

Frailty-Preventing Effect of an Intervention Program Using a Novel Complete Nutritional “COMB-FP Meal”: A Pilot Randomized Control Trial
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Popuration
- Males and females aged 60 years and above.
- Individuals who were classified as having pre-frailty or frailty according to the revised Japanese version of the Cardiovascular Health Study (J-CHS) standards.
- Individuals with a cognitive function test result ranging from normal to mild cognitive impairment (MCI).
- Individuals who could take a test meal twice a day
- Individuals who had received a full COVID-19 vaccination (took second shots and/or booster shots).
- Individuals who could provide a sufficient explanation of the purpose and content of the research, have the ability to provide consent, demonstrate a proper understanding of the subject, voluntarily apply for participation, and agree to participate in writing.
- Individuals who planned to donate blood during the trial or donated within the past four weeks.
- Individuals at risk of developing allergies due to test meals.
- Individuals with implantable medical electrical equipment, such as pacemakers or other metal medical equipment, or the absence of limbs
- Individuals requiring care, the presence of motor dysfunction, dementia, and an inability to perform the exercise program.
- Individuals with a history of gastrointestinal surgery or a severe digestive disorder.
- Individuals judged to be extremely picky eaters and have dysphagia or a small appetite.
- Individuals with extremely irregular eating habits.
- Individuals with a history of regular intake of protein supplements.
- Individuals undergoing exercise therapy or diet therapy.
- Individuals with excessive alcohol consumption (60 g/day) or heavy smoking (21 cigarettes/day).
- Individuals with irregular daily routines owing to night work or working shifts.
- Individuals consuming of foods for specific health issues, functional foods, and supplements that would affect the trial.
- Individuals without a microwave oven.
- Individuals deemed ineligible for participation by the principal investigator based on blood test results.
- Participation in other research that involves the consumption of other test foods or the use of pharmaceuticals and cosmetics within one month of providing informed consent or showing willingness to participate.
- Individuals judged ineligible by the principal investigator.
2.3. Randomization
2.4. Interventions
2.5. Outcomes
2.6. Procedures
2.7. Statistical Analysis
3. Results
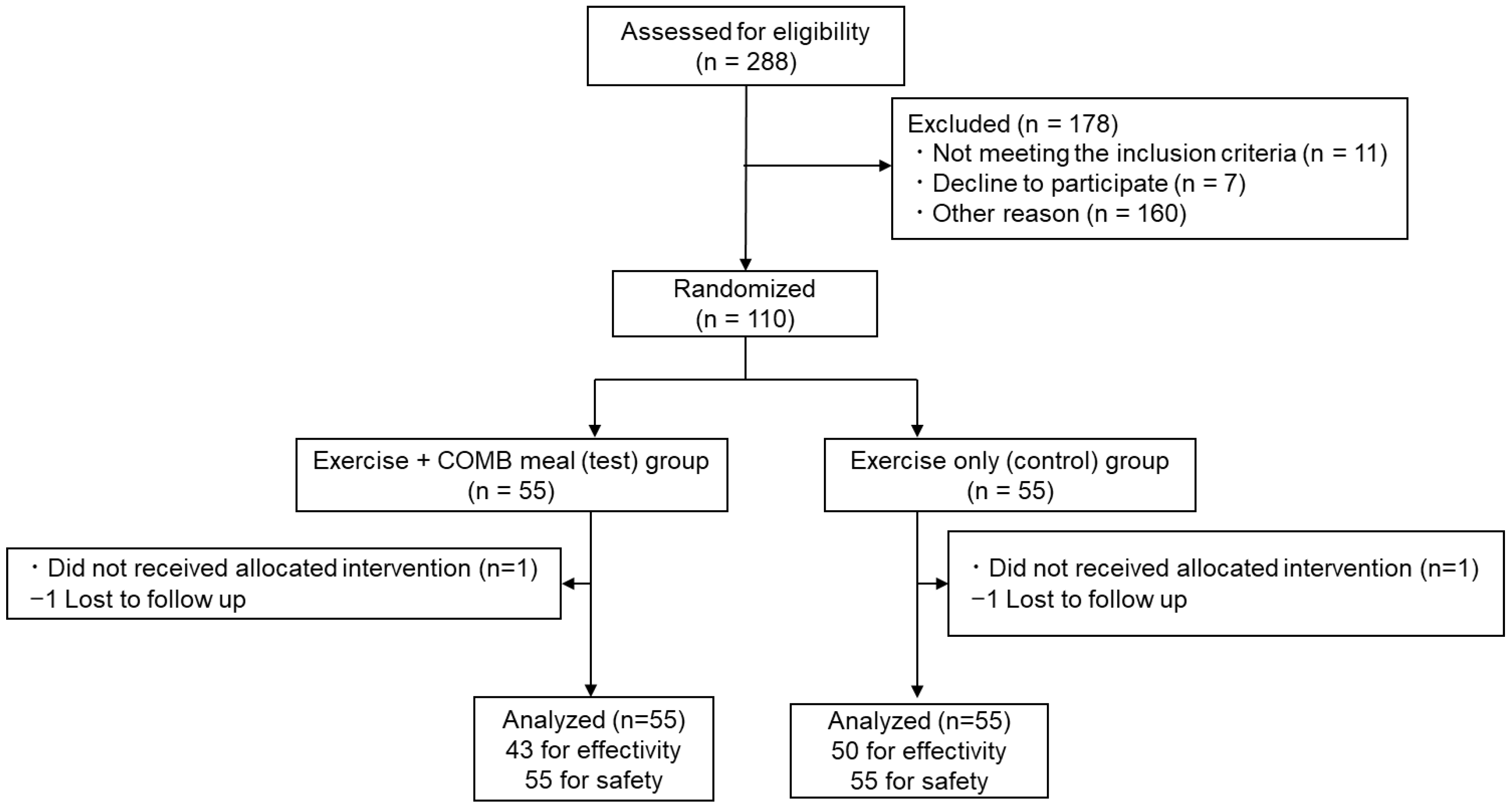
3.1. Participants
3.2. Effectiveness
3.3. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ni Lochlainn, M.; Cox, N.J.; Wilson, T.; Hayhoe, R.P.G.; Ramsay, S.E.; Granic, A.; Isanejad, M.; Roberts, H.C.; Wilson, D.; Welch, C.; et al. Nutrition and frailty: Opportunities for prevention and treatment. Nutrients 2021, 13, 2349. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Murayama, H.; Kobayashi, E.; Okamoto, S.; Fukaya, T.; Ishizaki, T.; Liang, J.; Shinkai, S. National prevalence of frailty in the older Japanese population: Findings from a nationally representative survey. Arch. Gerontol. Geriatr. 2020, 91, 104220. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D.; et al. Global Incidence of Frailty and Prefrailty among Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e198398. [Google Scholar] [CrossRef]
- Hsieh, T.J.; Su, S.C.; Chen, C.W.; Kang, Y.W.; Hu, M.H.; Hsu, L.L.; Wu, S.Y.; Chen, L.; Chang, H.Y.; Chuang, S.Y.; et al. Individualized home-based exercise and nutrition interventions improve frailty in older adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 119. [Google Scholar] [CrossRef]
- Sadjapong, U.; Yodkeeree, S.; Sungkarat, S.; Siviroj, P. Multicomponent exercise program reduces frailty and inflammatory biomarkers and improves physical performance in community-dwelling older adults: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 3760. [Google Scholar] [CrossRef]
- Yoon, D.H.; Lee, J.Y.; Song, W. Effects of Resistance Exercise Training on Cognitive Function and Physical Performance in Cognitive Frailty: A Randomized Controlled Trial. J. Nutr. Health Aging 2018, 22, 944–951. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef]
- Severin, R.; Berner, P.M.; Miller, K.L.; Mey, J. The Crossroads of Aging: An Intersection of Malnutrition, Frailty, and Sarcopenia. Top Geriatr. Rehabil. 2019, 35, 79–87. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of malnutrition in older adults: A multinational perspective using the mini nutritional assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low Nutrient Intake Is an Essential Component of Frailty in Older Persons. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Lee, Y.-H.; Huh, J.H.; Kang, D.R.; Rhee, Y.; Lim, S.-K. Early-stage chronic kidney disease, insulin resistance, and osteoporosis as risk factors of sarcopenia in aged population: The Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008–2009. Osteoporos. Int. 2014, 25, 2189–2198. [Google Scholar] [CrossRef]
- Kim, C.O.; Lee, K.R. Preventive effect of protein-energy supplementation on the functional decline of frail older adults with low socioeconomic status: A community-based randomized controlled study. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2013, 68, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Dirks, M.L.; Van Der Zwaluw, N.; Verdijk, L.B.; Van De Rest, O.; de Groot, L.C.; van Loon, L.J. Protein Supplementation Increases Muscle Mass Gain During Prolonged Resistance-Type Exercise Training in Frail Elderly People: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein Supplementation Improves Physical Performance in Frail Elderly People: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef]
- Oktaviana, J.; Zanker, J.; Vogrin, S.; Duque, G. The effect of protein supplements on functional frailty in older persons: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 86, 103938. [Google Scholar] [CrossRef]
- Orkaby, A.R.; Dushkes, R.; Ward, R.; Djousse, L.; Buring, J.E.; Lee, I.-M.; Cook, N.R.; LeBoff, M.S.; Okereke, O.I.; Copeland, T.; et al. Effect of Vitamin D3and Omega-3 Fatty Acid Supplementation on Risk of Frailty: An Ancillary Study of a Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2231206. [Google Scholar] [CrossRef]
- Wu, S.-Y.; Cheng, Y.-Y.; Chang, H.-Y.; Wang, P.-H.; Hsieh, I.-C.; Yeh, N.-H.; Huang, K.-C.; Pan, W.-H. Efficacy of Dietary Intervention with Group Activities on Dietary Intakes, Frailty Status, and Working Memory: A Cluster-Randomized Controlled Trial in Community Strongholds. Nutrients 2023, 15, 1976. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Cerundolo, N.; Catania, P.; Prati, B.; Tana, C.; Meschi, T. Gut microbiota, muscle mass and function in aging: A focus on physical frailty and sarcopenia. Nutrients 2019, 11, 1633. [Google Scholar] [CrossRef]
- Shintouo, C.M.; Mets, T.; Beckwee, D.; Bautmans, I.; Ghogomu, S.M.; Souopgui, J.; Leemans, L.; Meriki, H.D.; Njemini, R. Is inflammageing influenced by the microbiota in the aged gut? A systematic review. Exp. Gerontol. 2020, 141, 111079. [Google Scholar] [CrossRef]
- Kiewiet, M.B.G.; Elderman, M.E.; El Aidy, S.; Burgerhof, J.G.M.; Visser, H.; Vaughan, E.E.; Faas, M.M.; de Vos, P. Flexibility of Gut Microbiota in Ageing Individuals during Dietary Fiber Long-Chain Inulin Intake. Mol. Nutr. Food Res. 2021, 65, e2000390. [Google Scholar] [CrossRef]
- Ghosh, T.S.; Das, M.; Jeffery, I.B.; O’Toole, P.W. Adjusting for age improves identification of gut microbiome alterations in multiple diseases. Elife 2020, 9, e50240. [Google Scholar] [CrossRef]
- Berendsen, A.; Santoro, A.; Pini, E.; Cevenini, E.; Ostan, R.; Pietruszka, B.; Rolf, K.; Cano, N.; Caille, A.; Lyon-Belgy, N.; et al. A parallel randomized trial on the effect of a healthful diet on inflammageing and its consequences in European elderly people: Design of the NU-AGE dietary intervention study. Mech. Ageing Dev. 2013, 134, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, T.S.; Rampelli, S.; Jeffery, I.B.; Santoro, A.; Neto, M.; Capri, M.; Giampieri, E.; Jennings, A.; Candela, M.; Turroni, S.; et al. Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: The NU-AGE 1-year dietary intervention across five European countries. Gut 2020, 69, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Rydwik, E.; Lammes, E.; Frändin, K.; Akner, G. Effects of a physical and nutritional intervention program for frail elderly people over age 75. A randomized controlled pilot treatment trial Aging Clinical and Experimental Research. Aging Clin. Exp. Res. 2008, 20, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Nakazeko, T.; Shobako, N.; Hirano, Y.; Nakamura, F.; Honda, K. Novel dietary intervention program “COMB meal program” approaching health and presenteeism: Two pilot studies. J. Funct. Foods 2022, 92, 105050. [Google Scholar] [CrossRef]
- Shobako, N.; Goto, C.; Nakagawa, T.; Yamato, T.; Kondo, S.; Nakamura, F.; Nakazeko, T.; Hirano, Y.; Honda, K. Hypotensive and HbA1c reducing effect of novel dietary intervention program “COMB meal program”: Two randomized clinical trials. J. Funct. Foods 2022, 98, 105279. [Google Scholar] [CrossRef]
- Takahashi, K. Food Frequency Questionnaire Based on Food Groups for Estimating Individual Nutrient Intake. Jpn. J. Nutr. Diet. 2003, 61, 161–169. [Google Scholar] [CrossRef]
- Iida, S.; Aoki, C. Influence of Different Measurement Orders on the Fastest Walking and Normal Walking. Rigakuryoho Kagaku 2017, 32, 81–84. [Google Scholar] [CrossRef][Green Version]
- Satake, S. Kihon checklist and frailty. Jpn. J. Geriatr. 2018, 55, 319–328. [Google Scholar]
- Satake, S.; Arai, H. Questionnaire for medical checkup of old-old (QMCOO). Geriatr. Gerontol. Int. 2020, 20, 991–992. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Nishida, A.; Matsuda, S.; Kira, F.; Watanabe, S.; Kuriyama, M.; Kawakami, K.; Aikawa, Y.; Oda, N.; Arai, K.; et al. Usefulness of Machine Learning-Based Gut Microbiome Analysis for Identifying Patients with Irritable Bowels Syndrome. J. Clin. Med. 2020, 9, 2403. [Google Scholar] [CrossRef] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Re, R.; Pellegrini, N.; Proteggente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant Activity Applying an Improved Abts Radical Cation Decolorization Assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.; Lewis, M. The size of a pilot study for a clinical trial should be calculated in relation to considerations of precision and efficiency. J. Clin. Epidemiol. 2012, 65, 301–308. [Google Scholar] [CrossRef]
- Imro’Ati, T.A.; Sugihartono, T.; Widodo, B.; Nefertiti, E.P.; Rovian, I.; Wibawa, I.G.N. The relationship between serum total oxidant status, total antioxidant status, and oxidative stress index with severity levels of gastroesophageal reflux disease: A literature review. Open Access Maced. J. Med. Sci. 2021, 9, 584–589. [Google Scholar] [CrossRef]
- Feart, C. Nutrition and frailty: Current knowledge. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 95, 109703. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Soltani, A.; Abolhassani, N.; Marques-Vidal, P.; Aminian, K.; Vollenweider, P.; Paraschiv-Ionescu, A. Real-world gait speed estimation, frailty and handgrip strength: A cohort-based study. Sci. Rep. 2021, 11, 18966. [Google Scholar] [CrossRef]
- Jennings, A.; Cashman, K.D.; Gillings, R.; Cassidy, A.; Tang, J.; Fraser, W.; Dowling, K.G.; Hull, G.L.; Berendsen, A.A.; de Groot, L.C.; et al. A Mediterranean-like dietary pattern with Vitamin D3 (10 μg/d) supplements reduced the rate of bone loss in older Europeans with osteoporosis at baseline: Results of a 1-y randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the NU-AGE diet on cognitive functioning in older adults: A randomized controlled trial. Front. Physiol. 2018, 9, 349. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in older adults-recent advances and remaining challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, Y.; Li, H.; Dai, Y.; Chen, D.; Wang, M.; Jiang, X.; Huang, Z.; Yu, H.; Huang, J.; et al. Altered Fecal Microbiota Composition in Older Adults with Frailty. Front. Cell Infect. Microbiol. 2021, 11, 696186. [Google Scholar] [CrossRef] [PubMed]
- Salli, K.; Lehtinen, M.J.; Tiihonen, K.; Ouwehand, A.C. Xylitol’s health benefits beyond dental health: A comprehensive review. Nutrients 2019, 11, 1813. [Google Scholar] [CrossRef]
- Ogawa, T.; Hirose, Y.; Honda-Ogawa, M.; Sugimoto, M.; Sasaki, S.; Kibi, M.; Kawabata, S.; Ikebe, K.; Maeda, Y. Composition of salivary microbiota in elderly subjects. Sci. Rep. 2018, 8, 414. [Google Scholar] [CrossRef]
- Kostic, A.D.; Gevers, D.; Pedamallu, C.S.; Michaud, M.; Duke, F.; Earl, A.M.; Ojesina, A.I.; Jung, J.; Bass, A.J.; Tabernero, J.; et al. Genomic analysis identifies association of Fusobacterium with colorectal carcinoma. Genome Res. 2012, 22, 292–298. [Google Scholar] [CrossRef]
- Phillips, C.M.; Shivappa, N.; Hébert, J.R.; Perry, I.J. Dietary inflammatory index and mental health: A cross-sectional analysis of the relationship with depressive symptoms, anxiety and well-being in adults. Clin. Nutr. 2018, 37, 1485–1491. [Google Scholar] [CrossRef]
- Yelverton, C.A.; Rafferty, A.A.; Moore, R.L.; Byrne, D.F.; Mehegan, J.; Cotter, P.D.; Van Sinderen, D.; Murphy, E.F.; Killeen, S.L.; McAuliffe, F.M. Diet and mental health in pregnancy: Nutrients of importance based on large observational cohort data. Nutrition 2022, 96, 111582. [Google Scholar] [CrossRef]
- Ugartemendia, L.; Bravo, R.; Castaño, M.Y.; Cubero, J.; Zamoscik, V.; Kirsch, P.; Rodriguez, A.B.; Reuter, M. Influence of diet on mood and social cognition: A pilot study. Food Funct. 2020, 11, 8320–8330. [Google Scholar] [CrossRef]
- Saum, K.-U.; Dieffenbach, A.K.; Jansen, E.H.; Schöttker, B.; Holleczek, B.; Hauer, K.; Brenner, H. Association between Oxidative Stress and Frailty in an Elderly German Population: Results from the ESTHER Cohort Study. Gerontology 2015, 61, 407–415. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Nutritional Regulations | /500 kcal | ||
|---|---|---|---|
| Lower Limit | Upper Limit | ||
| Protein | g | 23.2 | 25.0 |
| Fat | g | 11.1 | 16.7 |
| Saturated fatty acids | g | 3.9 | |
| Carbohydrate | g | 62.5 | 81.3 |
| Fiber | g | 7.5 | |
| K | mg | 893 | |
| Ca | mg | 268 | 424 |
| Mg | mg | 132 | |
| P | mg | 357 | 509 |
| Ir | mg | 2.7 | 8.5 |
| Zn | mg | 3.9 | 7.3 |
| Cu | mg | 0.32 | 1.19 |
| Mn | mg | 1.43 | 1.86 |
| I | μg | 46 | 509 |
| Se | μg | 11 | 76 |
| Cr | μg | 4 | 85 |
| Mo | μg | 11 | 102 |
| RAE | μg | 321 | 458 |
| VD | μg | 3.6 | 16.9 |
| αTOC | mg | 2.5 | 144.1 |
| VK | μg | 54 | |
| VB1 | mg | 0.46 | |
| VB2 | mg | 0.54 | |
| Nia | mg | 5.0 | |
| VB6 | mg | 0.54 | 9.09 |
| VB12 | μg | 0.9 | |
| FA | μg | 86 | |
| PA | mg | 2.14 | |
| Biotin | μg | 17.9 | |
| VC | mg | 36 | |
| n6FA | g | 3.6 | |
| n3FA | g | 0.9 | |
| Salt equivalent | g | <3.0 | |
| Ile | mg | 486 | |
| Leu | mg | 947 | |
| Lys | mg | 729 | |
| Sulphur-containing amino acid | mg | 364 | |
| Aromatic amino acid | mg | 607 | |
| Thr | mg | 364 | |
| Trp | mg | 97 | |
| Val | mg | 631 | |
| His | mg | 243 | |
| Content | Unit | Amount | Content | Unit | Amount | Content | Unit | Amount |
|---|---|---|---|---|---|---|---|---|
| Energy | kcal | 483 | Se | μg | 33 | Biotin | μg | 17.4 |
| Protein | g | 24.0 | Cr | μg | 3 | VC | mg | 36 |
| Fat | g | 15.7 | Mo | μg | 30 | n6FA | g | 3.5 |
| Saturated fatty acids | g | 3.0 | RAE | μg | 317 | n3FA | g | 1.6 |
| Carbohydrate | g | 61.3 | VD | μg | 10.1 | Salt equivalent | g | 2.2 |
| Fiber | g | 8.3 | αTOC | mg | 2.7 | Ile | mg | 1005 |
| K | mg | 863 | VK | μg | 52 | Leu | mg | 1797 |
| Ca | mg | 259 | VB1 | mg | 0.46 | Lys | mg | 1767 |
| Mg | mg | 128 | VB2 | mg | 0.53 | Sulphur-containing amino acid | mg | 991 |
| P | mg | 362 | Nia | mg | 12.3 | Aromatic amino acid | mg | 1839 |
| Ir | mg | 3.6 | VB6 | mg | 0.52 | Thr | mg | 1028 |
| Zn | mg | 3.8 | VB12 | μg | 3.5 | Trp | mg | 292 |
| Cu | mg | 0.31 | FA | μg | 83 | Val | mg | 1229 |
| Mn | mg | 1.38 | PA | mg | 2.07 | His | mg | 856 |
| I | μg | 45 |
| Unit | Control | Test | p | |||||
|---|---|---|---|---|---|---|---|---|
| Male: Female | 28 | : | 27 | 27 | : | 28 | ||
| Frailty: Pre-frailty | 49 | : | 6 | 48 | : | 7 | ||
| Age | years | 64.9 | ± | 3.7 | 64.9 | ± | 3.8 | 0.980 |
| Grip strength | kg | 28.7 | ± | 9.0 | 27.7 | ± | 8.3 | 0.532 |
| Leg strength | kg | 31.0 | ± | 11.6 | 29.1 | ± | 10.5 | 0.374 |
| Walk speed | m/s | 1.39 | ± | 0.21 | 1.37 | ± | 0.19 | 0.500 |
| Bone density | % | 26.6 | ± | 3.4 | 26.9 | ± | 3.4 | 0.687 |
| MPI score | point | 66.4 | ± | 7.6 | 66.3 | ± | 7.9 | 0.929 |
| Energy intake | kcal/day | 1984.0 | ± | 559.1 | 2004.1 | ± | 499.9 | 0.843 |
| Protein intake | g/day | 70.1 | ± | 23.9 | 71.5 | ± | 24.3 | 0.766 |
| Body muscle mass | kg | 41.0 | ± | 7.7 | 41.1 | ± | 8.2 | 0.979 |
| Body muscle ratio | % | 66.1 | ± | 7.6 | 66.4 | ± | 7.1 | 0.861 |
| Trunk muscle mass | kg | 19.3 | ± | 3.8 | 19.2 | ± | 4.1 | 0.871 |
| Right arm muscle mass | kg | 2.2 | ± | 0.6 | 2.2 | ± | 0.7 | 0.933 |
| Left arm muscle mass | kg | 2.2 | ± | 0.6 | 2.1 | ± | 0.6 | 0.736 |
| Right leg muscle mass | kg | 6.8 | ± | 1.5 | 6.9 | ± | 1.6 | 0.909 |
| Left leg muscle mass | kg | 6.8 | ± | 1.5 | 6.8 | ± | 1.5 | 0.998 |
| Modified J-CHS score | point | 1.9 | ± | 0.7 | 1.8 | ± | 0.7 | 0.582 |
| Height | cm | 162.2 | ± | 7.9 | 163.0 | ± | 8.5 | 0.593 |
| Body weight | kg | 62.3 | ± | 10.7 | 62.0 | ± | 11.5 | 0.910 |
| BMI | kg/m2 | 23.6 | ± | 3.4 | 23.2 | ± | 3.0 | 0.489 |
| Body fat rate | % | 29.9 | ± | 8.0 | 29.6 | ± | 7.4 | 0.826 |
| SBP | mmHg | 133.3 | ± | 15.7 | 135.2 | ± | 13.7 | 0.491 |
| DBP | mmHg | 80.3 | ± | 9.3 | 77.9 | ± | 10.1 | 0.189 |
| Pulse rate | beats/min | 75.3 | ± | 10.9 | 72.3 | ± | 9.8 | 0.139 |
| TG | mg/dL | 92.4 | ± | 48.1 | 104.5 | ± | 70.2 | 0.294 |
| HDL-C | mg/dL | 67.9 | ± | 15.7 | 72.2 | ± | 20.5 | 0.223 |
| LDL-C | mg/dL | 130.6 | ± | 26.1 | 133.6 | ± | 30.5 | 0.581 |
| Non-HDL-C | mg/dL | 147.7 | ± | 28.8 | 151.4 | ± | 34.4 | 0.535 |
| Fasting blood glucose | mg/dL | 90.1 | ± | 8.7 | 88.2 | ± | 7.3 | 0.214 |
| HbA1c | % | 5.5 | ± | 0.3 | 5.5 | ± | 0.4 | 0.279 |
| Physical function | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| 95% CI | |||||||||||
| Grip strength | kg | Control | 50 | 29.3 | ± | 9.5 | 30.3 | ± | 8.9 | 0.3 | 0.607 |
| Test | 43 | 28.1 | ± | 9.0 | 29.4 | ± | 9.1 | (−0.8~1.3) | |||
| Leg strength | kg | Control | 46 | 34.7 | ± | 11.7 | 33.5 | ± | 13.3 | 1.4 | 0.387 |
| Test | 39 | 33.5 | ± | 11.5 | 33.7 | ± | 12.1 | (−1.8~4.6) | |||
| Walk speed | m/s | Control | 50 | 1.42 | ± | 0.17 | 1.39 | ± | 0.16 | 0.06 | 0.019 |
| Test | 43 | 1.38 | ± | 0.16 | 1.42 | ± | 0.14 | (0.01~0.12) | |||
| Bone density | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| 95% CI | |||||||||||
| Bone density | % | Control | 50 | 26.4 | ± | 3.3 | 26.7 | ± | 3.4 | 0.0 | 0.943 |
| Test | 43 | 26.8 | ± | 3.3 | 27.0 | ± | 3.4 | (−0.7~0.7) | |||
| Cognitive function | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| 95% CI | |||||||||||
| MPI score | point | Control | 49 | 65.8 | ± | 7.2 | 66.4 | ± | 7.3 | 2.4 | 0.038 |
| Test | 43 | 65.0 | ± | 7.4 | 68.1 | ± | 6.9 | - | |||
| WHO-5 | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| 95% CI | |||||||||||
| Total score | point | Control | 50 | 15.4 | ± | 4.3 | 16.1 | ± | 3.5 | 1.6 | 0.027 |
| Test | 43 | 14.3 | ± | 4.3 | 16.6 | ± | 3.4 | - | |||
| Q1 | point | Control | 50 | 3.0 | ± | 1.0 | 3.3 | ± | 0.9 | 0.2 | 0.264 |
| Test | 43 | 3.0 | ± | 1.0 | 3.4 | ± | 0.8 | - | |||
| Q2 | point | Control | 50 | 3.3 | ± | 0.8 | 3.5 | ± | 0.8 | 0.3 | 0.073 |
| Test | 43 | 3.2 | ± | 0.9 | 3.6 | ± | 0.8 | - | |||
| Q3 | point | Control | 50 | 3.1 | ± | 1.1 | 3.2 | ± | 0.9 | 0.5 | 0.013 |
| Test | 43 | 2.7 | ± | 1.0 | 3.3 | ± | 0.9 | - | |||
| Q4 | point | Control | 50 | 3.2 | ± | 1.1 | 3.2 | ± | 1.1 | 0.4 | 0.040 |
| Test | 43 | 2.8 | ± | 1.1 | 3.2 | ± | 0.9 | - | |||
| Q5 | point | Control | 50 | 2.8 | ± | 1.2 | 3.0 | ± | 0.8 | 0.2 | 0.337 |
| Test | 43 | 2.7 | ± | 1.2 | 3.1 | ± | 0.9 | - | |||
| Occupancy of gut flora | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| Genus | 95% CI | ||||||||||
| Blautia | % | Control | 48 | 5.3 | ± | 2.8 | 5.4 | ± | 2.7 | 1.2 | 0.029 |
| Test | 41 | 5.2 | ± | 2.7 | 6.5 | ± | 3.3 | - | |||
| Anaerostipes | % | Control | 48 | 1.7 | ± | 1.6 | 1.7 | ± | 1.5 | 0.7 | 0.008 |
| Test | 41 | 1.4 | ± | 2.0 | 2.1 | ± | 2.2 | - | |||
| Fusobacterium | % | Control | 48 | 0.8 | ± | 2.4 | 1.1 | ± | 3.2 | −0.6 | 0.037 |
| Test | 41 | 1.1 | ± | 2.7 | 0.7 | ± | 1.9 | - | |||
| Bifidobacterium | % | Control | 48 | 4.0 | ± | 3.9 | 3.7 | ± | 4.2 | −0.3 | 0.556 |
| Test | 41 | 3.8 | ± | 3.8 | 3.2 | ± | 3.6 | - | |||
| Faecalibacterium | % | Control | 48 | 4.6 | ± | 3.3 | 5.2 | ± | 3.1 | −0.4 | 0.397 |
| Test | 41 | 5.3 | ± | 3.3 | 5.5 | ± | 3.5 | - | |||
| Antioxidant activity | unit | n | Week 0 | Week 12 | ⊿ | p | |||||
| 95% CI | |||||||||||
| STAS | μM | Control | 50 | 1380.6 | ± | 160.8 | 1371.5 | ± | 148.1 | 53.2 | 0.003 |
| Test | 43 | 1325.3 | ± | 151.9 | 1369.3 | ± | 148.2 | (18.2~88.1) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakazeko, T.; Shobako, N.; Shioya, N.; Iwama, Y.; Hirano, Y.; Fujii, S.; Nakamura, F.; Honda, K. Frailty-Preventing Effect of an Intervention Program Using a Novel Complete Nutritional “COMB-FP Meal”: A Pilot Randomized Control Trial. Nutrients 2023, 15, 4317. https://doi.org/10.3390/nu15204317
Nakazeko T, Shobako N, Shioya N, Iwama Y, Hirano Y, Fujii S, Nakamura F, Honda K. Frailty-Preventing Effect of an Intervention Program Using a Novel Complete Nutritional “COMB-FP Meal”: A Pilot Randomized Control Trial. Nutrients. 2023; 15(20):4317. https://doi.org/10.3390/nu15204317
Chicago/Turabian StyleNakazeko, Takuo, Naohisa Shobako, Nobuhiko Shioya, Yoshitaka Iwama, Yukio Hirano, Shintaro Fujii, Futoshi Nakamura, and Keiko Honda. 2023. "Frailty-Preventing Effect of an Intervention Program Using a Novel Complete Nutritional “COMB-FP Meal”: A Pilot Randomized Control Trial" Nutrients 15, no. 20: 4317. https://doi.org/10.3390/nu15204317
APA StyleNakazeko, T., Shobako, N., Shioya, N., Iwama, Y., Hirano, Y., Fujii, S., Nakamura, F., & Honda, K. (2023). Frailty-Preventing Effect of an Intervention Program Using a Novel Complete Nutritional “COMB-FP Meal”: A Pilot Randomized Control Trial. Nutrients, 15(20), 4317. https://doi.org/10.3390/nu15204317