHD and Depressive Symptoms among First Year Medical Students: A Structural Equation Model Approach. Children 2021, 8, 401. [Google Scholar] [CrossRef]
- Im, D.S.; Tamarelli, C.M. Attention Deficit Hyperactivity Disorder in Medical Learners and Physicians and a Potentially Helpful Educational Tool. Adv. Med. Educ. Pract. 2023, 14, 435–442. [Google Scholar] [CrossRef]
- Fuermaier, A.B.M.; Tucha, L.; Butzbach, M.; Weisbrod, M.; Aschenbrenner, S.; Tucha, O. ADHD at the Workplace: ADHD Symptoms, Diagnostic Status, and Work-Related Functioning. J. Neural Transm. 2021, 128, 1021–1031. [Google Scholar] [CrossRef]
- Sedgwick-Müller, J.A.; Müller-Sedgwick, U.; Adamou, M.; Catani, M.; Champ, R.; Gudjónsson, G.; Hank, D.; Pitts, M.; Young, S.; Asherson, P. University Students with Attention Deficit Hyperactivity Disorder (ADHD): A Consensus Statement from the UK Adult ADHD Network (UKAAN). BMC Psychiatry 2022, 22, 292. [Google Scholar] [CrossRef]
- Agarwal, R.; Goldenberg, M.; Perry, R.; IsHak, W.W. The Quality of Life of Adults with Attention Deficit Hyperactivity Disorder: A Systematic Review. Innov. Clin. Neurosci. 2012, 9, 10–21. [Google Scholar]
- Franke, B.; Faraone, S.V.; Asherson, P.; Buitelaar, J.; Bau, C.H.D.; Ramos-Quiroga, J.A.; Mick, E.; Grevet, E.H.; Johansson, S.; Haavik, J.; et al. The Genetics of Attention Deficit/Hyperactivity Disorder in Adults, a Review. Mol. Psychiatry 2012, 17, 960–987. [Google Scholar] [CrossRef] [PubMed]
- Holton, K.F.; Nigg, J.T. The Association of Lifestyle Factors and ADHD in Children. J. Atten. Disord. 2020, 24, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kondo, M.; Sakai, M.; Takabatake, S.; Furukawa, T.A.; Akechi, T. Association of Autism Spectrum Disorder and Attention Deficit Hyperactivity Disorder Traits with Depression and Empathy Among Medical Students. Adv. Med. Educ. Pract. 2021, 12, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Román, A.; Mitchell, R.; Cortese, S. Sleep in Adults with ADHD: Systematic Review and Meta-Analysis of Subjective and Objective Studies. Neurosci. Biobehav. Rev. 2018, 89, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Del-Ponte, B.; Quinte, G.C.; Cruz, S.; Grellert, M.; Santos, I.S. Dietary Patterns and Attention Deficit/Hyperactivity Disorder (ADHD): A Systematic Review and Meta-Analysis. J. Affect. Disord. 2019, 252, 160–173. [Google Scholar] [CrossRef]
- Farsad-Naeimi, A.; Asjodi, F.; Omidian, M.; Askari, M.; Nouri, M.; Pizarro, A.B.; Daneshzad, E. Sugar Consumption, Sugar Sweetened Beverages and Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2020, 53, 102512. [Google Scholar] [CrossRef]
- Yu, C.-J.; Du, J.-C.; Chiou, H.-C.; Feng, C.-C.; Chung, M.-Y.; Yang, W.; Chen, Y.-S.; Chien, L.-C.; Hwang, B.; Chen, M.-L. Sugar-Sweetened Beverage Consumption Is Adversely Associated with Childhood Attention Deficit/Hyperactivity Disorder. Int. J. Environ. Res. Public Health 2016, 13, 678. [Google Scholar] [CrossRef]
- Anjum, I.; Jaffery, S.S.; Fayyaz, M.; Wajid, A.; Ans, A.H. Sugar Beverages and Dietary Sodas Impact on Brain Health: A Mini Literature Review. Cureus 2018, 10, e2756. [Google Scholar] [CrossRef]
- Schwartz, D.L.; Gilstad-Hayden, K.; Carroll-Scott, A.; Grilo, S.A.; McCaslin, C.; Schwartz, M.; Ickovics, J.R. Energy Drinks and Youth Self-Reported Hyperactivity/Inattention Symptoms. Acad. Pediatr. 2015, 15, 297–304. [Google Scholar] [CrossRef]
- Plumber, N.; Majeed, M.; Ziff, S.; Thomas, S.E.; Bolla, S.R.; Gorantla, V.R. Stimulant Usage by Medical Students for Cognitive Enhancement: A Systematic Review. Cureus 2021, 13, e15163. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Kiatrungrit, K.; Putthisri, S.; Hongsanguansri, S.; Wisajan, P.; Jullagate, S. Validity and Reliability of Adult ADHD Self-Report Scale Thai Version (ASRS-V1.1 TH). Shanghai Arch. Psychiatry 2017, 29, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.E.; Ford, T.; Russell, G. The Relationship between Financial Difficulty and Childhood Symptoms of Attention Deficit/Hyperactivity Disorder: A UK Longitudinal Cohort Study. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Tillman, C.; Granvald, V. The Role of Parental Education in the Relation between ADHD Symptoms and Executive Functions in Children. J. Atten. Disord. 2015, 19, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a Large, Multi-University Sample of College Students: Sleep Problem Prevalence, Sex Differences, and Mental Health Correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- Small, G.W.; Lee, J.; Kaufman, A.; Jalil, J.; Siddarth, P.; Gaddipati, H.; Moody, T.D.; Bookheimer, S.Y. Brain Health Consequences of Digital Technology Use. Dialogues Clin. Neurosci. 2020, 22, 179–187. [Google Scholar] [CrossRef]
- Hongsanun, W.; Kitreerawutiwong, N. Development of a Thai Adolescent Sugar Sweetened Beverage Intake Questionnaire (THASSI). Ph.D. Thesis, Naresuan University, Phitsanuloke, Thailand, 2020. [Google Scholar]
- How Much Sugar Is Too Much? Available online: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/sugar/how-much-sugar-is-too-much (accessed on 10 October 2023).
- Ghanizadeh, A. Agreement between Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, and the Proposed DSM-V Attention Deficit Hyperactivity Disorder Diagnostic Criteria: An Exploratory Study. Compr. Psychiatry 2013, 54, 7–10. [Google Scholar] [CrossRef]
- Kessler, R.C.; Adler, L.; Ames, M.; Demler, O.; Faraone, S.; Hiripi, E.; Howes, M.J.; Jin, R.; Secnik, K.; Spencer, T.; et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): A Short Screening Scale for Use in the General Population. Psychol. Med. 2005, 35, 245–256. [Google Scholar] [CrossRef]
- Hakim Shooshtari, M.; Shariati, B.; Kamalzadeh, L.; Naserbakht, M.; Tayefi, B.; Taban, M. The Prevalence of Attention Deficit Hyperactivity Disorder in Iran: An Updated Systematic Review. Med. J. Islam. Repub. Iran 2021, 35, 8. [Google Scholar] [CrossRef]
- Tuttle, J.P.; Scheurich, N.E.; Ranseen, J. Prevalence of ADHD Diagnosis and Nonmedical Prescription Stimulant Use in Medical Students. Acad. Psychiatry 2010, 34, 220–223. [Google Scholar] [CrossRef]
- Mattos, P.; Nazar, B.P.; Tannock, R. By the Book: ADHD Prevalence in Medical Students Varies with Analogous Methods of Addressing DSM Items. Rev. Bras. Psiquiatr. 2018, 40, 382–387. [Google Scholar] [CrossRef]
- Atwoli, L.; Owiti, P.; Manguro, G.; Ndambuki, D. Attention Deficit Hyperactivity Disorder Symptom Self-Report among Medical Students in Eldoret, Kenya. Afr. J. Psychiatry 2011, 14, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, M.; Lallès, J.-P.; Malbert, C.-H.; Val-Laillet, D. Dietary Sugars: Their Detection by the Gut–Brain Axis and Their Peripheral and Central Effects in Health and Diseases. Eur. J. Nutr. 2015, 54, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Jamar, G.; Ribeiro, D.A.; Pisani, L.P. High-Fat or High-Sugar Diets as Trigger Inflammation in the Microbiota-Gut-Brain Axis. Crit. Rev. Food Sci. Nutr. 2021, 61, 836–854. [Google Scholar] [CrossRef]
- Bonaz, B.; Bazin, T.; Pellissier, S. The Vagus Nerve at the Interface of the Microbiota-Gut-Brain Axis. Front. Neurosci. 2018, 12, 49. [Google Scholar] [CrossRef]
- Shabab, T.; Khanabdali, R.; Moghadamtousi, S.Z.; Kadir, H.A.; Mohan, G. Neuroinflammation Pathways: A General Review. Int. J. Neurosci. 2017, 127, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Anas Sohail, A.; Ortiz, F.; Varghese, T.; Fabara, S.P.; Batth, A.S.; Sandesara, D.P.; Sabir, A.; Khurana, M.; Datta, S.; Patel, U.K. The Cognitive-Enhancing Outcomes of Caffeine and L-Theanine: A Systematic Review. Cureus 2021, 13, e20828. [Google Scholar] [CrossRef]
- Pellow, J.; Solomon, E.M.; Barnard, C.N. Complementary and Alternative Medical Therapies for Children with Attention-Deficit/Hyperactivity Disorder (ADHD). Altern. Med. Rev. J. Clin. Ther. 2011, 16, 323–337. [Google Scholar]
- Konikowska, K.; Regulska-Ilow, B.; Rózańska, D. The Influence of Components of Diet on the Symptoms of ADHD in Children. Rocz. Panstw. Zakl. Hig. 2012, 63, 127–134. [Google Scholar]
- Heilskov Rytter, M.J.; Andersen, L.B.B.; Houmann, T.; Bilenberg, N.; Hvolby, A.; Mølgaard, C.; Michaelsen, K.F.; Lauritzen, L. Diet in the Treatment of ADHD in Children—A Systematic Review of the Literature. Nord. J. Psychiatry 2015, 69, 1–18. [Google Scholar] [CrossRef]
- McCann, D.; Barrett, A.; Cooper, A.; Crumpler, D.; Dalen, L.; Grimshaw, K.; Kitchin, E.; Lok, K.; Porteous, L.; Prince, E.; et al. Food Additives and Hyperactive Behaviour in 3-Year-Old and 8/9-Year-Old Children in the Community: A Randomised, Double-Blinded, Placebo-Controlled Trial. Lancet 2007, 370, 1560–1567. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.J.; Kuczek, T.; Burgess, J.R.; Hurt, E.; Arnold, L.E. Dietary Sensitivities and ADHD Symptoms: Thirty-Five Years of Research. Clin. Pediatr. 2011, 50, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S. The Association between ADHD and Obesity: Intriguing, Progressively More Investigated, but Still Puzzling. Brain Sci. 2019, 9, 256. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Moreira-Maia, C.R.; Fleur, D.S.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association Between ADHD and Obesity: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef]
- Tandon, P.S.; Sasser, T.; Gonzalez, E.S.; Whitlock, K.B.; Christakis, D.A.; Stein, M.A. Physical Activity, Screen Time, and Sleep in Children With ADHD. J. Phys. Act. Health 2019, 16, 416–422. [Google Scholar] [CrossRef]
- Peralta, G.P.; Forns, J.; García de la Hera, M.; González, L.; Guxens, M.; López-Vicente, M.; Sunyer, J.; Garcia-Aymerich, J.; Sleeping, T.V. Cognitively Stimulating Activities, Physical Activity, and Attention-Deficit Hyperactivity Disorder Symptom Incidence in Children: A Prospective Study. J. Dev. Behav. Pediatr. JDBP 2018, 39, 192–199. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Overall | Total Added Sugar Consumption from Common Beverages in g/Day | p-Value | |||
|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | |||
| (n = 441) | (n = 147) | (n = 147) | (n = 147) | ||
| Sex (n (%)) | |||||
| Male | 178 (40.4%) | 59 (40.1%) | 54 (36.7%) | 65 (44.2%) | 0.476 |
| Female | 263 (59.6%) | 88 (59.9%) | 93 (63.3%) | 82 (55.8%) | |
| Age (years, mean ± SD) | 20.6 ± 1.9 | 20.8 ± 1.9 | 20.3 ± 1.9 | 20.5 ± 2.0 | 0.237 |
| Weight (kg, mean ± SD) | 59.3 ± 13.1 | 60.5 ± 13.9 | 58.3 ± 11.8 | 59.0 ± 13.6 | 0.342 |
| Height (cm, mean ± SD) | 165.4 ± 8.2 | 165.4 ± 8.1 | 164.4 ± 7.7 | 166.5 ± 8.5 | 0.261 |
| BMI (kg/m2, mean ± SD) | 21.5 ± 3.7 | 22.0 ± 4.0 | 21.5 ± 3.4 | 21.2 ± 3.8 | 0.072 |
| Year of study (n (%)) | |||||
| 1st | 103 (23.4%) | 26 (17.7%) | 40 (27.2%) | 37 (25.2%) | 0.140 |
| 2nd | 53 (12.0%) | 19 (12.9%) | 18 (12.2%) | 16 (10.9%) | |
| 3rd | 102 (23.1%) | 33 (22.4%) | 32 (21.8%) | 37 (25.2%) | |
| 4th | 79 (17.9%) | 28 (19.0%) | 26 (17.7%) | 25 (17.0%) | |
| 5th | 38 (8.6%) | 15 (10.2%) | 14 (9.5%) | 9 (6.1%) | |
| 6th | 66 (15.0%) | 26 (17.7%) | 17 (11.6%) | 23 (15.6%) | |
| Clinical year (n(%)) | 183 (41.5%) | 69 (46.9%) | 57 (38.8%) | 57 (38.8%) | 0.156 |
| History of ADHD in family (n (%)) | 11 (2.5%) | 2 (1.4%) | 5 (3.4%) | 4 (2.7%) | 0.455 |
| Maternal education (n (%)) | |||||
| Below bachelor’s degree | 98 (22.3%) | 37 (25.3%) | 28 (19.0%) | 33 (22.4%) | 0.592 |
| Bachelor’s degree | 251 (57.0%) | 83 (56.8%) | 82 (55.8%) | 86 (58.5%) | |
| Above bachelor’s degree | 91 (20.7%) | 26 (17.8%) | 37 (25.2%) | 28 (19.0%) | |
| Paternal education (n (%)) | |||||
| Below bachelor’s degree | 99 (22.6%) | 39 (26.9%) | 27 (18.4%) | 33 (22.4%) | 0.414 |
| Bachelor’s degree | 218 (49.7%) | 68 (46.9%) | 78 (53.1%) | 72 (49.0%) | |
| Above bachelor’s degree | 122 (27.8%) | 38 (26.2%) | 42 (28.6%) | 42 (28.6%) | |
| Monthly allowance (n (%)) | |||||
| Below THB 10,000 per month * | 345 (78.2%) | 112 (76.2%) | 119 (81.0%) | 114 (77.6%) | 0.778 |
| Above THB 10,000 per month * | 96 (21.8%) | 35 (23.8%) | 28 (19.0%) | 33 (22.4%) | |
| Monthly family’s income (n (%)) | |||||
| Below THB 50,000 per month * | 187 (42.4%) | 74 (50.3%) | 52 (35.4%) | 61 (41.5%) | 0.125 |
| Above THB 50,000 per month * | 254 (57.6%) | 73 (49.7%) | 95 (64.6%) | 86 (58.5%) | |
| Daily sleep duration (hours, median (IQR)) | 6 (6–7) | 6 (6–7) | 7 (6–7) | 6 (6–7) | 0.088 |
| Daily sleep duration < 7 h (n (%)) | 245 (55.6%) | 96 (65.3%) | 71 (48.3%) | 78 (53.1%) | 0.035 |
| Daily screen time (hours, median (IQR)) | 8 (6–10) | 8 (6–10) | 8 (6–10) | 8 (6–10) | 0.723 |
| Daily screen time ≥ 7 h (n (%)) | 309 (70.1%) | 106 (72.1%) | 100 (68.0%) | 103 (70.1) | 0.703 |
| Total added-sugar consumption from common beverages (g/day, median (IQR)) | 24 (13–16) | 9 (4–13) | 24 (20–28) | 46 (36–60) | <0.001 |
| Overall | Total Added-Sugar Consumption from Common Beverages in g/Day | p-Value | |||
|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | |||
| (n = 441) | (n = 147) | (n = 147) | (n = 147) | ||
| ASRS v1.1 risk score (median (IQR)) | 1 (0–3) | 1 (0–3) | 1 (0–3) | 2 (0–3) | 0.156 |
| ADHD symptoms | |||||
| Presence | 132 (29.9%) | 38 (25.9%) | 45 (30.6%) | 49 (33.3%) | 0.162 |
| Absence | 309 (70.1%) | 109 (74.1%) | 102 (69.4%) | 98 (66.7%) | |
| You sometimes/often/very often have trouble wrapping up the final details of a project, once the challenging parts have been done | 215 (48.8%) | 62 (42.2%) | 74 (50.3%) | 79 (53.7%) | 0.048 |
| You sometimes/often/very often have difficulty getting things in order when you have to do a task that requires organization | 150 (34.0%) | 47 (32.0%) | 48 (32.7%) | 55 (37.4%) | 0.325 |
| You sometimes/often/very often have problems remembering appointments or obligations | 163 (37.0%) | 56 (38.1%) | 53 (36.1%) | 54 (36.7%) | 0.809 |
| You often/very often have a task that requires a lot of thought, how often do you avoid or delay getting started | 92 (20.9%) | 24 (16.3%) | 38 (25.9%) | 30 (20.4%) | 0.390 |
| You often/very often fidget or squirm with your hands or feet when you have to sit down for a long time | 102 (23.1%) | 32 (21.8%) | 28 (19.0%) | 42 (28.6%) | 0.167 |
| You often/very often feel overly active and compelled to do things, like you were driven by a motor | 35 (7.9%) | 13 (8.8%) | 9 (6.1%) | 13 (8.8%) | 1.000 |
| With ADHD Symptoms | Without ADHD Symptoms | p-Value | |
|---|---|---|---|
| (n = 132) | (n = 309) | ||
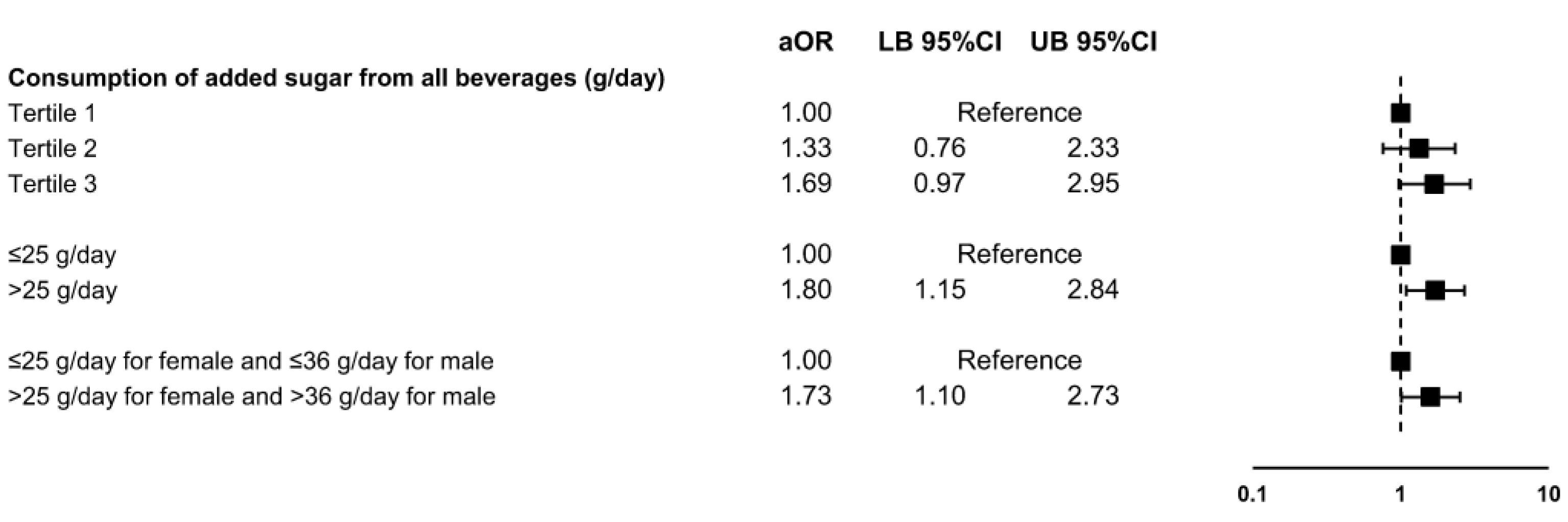
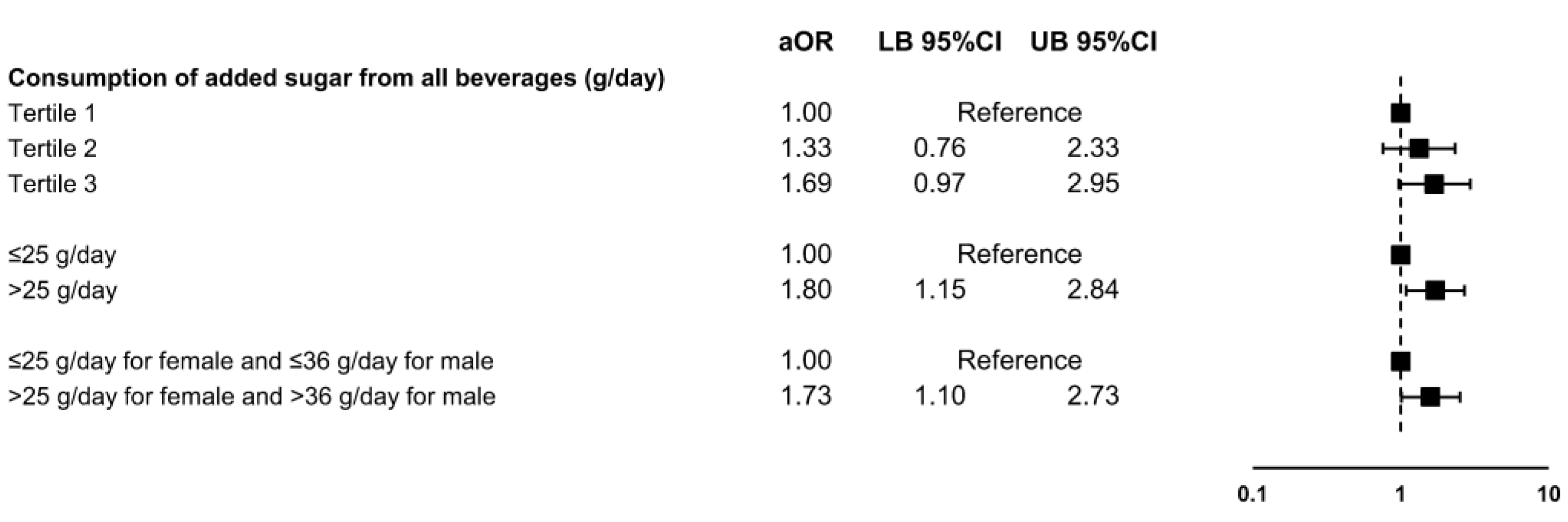
| Daily consumption of added sugar from all beverages (g/day) (n (%)) | |||
| Tertile 1 | 38 (28.8%) | 109 (35.3%) | 0.359 |
| Tertile 2 | 45 (34.1%) | 102 (33.0%) | |
| Tertile 3 | 49 (37.1%) | 98 (31.7%) | |
| ≤25 g/day | 59 (44.7%) | 169 (54.7%) | 0.061 |
| >25 g/day | 73 (55.3%) | 140 (45.3%) | |
| ≤recommended cutoff points | 68 (51.5%) | 191 (61.8%) | 0.046 |
| >recommended cutoff points | 64 (48.5%) | 118 (38.2%) | |
| Daily consumption of added sugar (g/day) (median (IQR)) | |||
| All beverages | 26 (13–37) | 23 (13–35) | 0.162 |
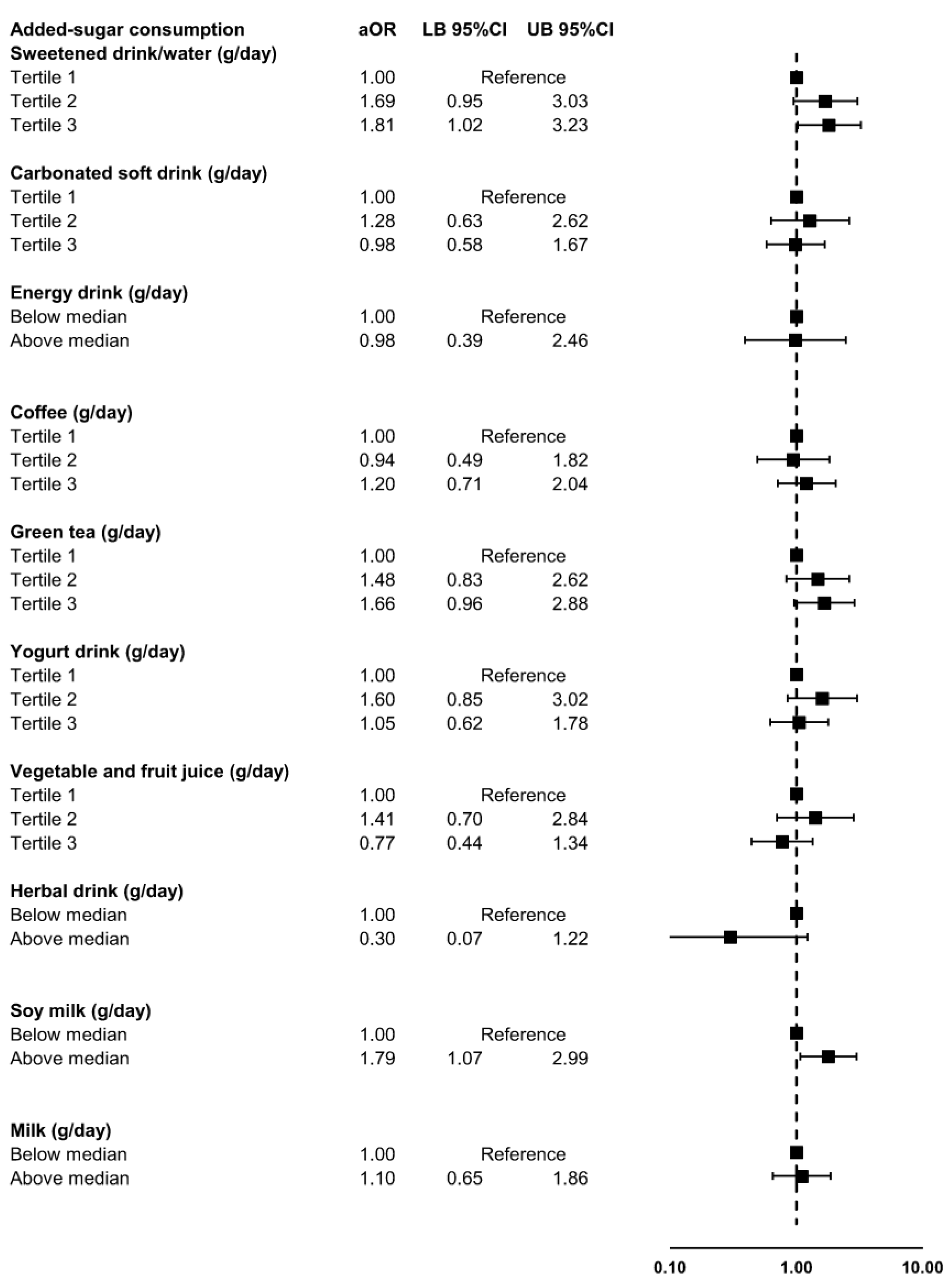
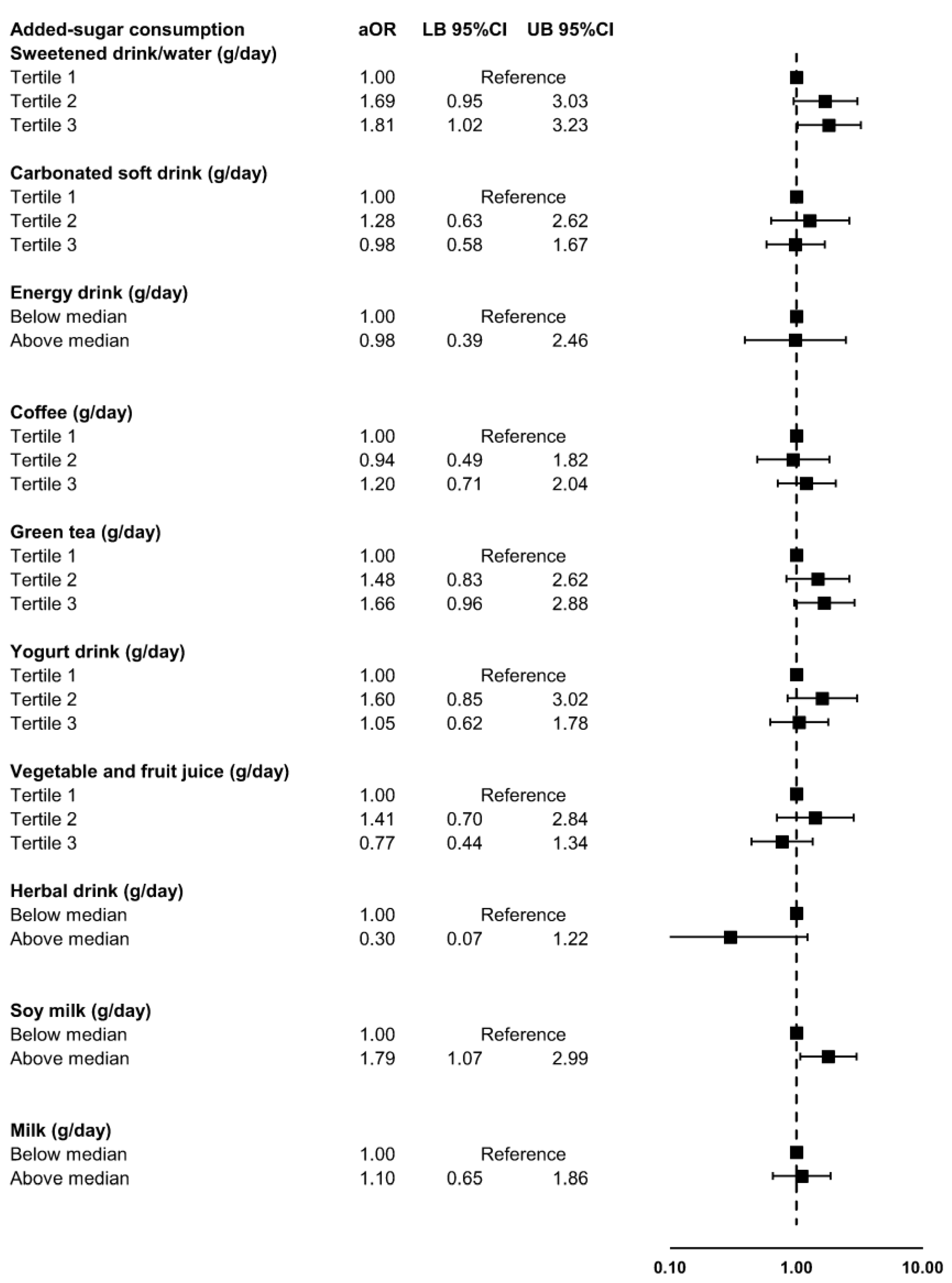
| Only sweetened drinks/water | 4 (0–6) | 2 (0–5) | 0.045 |
| Only carbonated soft drinks | 0 (0–4) | 0 (0–4) | 0.869 |
| Only energy drinks | 0 (0–0) | 0 (0–0) | 0.334 |
| Only coffee | 1 (0–8) | 0 (0–5) | 0.376 |
| Only green tea | 2 (0–8) | 0 (0–4) | 0.030 |
| Only yogurt drinks | 3 (0–6) | 0 (0–6) | 0.668 |
| Only vegetable and fruit juice | 0 (0–4) | 0 (0–5) | 0.513 |
| Only herbal drinks | 0 (0–0) | 0 (0–0) | 0.210 |
| Only soy milk | 0 (0–1) | 0 (0–0) | 0.073 |
| Only milk | 0 (0–2) | 0 (0–2) | 0.999 |
| With ADHD Symptoms | Without ADHD Symptoms | p-Value | |
|---|---|---|---|
| (n = 132) | (n = 309) | ||
| Sex (n (%)) | |||
| Male | 54 (40.9%) | 124 (40.1%) | 0.916 |
| Female | 78 (59.1%) | 185 (59.9%) | |
| Age (years, mean ± SD) | 20.9 ± 2.1 | 20.4 ± 1.8 | 0.015 |
| Age > 20 years (n(%)) | 66 (50.0%) | 134 (43.4%) | 0.211 |
| BMI (kg/m2, mean ± SD) | 22.3 ± 4.4 | 21.2 ± 3.4 | 0.007 |
| Overweight (n(%)) | 75 (56.8%) | 143 (46.3%) | 0.048 |
| Year of study (n (%)) | |||
| 1st | 26 (19.7%) | 77 (24.9%) | 0.019 |
| 2nd | 16 (12.1%) | 37 (12.0%) | |
| 3rd | 28 (21.2%) | 74 (23.9%) | |
| 4th | 18 (13.6%) | 61 (19.7%) | |
| 5th | 12 (9.1%) | 26 (8.4%) | |
| 6th | 32 (24.2%) | 34 (11.0%) | |
| Clinical year (n(%)) | 62 (47.0%) | 121 (39.2%) | 0.140 |
| History of ADHD in family (n (%)) | 4 (3.0%) | 7 (2.3%) | 0.740 |
| Maternal education (n (%)) | |||
| Below bachelor’s degree | 22 (16.7%) | 76 (24.7%) | 0.158 |
| Bachelor’s degree | 79 (59.8%) | 172 (55.8%) | |
| Above bachelor’s degree | 31 (23.5%) | 60 (19.5%) | |
| Paternal education (n (%)) | |||
| Below bachelor’s degree | 24 (18.2%) | 75 (24.4%) | 0.346 |
| Bachelor’s degree | 68 (51.5%) | 150 (48.9%) | |
| Above bachelor’s degree | 40 (30.3%) | 82 (26.7%) | |
| Monthly allowance (n (%)) | |||
| Below THB 10,000 per month * | 96 (72.7%) | 249 (80.6%) | 0.078 |
| Above THB 10,000 per month * | 36 (27.3%) | 60 (19.4%) | |
| Monthly family’s income (n (%)) | |||
| Below THB 50,000 per month * | 49 (37.1%) | 138 (44.7%) | 0.171 |
| Above THB 50,000 per month * | 83 (62.9%) | 171 (55.3%) | |
| Daily sleep duration (hours, median (IQR)) | 6 (6–7) | 6 (6–7) | 0.097 |
| Daily sleep duration < 7 h (n (%)) | 79 (59.8%) | 166 (53.7%) | 0.251 |
| Daily screen time (hours, median (IQR)) | 9 (8–11) | 8 (6–10) | 0.011 |
| Daily screen time ≥ 7 h (n (%)) | 104 (78.8%) | 205 (66.3%) | 0.009 |
| Daily consumption of added sugar from common beverages > 25 g/day (n (%)) | 73 (55.3%) | 140 (45.3%) | 0.061 |
| Factors | Adjusted Odds Ratio (95%CI) | p-Value |
|---|---|---|
| Female | 1.04 (0.67 to 1.62) | 0.853 |
| Age > 20 years (n(%)) | 0.93 (0.36 to 2.42) | 0.879 |
| Overweight (n(%)) | 1.92 (1.05 to 3.50) | 0.033 |
| Clinical year (n(%)) | 1.33 (0.51 to 3.47) | 0.558 |
| History of ADHD in family (n (%)) | 1.28 (0.35 to 4.65) | 0.712 |
| Maternal education (n (%)) | ||
| Below bachelor’s degree | 1.00 (Reference) | |
| Bachelor’s degree | 1.43 (0.71 to 2.85) | 0.315 |
| Above bachelor’s degree | 1.69 (0.75 to 3.81) | 0.208 |
| Paternal education (n (%)) | ||
| Below bachelor’s degree | 1.00 (Reference) | |
| Bachelor’s degree | 1.15 (0.59 to 2.24) | 0.675 |
| Above bachelor’s degree | 1.16 (0.54 to 2.49) | 0.699 |
| Monthly allowance above THB 10,000 per month * (n (%)) | 1.48 (0.88 to 2.49) | 0.139 |
| Monthly family’s income above THB 50,000 per month * (n (%)) | 1.02 (0.63 to 1.68) | 0.925 |
| Daily sleep duration < 7 h (n (%)) | 1.22 (0.79 to 1.90) | 0.367 |
| Daily screen time ≥ 7 h (n (%)) | 1.97 (1.20 to 3.23) | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yingchankul, N.; Panuspanudechdamrong, C.; Techapipatchai, N.; Chanmuang, T.; Netsiri, P.; Karawekpanyawong, N.; Tanasombatkul, K.; Phinyo, P. Is the Consumption of Added Sugar from Common Beverages Associated with the Presence of Attention Deficit Hyperactivity Disorder Symptoms in Thai Medical Students? Nutrients 2023, 15, 4395. https://doi.org/10.3390/nu15204395
Yingchankul N, Panuspanudechdamrong C, Techapipatchai N, Chanmuang T, Netsiri P, Karawekpanyawong N, Tanasombatkul K, Phinyo P. Is the Consumption of Added Sugar from Common Beverages Associated with the Presence of Attention Deficit Hyperactivity Disorder Symptoms in Thai Medical Students? Nutrients. 2023; 15(20):4395. https://doi.org/10.3390/nu15204395
Chicago/Turabian StyleYingchankul, Nalinee, Chompimaksorn Panuspanudechdamrong, Nuthakul Techapipatchai, Tiphakorn Chanmuang, Pintira Netsiri, Nuntaporn Karawekpanyawong, Krittai Tanasombatkul, and Phichayut Phinyo. 2023. "Is the Consumption of Added Sugar from Common Beverages Associated with the Presence of Attention Deficit Hyperactivity Disorder Symptoms in Thai Medical Students?" Nutrients 15, no. 20: 4395. https://doi.org/10.3390/nu15204395
APA StyleYingchankul, N., Panuspanudechdamrong, C., Techapipatchai, N., Chanmuang, T., Netsiri, P., Karawekpanyawong, N., Tanasombatkul, K., & Phinyo, P. (2023). Is the Consumption of Added Sugar from Common Beverages Associated with the Presence of Attention Deficit Hyperactivity Disorder Symptoms in Thai Medical Students? Nutrients, 15(20), 4395. https://doi.org/10.3390/nu15204395