
Water-Soluble Vitamins Status in Patients Undergoing Maintenance Hemodialysis


 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Anthropometric Measurements
2.3. Biochemistry
2.4. Analysis of Water-Soluble Vitamins with the HPLC Method
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Populations
3.2. Biochemical Parameters
3.3. Blood Concentration of Water-Soluble Vitamins
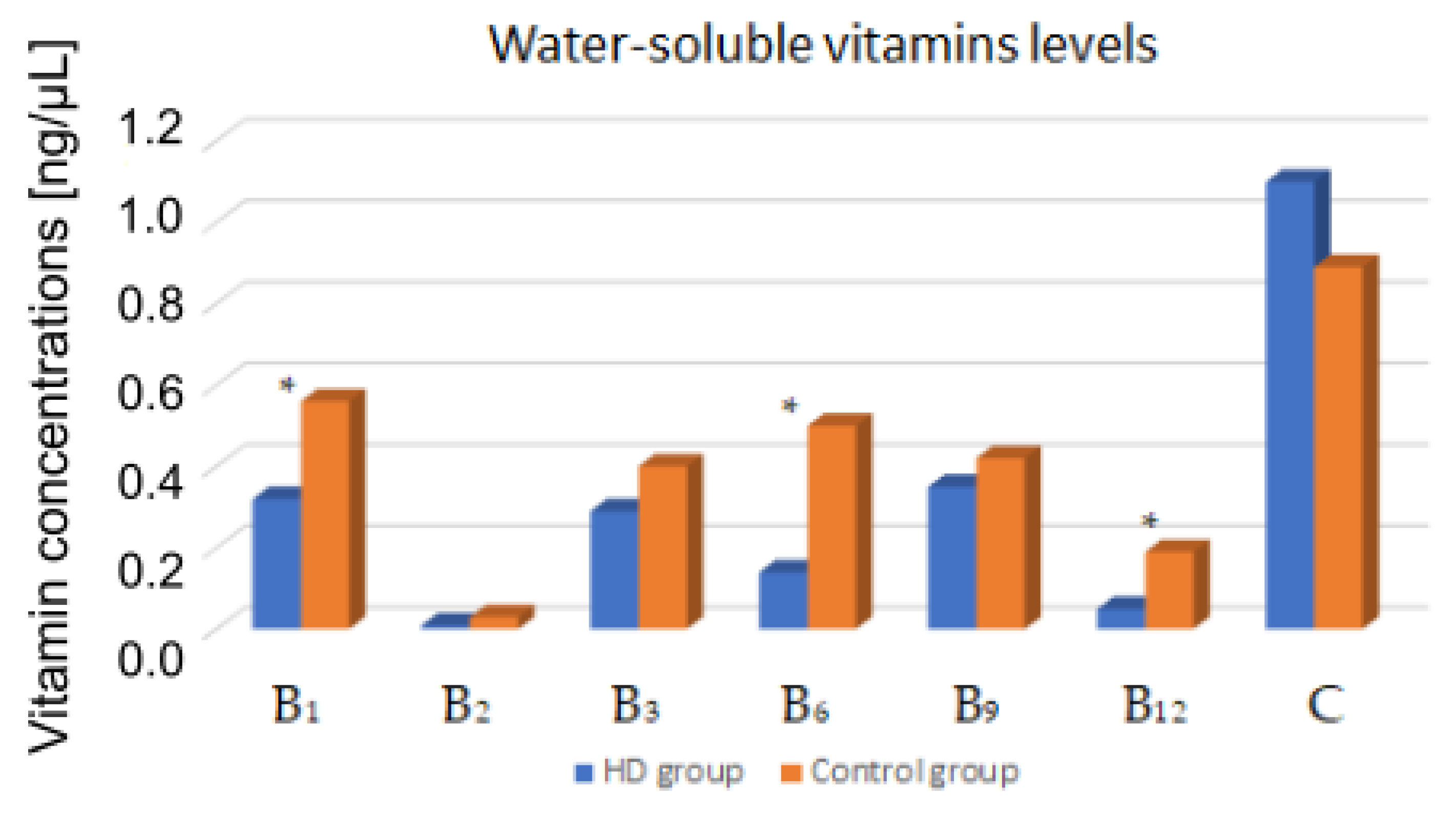
3.3.1. HD Patients vs. Control Group
3.3.2. Multivariate Regression
3.3.3. HD Patients with and without DM
4. Discussion
5. Conclusions
6. Clinical Implication
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sabatino, A.; Regolisti, G.; Karupaiah, T.; Sahathevan, S.; Sadu Singh, B.K.; Khor, B.H.; Salhab, N.; Karavetian, M.; Cupisti, A.; Fiaccadori, E. Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis. Clin. Nutr. 2017, 36, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Clase, C.M.; Ki, V.; Holden, R.M. Water-soluble vitamins in people with low glomerular filtration rate or on dialysis: A review. Semin. Dial. 2013, 26, 546–567. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Clark, W.R. Haemodialysis membranes. Nat. Rev. Nephrol. 2018, 14, 394–410. [Google Scholar] [CrossRef]
- Jankowska, M.; Lichodziejewska-Niemierko, M.; Rutkowski, B.; Dębska-Ślizień, A.; Małgorzewicz, S. Water soluble vitamins and peritoneal dialysis—State of the art. Clin. Nutr. 2017, 36, 1483–1489. [Google Scholar] [CrossRef]
- Lasseur, C.; Parrot, F.; Delmas, Y.; Level, C.; Ged, C.; Redonnet-Vernhet, I.; Montaudon, D.; Combe, C.; Chauveau, P. Impact of high-flux/high-efficiency dialysis on folate and homocysteine metabolism. J. Nephrol. 2001, 14, 32–35. [Google Scholar] [PubMed]
- Heinz, J.; Domröse, U.; Westphal, S.; Luley, C.; Neumann, K.H.; Dierkes, J. Washout of water-soluble vitamins and of homocysteine during haemodialysis: Effect of high-flux and low-flux dialyser membranes. Nephrology 2008, 13, 384–389. [Google Scholar] [CrossRef]
- Coveney, N.; Polkinghorne, K.R.; Linehan, L.; Corradini, A.; Kerr, P.G. Water-soluble vitamin levels in extended hours hemodialysis. Hemodial. Int. 2011, 15, 30–38. [Google Scholar] [CrossRef]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Fissell, R.B.; Bragg-Gresham, J.L.; Gillespie, B.W.; Goodkin, D.A.; Bommer, J.; Saito, A.; Akiba, T.; Port, F.K.; Young, E.W. International Variation in Vitamin Prescription and Association with Mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2004, 44, 293–299. [Google Scholar] [CrossRef]
- Mataix, J.; Aranda, P.; Sánchez, C.; Montellano, M.A.; Planells, E.; Llopis, J. Assessment of thiamin (vitamin B1) and riboflavin (vitamin B2) status in an adult Mediterranean population. Br. J. Nutr. 2003, 90, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Nowak, P.J.; Wilk, R.; Prymont-Przyminska, A.; Zwolinska, A.; Sarniak, A.; Wlodarczyk, A.; de Graft-Johnson, J.; Mamelka, B.; Zasowska-Nowak, A.; Bartnicki, P.; et al. Hemodialysis Decreases the Concentration of Accumulated Plant Phenols in the Plasma of Patients on Maintenance Dialysis: Influence of Residual Renal Function. Ther. Apher. Dial. 2017, 21, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Zahan, M.S.; Ahmed, K.A.; Moni, A.; Sinopoli, A.; Ha, H.; Uddin, M.J. Kidney protective potential of lactoferrin: Pharmacological insights and therapeutic advances. Korean J. Physiol. Pharmacol. 2022, 26, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Zapata, R.C.; Pezeshki, A.; Knight, C.G.; Tuor, U.I.; Chelikani, P.K. Whey Protein and Its Components Lactalbumin and Lactoferrin Affect Energy Balance and Protect against Stroke Onset and Renal Damage in Salt-Loaded, High-Fat Fed Male Spontaneously Hypertensive Stroke-Prone Rats. J. Nutr. 2020, 150, 763–774. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.H.; Chiu, I.J.; Lin, Y.F.; Chen, Y.J.; Lee, Y.H.; Chiu, H.W. Lactoferrin Contributes a Renoprotective Effect in Acute Kidney Injury and Early Renal Fibrosis. Pharmaceutics 2020, 12, 434. [Google Scholar] [CrossRef]
- Deshmukh, S.V.; Prabhakar, B.; Kulkarni, Y.A. Water Soluble Vitamins and their Role in Diabetes and its Complications. Curr. Diabetes Rev. 2020, 16, 649–656. [Google Scholar] [CrossRef]
- Xiong, R.; Yuan, Y.; Zhu, Z.; Wu, Y.; Ha, J.; Han, X.; Wang, W.; He, M. Micronutrients and Diabetic Retinopathy: Evidence From The National Health and Nutrition Examination Survey and a Meta-analysis. Am. J. Ophthalmol. 2022, 238, 141–156. [Google Scholar] [CrossRef]
- Daugirdas, J.T. The post: Pre-dialysis plasma urea nitrogen ratio to estimate K.t/V and NPCR: Mathematical modeling. Int. J. Artif. Organs 1989, 12, 411–419. [Google Scholar] [PubMed]
- Said, H.M. Water-soluble vitamins. World Rev. Nutr. Diet. 2015, 111, 30–37. [Google Scholar] [CrossRef]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B Vitamins and One-Carbon Metabolism: Implications in Human Health and Disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef]
- Hrubša, M.; Siatka, T.; Nejmanová, I.; Vopršalová, M.; Kujovská Krčmová, L.; Matoušová, K.; Javorská, L.; Macáková, K.; Mercolini, L.; Remião, F.; et al. Biological Properties of Vitamins of the B-Complex, Part 1: Vitamins B1, B2, B3, and B5. Nutrients 2022, 14, 484. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hong, S.Y.; Yang, D.H.; Chang, S.K. Plasma homocysteine, vitamin B6, vitamin B12 and folic acid in end-stage renal disease during low-dose supplementation with folic acid. Am. J. Nephrol. 1998, 18, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.; Sperschneider, H.; Koppe, S. Vitamin levels in chronic renal failure and need for supplementation. Blood Purif. 1985, 3, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Bévier, A.; Novel-Catin, E.; Blond, E.; Pelletier, S.; Parant, F.; Koppe, L.; Fouque, D. Water-Soluble Vitamins and Trace Elements Losses during On-Line Hemodiafiltration. Nutrients 2022, 14, 3454. [Google Scholar] [CrossRef] [PubMed]
- Schwotzer, N.; Kanemitsu, M.; Kissling, S.; Darioli, R.; Benghezal, M.; Rezzi, S.; Burnier, M.; Pruijm, M. Water-Soluble Vitamin Levels and Supplementation in Chronic Online Hemodiafiltration Patients. Kidney Int. Rep. 2020, 5, 2160–2167. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.L. Thiamin in Clinical Practice. J. Parenter. Enteral. Nutr. 2015, 39, 503–520. [Google Scholar] [CrossRef]
- Jankowska, M.; Rudnicki-Velasquez, P.; Storoniak, H.; Rutkowski, P.; Rutkowski, B.; Krzymiński, K.; Dębska-Ślizień, A. Thiamine Diphosphate Status and Dialysis-Related Losses in End-Stage Kidney Disease Patients Treated with Hemodialysis. Blood Purif. 2017, 44, 294–300. [Google Scholar] [CrossRef]
- Nakatani-Enomoto, S.; Moriya, A.; Kikuchi, S.; Mochizuki, H.; Sugiura, Y.; Ugawa, Y. Wernicke encephalopathy in a non-alcoholic patient with diabetic nephropathy under hemodialysis. Rinsho Shinkeigaku 2010, 50, 409–411. [Google Scholar] [CrossRef]
- Ueda, K.; Takada, D.; Mii, A.; Tsuzuku, Y.; Saito, S.K.; Kaneko, T.; Utsumi, K.; Iino, Y.; Katayama, Y. Severe thiamine deficiency resulted in Wernicke’s encephalopathy in a chronic dialysis patient. Clin. Exp. Nephrol. 2006, 10, 290–293. [Google Scholar] [CrossRef]
- Pácal, L.; Kuricová, K.; Kaňková, K. Evidence for altered thiamine metabolism in diabetes: Is there a potential to oppose gluco- and lipotoxicity by rational supplementation? World J. Diabetes 2014, 5, 288–295. [Google Scholar] [CrossRef]
- Raval, A.D.; Thakker, D.; Rangoonwala, A.N.; Gor, D.; Walia, R. Vitamin B and its derivatives for diabetic kidney disease. Cochrane Database Syst. Rev. 2015, 1, CD009403. [Google Scholar] [CrossRef] [PubMed]
- Hammes, H.P.; Du, X.; Edelstein, D.; Taguchi, T.; Matsumura, T.; Ju, Q.; Lin, J.; Bierhaus, A.; Nawroth, P.; Hannak, D.; et al. Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nat. Med. 2003, 9, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, A.; Barutta, F.; Bellucci, L.; Trento, M.; Gruden, G.; Porta, M.; Beltramo, E. Reduced Thiamine Availability and Hyperglycemia Impair Thiamine Transport in Renal Glomerular Cells through Modulation of Thiamine Transporter 2. Biomedicines 2021, 9, 385. [Google Scholar] [CrossRef] [PubMed]
- Beltramo, E.; Mazzeo, A.; Porta, M. Thiamine and diabetes: Back to the future? Acta Diabetol. 2021, 58, 1433–1439. [Google Scholar] [CrossRef]
- Jankowska, M.; Szupryczyńska, N.; Dębska-Ślizień, A.; Borek, P.; Kaczkan, M.; Rutkowski, B.; Małgorzewicz, S. Dietary Intake of Vitamins in Different Options of Treatment in Chronic Kidney Disease: Is There a Deficiency? Transplant. Proc. 2016, 48, 1427–1430. [Google Scholar] [CrossRef]
- Bossola, M.; Di Stasio, E.; Viola, A.; Leo, A.; Carlomagno, G.; Monteburini, T.; Cenerelli, S.; Santarelli, S.; Boggi, R.; Miggiano, G.; et al. Dietary intake of trace elements, minerals, and vitamins of patients on chronic hemodialysis. Int. Urol. Nephrol. 2014, 46, 809–815. [Google Scholar] [CrossRef]
- Ramirez, G.; Chen, M.; Boyce, H.W.; Fuller, S.M.; Butcher, D.E.; Brueggemeyer, C.D.; Newton, J.L. The plasma and red cell vitamin B levels of chronic hemodialysis patients: A longitudinal study. Nephron 1986, 42, 41–46. [Google Scholar] [CrossRef]
- Lenglet, A.; Liabeuf, S.; Guffroy, P.; Fournier, A.; Brazier, M.; Massy, Z.A. Use of nicotinamide to treat hyperphosphatemia in dialysis patients. Drugs R D 2013, 13, 165–173. [Google Scholar] [CrossRef]
- Stach, K.; Stach, W.; Augoff, K. Vitamin B6 in Health and Disease. Nutrients 2021, 13, 3229. [Google Scholar] [CrossRef]
- Nix, W.A.; Zirwes, R.; Bangert, V.; Kaiser, R.P.; Schilling, M.; Hostalek, U.; Obeid, R. Vitamin B status in patients with type 2 diabetes mellitus with and without incipient nephropathy. Diabetes Res. Clin. Pract. 2015, 107, 157–165. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Wang, A.Y. Vitamin B12 and chronic kidney disease. Vitam. Horm. 2022, 119, 325–353. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Cappuccilli, M.L.; Magnoni, G.; Croci Chiocchini, A.L.; Aiello, V.; Napoletano, A.; Iacovella, F.; Troiano, A.; Mancini, R.; Capelli, I.; et al. The link between homocysteine, folic acid and vitamin B12 in chronic kidney disease. G. Ital. Nefrol. 2021, 38, 1–17. [Google Scholar] [PubMed]
- Crews, D.C.; Kuczmarski, M.F.; Miller, E.R.; Zonderman, A.B.; Evans, M.K.; Powe, N.R. Dietary habits, poverty, and chronic kidney disease in an urban population. J. Ren. Nutr. 2015, 25, 103–110. [Google Scholar] [CrossRef]
- Descombes, E.; Hanck, A.B.; Fellay, G. Water soluble vitamins in chronic hemodialysis patients and need for supplementation. Kidney Int. 1993, 43, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Morena, M.; Cristol, J.P.; Bosc, J.Y.; Tetta, C.; Forret, G.; Leger, C.L.; Delcourt, C.; Papoz, L.; Descomps, B.; Canaud, B. Convective and diffusive losses of vitamin C during haemodiafiltration session: A contributive factor to oxidative stress in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 422–427. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | HD Patients n = 142 | Control Group n = 31 |
|---|---|---|
| Female/Man | 57/85 | 16/15 |
| Female/Man (%) | 40.1/59.9 | 51.6/48.4 |
| Age (years) range | 64 ± 15.2 (66) 21–97 | 41.1 ± 10 (38) 30–72 |
| BMI (kg/m2) | 25.1 ± 6.5 (24.6) | 26.6 ± 4.1 |
| Dialysis vintage (months) | 51.6 ± 54.2 (33) | - |
| Kt/V | 1.65 ± 0.33 (1.67) | - |
| nPCR (g/kg/day) | 1.08 ± 0.24 | - |
| Common causes of CKD | ||
| Unknown nephropathy (%) | 19.1 | |
| Diabetic nephropathy (%) | 15.6 | |
| Chronic glomerulonephritis (%) | 14.5 | |
| Hypertensive nephropathy (%) | 5.2 | |
| Chronic pyelonephritis (%) | 5.2 | |
| Polycystic kidney disease (%) | 4.1 |
| Parameters | HD Patients n = 142 | References Values |
|---|---|---|
| Hemoglobin (g/dL) | 10.7 ± 1.3 (10.7) | 9.5–12.5 |
| Albumin (g/L) | 35.6 ± 3.9 (36) | 38–48 |
| BUN before HD (mg/dL) | 57.4 ± 12.6 | 8.4–25.7 |
| BUN after HD (mg/dL) | 14.6 ± 4.5 (13.5) | 8.4–25.7 |
| Sodium (mmol/L) | 137.1 ± 2.9 | 136–145 |
| Potassium (mmol/L) | 5.3 ± 0.6 | 3.5–5.1 |
| Calcium (mg/dL) | 8.5 ± 0.9 (8.5) | 8.9–10 |
| Phosphorus (mg/dL) | 5.1 ± 1.3 | 2.3–4.7 |
| Vitamin | HD Patients n = 142 | Control Group n = 31 | p |
|---|---|---|---|
| B1—thiamine (ng/μL) | 0.32 ± 0.34 (0.15) | 0.56 ± 0.38 | <0.001 |
| B2—riboflavin (ng/μL) | 0.009 ± 0.007 (0.006) | 0.03 ± 0.03 (0.008) | 0.17 |
| B3—niacin (ng/μL) | 0.29 ± 0.21 (0.32) | 0.4 ± 0.38 (0.54) | 0.12 |
| B6—pyridoxine (ng/μL) | 0.14 ± 0.16 (0.08) | 0.5 ± 0.26 | <0.001 |
| B9—folic acid (ng/μL) | 0.35 ± 0.34 (0.19) | 0.42 ± 0.28 | 0.13 |
| B12—cobalamin (ng/μL) | 0.05 ± 0.04 (0.03) | 0.19 ± 0.17 (0.13) | <0.001 |
| C—ascorbic acid (ng/μL) | 1.1 ± 0.79 (0.88) | 0.89 ± 0.22 (0.93) | 0.69 |
| Regression Model | B | Standard Error | Beta | p-Value |
|---|---|---|---|---|
| Vitamin B1 concentration | ||||
| Constant | −1.3 | 0.51 | 0.02 | |
| Kt/V | 1.91 | 0.49 | 1.84 | <0.001 |
| nPCR | −5.25 | 1.21 | −3.96 | <0.001 |
| BUN before HD | 0.07 | 0.02 | 3.26 | <0.001 |
| Vitamin B9 concentration | ||||
| Constant | −2.15 | 1.04 | 0.049 | |
| Kt/V | 1.9 | 0.77 | 1.41 | 0.02 |
| nPCR | −4.93 | 1.91 | −2.78 | 0.02 |
| BUN before HD | 0.06 | 0.03 | 2.39 | 0.02 |
| Albumin | 0.03 | 0.02 | 0.25 | 0.16 |
| Vitamin | HD Patients with DM n = 55 | HD Patients without DM n = 87 | p |
|---|---|---|---|
| B1—thiamine (ng/μL) | 0.24 ± 0.28 (0.09) | 0.36 ± 0.37 (0.28) | 0.04 |
| B2—riboflavin (ng/μL) | 0.009 ± 0.008 (0.006) | 0.009 ± 0.006 (0.007) | 0.59 |
| B3—niacin (ng/μL) | 0.28 ± 0.22 (0.31) | 0.29 ± 0.21 (0.35) | 0.7 |
| B6—pyridoxine (ng/μL) | 0.15 ± 0.15 (0.09) | 0.14 ± 0.17 (0.07) | 0.44 |
| B9—folic acid (ng/μL) | 0.31 ± 0.34 (0.12) | 0.39 ± 0.34 (0.28) | 0.16 |
| B12—cobalamin (ng/μL) | 0.04 ± 0.02 (0.03) | 0.05 ± 0.04 (0.04) | 0.72 |
| C—ascorbic acid (ng/μL) | 1.1 ± 0.91 (0.83) | 1.1 ± 0.71 (0.98) | 0.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaczkan, M.; Czaja-Stolc, S.; Szczuko, M.; Drozd, A.; Rutkowski, P.; Dębska-Ślizień, A.; Małgorzewicz, S. Water-Soluble Vitamins Status in Patients Undergoing Maintenance Hemodialysis. Nutrients 2023, 15, 440. https://doi.org/10.3390/nu15020440
Kaczkan M, Czaja-Stolc S, Szczuko M, Drozd A, Rutkowski P, Dębska-Ślizień A, Małgorzewicz S. Water-Soluble Vitamins Status in Patients Undergoing Maintenance Hemodialysis. Nutrients. 2023; 15(2):440. https://doi.org/10.3390/nu15020440
Chicago/Turabian StyleKaczkan, Małgorzata, Sylwia Czaja-Stolc, Małgorzata Szczuko, Arleta Drozd, Przemysław Rutkowski, Alicja Dębska-Ślizień, and Sylwia Małgorzewicz. 2023. "Water-Soluble Vitamins Status in Patients Undergoing Maintenance Hemodialysis" Nutrients 15, no. 2: 440. https://doi.org/10.3390/nu15020440
APA StyleKaczkan, M., Czaja-Stolc, S., Szczuko, M., Drozd, A., Rutkowski, P., Dębska-Ślizień, A., & Małgorzewicz, S. (2023). Water-Soluble Vitamins Status in Patients Undergoing Maintenance Hemodialysis. Nutrients, 15(2), 440. https://doi.org/10.3390/nu15020440