
Parental Feeding Styles and Risk of a New Carious Lesion in Preschool Children: A Longitudinal Study


Abstract
:1. Introduction
2. Materials and Methods
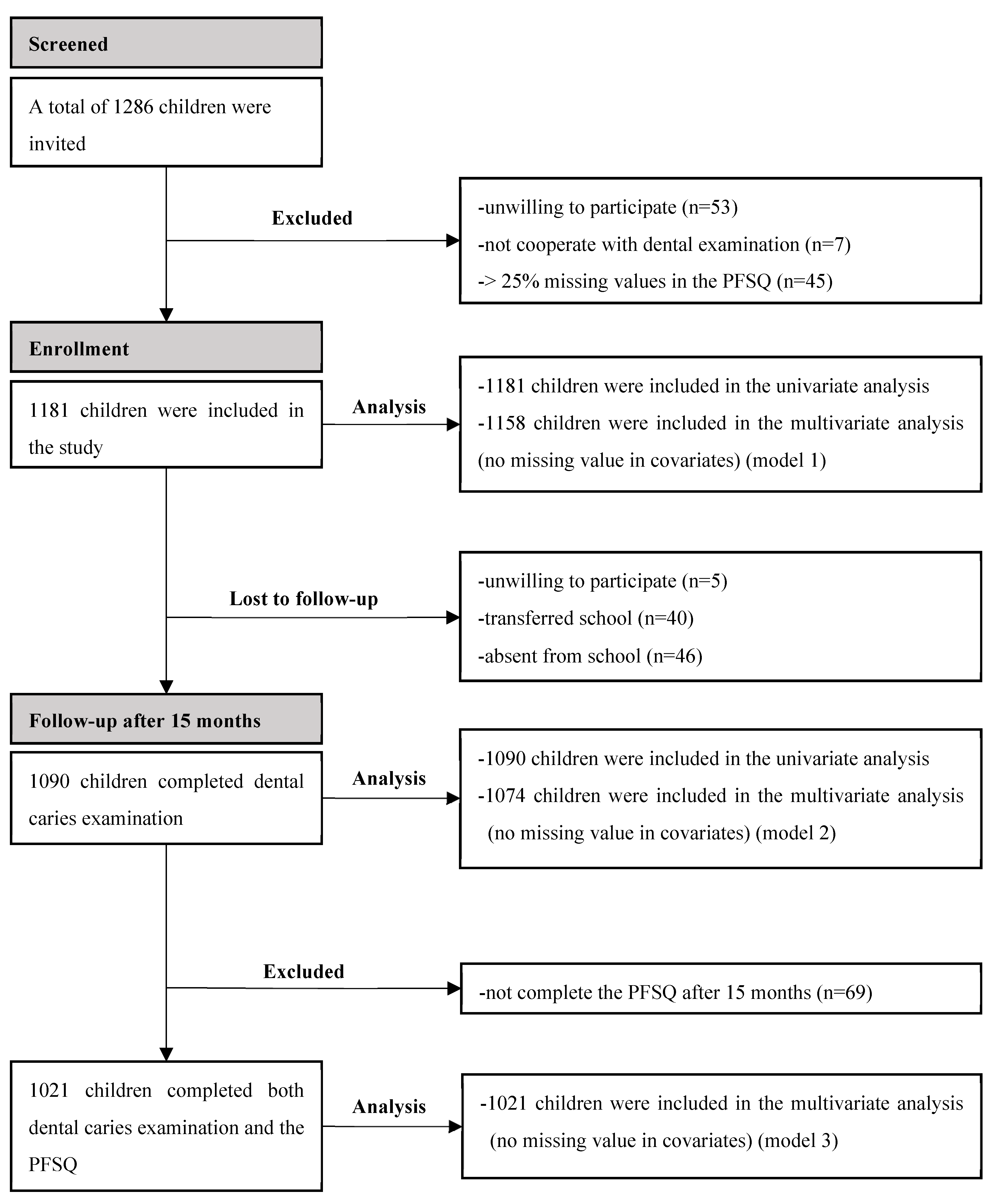
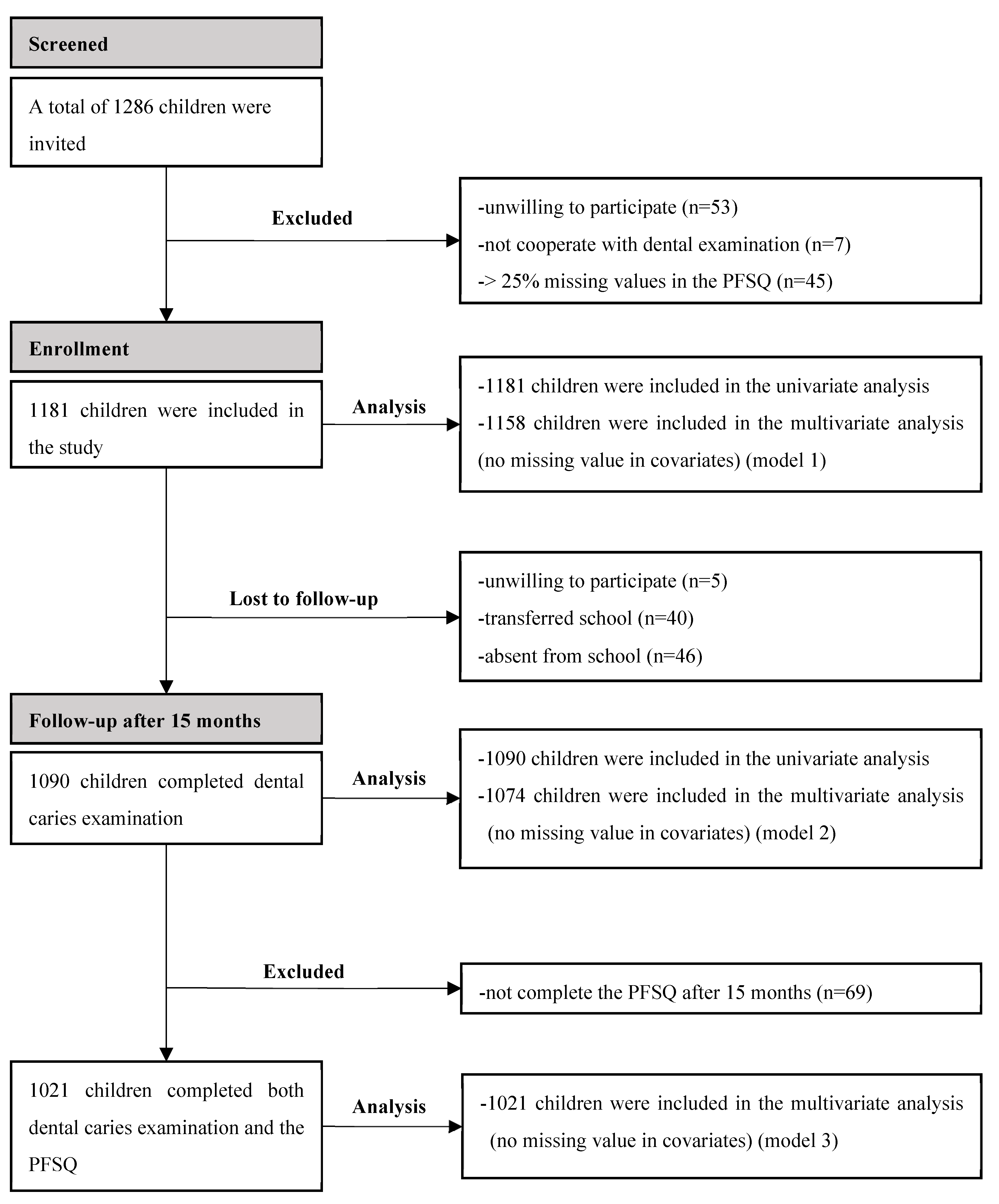
2.1. Study Design and Procedure
2.2. Sample Size
2.3. Clinical Examination
2.4. Questionnaires
2.5. Statistical Analysis
3. Results
3.1. General Information
3.2. Internal Reliability of the Parental Feeding Style Questionnaire
3.3. Construct Validity of the Parental Feeding Style Questionnaire
3.4. Reliability of Caries Diagnosis
3.5. Association between Parental Feeding Styles and Caries Status at Baseline
3.6. Longitudinal Associations between Baseline Parental Feeding Styles and Risk of a New Carious Lesion after 15 Months
3.7. Longitudinal Association between the Change in Parental Feeding Styles during the 15 Months and Risk of a New Carious Lesion after 15 Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drury, T.F.; Horowitz, A.M.; Ismail, A.I.; Maertens, M.P.; Rozier, R.G.; Selwitz, R.H. Diagnosing and reporting early childhood caries for research purposes. A report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J. Public Health Dent. 1999, 59, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Uribe, S.E.; Innes, N.; Maldupa, I. The global prevalence of early childhood caries: A systematic review with meta-analysis using the WHO diagnostic criteria. Int. J. Paediatr. Dent. 2021, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Du, M.Q.; Li, Z.; Jiang, H.; Wang, X.; Feng, X.P.; Hu, Y.; Lin, H.C.; Wang, B.; Si, Y.; Wang, C.X.; et al. Dental Caries Status and its Associated Factors among 3- to 5-year-old Children in China: A National Survey. Chin. J. Dent. Res. 2018, 21, 167–179. [Google Scholar] [CrossRef]
- Seow, W.K. Early Childhood Caries. Pediatr. Clin. N. Am. 2018, 65, 941–954. [Google Scholar] [CrossRef]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.J.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Baughcum, A.E.; Powers, S.W.; Johnson, S.B.; Chamberlin, L.A.; Deeks, C.M.; Jain, A.; Whitaker, R.C. Maternal feeding practices and beliefs and their relationships to overweight in early childhood. J. Dev. Behav. Pediatr. 2001, 22, 391–408. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.; Holub, S. Comprehensive feeding practices questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef]
- Wardle, J.; Sanderson, S.; Guthrie, C.A.; Rapoport, L.; Plomin, R. Parental feeding style and the intergenerational transmission of obesity risk. Obes. Res. 2002, 10, 453–462. [Google Scholar] [CrossRef]
- Tam, W.; Keung, V.; Lee, A.; Lo, K.; Cheung, C. Chinese translation and validation of a parental feeding style questionnaire for parents of Hong Kong preschoolers. BMC Public Health 2014, 14, 1194. [Google Scholar] [CrossRef]
- Inhulsen, M.-B.M.R.; Merelle, S.Y.M.; Renders, C.M. Parental feeding styles, young children’s fruit, vegetable, water and sugar-sweetened beverage consumption, and the moderating role of maternal education and ethnic background. Public Health Nutr. 2017, 20, 2124–2133. [Google Scholar] [CrossRef]
- Lo, K.; Cheung, C.; Lee, A.; Tam, W.W.S.; Keung, V. Associations between Parental Feeding Styles and Childhood Eating Habits: A Survey of Hong Kong Pre-School Children. PLoS ONE 2015, 10, e0124753. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.; Kremers, S.P.J.; Oenema, A.; van de Mheen, D. Associations of parental feeding styles with child snacking behaviour and weight in the context of general parenting. Public Health Nutr. 2014, 17, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Sleddens, E.F.; Kremers, S.P.; De Vries, N.K.; Thijs, C. Relationship between parental feeding styles and eating behaviours of Dutch children aged 6–7. Appetite 2010, 54, 30–36. [Google Scholar] [CrossRef] [PubMed]
- China Statistical Publishing House. Main economic indicators of Guangzhou and Shenzhen (2021). In Guang Dong Statistical Yearbook 2022; China Statistical Publishing House: Beijing, China, 2022; p. 626. [Google Scholar] [CrossRef]
- Water Supply Quality in Guangzhou. 2021. Available online: http://swj.gz.gov.cn/mssw/szy/szgg/szgg/content/post_7957855.html (accessed on 16 June 2023).
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; pp. 42–47. [Google Scholar]
- Per Capita Disposable Income and Expenditure of Urban Residents in Guangzhou in 2021. Available online: https://gdzd.stats.gov.cn/gzdcd/gz_tjsj/202202/t20220217_179293.html (accessed on 9 October 2023).
- Kelley, T.L. The selection of upper and lower groups for the validation of test Items. J. Educ. Psychol. 1939, 30, 17–24. [Google Scholar] [CrossRef]
- Eichler, J.; Schmidt, R.; Poulain, T.; Hiemisch, A.; Kiess, W.; Hilbert, A. Stability, Continuity, and Bi-Directional Associations of Parental Feeding Practices and Standardized Child Body Mass Index in Children from 2 to 12 Years of Age. Nutrients 2019, 11, 1751. [Google Scholar] [CrossRef]
- Nembhwani, H.V.; Winnier, J. Impact of problematic eating behaviour and parental feeding styles on early childhood caries. Int. J. Paediatr. Dent. 2020, 30, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 24. [Google Scholar] [CrossRef]
- Beckers, D.; Karssen, L.T.; Vink, J.M.; Burk, W.J.; Larsen, J.K. Food parenting practices and children’s weight outcomes: A systematic review of prospective studies. Appetite 2021, 158, 105010. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nyvad, B. The Role of Bacteria in the Caries Process: Ecological Perspectives. J. Dent. Res. 2011, 90, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, S.; Liu, P.; Lee, G.H.M.; Lo, E.C.M.; Yiu, C.K.Y. Risk Indicators for Noncavitated and Cavitated Carious Lesions in Preschool Children. Int. Dent. J. 2023, 73, 738–745. [Google Scholar] [CrossRef]
- Parisotto, T.M.; Steiner-Oliveira, C.; Duque, C.; Peres, R.C.; Rodrigues, L.K.; Nobre-dos-Santos, M. Relationship among microbiological composition and presence of dental plaque, sugar exposure, social factors and different stages of early childhood caries. Arch. Oral Biol. 2010, 55, 365–373. [Google Scholar] [CrossRef]
- Li, J.; Fan, W.; Zhou, Y.; Wu, L.; Liu, W.; Huang, S. The status and associated factors of early childhood caries among 3- to 5-year-old children in Guangdong, Southern China: A provincial cross-sectional survey. BMC Oral Health 2020, 20, 265. [Google Scholar] [CrossRef]
- Davis, E.; Martinez, G.; Blostein, F.; Marshall, T.; Jones, A.D.; Jansen, E.; McNeil, D.W.; Neiswanger, K.; Marazita, M.L.; Foxman, B. Dietary Patterns and Risk of a New Carious Lesion Postpartum: A Cohort Study. J. Dent. Res. 2022, 101, 295–303. [Google Scholar] [CrossRef]
- Echeverria, M.S.; Schuch, H.S.; Cenci, M.S.; Motta, J.V.S.; Bertoldi, A.D.; Hallal, P.C.; Demarco, F.F. Trajectories of Sugar Consumption and Dental Caries in Early Childhood. J. Dent. Res. 2022, 101, 724–730. [Google Scholar] [CrossRef]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef]
- Gotler, M.; Oren, L.; Spierer, S.; Yarom, N.; Ashkenazi, M. The impact of COVID-19 lockdown on maintenance of children’s dental health: A questionnaire-based survey. J. Am. Dent. Assoc. 2022, 153, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Thapaliya, G.; Aghababian, A.; Sadler, J.; Smith, K.; Carnell, S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite 2021, 161, 105119. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parental Feeding Style Questionnaire | Mean Score (SD) | Cronbach’s Alpha | Item-Deleted Cronbach’s Alpha |
|---|---|---|---|
| Instrumental feeding (4 items) | 2.59 (0.59) | 0.63 | 0.51–0.62 |
| Emotional feeding (5 items) | 2.27 (0.67) | 0.84 | 0.79–0.83 |
| Prompting or encouragement to eat (8 items) | 3.90 (0.68) | 0.89 | 0.86–0.89 |
| Control over eating (10 items) | 3.67 (0.48) | 0.67 | 0.62–0.72 |
| Total (27 items) | 0.79 | 0.77–0.80 |
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | |
|---|---|---|---|---|---|---|
| Instrumental feeding | ||||||
| In order to get my child to behave him/herself I promise him/her something to eat. | −0.06 | 0.21 | 0.03 | −0.15 | 0.72 | −0.02 |
| If my child misbehaves I withhold his/her favourite food. | 0.04 | 0.13 | 0.11 | 0.07 | 0.63 | 0.01 |
| I use puddings as a bribe to get my child to eat his/her main course. | −0.11 | 0.27 | −0.06 | −0.36 | 0.45 | −0.19 |
| I reward my child with something to eat when s/he is well behaved. | 0.12 | 0.24 | −0.01 | 0.01 | 0.74 | 0.07 |
| Emotional feeding | ||||||
| I give my child something to eat to make him/her feel better when s/he is feeling upset. | 0.06 | 0.63 | 0.04 | −0.03 | 0.40 | 0.00 |
| I give my child something to eat to make him/her feel better when s/he has been hurt. | 0.02 | 0.78 | 0.03 | −0.04 | 0.23 | −0.02 |
| I give my child something to eat if s/he is feeling bored. | −0.06 | 0.75 | 0.02 | −0.18 | 0.09 | −0.03 |
| I give my child something to eat to make him/her feel better when s/he is worried. | 0.03 | 0.83 | 0.02 | −0.12 | 0.14 | −0.02 |
| I give my child something to eat to make him/her feel better when s/he is feeling angry. | 0.00 | 0.74 | −0.12 | −0.19 | 0.11 | −0.07 |
| Promoting and encouragement to eat | ||||||
| I encourage my child to look forward to the meal. | 0.68 | 0.08 | 0.13 | 0.09 | −0.01 | 0.12 |
| I praise my child if s/he eats what I give him/her. | 0.65 | 0.06 | 0.09 | −0.04 | 0.18 | −0.17 |
| I encourage my child to eat a wide variety of foods. | 0.75 | −0.04 | 0.15 | −0.02 | 0.02 | 0.15 |
| I present food in an attractive way to my child. | 0.64 | 0.14 | 0.15 | −0.04 | −0.12 | −0.05 |
| I encourage my child to taste each of the foods I serve at mealtimes. | 0.78 | −0.09 | 0.20 | 0.06 | −0.01 | 0.19 |
| I encourage my child to try foods that s/he hasn’t tasted before. | 0.75 | −0.11 | 0.18 | 0.00 | −0.01 | 0.21 |
| I encourage my child to enjoy his/her food. | 0.78 | −0.02 | 0.15 | 0.09 | −0.06 | 0.15 |
| I praise my child if s/he eats a new food. | 0.78 | −0.02 | 0.18 | 0.01 | 0.12 | −0.01 |
| Control over eating | ||||||
| I decide when it is time for my child to have a snack. | 0.24 | 0.05 | 0.78 | −0.04 | 0.08 | −0.01 |
| I decide how many snacks my child should have. | 0.24 | −0.08 | 0.78 | 0.04 | 0.12 | 0.08 |
| I decide what my child eats between meals. | 0.27 | 0.03 | 0.77 | 0.02 | −0.03 | 0.03 |
| I decide the times when my child eats his/her meals. | 0.29 | −0.04 | 0.62 | 0.08 | −0.02 | 0.27 |
| I insist my child eats meals at the table. | 0.32 | −0.07 | 0.24 | 0.26 | 0.01 | 0.67 |
| I allow my child to choose which foods to have for meals *. | −0.12 | 0.03 | −0.11 | 0.35 | −0.03 | −0.65 |
| I allow my child to wander around during a meal *. | 0.11 | −0.13 | −0.04 | 0.60 | −0.08 | 0.47 |
| I allow my child to decide when s/he has had enough snacks to eat *. | −0.03 | −0.14 | −0.04 | 0.66 | 0.00 | −0.20 |
| I let my child eat between meals whenever s/he wants *. | 0.08 | −0.07 | 0.10 | 0.76 | −0.06 | 0.00 |
| I let my child decide when s/he would like to have her meal *. | −0.03 | −0.16 | 0.02 | 0.71 | −0.01 | 0.04 |
| OR (95%CI) | p | |
|---|---|---|
| Parental feeding style | ||
| Instrumental feeding | 1.13 (0.88–1.46) | 0.329 |
| Emotional feeding | 0.97 (0.78–1.22) | 0.806 |
| Prompting or encouragement to eat | 0.87 (0.70–1.07) | 0.174 |
| Control over eating | 0.60 (0.44–0.83) | 0.002 |
| Age (months) | 1.08 (1.04–1.12) | <0.001 |
| BMI | 1.01 (0.90–1.12) | 0.924 |
| Visible plaque index a | 1.29 (1.20–1.39) | <0.001 |
| Gender | ||
| Female (Ref: male) | 1.02 (0.79–1.33) | 0.854 |
| Residence | ||
| Suburban (Ref: urban) | 1.61 (1.20–2.15) | 0.001 |
| Paternal education level | ||
| High school or below (Ref: college or above) | 1.25 (0.84–1.86) | 0.280 |
| Maternal education level | ||
| High school or below (Ref: college or above) | 1.79 (1.19–2.69) | 0.005 |
| Household monthly income | ||
| High-income (Ref: low-income) | 0.81 (0.59–1.11) | 0.194 |
| Moderate-income (Ref: low-income) | 0.89 (0.64–1.24) | 0.498 |
| Frequency of eating deserts | ||
| ≥2 times per week (Ref: <1 time per week) | 1.29 (0.92–1.81) | 0.143 |
| 1 time per week (Ref: <1 time per week) | 1.24 (0.82–1.88) | 0.300 |
| Frequency of drinking sugar-sweetened beverages | ||
| ≥2 times per week (Ref: <1 time per week) | 1.43 (0.85–2.41) | 0.180 |
| 1 time per week (Ref: <1 time per week) | 1.50 (1.00–2.23) | 0.049 |
| Consumption of sweets before sleep | ||
| Frequently (Ref: never) | 1.47 (1.00–2.15) | 0.048 |
| Occasionally (Ref: never) | 1.22 (0.91–1.64) | 0.190 |
| Frequency of toothbrushing | ||
| <2 times per day (Ref: ≥2 times per day) | 0.85 (0.65–1.12) | 0.258 |
| Supervised toothbrushing | ||
| Occasionally or never (Ref: frequently) | 0.87 (0.67–1.14) | 0.323 |
| Using fluoride toothpaste | ||
| No (Ref: yes) | 0.94 (0.69–1.28) | 0.680 |
| Unknown (Ref: yes) | 0.87 (0.61–1.23) | 0.425 |
| Professional fluoride application within 6 months | ||
| No (Ref: yes) | 0.73 (0.53–0.98) | 0.038 |
| Unknown (Ref: yes) | 0.84 (0.50–1.40) | 0.499 |
| OR (95%CI) | p | |
|---|---|---|
| Parental feeding style | ||
| Instrumental feeding | 1.05 (0.79–1.39) | 0.749 |
| Emotional feeding | 0.94 (0.73–1.20) | 0.609 |
| Prompting or encouragement to eat | 0.93 (0.73–1.17) | 0.537 |
| Control over eating | 0.88 (0.62–1.25) | 0.485 |
| Age (months) | 1.04 (1.00–1.09) | 0.044 |
| BMI | 0.99 (0.88–1.11) | 0.867 |
| Visible plaque index a | 1.11 (1.03–1.21) | 0.010 |
| Past caries experience | ||
| Caries (Ref: caries-free) | 5.58 (4.16–7.48) | <0.001 |
| Gender | ||
| Female (Ref: male) | 1.00 (0.75–1.32) | 0.991 |
| Residence | ||
| Suburban (Ref: urban) | 1.13 (0.81–1.57) | 0.470 |
| Paternal education level | ||
| High school or below (Ref: college or above) | 1.32 (0.83–2.08) | 0.236 |
| Maternal education level | ||
| High school or below (Ref: college or above) | 0.79 (0.50–1.25) | 0.311 |
| Household monthly income | ||
| High-income (Ref: low-income) | 0.93 (0.66–1.31) | 0.683 |
| Moderate-income (Ref: low-income) | 1.13 (0.78–1.62) | 0.519 |
| Frequency of eating deserts | ||
| ≥2 times per week (Ref: <1 time per week) | 1.21 (0.83–1.77) | 0.322 |
| 1 time per week (Ref: <1 time per week) | 0.70 (0.45–1.10) | 0.118 |
| Frequency of drinking sugar-sweetened beverages | ||
| ≥2 times per week (Ref: <1 time per week) | 0.90 (0.50–1.59) | 0.707 |
| 1 time per week (Ref: <1 time per week) | 1.05 (0.67–1.65) | 0.821 |
| Consumption of sweets before sleep | ||
| Frequently (Ref: never) | 0.94 (0.62–1.42) | 0.771 |
| Occasionally (Ref: never) | 1.02 (0.74–1.42) | 0.896 |
| Frequency of toothbrushing | ||
| <2 times per day (Ref: ≥2 times per day) | 1.21 (0.89–1.64) | 0.218 |
| Supervised toothbrushing | ||
| Occasionally or never (Ref: frequently) | 1.45 (1.08–1.95) | 0.015 |
| Using fluoride toothpaste | ||
| No (Ref: yes) | 0.92 (0.65–1.29) | 0.621 |
| Unknown (Ref: yes) | 0.77 (0.53–1.12) | 0.174 |
| Professional fluoride application within 6 months | ||
| No (Ref: yes) | 0.88 (0.63–1.23) | 0.463 |
| Unknown (Ref: yes) | 1.39 (0.78–2.47) | 0.268 |
| Instrumental Feeding (OR, 95%CI) | Emotional Feeding (OR, 95%CI) | Prompting or Encouragement to Eat (OR, 95%CI) | Control over Eating (OR, 95%CI) | |
|---|---|---|---|---|
| Increasing scores | 1.91 (1.18–3.12) ** | 1.46 (0.87–2.44) | 0.87 (0.52–1.48) | 0.50 (0.31–0.83) ** |
| Decreasing scores | 1.17 (0.75–1.83) | 1.13 (0.68–1.89) | 0.68 (0.41–1.14) | 0.68 (0.41–1.14) |
| Always-high scores | 1.18 (0.67–2.09) | 0.96 (0.54–1.68) | 1.49 (0.82–2.73) | 0.42 (0.23–0.77) ** |
| Always-intermediate scores | 1.29 (0.77–2.17) | 1.33 (0.76–2.31) | 0.85 (0.50–1.46) | 0.51 (0.30–0.86) * |
| Always-low scores | 1.00 | 1.00 | 1.00 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, J.; Tao, Y.; Pang, L.; Cao, Y.; Lin, H.; Zhou, Y. Parental Feeding Styles and Risk of a New Carious Lesion in Preschool Children: A Longitudinal Study. Nutrients 2023, 15, 4387. https://doi.org/10.3390/nu15204387
Wen J, Tao Y, Pang L, Cao Y, Lin H, Zhou Y. Parental Feeding Styles and Risk of a New Carious Lesion in Preschool Children: A Longitudinal Study. Nutrients. 2023; 15(20):4387. https://doi.org/10.3390/nu15204387
Chicago/Turabian StyleWen, Jie, Ye Tao, Liangyue Pang, Yina Cao, Huancai Lin, and Yan Zhou. 2023. "Parental Feeding Styles and Risk of a New Carious Lesion in Preschool Children: A Longitudinal Study" Nutrients 15, no. 20: 4387. https://doi.org/10.3390/nu15204387
APA StyleWen, J., Tao, Y., Pang, L., Cao, Y., Lin, H., & Zhou, Y. (2023). Parental Feeding Styles and Risk of a New Carious Lesion in Preschool Children: A Longitudinal Study. Nutrients, 15(20), 4387. https://doi.org/10.3390/nu15204387