

Early-Life Gut Health Indicators and Reported Prevalence of Infant Functional Constipation by Healthcare Professionals
 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Methodology
- i.
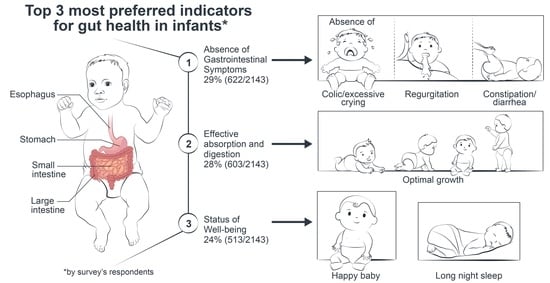
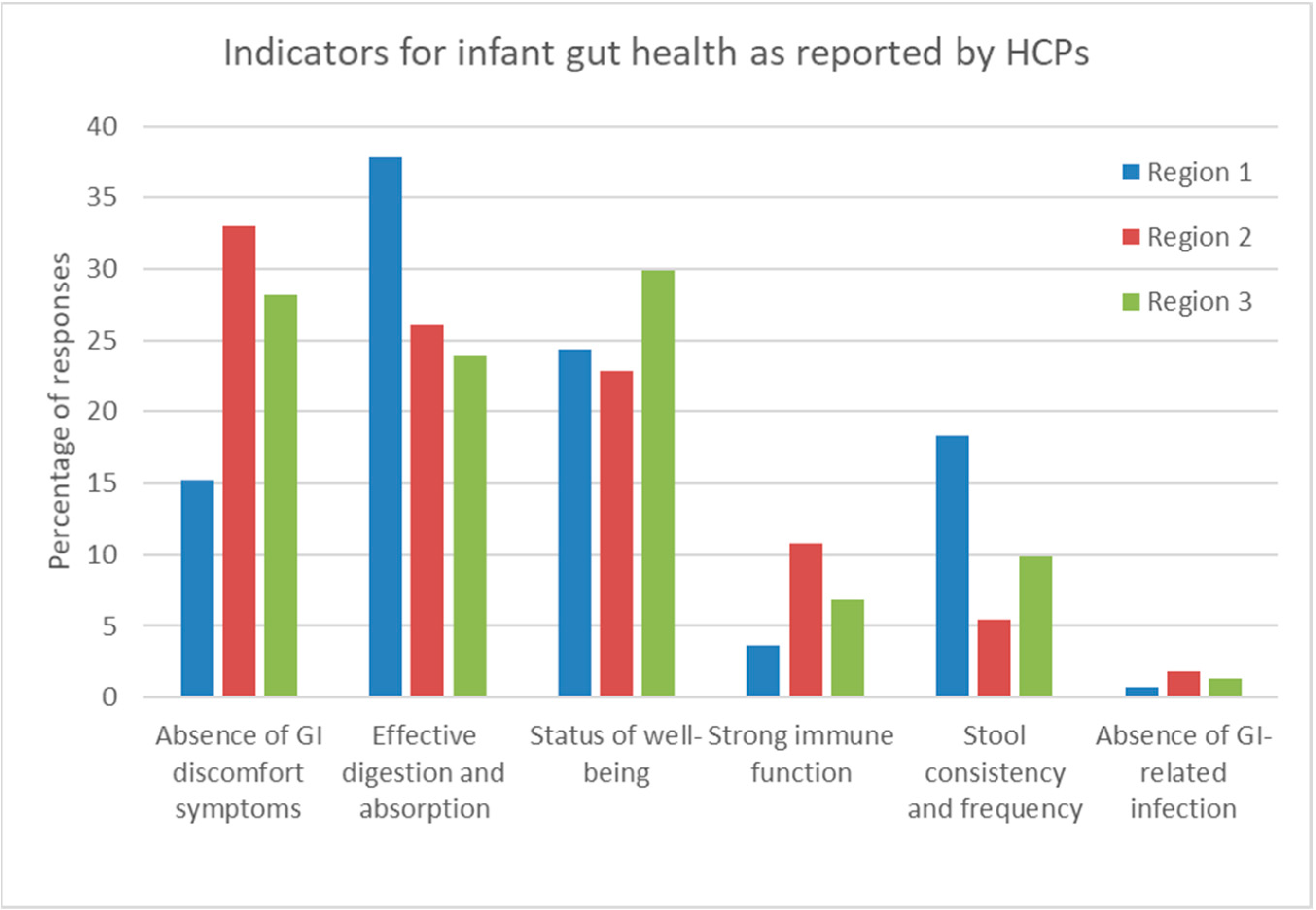
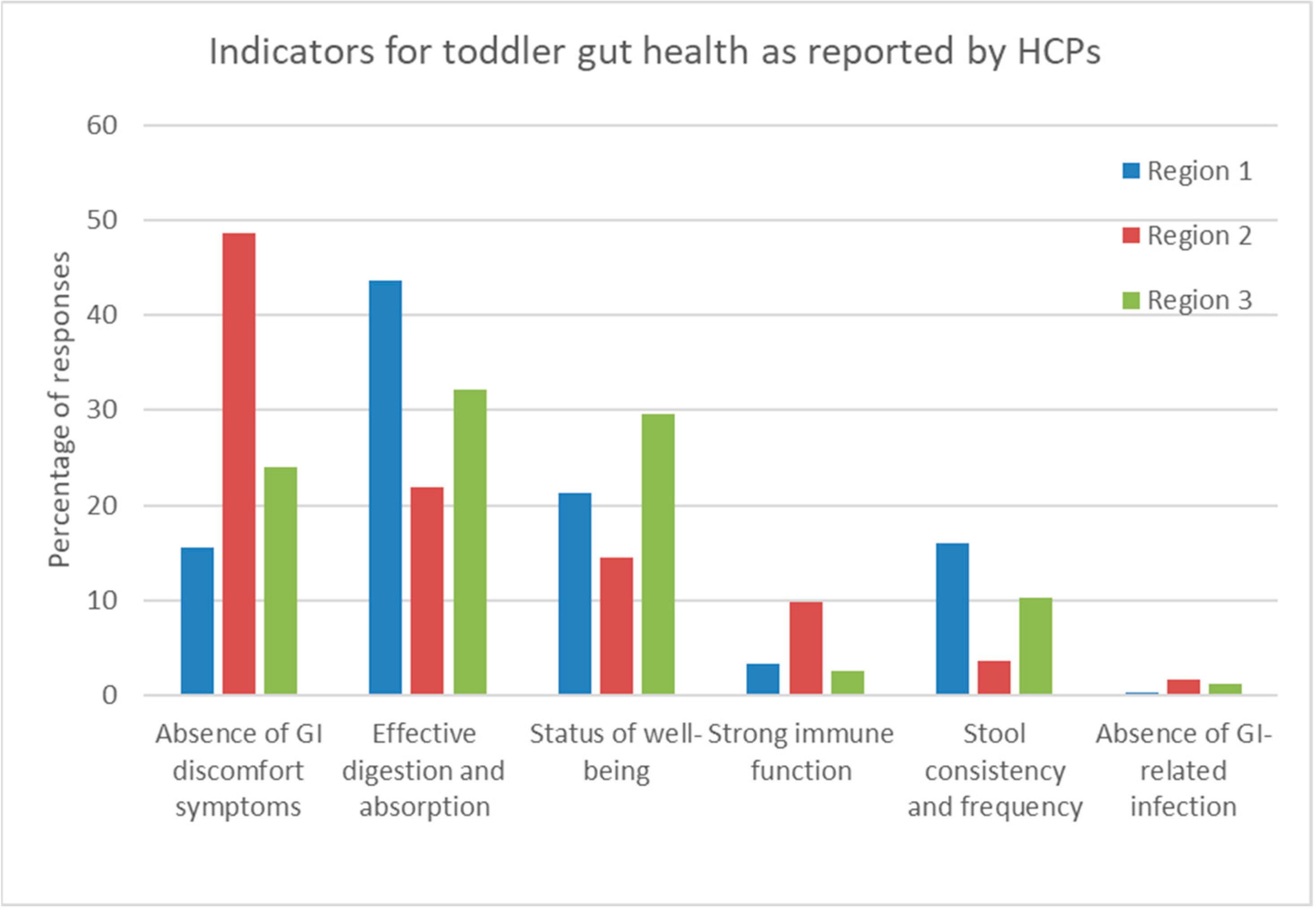
- Absence of GI discomfort symptoms, i.e., no FC;
- ii.
- Absence of GI-related infection;
- iii.
- Effective digestion and absorption of food as indicated by normal growth;
- iv.
- Well-being status, i.e., no excessive crying, good sleep during the night, good quality of life of the parents, and stool consistency and frequency;
- v.
- Strong immune function due to an optimal gut microbiota diversity.
3. Results
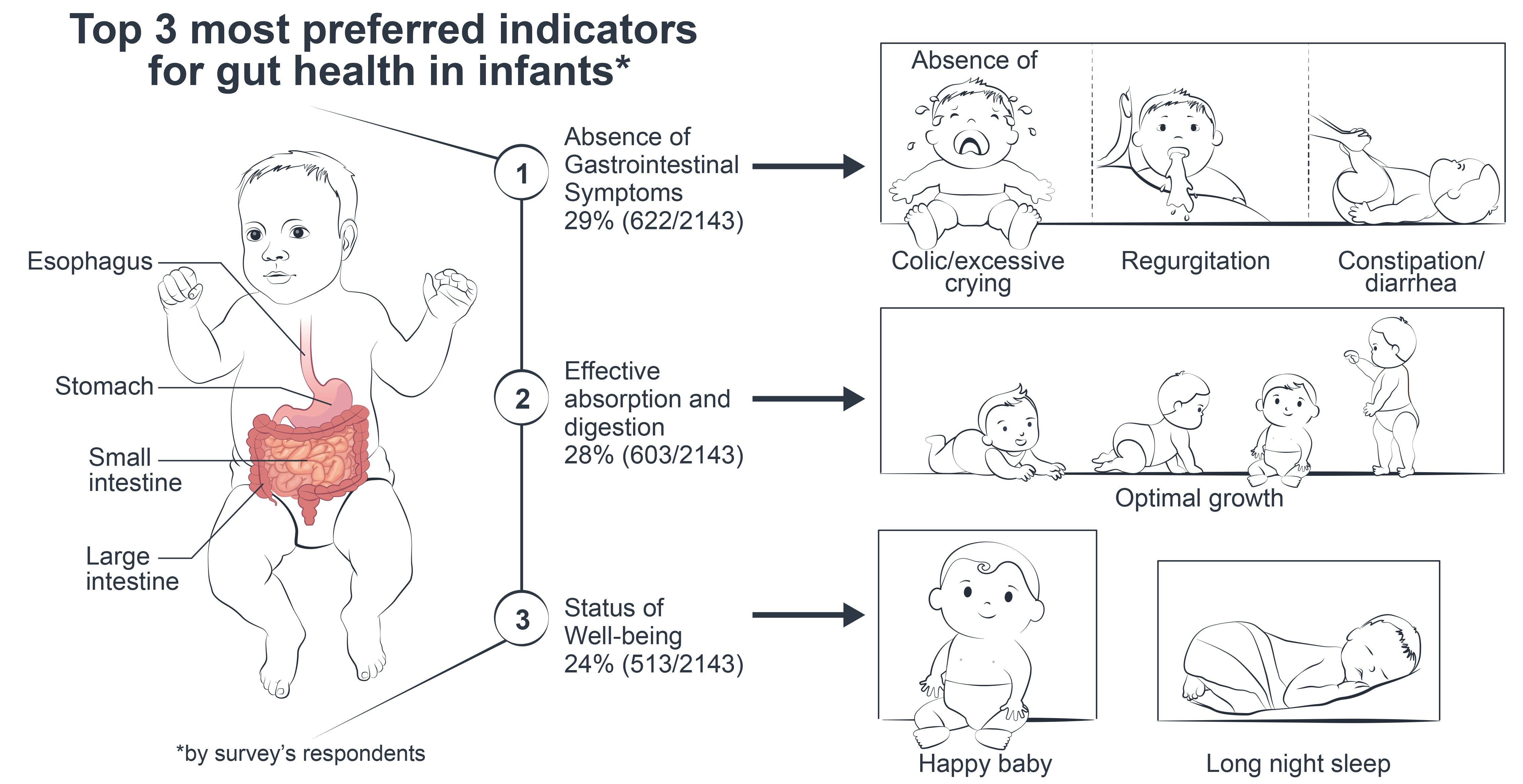
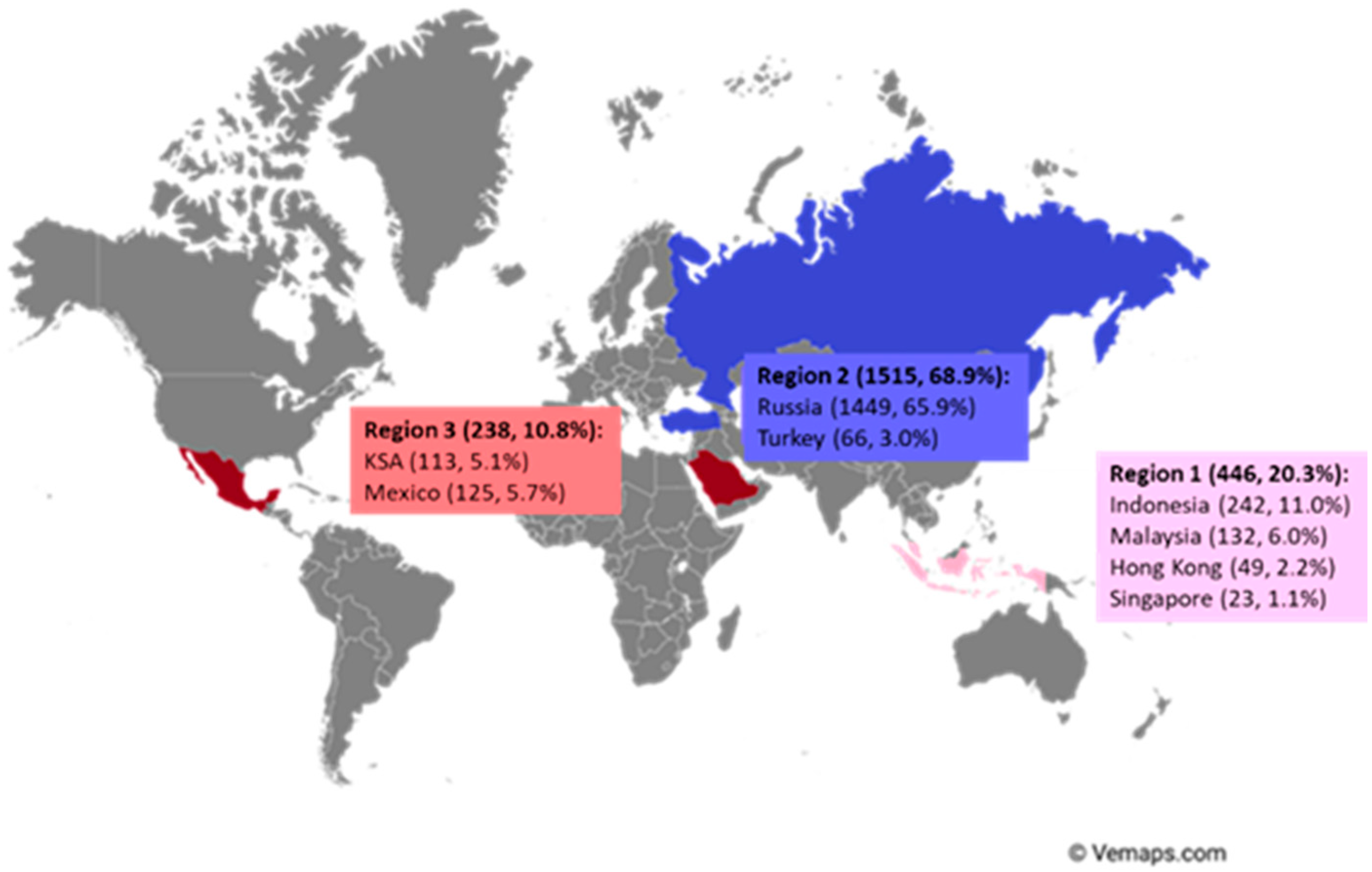
3.1. The Demographics of Respondents
3.1.1. Indicators of Gut Health in Infants and Toddlers
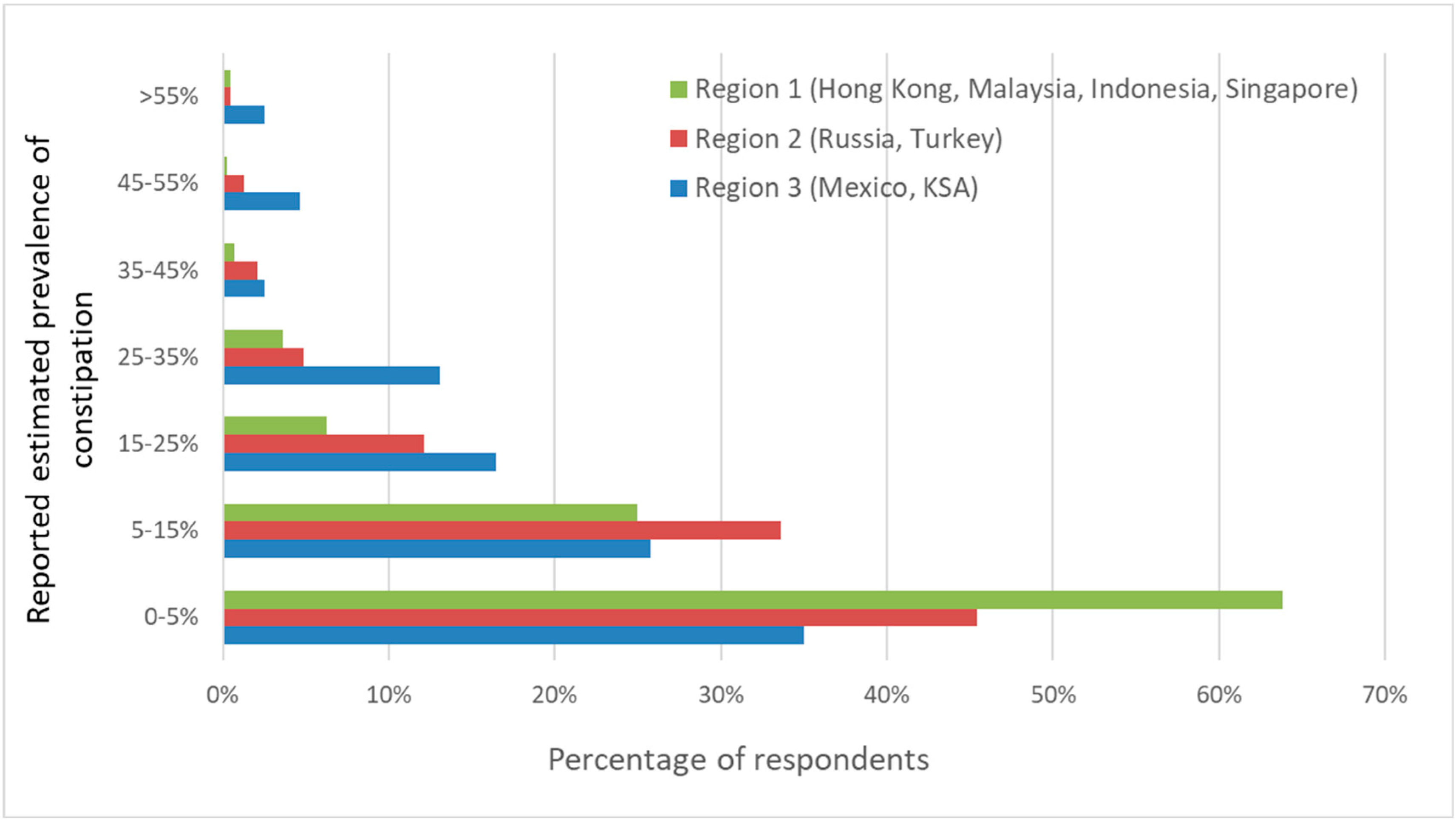
3.1.2. Prevalence of FC in Infants
3.1.3. Impact of FC in Infants on Quality of Life
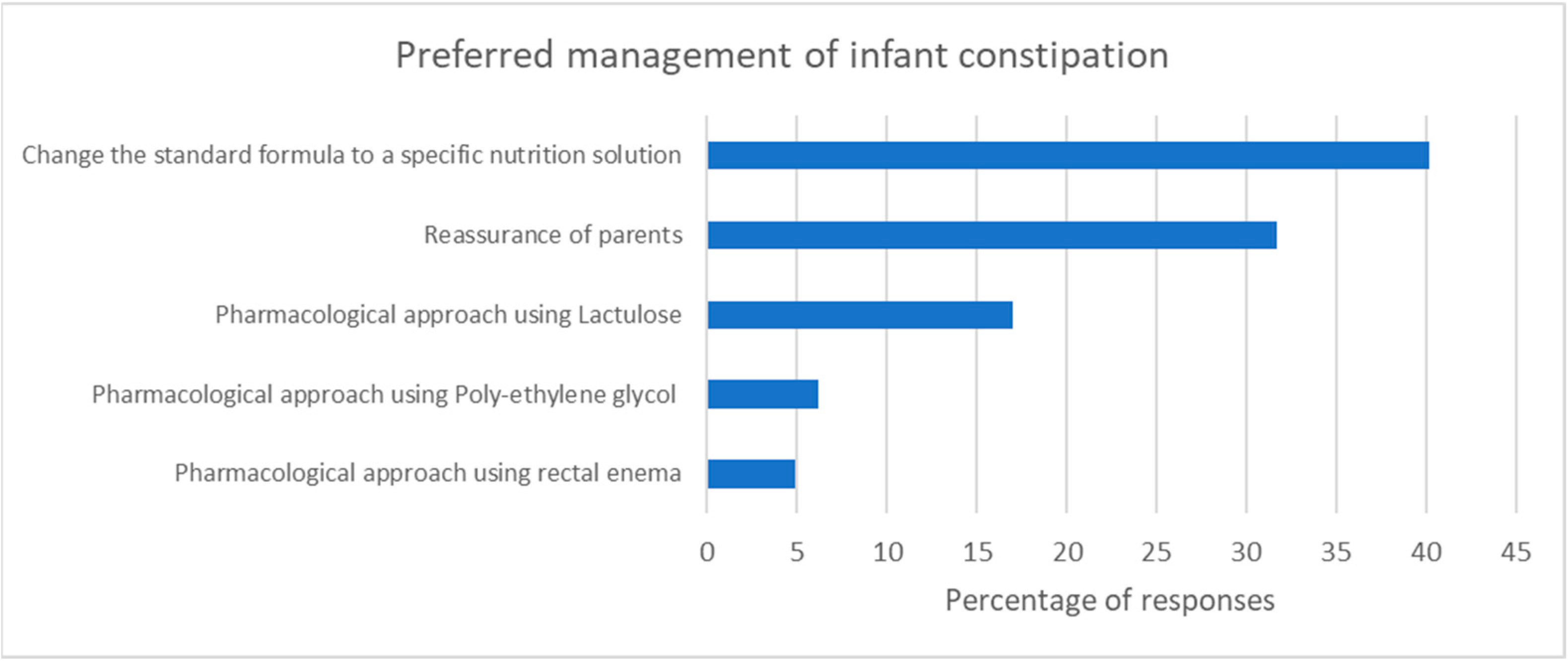
3.1.4. Management of FC in Infants
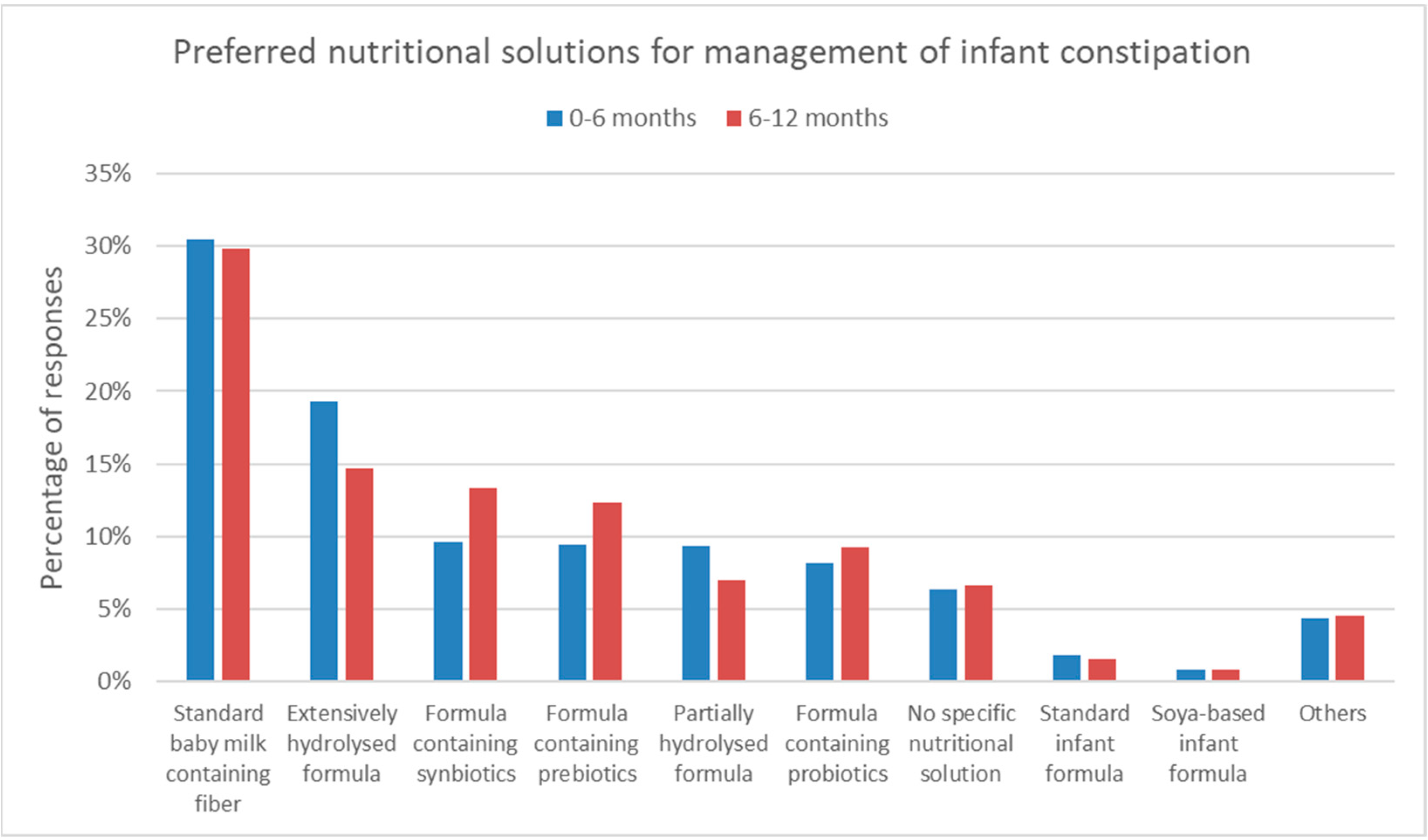
3.1.5. Preferred Nutritional Management of FC in Infants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| 1. In your opinion, what will be the best indicator to assess healthy GI tract in infants: 1. Absence of GI discomfort symptoms i.e., no constipation 2. Absence of GI-related infection 3. Effective digestion and absorption of food as indicated by normal growth 4. Status of well-being ie no excessive crying, good sleep during the night, good quality of life of the parents 5. Stool consistency and frequency 6. Strong immune function from inside due the optimal gut microbiota diversity 7. Others; please specify: _____________________ |
| 2. In your opinion, what will be the best indicator to assess healthy GI tract in toddlers: 1. Absence of GI discomfort symptoms i.e., no GER, no constipation + crying, no colic 2. Absence of GI-related infection 3. Effective digestion and absorption of food as indicated by normal growth 4. Status of well-being ie no excessive crying, good sleep during the night, good quality of life of the parents 5. Stool consistency and frequency 6. Strong immune function from inside due the optimal gut microbiota diversity 7. Others; please specify: _____________________ |
| 3. What is the average prevalence of infantile constipation in your practice within the last one week? 1. 0–5% 2. 6–15% 3. 16–25% 4. 26–35% 5. 36–45% 6. 46–55% 7. More than 55% |
| 4. At which age do you encounter the highest incidence of the infant’s constipation in your practice? 1. 0–2.9 months 2. 3–5.9 months 3. 6–8.9 months 4. 9–12 months 5. Others: ___________________ |
| 5. How frequently do you observe constipation affects the quality of life of infants and their parents in the last week? 1. Almost Always: >70% 2. Sometimes: 30–69% 3. Rarely: 10–29% 4. Never: <10% |
| 6. Please rank the following treatments that you usually practice when managing constipation in infants 0–12 months: (no#1: the most frequent; no#6: the least frequent) 1. Change the standard formula to a specific nutrition solution 2. Pharmacological approach using Lactulose 3. Pharmacological approach using Poly-ethylene Glycol (PEG) 4. Pharmacological approach using rectal enema 5. Pharmacological approach using Sodium picosulfate 6. Reassurance of parents |
| 7. Which specific nutrition solution do you often use in managing constipation in nonbreastfed 0–6 months old infants? 1. Extensively hydrolysed formula 2. Formula containing fiber (i.e., inulin or carob bean gum) 3. Formula containing milk-fat 4. Formula containing prebiotics (fructo-oligosacharides or galacto-oligosaccharides) 5. Formula containing probiotics (Bifidobacteria or Lactobacillus Sp.) 6. Formula containing synbiotics (combination between prebiotics and probiotics) 7. Goat milk–based infant formula 8. Magnesium-rich formula 9. No specific nutrition solution 10. Partially hydrolyzed formula 11. Soya-based infant formula 12. Standard infant formula 13. Don’t know 14. Others; please specify: _____________________________ |
| 8. Which specific nutrition solution do you often use in managing constipation in nonbreastfed 6–12 months old infants? 1. Extensively hydrolysed formula 2. Formula containing fiber (i.e., inulin or carob bean gum) 3. Formula containing milk-fat 4. Formula containing prebiotics (fructo-oligosacharides or galacto-oligosaccharides) 5. Formula containing probiotics (Bifidobacteria or Lactobacillus Sp.) 6. Formula containing synbiotics (combination between prebiotics and probiotics) 7. Goat milk–based infant formula 8. Magnesium-rich formula 9. No specific nutrition solution 10. Partially hydrolyzed formula 11. Soya-based infant formula 12. Standard infant formula 13. Don’t know 14. Others; please specify: _____________________________ |
References
- Huppertz, T.; Chia, L.W. Milk protein coagulation under gastric conditions: A review. Int. Dairy J. 2020, 113, 104882. [Google Scholar] [CrossRef]
- Hamosh, M. Digestion in the Newborn. Clin. Perinatol. 1996, 23, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Mason, S. Some Aspects of Gastric Function in the Newborn. Arch. Dis. Child. 1962, 37, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A. Modulation of the Gastrointestinal Tract of Infants by Human Milk. Interfaces and Interactions. An Evolutionary Perspective. J. Nutr. 2000, 130, 426S–431S. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C. ‘Gut health’: A new objective in medicine? BMC Med. 2011, 9, 24. [Google Scholar] [CrossRef]
- Muhardi, L.; Aw, M.M.; Hasosah, M.; Ng, R.T.; Chong, S.Y.; Hegar, B.; Toro-Monjaraz, E.; Darma, A.; Cetinkaya, M.; Chow, C.M.; et al. A Narrative Review on the Update in the Prevalence of Infantile Colic, Regurgitation, and Constipation in Young Children: Implications of the ROME IV Criteria. Front. Pediatr. 2022, 9, 1493. [Google Scholar] [CrossRef]
- Mai, V. Dietary Modification of the Intestinal Microbiota. Nutr. Rev. 2004, 62, 235–242. [Google Scholar] [CrossRef]
- Rothbart, M.K. Measurement of Temperament in infancy. Child Development 1981, 52, 569–578. [Google Scholar] [CrossRef]
- Blunden, S.L.; Thompson, K.; Dawson, D. Behavioural sleep treatments and night time crying in infants: Challenging the status quo. Sleep Med. Rev. 2011, 15, 327–334. [Google Scholar] [CrossRef]
- West, L.N.; Zakharova, I.; Huysentruyt, K.; Chong, S.-Y.; Aw, M.M.; Darma, A.; Hegar, B.; Ng, R.T.; Hasosah, M.; Toro-Monjaraz, E.; et al. Reported Prevalence and Nutritional Management of Functional Constipation among Young Children from Healthcare Professionals in Eight Countries across Asia, Europe and Latin America. Nutrients 2022, 14, 4067. [Google Scholar] [CrossRef]
- De Onis, M.; Garza, C.; Victora, C.G.; Onyango, A.W.; Frongillo, E.A.; Martines, J. The WHO Multicentre Growth Reference Study: Planning, study design, and methodology. Food. Nutr. Bull. 2004, 25, S15–S26. [Google Scholar] [CrossRef] [PubMed]
- Manson, W.G.; Weaver, L.T. Fat digestion in the neonate. Arch. Dis. Child. Fetal Neonatal Ed. 1997, 76, F206–F211. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Lamb, K.; Grimes, C.; Laws, R.; Bolton, K.; Ong, K.K.; Campbell, K. Rapid weight gain during infancy and subsequent adiposity: A systematic review and meta-analysis of evidence. Obes. Rev. 2017, 19, 321–332. [Google Scholar] [CrossRef]
- Wells, J.C.K.; Fewtrell, M.S. Is body composition important for paediatricians?: Figure 1. Arch. Dis. Child. 2007, 93, 168–172. [Google Scholar] [CrossRef]
- Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.P. Epidemiology of functional gastrointestinal disorders in infants and tod-dlers: A systematic review. World J. Gastroenterol. 2016, 22, 6547–6558. [Google Scholar] [CrossRef] [PubMed]
- Boronat, A.; Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of functional gastrointestinal disorders in children and adolescents: A systematic review. World J. Gastroenterol. 2017, 23, 3915–3927. [Google Scholar] [CrossRef]
- Huang, Y.; Tan, S.Y.; Parikh, P.; Buthmanaban, V.; Rajindrajith, S.; Benninga, M.A. Prevalence of functional gastrointestinal disorders in infants and young children in China. BMC Pediatr. 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Abkari, A.; Bellaiche, M.; Benninga, M.; Chouraqui, J.P.; Çokura, F.; Harb, T.; Hegar, B.; Lifschitz, C.; Ludwig, T.; et al. Prevalence and Health Outcomes of Functional Gastrointestinal Symptoms in Infants From Birth to 12 Months of Age. J. Craniofacial Surg. 2015, 61, 531–537. [Google Scholar] [CrossRef]
- Zeevenhooven, J.; Koppen, I.J.N.; Benninga, M.A. The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers. Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 1–13. [Google Scholar] [CrossRef]
- Chew, K.S.; Em, J.M.; Koay, Z.L.; Jalaludin, M.Y.; Ng, R.T.; Lum, L.C.S.; Lee, W.S. Low prevalence of infantile functional gastrointestinal disorders (FGIDs) in a multi-ethnic Asian population. Pediatr. Neonatol. 2021, 62, 49–54. [Google Scholar] [CrossRef]
- Vriesman, M.H.; Koppen, I.J.N.; Camilleri, M.; Di Lorenzo, C.; Benninga, M.A. Management of functional constipation in children and adults. Nat. Rev. Gastroenterol. Hepatol. 2019, 17, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shang, L.; Zhang, Y.; Tian, J.; Wang, B.; Yang, X.; Sun, L.; Du, C.; Jiang, X.; Xu, Y. Impact of Functional Constipation on Health-Related Quality of Life in Preschool Children and Their Families in Xi’an, China. PLoS ONE 2013, 8, e77273. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Hauser, B.; Salvatore, S. Functional Gastrointestinal Disorders in Infancy: Impact on the Health of the Infant and Family. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Widodo, A.; Hegar, B.; Vandenplas, Y. Pediatricians lack knowledge for the diagnosis and management of functional con-stipation in children over 6 mo of age. World J. Clin. Pediatr. 2018, 7, 56–61. [Google Scholar] [CrossRef]
- Hepner, K.A.; Sechrest, L. Confirmatory factor analysis of the Child Health Questionnaire-Parent Form 50 in a predominantly minority sample. Qual. Life Res. 2002, 11, 763–773. [Google Scholar] [CrossRef]
- Tabbers, M.M.; Boluyt, N.; Berger, M.Y.; Benninga, M.A. Clinical practice: Diagnosis and treatment of functional consti-pation. Eur. J. Pediatr. 2011, 170, 955–963. [Google Scholar] [CrossRef]
- Salvatore, S.; Abkari, A.; Cai, W.; Catto-Smith, A.; Cruchet, S.; Gottrand, F.; Hegar, B.; Lifschitz, C.; Ludwig, T.; Shah, N.; et al. Review shows that parental reassurance and nutritional advice help to optimise the management of func-tional gastrointestinal disorders in infants. Acta Paediatr. Int. J. Paediatr. 2018, 107, 1512–1520. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Zakharova, I.; Dmitrieva, Y. Oligosaccharides in infant formula: More evidence to validate the role of prebiotics. Br. J. Nutr. 2015, 113, 1339–1344. [Google Scholar] [CrossRef]
- Quinlan, P.T.; Lockton, S.; Irwin, J.; Lucas, A.L. The Relationship between Stool Hardness and Stool Composition in Breast- and Formula-Fed Infants. J. Craniofacial Surg. 1995, 20, 81–90. [Google Scholar] [CrossRef]
- Tabbers, M.M.; DiLorenzo, C.; Berger, M.Y.; Faure, C.; Langendam, M.W.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M.A. Evaluation and treatment of functional constipation in infants and children: Evidence-based recom-mendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef]
- Looijesteijn, E.; Brouwer, R.W.W.; Schoemaker, R.J.W.; Ulfman, L.H.; Ham, S.L.; Jeurink, P.; Karaglani, E.; van Ijcken, W.F.J.; Manios, Y. Effect of bovine milk fat-based infant formulae on microbiota, metabolites and stool parameters in healthy term infants in a randomized, crossover, placebo-controlled trial. BMC Nutr. 2022, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Huang, W.; Xu, X.; Wang, L.; Wang, Q.; Li, S.; Yuan, X. Stool Saponified Fatty Acid, Behavior, Growth, and Stool Characteristics in Infants Fed a High-OPO Formula: A Randomized, Double-Blind Clinical Trial. Front. Pediatr. 2021, 9, 712201. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency of Observing FC Affecting QoL # | Overall | Pediatricians | General Practitioners | Pediatric Gastro-enterologists | Other Professions |
|---|---|---|---|---|---|
| Almost always (>70%) | 703/2182 (32.2%) | 539/1751 (30.8%) | 36/138 (26.1%) | 84/154 (54.5%) | 44/139 (31.7%) |
| Sometimes (30–70%) | 754/2182 (34.6%) | 618/1751 (35.3%) | 41/138 (29.7%) | 46/154 (29.9%) | 49/139 (35.3%) |
| Rarely (10–30%) | 575/2184 (26.4%) | 481/1751 (27.5%) | 39/138 (28.3%) | 21/154 (13.6%) | 34/139 (24.5%) |
| Never (<10%) | 150/2184 (6.9%) | 113/1751 (6.5%) | 22/138 (15.9%) | 3/154 (1.9%) | 12/139 (8.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhardi, L.; Delsing, D.J.M.; Zakharova, I.; Huysentruyt, K.; Chong, S.-Y.; Ng, R.T.; Darma, A.; Hegar, B.; Hasosah, M.; Toro-Monjaraz, E.; et al. Early-Life Gut Health Indicators and Reported Prevalence of Infant Functional Constipation by Healthcare Professionals. Nutrients 2023, 15, 298. https://doi.org/10.3390/nu15020298
Muhardi L, Delsing DJM, Zakharova I, Huysentruyt K, Chong S-Y, Ng RT, Darma A, Hegar B, Hasosah M, Toro-Monjaraz E, et al. Early-Life Gut Health Indicators and Reported Prevalence of Infant Functional Constipation by Healthcare Professionals. Nutrients. 2023; 15(2):298. https://doi.org/10.3390/nu15020298
Chicago/Turabian StyleMuhardi, Leilani, Dianne J. M. Delsing, Irina Zakharova, Koen Huysentruyt, Sze-Yee Chong, Ruey Terng Ng, Andy Darma, Badriul Hegar, Mohammed Hasosah, Erick Toro-Monjaraz, and et al. 2023. "Early-Life Gut Health Indicators and Reported Prevalence of Infant Functional Constipation by Healthcare Professionals" Nutrients 15, no. 2: 298. https://doi.org/10.3390/nu15020298
APA StyleMuhardi, L., Delsing, D. J. M., Zakharova, I., Huysentruyt, K., Chong, S.-Y., Ng, R. T., Darma, A., Hegar, B., Hasosah, M., Toro-Monjaraz, E., Cetinkaya, M., Chow, C.-M., Aw, M. M., Kudla, U., West, L. N., & Vandenplas, Y. (2023). Early-Life Gut Health Indicators and Reported Prevalence of Infant Functional Constipation by Healthcare Professionals. Nutrients, 15(2), 298. https://doi.org/10.3390/nu15020298