
Brazilian Propolis Intake Decreases Body Fat Mass and Oxidative Stress in Community-Dwelling Elderly Females: A Randomized Placebo-Controlled Trial

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
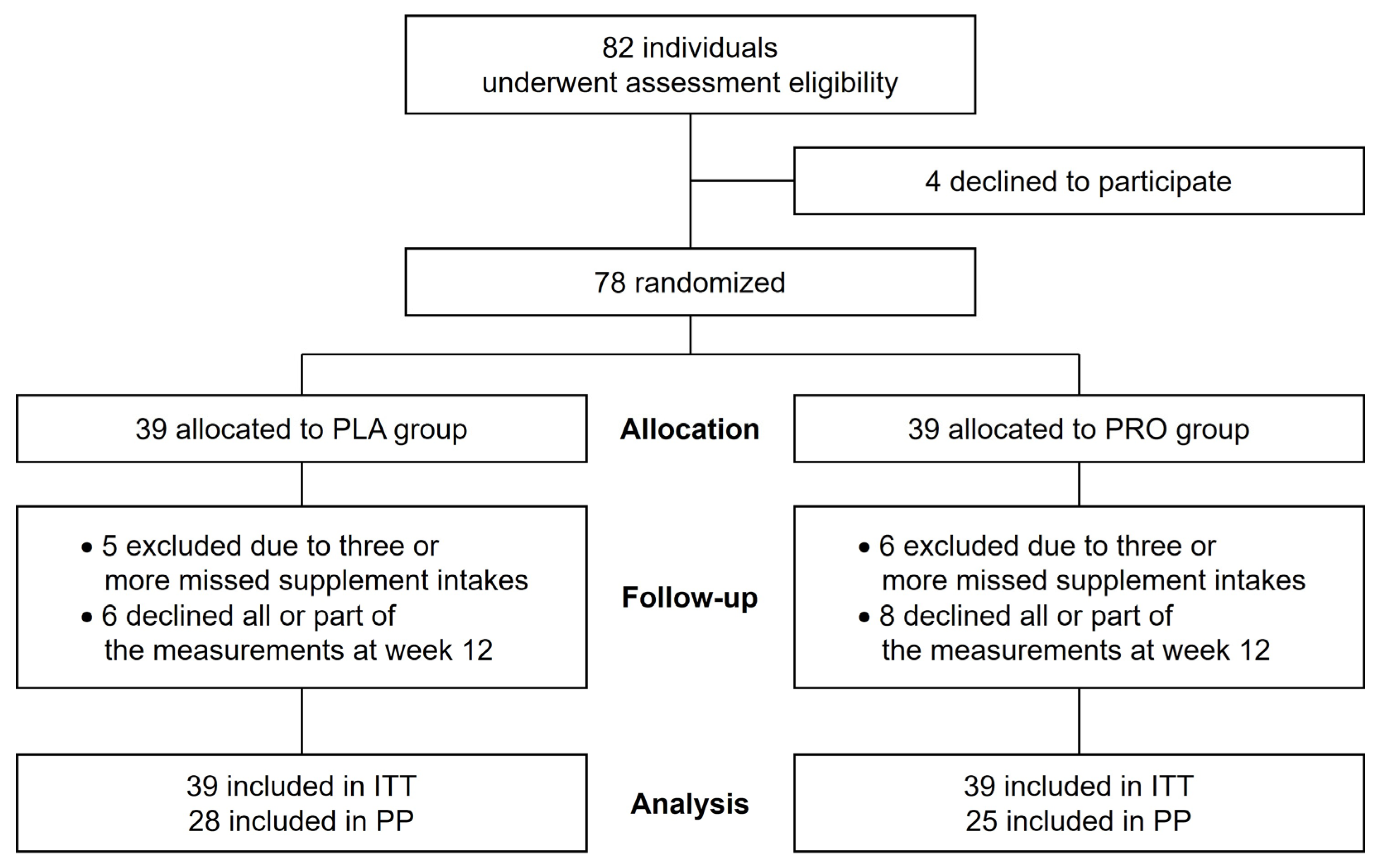
2.1. Participants
2.2. Study Design
2.3. Brazilian Propolis Supplementation
2.4. Assessment Procedures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kozakowski, J.; Gietka-Czernel, M.; Leszczynska, D.; Majos, A. Obesity in menopause—Our negligence or an unfortunate inevitability? Przegląd Menopauzalny 2017, 16, 61–65. [Google Scholar] [CrossRef]
- Donato, G.B.; Fuchs, S.C.; Oppermann, K.; Bastos, C.; Spritzer, P.M. Association between menopause status and central adiposity measured at different cutoffs of waist circumference and waist-to-hip ratio. Menopause 2006, 13, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Fukuo, K.; Suzuki, K.; Yoshino, G.; Kazumi, T. Relationships of systemic oxidative stress to body fat distribution, adipokines and inflammatory markers in healthy middle-aged women. Endocr. J. 2009, 56, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Fantuzzi, G. Adipose tissue, adipokines, and inflammation. J. Allergy Clin. Immunol. 2005, 115, 911–919. [Google Scholar] [CrossRef]
- Weyer, C.; Funahashi, T.; Tanaka, S.; Hotta, K.; Matsuzawa, Y.; Pratley, R.E.; Tataranni, P.A. Hypoadiponectinemia in obesity and type 2 diabetes: Close association with insulin resistance and hyperinsulinemia. J. Clin. Endocrinol. Metab. 2001, 86, 1930–1935. [Google Scholar] [CrossRef]
- Ryan, A.S.; Berman, D.M.; Nicklas, B.J.; Sinha, M.; Gingerich, R.L.; Meneilly, G.S.; Egan, J.M.; Elahi, D. Plasma adiponectin and leptin levels, body composition, and glucose utilization in adult women with wide ranges of age and obesity. Diabetes Care 2003, 26, 2383–2388. [Google Scholar] [CrossRef]
- Kim, Y.; Park, C.W. Mechanisms of Adiponectin Action: Implication of Adiponectin Receptor Agonism in Diabetic Kidney Disease. Int. J. Mol. Sci. 2019, 20, 1782. [Google Scholar] [CrossRef] [PubMed]
- Iwabu, M.; Yamauchi, T.; Okada-Iwabu, M.; Sato, K.; Nakagawa, T.; Funata, M.; Yamaguchi, M.; Namiki, S.; Nakayama, R.; Tabata, M.; et al. Adiponectin and AdipoR1 regulate PGC-1alpha and mitochondria by Ca2+ and AMPK/SIRT1. Nature 2010, 464, 1313–1319. [Google Scholar] [CrossRef]
- Martínez-Fernández, L.; Laiglesia, L.M.; Huerta, A.E.; Martínez, J.A.; Moreno-Aliaga, M.J. Omega-3 fatty acids and adipose tissue function in obesity and metabolic syndrome. Prostaglandins Other Lipid Mediat. 2015, 121, 24–41. [Google Scholar] [CrossRef]
- Meydani, M.; Hasan, S.T. Dietary polyphenols and obesity. Nutrients 2010, 2, 737–751. [Google Scholar] [CrossRef]
- Mongioi, L.M.; La Vignera, S.; Cannarella, R.; Cimino, L.; Compagnone, M.; Condorelli, R.A.; Calogero, A.E. The Role of Resveratrol Administration in Human Obesity. Int. J. Mol. Sci. 2021, 22, 4362. [Google Scholar] [CrossRef] [PubMed]
- Pasupuleti, V.R.; Sammugam, L.; Ramesh, N.; Gan, S.H. Honey, Propolis, and Royal Jelly: A Comprehensive Review of Their Biological Actions and Health Benefits. Oxid Med. Cell Longev. 2017, 2017, 1259510. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, H. Effects of Propolis Extract and Propolis-Derived Compounds on Obesity and Diabetes: Knowledge from Cellular and Animal Models. Molecules 2019, 24, 4394. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Ohhata, M.; Fujii, M.; Oda, S.; Kusaka, Y.; Matsumoto, M.; Nakamoto, A.; Taki, T.; Nakamoto, M.; Shuto, E. Brazilian Green Propolis Promotes Weight Loss and Reduces Fat Accumulation in C57BL/6 Mice Fed A High-Fat Diet. Biol. Pharm. Bull. 2017, 40, 391–395. [Google Scholar] [CrossRef]
- Kitamura, H.; Naoe, Y.; Kimura, S.; Miyamoto, T.; Okamoto, S.; Toda, C.; Shimamoto, Y.; Iwanaga, T.; Miyoshi, I. Beneficial effects of Brazilian propolis on type 2 diabetes in ob/ob mice: Possible involvement of immune cells in mesenteric adipose tissue. Adipocyte 2013, 2, 227–236. [Google Scholar] [CrossRef]
- Silveira, M.A.D.; Teles, F.; Berretta, A.A.; Sanches, T.R.; Rodrigues, C.E.; Seguro, A.C.; Andrade, L. Effects of Brazilian green propolis on proteinuria and renal function in patients with chronic kidney disease: A randomized, double-blind, placebo-controlled trial. BMC Nephrol. 2019, 20, 140. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, H.M.; Anees, M.M.; Van Dyke, T.E. Propolis Improves Periodontal Status and Glycemic Control in Patients With Type 2 Diabetes Mellitus and Chronic Periodontitis: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 1418–1426. [Google Scholar] [CrossRef]
- Gao, W.; Pu, L.; Wei, J.; Yao, Z.; Wang, Y.; Shi, T.; Zhao, L.; Jiao, C.; Guo, C. Serum Antioxidant Parameters are Significantly Increased in Patients with Type 2 Diabetes Mellitus after Consumption of Chinese Propolis: A Randomized Controlled Trial Based on Fasting Serum Glucose Level. Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2018, 9, 101–111. [Google Scholar] [CrossRef]
- Hesami, S.; Hashemipour, S.; Shiri-Shahsavar, M.R.; Koushan, Y.; Khadem Haghighian, H. Administration of Iranian Propolis attenuates oxidative stress and blood glucose in type II diabetic patients: A randomized, double-blind, placebo-controlled, clinical trial. Casp. J. Intern. Med. 2019, 10, 48–54. [Google Scholar] [CrossRef]
- Burdock, G.A. Review of the biological properties and toxicity of bee propolis (propolis). Food Chem. Toxicol. 1998, 36, 347–363. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Takahashi, K.; Sugioka, Y.; Inui, K.; Okano, T.; Mandai, K.; Yamada, Y.; Shintani, A.; Koike, T. Double-blinded randomized controlled trial to reveal the effects of Brazilian propolis intake on rheumatoid arthritis disease activity index; BeeDAI. PLoS ONE 2021, 16, e0252357. [Google Scholar] [CrossRef]
- Zhao, L.; Pu, L.; Wei, J.; Li, J.; Wu, J.; Xin, Z.; Gao, W.; Guo, C. Brazilian Green Propolis Improves Antioxidant Function in Patients with Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2016, 13, 498. [Google Scholar] [CrossRef]
- Silveira, M.A.D.; de Souza, S.P.; Dos Santos Galvão, E.B.; Teixeira, M.B.; Gomes, M.M.D.; Damiani, L.P.; Bahiense, B.A.; Cabral, J.B.; De Oliveira, C.; Mascarenhas, T.R.; et al. The use of standardized Brazilian green propolis extract (EPP-AF) as an adjunct treatment for hospitalized COVID-19 patients (BeeCovid2): A structured summary of a study protocol for a randomized controlled trial. Trials 2022, 23, 255. [Google Scholar] [CrossRef]
- Zhu, A.; Wu, Z.; Zhong, X.; Ni, J.; Li, Y.; Meng, J.; Du, C.; Zhao, X.; Nakanishi, H.; Wu, S. Brazilian Green Propolis Prevents Cognitive Decline into Mild Cognitive Impairment in Elderly People Living at High Altitude. J. Alzheimers Dis. 2018, 63, 551–560. [Google Scholar] [CrossRef]
- Fukui, T.; Yamauchi, K.; Maruyama, M.; Yasuda, T.; Kohno, M.; Abe, Y. Significance of measuring oxidative stress in lifestyle-related diseases from the viewpoint of correlation between d-ROMs and BAP in Japanese subjects. Hypertens. Res. 2011, 34, 1041–1045. [Google Scholar] [CrossRef]
- Shepherd, J.A.; Ng, B.K.; Sommer, M.J.; Heymsfield, S.B. Body composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef]
- Ponti, F.; Santoro, A.; Mercatelli, D.; Gasperini, C.; Conte, M.; Martucci, M.; Sangiorgi, L.; Franceschi, C.; Bazzocchi, A. Aging and Imaging Assessment of Body Composition: From Fat to Facts. Front. Endocrinol. 2019, 10, 861. [Google Scholar] [CrossRef]
- Nishikawa, S.; Aoyama, H.; Kamiya, M.; Higuchi, J.; Kato, A.; Soga, M.; Kawai, T.; Yoshimura, K.; Kumazawa, S.; Tsuda, T. Artepillin C, a Typical Brazilian Propolis-Derived Component, Induces Brown-Like Adipocyte Formation in C3H10T1/2 Cells, Primary Inguinal White Adipose Tissue-Derived Adipocytes, and Mice. PLoS ONE 2016, 11, e0162512. [Google Scholar] [CrossRef]
- Ueda, M.; Hayashibara, K.; Ashida, H. Propolis extract promotes translocation of glucose transporter 4 and glucose uptake through both PI3K- and AMPK-dependent pathways in skeletal muscle. Biofactors 2013, 39, 457–466. [Google Scholar] [CrossRef]
- Day, E.A.; Ford, R.J.; Steinberg, G.R. AMPK as a Therapeutic Target for Treating Metabolic Diseases. Trends Endocrinol. Metab. 2017, 28, 545–560. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Apitherapy for Age-Related Skeletal Muscle Dysfunction (Sarcopenia): A Review on the Effects of Royal Jelly, Propolis, and Bee Pollen. Foods 2020, 9, 1362. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Ten Haaf, D.S.M.; Eijsvogels, T.M.H.; Bongers, C.; Horstman, A.M.H.; Timmers, S.; de Groot, L.; Hopman, M.T.E. Protein supplementation improves lean body mass in physically active older adults: A randomized placebo-controlled trial. J. Cachexia Sarcopenia Muscle 2019, 10, 298–310. [Google Scholar] [CrossRef]
- Kinoshita, T.; Matsumoto, A.; Yoshino, K.; Furukawa, S. The effects of licorice flavonoid oil with respect to increasing muscle mass: A randomized, double-blind, placebo-controlled trial. J. Sci. Food Agric. 2017, 97, 2339–2345. [Google Scholar] [CrossRef]
- Ikeda, R.; Yanagisawa, M.; Takahashi, N.; Kawada, T.; Kumazawa, S.; Yamaotsu, N.; Nakagome, I.; Hirono, S.; Tsuda, T. Brazilian propolis-derived components inhibit TNF-α-mediated downregulation of adiponectin expression via different mechanisms in 3T3-L1 adipocytes. Biochim. Biophys. Acta 2011, 1810, 695–703. [Google Scholar] [CrossRef]
- Cartwright, M.J.; Tchkonia, T.; Kirkland, J.L. Aging in adipocytes: Potential impact of inherent, depot-specific mechanisms. Exp. Gerontol. 2007, 42, 463–471. [Google Scholar] [CrossRef]
- Okamoto, Y.; Kihara, S.; Funahashi, T.; Matsuzawa, Y.; Libby, P. Adiponectin: A key adipocytokine in metabolic syndrome. Clin. Sci. 2006, 110, 267–278. [Google Scholar] [CrossRef]
- Matsuzawa, Y. Therapy Insight: Adipocytokines in metabolic syndrome and related cardiovascular disease. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 35–42. [Google Scholar] [CrossRef]
- Cho, S.A.; Joo, H.J.; Cho, J.Y.; Lee, S.H.; Park, J.H.; Hong, S.J.; Yu, C.W.; Lim, D.S. Visceral Fat Area and Serum Adiponectin Level Predict the Development of Metabolic Syndrome in a Community-Based Asymptomatic Population. PloS ONE 2017, 12, e0169289. [Google Scholar] [CrossRef]
- Guimaraes, N.S.; Mello, J.C.; Paiva, J.S.; Bueno, P.C.; Berretta, A.A.; Torquato, R.J.; Nantes, I.L.; Rodrigues, T. Baccharis dracunculifolia, the main source of green propolis, exhibits potent antioxidant activity and prevents oxidative mitochondrial damage. Food Chem. Toxicol. 2012, 50, 1091–1097. [Google Scholar] [CrossRef]
- Veiga, R.S.; De Mendonca, S.; Mendes, P.B.; Paulino, N.; Mimica, M.J.; Lagareiro Netto, A.A.; Lira, I.S.; Lopez, B.G.; Negrao, V.; Marcucci, M.C. Artepillin C and phenolic compounds responsible for antimicrobial and antioxidant activity of green propolis and Baccharis dracunculifolia DC. J. Appl. Microbiol. 2017, 122, 911–920. [Google Scholar] [CrossRef]
- Nakamura, T.; Ohta, Y.; Ohashi, K.; Ikeno, K.; Watanabe, R.; Tokunaga, K.; Harada, N. Protective effect of Brazilian propolis against hepatic oxidative damage in rats with water-immersion restraint stress. Phytother. Res. 2012, 26, 1482–1489. [Google Scholar] [CrossRef]
- Ni, J.; Wu, Z.; Meng, J.; Zhu, A.; Zhong, X.; Wu, S.; Nakanishi, H. The Neuroprotective Effects of Brazilian Green Propolis on Neurodegenerative Damage in Human Neuronal SH-SY5Y Cells. Oxid Med. Cell Longev. 2017, 2017, 7984327. [Google Scholar] [CrossRef]
- Kim, T.; Yang, Q. Peroxisome-proliferator-activated receptors regulate redox signaling in the cardiovascular system. World J. Cardiol. 2013, 5, 164–174. [Google Scholar] [CrossRef]
- Corona, J.C.; Duchen, M.R. PPARγ as a therapeutic target to rescue mitochondrial function in neurological disease. Free. Radic. Biol. Med. 2016, 100, 153–163. [Google Scholar] [CrossRef]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef]
- Doshi, S.B.; Agarwal, A. The role of oxidative stress in menopause. J. Mid-Life Health 2013, 4, 140–146. [Google Scholar] [CrossRef]
- Okamoto, Y.; Tobe, T.; Ueda, K.; Takada, T.; Kojima, N. Oral administration of Brazilian propolis exerts estrogenic effect in ovariectomized rats. J. Toxicol. Sci. 2015, 40, 235–242. [Google Scholar] [CrossRef]
- Stepan, J.J.; Hruskova, H.; Kverka, M. Update on Menopausal Hormone Therapy for Fracture Prevention. Curr. Osteoporos. Rep. 2019, 17, 465–473. [Google Scholar] [CrossRef]
- Mangge, H.; Zelzer, S.; Puerstner, P.; Schnedl, W.J.; Reeves, G.; Postolache, T.T.; Weghuber, D. Uric acid best predicts metabolically unhealthy obesity with increased cardiovascular risk in youth and adults. Obes. (Silver Spring) 2013, 21, E71–E77. [Google Scholar] [CrossRef]
- Lim, S.; Meigs, J.B. Links between ectopic fat and vascular disease in humans. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1820–1826. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PLA (n = 28) | Propolis (n = 25) | p Value | |
|---|---|---|---|
| Physical characteristics | |||
| Age (years) | 75 (69–78) | 75 (72–78) | 0.447 a |
| Height (cm) | 149.7 ± 1.0 | 151.2 ± 1.1 | 0.287 b |
| Body mass (kg) | 53.0 ± 1.6 | 55.1 ± 1.6 | 0.368 b |
| BMI (kg/m2) | 23.7 ± 0.7 | 24.0 ± 0.6 | 0.716 b |
| Body composition | |||
| Fat mass (kg) | 16.2 ± 1.1 | 17.0 ± 0.9 | 0.576 b |
| Fat mass (%) | 32.4 ± 1.2 | 33.0 ± 1.0 | 0.675 b |
| Lean body mass (kg) | 32.8 ± 0.7 | 33.8 ± 0.7 | 0.368 b |
| Bone mineral density | |||
| Lumbar spine (g/cm2) | 0.80 ± 0.02 | 0.80 ± 0.03 | 0.955 b |
| Proximal femur (g/cm2) | 0.70 ± 0.02 | 0.69 ± 0.02 | 0.556 b |
| Muscle function | |||
| Hand grip strength (kg) | 25.1 ± 0.6 | 25.0 ± 0.6 | 0.841 b |
| Knee extension strength (Nm) | 94.0 ± 3.5 | 92.7 ± 4.1 | 0.809 b |
| Blood markers | |||
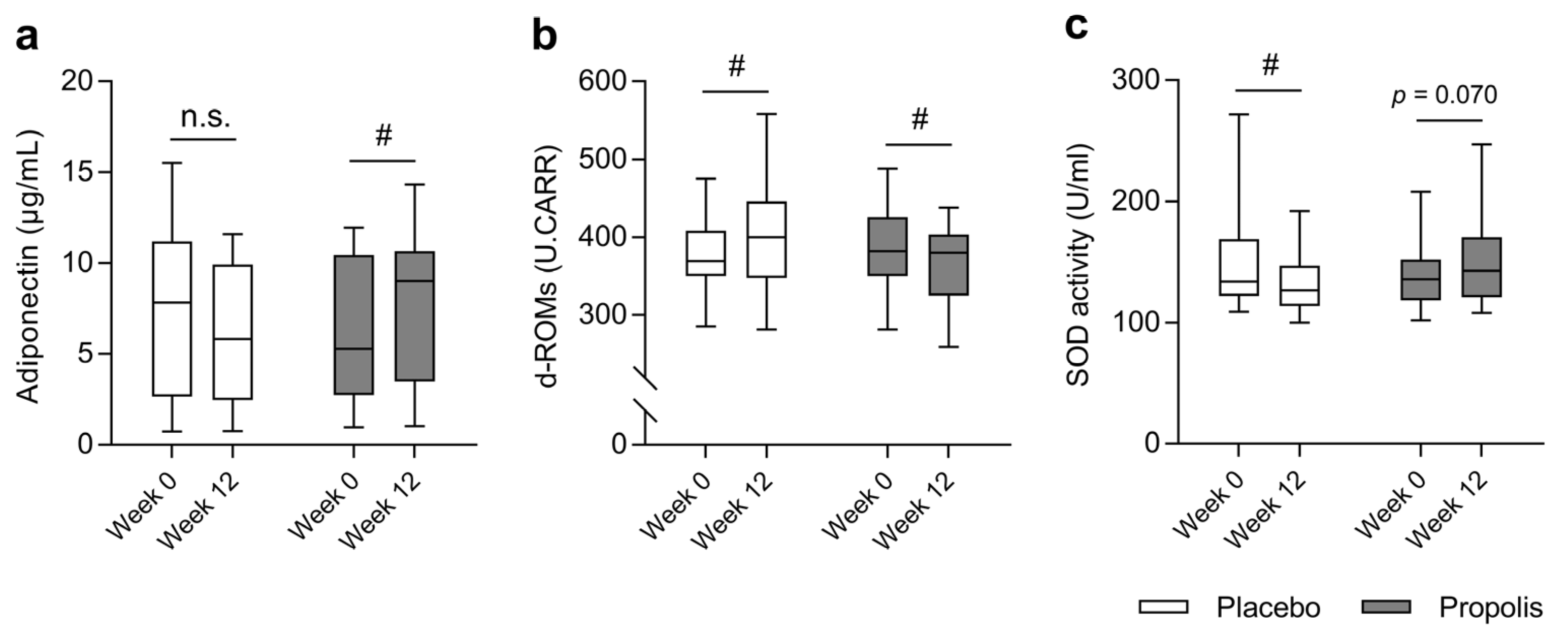
| Adiponectin (μg/mL) | 7.8 (3.1–11.0) | 5.3 (2.8–10.0) | 0.675 a |
| d-ROMs (U. CARR) | 374.5 ± 9.1 | 385.6 ± 11.8 | 0.451 b |
| SOD activity (U/mL) | 134 (122–162) | 136 (119–152) | 0.539 a |
| Placebo (n = 28) | Propolis (n = 25) | p Value (PP Analysis) | p Value (ITT Analysis) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | Time | Group | Interaction | Time | Group | Interaction | |
| Body mass (kg) | 53.0 ± 1.6 | 52.8 ± 1.7 | 55.1 ± 1.6 | 54.9 ± 1.5 | 0.170 | 0.361 | 0.830 | 0.039 | 0.497 | 0.368 |
| BMI (kg/m2) | 23.7 ± 0.7 | 23.6 ± 0.7 | 24.0 ± 0.6 | 24.0 ± 0.6 | 0.157 | 0.700 | 0.755 | 0.037 | 0.701 | 0.328 |
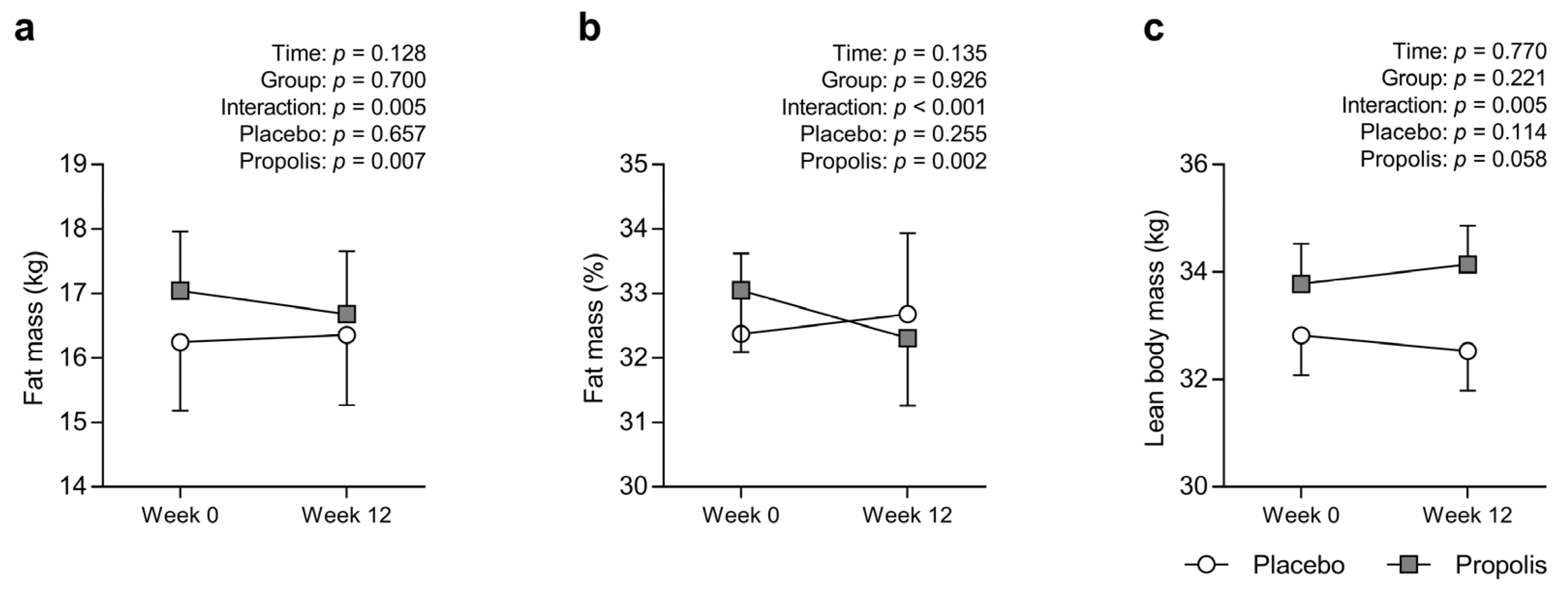
| Fat mass (kg) | 16.2 ± 1.1 | 16.4 ± 1.1 | 17.0 ± 0.9 | 16.7 ± 1.0 * | 0.128 | 0.700 | 0.005 | 0.384 | 0.479 | 0.077 |
| Fat mass (%) | 32.4 ± 1.2 | 32.7 ± 1.3 | 33.0 ± 1.0 | 32.3 ± 1.0 * | 0.135 | 0.926 | <0.001 | 0.297 | 0.440 | 0.005 |
| Lean body mass (kg) | 32.8 ± 0.7 | 32.5 ± 0.7 | 33.8 ± 0.7 | 34.1 ± 0.7 | 0.770 | 0.221 | 0.005 | 0.941 | 0.509 | 0.003 |
| Lumbar spine BMD (g/cm2) | 0.80 ± 0.02 | 0.79 ± 0.02 | 0.80 ± 0.03 | 0.80 ± 0.04 | 0.855 | 0.920 | 0.569 | 0.663 | 0.563 | 0.496 |
| Proximal femur BMD (g/cm2) | 0.70 ± 0.02 | 0.70 ± 0.02 | 0.69 ± 0.02 | 0.68 ± 0.02 | 0.522 | 0.556 | 0.989 | 0.267 | 0.284 | 0.664 |
| Hand grip strength (kg) | 25.1 ± 0.6 | 24.6 ± 0.6 | 25.0 ± 0.6 | 25.1 ± 0.7 | 0.491 | 0.860 | 0.265 | 0.203 | 0.550 | 0.294 |
| Knee extension strength (Nm) | 94.0 ± 3.5 | 97.1 ± 4.4 | 92.7 ± 4.1 | 97.2 ± 4.9 | 0.043 | 0.921 | 0.684 | <0.001 | 0.813 | 0.498 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanazashi, M.; Iida, T.; Nakanishi, R.; Tanaka, M.; Ikeda, H.; Takamiya, N.; Maeshige, N.; Kondo, H.; Nishigami, T.; Harada, T.; et al. Brazilian Propolis Intake Decreases Body Fat Mass and Oxidative Stress in Community-Dwelling Elderly Females: A Randomized Placebo-Controlled Trial. Nutrients 2023, 15, 364. https://doi.org/10.3390/nu15020364
Kanazashi M, Iida T, Nakanishi R, Tanaka M, Ikeda H, Takamiya N, Maeshige N, Kondo H, Nishigami T, Harada T, et al. Brazilian Propolis Intake Decreases Body Fat Mass and Oxidative Stress in Community-Dwelling Elderly Females: A Randomized Placebo-Controlled Trial. Nutrients. 2023; 15(2):364. https://doi.org/10.3390/nu15020364
Chicago/Turabian StyleKanazashi, Miho, Tadayuki Iida, Ryosuke Nakanishi, Masayuki Tanaka, Hiromi Ikeda, Naomi Takamiya, Noriaki Maeshige, Hiroyo Kondo, Tomohiko Nishigami, Toshihide Harada, and et al. 2023. "Brazilian Propolis Intake Decreases Body Fat Mass and Oxidative Stress in Community-Dwelling Elderly Females: A Randomized Placebo-Controlled Trial" Nutrients 15, no. 2: 364. https://doi.org/10.3390/nu15020364
APA StyleKanazashi, M., Iida, T., Nakanishi, R., Tanaka, M., Ikeda, H., Takamiya, N., Maeshige, N., Kondo, H., Nishigami, T., Harada, T., & Fujino, H. (2023). Brazilian Propolis Intake Decreases Body Fat Mass and Oxidative Stress in Community-Dwelling Elderly Females: A Randomized Placebo-Controlled Trial. Nutrients, 15(2), 364. https://doi.org/10.3390/nu15020364