
A Randomized Controlled Trial of Soy Isoflavone Intake on Mammographic Density among Malaysian Women

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data Collection
2.3. Intervention and Compliance
2.4. Outcome Measurements
2.5. Statistical Analysis
3. Results
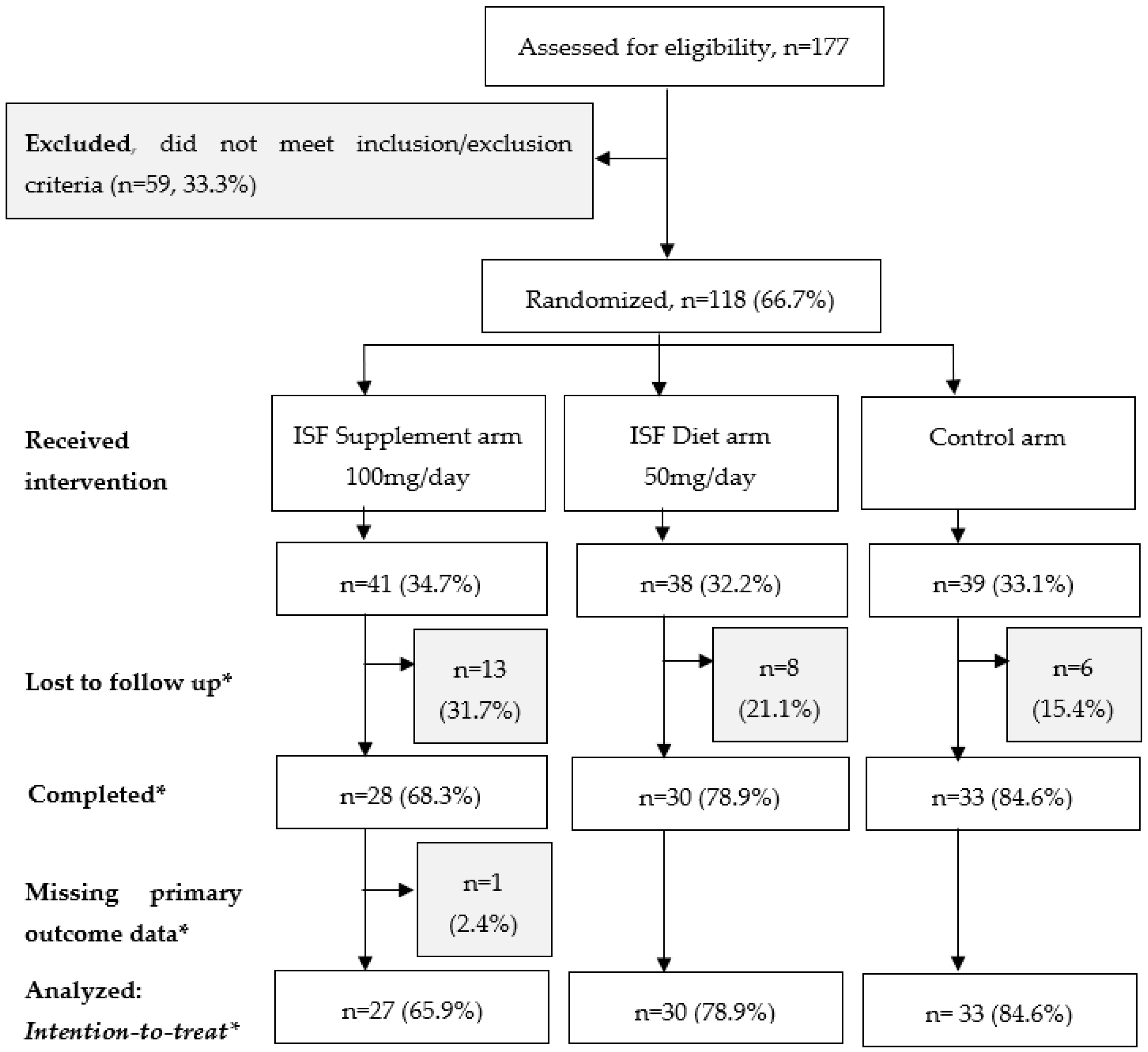
3.1. Follow Up during the Study Period
3.2. Description of Participants in the Primary Analysis
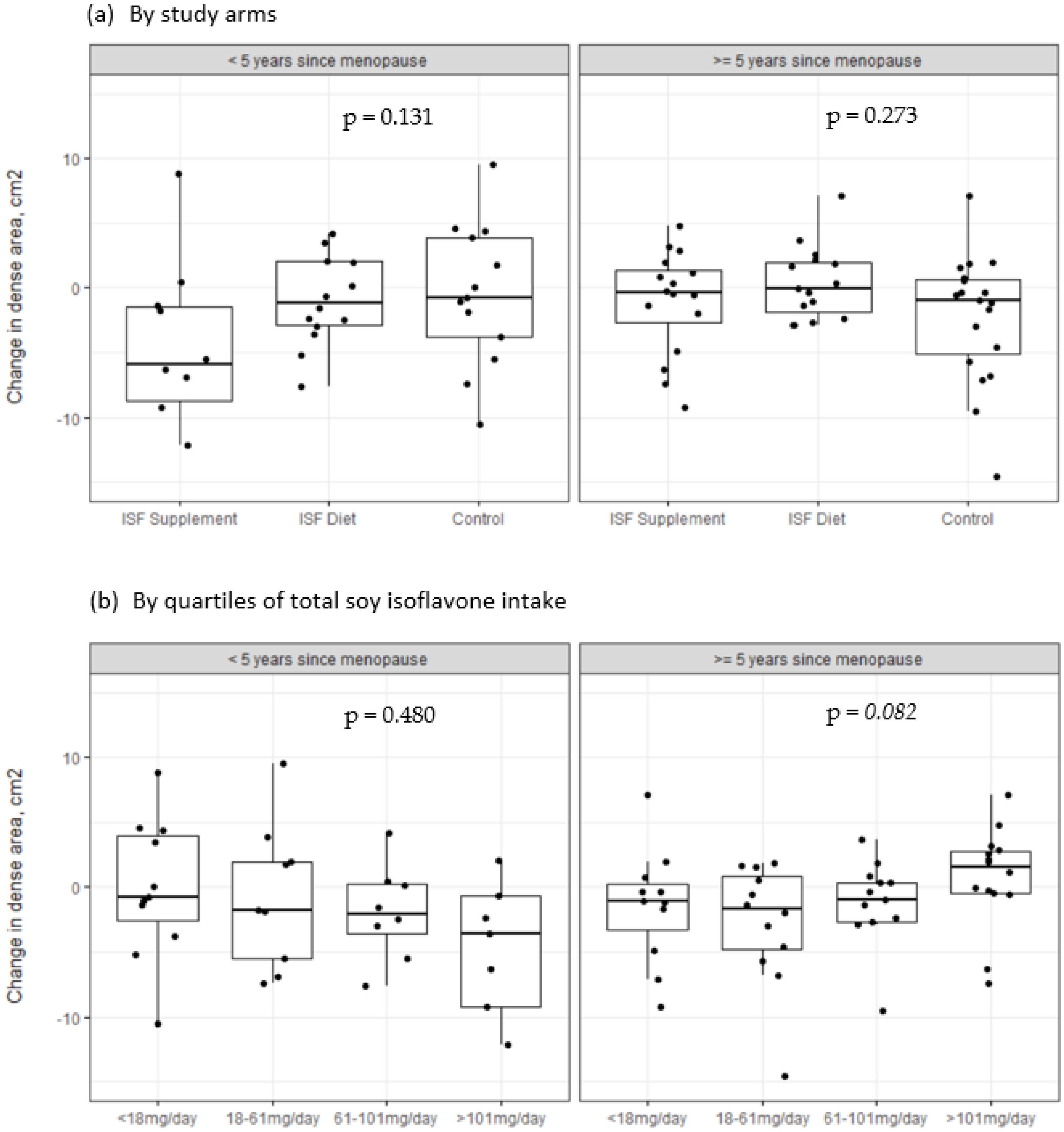
3.3. Change in Mammographic Density over the Study Period
3.4. Changes in Mammographic Density over Time
3.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; Fidler-Benaoudia, M.M. Global burden and trends in premenopausal and postmenopausal breast cancer: A population-based study. Lancet Glob. Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef] [PubMed]
- Porter, P. “Westernizing” women’s risks? Breast cancer in lower-income countries. N. Engl. J. Med. 2008, 358, 213–216. [Google Scholar] [CrossRef]
- Sung, H.; Rosenberg, P.S.; Chen, W.Q.; Hartman, M.; Lim, W.Y.; Chia, K.S.; Wai-Kong Mang, O.; Chiang, C.J.; Kang, D.; Ngan, R.K.C.; et al. Female Breast Cancer Incidence among Asian and Western Populations: More Similar Than Expected. J. Natl. Cancer Inst. 2015, 107, djv107. [Google Scholar] [CrossRef]
- Stanford, J.L.; Herrinton, L.J.; Schwartz, S.M.; Weiss, N.S. Breast cancer incidence in asian migrants to the United States and their descendants. Epidemiology 1995, 6, 181–183. [Google Scholar] [CrossRef]
- Nelson, H.D.; Fu, R.; Zakher, B.; McDonagh, M.; Pappas, M.; Stillman, L. Medication Use for the Risk Reduction of Primary Breast Cancer in Women: A Systematic Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2019.
- Wu, A.H.; Yu, M.C.; Tseng, C.C.; Pike, M.C. Epidemiology of soy exposures and breast cancer risk. Br. J. Cancer 2008, 98, 9–14. [Google Scholar] [CrossRef]
- Chen, L.R.; Ko, N.Y.; Chen, K.H. Isoflavone supplements for menopausal women: A systematic review. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Bhattacharya, T.; Dutta, S.; Akter, R.; Rahman, M.H.; Karthika, C.; Nagaswarupa, H.P.; Murthy, H.C.A.; Fratila, O.; Brata, R.; Bungau, S. Role of Phytonutrients in Nutrigenetics and Nutrigenomics Perspective in Curing Breast Cancer. Biomolecules 2021, 11, 1176. [Google Scholar] [CrossRef] [PubMed]
- Ţiţ, D.M.; Pallag, A.; Iovan, C.; Furău, G.; Furău, C.; Bungău, S. Somatic-vegetative Symptoms Evolution in Postmenopausal Women Treated with Phytoestrogens and Hormone Replacement Therapy. Iran J. Public Health 2017, 46, 1528. [Google Scholar]
- Tit, D.M.; Bungau, S.; Iovan, C.; Cseppento, D.C.N.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the Hormone Replacement Therapy and of Soy Isoflavones on Bone Resorption in Postmenopause. J. Clin. Med. 2018, 7, 297. [Google Scholar] [CrossRef]
- Trock, B.J.; Hilakivi-Clarke, L.; Clarke, R. Meta-Analysis of Soy Intake and Breast Cancer Risk. J. Natl. Cancer Inst. 2006, 98, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liu, X.; Ren, S. Tofu intake is inversely associated with risk of breast cancer: A meta-analysis of observational studies. PLoS ONE 2020, 15, e0226745. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Rao, Y.; Zheng, Y.; Wei, S.; Li, Y.; Guo, T.; Yin, P. Association between soy isoflavone intake and breast cancer risk for pre- and post-menopausal women: A meta-analysis of epidemiological studies. PLoS ONE 2014, 9, e89288. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Madhavan, G.; Tice, J.A.; Leinster, S.J.; Cassidy, A. Effects of isoflavones on breast density in pre-and post-menopausal women: A systematic review and meta-analysis of randomized controlled trials. Hum. Reprod. Update 2010, 16, 745–760. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Spicer, D.; Garcia, A.; Tseng, C.C.; Hovanessian-Larsen, L.; Sheth, P.; Martin, S.E.; Hawes, D.; Russell, C.; MacDonald, H.; et al. Double-blind randomized 12-month soy intervention had no effects on breast MRI fibroglandular tissue density or mammographic density. Cancer Prev. Res. 2015, 8, 942–951. [Google Scholar] [CrossRef]
- Delmanto, A.; Nahas-Neto, J.; Traiman, P.; Uemura, G.; Pessoa, E.C.; Nahas, E.A.P. Effects of soy isoflavones on mammographic density and breast parenchyma in postmenopausal women: A randomized, double-blind, placebo-controlled clinical trial. Menopause 2013, 20, 1049–1054. [Google Scholar] [CrossRef]
- Maskarinec, G.; Verheus, M.; Steinberg, F.M.; Amato, P.; Cramer, M.K.; Lewis, R.D.; Murray, J.M.; Young, R.L.; Wong, W.W. Various doses of soy isoflavones do not modify mammographic density in postmenopausal women. J. Nutr. 2009, 139, 981–986. [Google Scholar] [CrossRef]
- Maskarinec, G.; Takata, Y.; Franke, A.A.; Williams, A.E.; Murphy, S.P. A 2-year soy intervention in premenopausal women not change mammographic densities. J. Nutr. 2004, 134, 3089–3094. [Google Scholar] [CrossRef]
- Maskarinec, G.; Williams, A.E.; Carlin, L. Mammographic densities in a one-year isoflavone intervention. Eur. J. Cancer Prev. 2003, 12, 165–169. [Google Scholar] [CrossRef]
- Verheus, M.; Van Gils, C.H.; Kreijkamp-Kaspers, S.; Kok, L.; Peeters, P.H.M.; Grobbee, D.E.; Van Der Schouw, Y.T. Soy protein containing isoflavones and mammographic density in a randomized controlled trial in postmenopausal women. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2632–2638. [Google Scholar] [CrossRef]
- Nagata, C. Factors to consider in the association between soy isoflavone intake and breast cancer risk. J. Epidemiol. 2010, 20, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Maskarinec, G.; Ju, D.; Morimoto, Y.; Franke, A.A.; Stanczyk, F.Z. Soy Food Intake and Biomarkers of Breast Cancer Risk: Possible Difference in Asian Women? Nutr. Cancer 2017, 69, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, B.J.; Teter, B.E.; Barba, M.; Byrne, C.; Cavalleri, A.; Grant, B.J.; Horvath, P.J.; Morelli, D.; Venturelli, E.; Muti, P.C. Equol status modifies the association of soy intake and mammographic density in a sample of postmenopausal women. Cancer Epidemiol. Biomark. Prev. 2008, 17, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.; Byrne, C.; Kurzer, M.S.; Fang, C.Y. Equol-producing status, isoflavone intake, and breast density in a sample of U.S. Chinese women. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1975–1983. [Google Scholar] [CrossRef]
- Tan, M.M.; Ho, W.K.; Yoon, S.Y.; Mariapun, S.; Hasan, S.N.; Shin-Chi Lee, D.; Hassan, T.; Lee, S.Y.; Phuah, S.Y.; Sivanandan, K.; et al. A case-control study of breast cancer risk factors in 7,663 women in Malaysia. PLoS ONE 2018, 13, e0203469. [Google Scholar] [CrossRef]
- Soh, W.H.; Rajaram, N.; Mariapun, S.; Eriksson, M.; Fadzli, F.; Ho, W.K.; Mohd Taib, N.A.; Hall, P.; Teo, S.H. Physical activity and mammographic density in an Asian multi-ethnic cohort. Cancer Causes Control. 2018, 29, 883–894. [Google Scholar] [CrossRef]
- Ali Zainuddin, A.; Nadzri Jai, A.; Baharuddin, A.; Mahadir Naidu, B.; Ying Ying, C.; Siew Man, C.; Nordin, F.; Hashim, H.; Guat Hiong, T.; Yi Yi, K.; et al. National Health and Morbidity Survey 2014: Malaysian Adult Nutrition Survey. Volume 1: Methodology and General Findings; Institute for Public Health (IKU): Selangor, Malaysia, 2014.
- Singapore Health Promotion Board. Energy & Nutrient Composition Search 2011. Available online: https://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 22 January 2021).
- Institute for Medical Research. Food Compositon Database Module Industry 1997. Available online: https://myfcd.moh.gov.my/myfcd97/ (accessed on 27 October 2020).
- Franke, A.A.; Hankin, J.H.; Yu, M.C.; Maskarinec, G.; Low, S.H.; Custer, L.J. Isoflavone levels in soy foods consumed by multiethnic populations in Singapore and Hawaii. J. Agric. Food Chem. 1999, 47, 977–986. [Google Scholar] [CrossRef]
- Eriksson, M.; Li, J.; Leifland, K.; Czene, K.; Hall, P. A comprehensive tool for measuring mammographic density changes over time. Breast Cancer Res. Treat. 2018, 169, 371–379. [Google Scholar] [CrossRef]
- Samavat, H.; Ursin, G.; Emory, T.H.; Lee, E.; Wang, R.; Torkelson, C.J.; Dostal, A.M.; Swenson, K.; Le, C.T.; Yang, C.S.; et al. A randomized controlled trial of green tea extract supplementation and mammographic density in postmenopausal women at increased risk of breast cancer. Cancer Prev. Res. 2017, 10, 710–718. [Google Scholar] [CrossRef]
- Azam, S.; Eriksson, M.; Sjölander, A.; Hellgren, R.; Gabrielson, M.; Czene, K.; Hall, P. Mammographic Density Change and Risk of Breast Cancer. J. Natl. Cancer Inst. 2020, 112, 391–399. [Google Scholar] [CrossRef]
- Mokhtary, A.; Karakatsanis, A.; Valachis, A. Mammographic Density Changes over Time and Breast Cancer Risk: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 4805. [Google Scholar] [CrossRef] [PubMed]
- Shawky, M.S.; Martin, H.; Hugo, H.J.; Lloyd, T.; Britt, K.L.; Redfern, A.; Thompson, E.E.W. Mammographic density: A potential monitoring biomarker for adjuvant and preventative breast cancer endocrine therapies. Oncotarget 2017, 8, 5578. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; Warwick, J.; Pinney, E.; Duffy, S.W.; Cawthorn, S.; Howell, A.; Forbes, J.F.; Warren, R.M.L. Tamoxifen-induced reduction in mammographic density and breast cancer risk reduction: A nested case-control study. J. Natl. Cancer Inst. 2011, 103, 744–752. [Google Scholar] [CrossRef]
- Qin, L.-Q.; Xu, J.-Y.; Wang, P.-Y.; Hoshi, K. Soyfood Intake in the Prevention of Breast Cancer Risk in Women: A Meta-Analysis of Observational Epidemiological Studies; Center for Academic Publications Japan: Tokyo, Japan, 2006; Volume 52, pp. 428–436. [Google Scholar]
- Zhao, T.T.; Jin, F.; Li, J.G.; Xu, Y.Y.; Dong, H.T.; Liu, Q.; Xing, P.; Zhu, G.L.; Xu, H.; Miao, Z.F. Dietary isoflavones or isoflavone-rich food intake and breast cancer risk: A meta-analysis of prospective cohort studies. Clin. Nutr. 2019, 38, 136–145. [Google Scholar] [CrossRef]
- Wei, Y.; Lv, J.; Guo, Y.; Bian, Z.; Gao, M.; Du, H.; Yang, L.; Chen, Y.; Zhang, X.; Wang, T.; et al. Soy intake and breast cancer risk: A prospective study of 300,000 Chinese women and a dose–response meta-analysis. Eur. J. Epidemiol. 2020, 35, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Chatterton, R.T.; Michel, N.; Bryk, M.; Lee, O.; Ivancic, D.; Heinz, R.; Zalles, C.M.; Helenowski, I.B.; Jovanovic, B.D.; et al. Soy isoflavone supplementation for breast cancer risk reduction: A randomized phase II trial. Cancer Prev. Res. 2012, 5, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Korde, L.A.; Wu, A.H.; Fears, T.; Nomura, A.M.Y.; West, D.W.; Kolonel, L.N.; Pike, M.C.; Hoover, R.N.; Ziegler, R.G. Childhood soy intake and breast cancer risk in Asian American women. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1050–1059. [Google Scholar] [CrossRef]
- Messina, M. Impact of Soy Foods on the Development of Breast Cancer and the Prognosis of Breast Cancer Patients. Complement Med. Res. 2016, 23, 75–80. [Google Scholar] [CrossRef]
- Lee, S.A.; Shu, X.O.; Li, H.; Yang, G.; Cai, H.; Wen, W.; Ji, B.T.; Gao, J.; Gao, Y.T.; Zheng, W. Adolescent and adult soy food intake and breast cancer risk: Results from the Shanghai Women’s Health Study. Am. J. Clin. Nutr. 2009, 89, 1920–1926. [Google Scholar] [CrossRef]
- Eriksson, M.; Czene, K.; Conant, E.F.; Hall, P. Use of Low-Dose Tamoxifen to Increase Mammographic Screening Sensitivity in Premenopausal Women. Cancers 2021, 13, 302. [Google Scholar] [CrossRef]
- Ghosh, K.; Hartmann, L.C.; Reynolds, C.; Visscher, D.W.; Brandt, K.R.; Vierkant, R.A.; Scott, C.G.; Radisky, D.C.; Sellers, T.A.; Pankratz, V.S.; et al. Association between mammographic density and age-related lobular involution of the breast. J. Clin. Oncol. 2010, 28, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.; Martin, L.; Stone, J.; Little, L.; Minkin, S.; Yaffe, M. A Longitudinal Study of the Effects of Menopause on Mammographic Features1 | Cancer Epidemiology, Biomarkers & Prevention|American Association for Cancer Research. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1048–1053. [Google Scholar]
- Maskarinec, G.; Ju, D.; Horio, D.; Loo, L.W.M.; Hernandez, B.Y. Involution of breast tissue and mammographic density. Breast Cancer Res. 2016, 18, 128. [Google Scholar] [CrossRef]
- Milanese, T.R.; Hartmann, L.C.; Sellers, T.A.; Frost, M.H.; Vierkant, R.A.; Maloney, S.D.; Pankratz, V.S.; Degnim, A.C.; Vachon, C.M.; Reynolds, C.A.; et al. Age-related lobular involution and risk of breast cancer. J. Natl. Cancer Inst. 2006, 98, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Desroches, S.; Lapointe, A.; Ratté, S.; Gravel, K.; Légaré, F.; Turcotte, S. Interventions to enhance adherence to dietary advice for preventing and managing chronic diseases in adults. Cochrane Database Syst. Rev. 2013, 2013, CD008722. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Distribution of Participants by Study Arm | |||||
|---|---|---|---|---|---|
| Description of Follow Up | Overall (n = 118) | ISF Supplements (n = 41) | ISF Diet (n = 38) | Control (n = 39) | p Value |
| Follow up status, n (%) | |||||
| Completed | 91 (77.1) | 28 (68.3) | 30 (78.9) | 33 (84.6) | 0.225 |
| Lost in follow up | 27 (22.9) | 13 (31.7) | 8 (21.1) | 6 (15.4) | |
| Duration of follow up, months, median (IQR) | |||||
| Completed | 13.3 (1.4) | 13.5 (1.7) | 13.2 (1.3) | 13.2 (1.2) | 0.651 |
| Lost in follow up | 6.2 (8.8) | 6.4 (9.3) | 4.1 (5.9) | 8.1 (2.6) | 0.354 |
| Reasons for failure to follow up, n (%) | |||||
| Adverse events | 13 (48.1) | 8 (61.5) | 4 (50.0) | 1 (16.7) | 0.332 |
| No longer interested | 7 (25.9) | 2 (15.4) | 3 (37.5) | 2 (33.3) | |
| COVID-19 pandemic | 7 (25.9) | 3 (23.1) | 1 (12.5) | 3 (50.0) | |
| Distribution by Study Arm | |||||
|---|---|---|---|---|---|
| Characteristics | Overall (n = 90) | ISF Supplements (n = 27) | ISF Diet (n = 30) | Control (n = 33) | p Value |
| Demographic | |||||
| Age in years, median (IQR) | 57 (6.0) | 58 (5.0) | 56 (5.8) | 56 (8.0) | 0.470 |
| Ethnicity, n (%) | |||||
| Chinese | 71 (78.9) | 20 (74.1) | 25 (83.3) | 26 (78.8) | 0.781 |
| Indian | 11 (12.2) | 5 (18.5) | 2 (6.7) | 4 (12.1) | |
| Malay | 8 (8.9) | 2 (7.4) | 3 (10.0) | 3 (9.1) | |
| Education, n (%) | |||||
| Up to secondary | 28 (31.1) | 8 (29.6) | 12 (40.0) | 8 (24.2) | 0.410 |
| Tertiary | 61 (67.8) | 18 (66.7) | 18 (60.0) | 25 (75.8) | |
| Monthly household income, n (%) | |||||
| <RM 5000 | 33 (36.7) | 10 (37.0) | 12 (40.0) | 11 (33.3) | 0.987 |
| RM 5000–10,000 | 28 (31.1) | 8 (29.6) | 9 (30.0) | 11 (33.3) | |
| >RM 10,000 | 26 (28.9) | 8 (29.6) | 8 (26.7) | 10 (30.3) | |
| Reproductive | |||||
| No. of children, n (%) | |||||
| None | 17 (18.9) | 5 (18.5) | 7 (23.3) | 5 (15.2) | 0.746 |
| 1–2 | 40 (44.4) | 11 (40.7) | 15 (50.0) | 14 (42.4) | |
| >3 | 32 (35.6) | 10 (37.0) | 8 (26.7) | 14 (42.4) | |
| Menopausal status at enrolment, n (%) | |||||
| Peri-menopause | 9 (10.0) | 4 (14.8) | 2 (6.7) | 3 (9.1) | 0.618 |
| Post-menopause | 81 (90.0) | 23 (85.2) | 28 (93.3) | 30 (90.9) | |
| Age at last menstrual period, median (IQR) | 51 (5.5) | 52 (4.0) | 51 (5.0) | 49 (5.0) | 0.079 |
| Years since last menstrual period, n (%) | |||||
| Less than 5 years | 37 (41.1) | 10 (37.0) | 14 (46.7) | 13 (39.4) | 0.736 |
| 5 years or more | 50 (55.6) | 16 (59.3) | 15 (50.0) | 19 (57.6) | |
| History of hysterectomy or oophorectomy, n (%) | 10 (11.1) | 2 (7.4) | 2 (6.7) | 6 (18.2) | 0.310 |
| Use of oral contraceptives, n (%) | 29 (32.2) | 8 (29.6) | 11 (36.7) | 10 (30.3) | 0.847 |
| Family history and screening | |||||
| 1° Family history, n (%) | |||||
| Any cancer | 42 (46.7) | 16 (59.3) | 13 (43.3) | 13 (39.4) | 0.289 |
| Breast cancer | 11 (12.2) | 5 (18.5) | 3 (10.0) | 3 (9.1) | 0.475 |
| Last mammogram, n (%) | |||||
| 1–2 years | 27 (30.0) | 8 (29.6) | 10 (33.3) | 9 (27.3) | 0.405 |
| More than 2 years | 59 (65.6) | 18 (66.7) | 17 (56.7) | 24 (72.7) | |
| Never | 4 (4.4) | 1 (3.7) | 3 (10.0) | 0 (0) | |
| Lifestyle factors at enrolment | |||||
| BMI, kg/m2, n (%) | |||||
| <25 (low) | 53 (58.9) | 15 (55.6) | 17 (56.7) | 21 (63.6) | 0.800 |
| ≥25 (high) | 37 (41.1) | 12 (44.4) | 13 (43.3) | 12 (36.4) | |
| Physical activity, MET-hours/week, n (%) | |||||
| ≤10 (low) | 46 (51.1) | 16 (59.3) | 13 (43.3) | 17 (51.5) | 0.663 |
| >10 (moderate/high) | 41 (45.6) | 11 (40.7) | 15 (50.0) | 15 (45.5) | |
| Mammographic density at enrolment, median (IQR) | |||||
| Dense area, cm2 | 14.6 (18.7) | 19.9 (15.0) | 11.3 (19.3) | 7.6 (18.1) | 0.172 |
| Percent density, % | 12.7 (22.1) | 14.5 (21.4) | 9.0 (21.0) | 7.8 (22.4) | 0.200 |
| Distribution by Study Arm, Median (IQR) | ||||
|---|---|---|---|---|
| Measures | ISF Supplements (n = 27) | ISF Diet (n = 30) | Control (n = 33) | parm |
| Weight, kg | ||||
| At enrolment | 61.2 (11.8) | 59.1 (12.9) | 58.5 (13.3) | 0.931 |
| After 12 months | 61.5 (15.5) | 60.9 (14.7) | 58.8 (14.2) | 0.956 |
| pchange | 0.999 | 0.524 | 0.290 | |
| BMI, kg/m2 | ||||
| At enrolment | 24.2 (5.2) | 24.0 (4.2) | 23.0 (5.5) | 0.941 |
| After 12 months | 24.2 (5.7) | 24.3 (5.8) | 24.0 (5.3) | 0.967 |
| pchange | 0.878 | 0.503 | 0.272 | |
| Waist-to-hip ratio | ||||
| At enrolment | 0.9 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.545 |
| After 12 months | 0.8 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.834 |
| pchange | 0.934 | 0.598 | 0.177 | |
| Calorie intake, kcal/day | ||||
| At enrolment | 1528.1 (333.2) | 1586.5 (686.1) | 1528.7 (727.1) | 0.816 |
| After 12 months | 1496.2 (525.1) | 1788.9 (692.8) | 1556.4 (848.4) | 0.200 |
| pchange | 0.012 | 0.097 | 0.708 | |
| Carbohydrate intake, g/day | ||||
| At enrolment | 223.4 (91.9) | 239.8 (137.9) | 232.6 (132.2) | 0.946 |
| After 12 months | 228.1 (93.2) | 257.6 (109.8) | 242.8 (122.5) | 0.382 |
| pchange | 0.097 | 0.330 | 0.881 | |
| Protein intake, g/day | ||||
| At enrolment | 58.3 (22.2) | 54.4 (23.6) | 56.7 (30.0) | 0.424 |
| After 12 months | 51.5 (29.2) | 70.9 (23.6) | 59.6 (25.7) | 0.004 |
| pchange | 0.044 | 0.006 | 0.408 | |
| Fat, g/day | ||||
| At enrolment | 43.0 (20.4) | 37.0 (20.5) | 39.3 (24.3) | 0.084 |
| After 12 months | 42.5 (17.2) | 44.4 (22.9) | 39.3 (33.3) | 0.830 |
| pchange | 0.021 | 0.040 | 0.315 | |
| Soy isoflavone intake, mg/day | ||||
| At enrolment | 27.9 (25.6) | 17.6 (26.4) | 15.3 (17.2) | 0.121 |
| After 12 months | 101.4 (55.6) | 82.3 (39.1) | 18.1 (19.2) | <0.001 |
| pchange | <0.001 | <0.001 | 0.062 | |
| Change in Dense Area, Median (IQR) | |||||
|---|---|---|---|---|---|
| Study arm, by Type of Analysis | n | Absolute Change (cm2) | p Value | Relative Change (%) | p Value |
| All completed participants | |||||
| ISF Supplement | 27 | −1.3 (7.3) | 0.479 | −11.5 (43.8) | 0.999 |
| ISF Diet | 30 | −0.5 (4.5) | −10.9 (48.1) | ||
| Control | 33 | −0.8 (6.3) | −17.8 (51.6) | ||
| Per-protocol participants † | |||||
| ISF Supplement | 15 | −0.5 (8.4) | 0.659 | −11.1 (51.5) | 0.935 |
| ISF Diet | 24 | −0.5 (4.5) | −10.9 (47.6) | ||
| Control | 29 | −0.6 (6.3) | −17.8 (54.0) | ||
| Sensitivity analyses | |||||
| Excl. low MD at enrolment ‡ | |||||
| ISF Supplement | 23 | −1.7 (7.6) | 0.449 | −11.5 (35.5) | 0.372 |
| ISF Diet | 20 | −0.9 (5.0) | −2.3 (28.9) | ||
| Control | 21 | −1.0 (8.8) | −6.9 (47.4) | ||
| Excl. high enrolment isoflavone intake § | |||||
| ISF Supplement | 16 | −0.9 (6.2) | 0.573 | −10.3 (37.4) | 0.908 |
| ISF Diet | 20 | −0.5 (4.7) | −7.9 (49.8) | ||
| Control | 29 | −0.8 (6.3) | −17.8 (50.3) | ||
| By total isoflavone intake | |||||
| <18 mg/day | 23 | −0.8 (5.5) | 0.555 | −20.7 (55.8) | 0.610 |
| 18–61 mg/day | 22 | −1.8 (6.9) | −11.9 (56.0) | ||
| 61–101 mg/day | 21 | −1.3 (3.2) | −9.4 (34.9) | ||
| >101 mg/day | 24 | −0.2 (6.9) | −7.4 (50.1) | ||
| Description of Previous Mammogram and Change over Time | Distribution of MD Change by Study Arm | |||
|---|---|---|---|---|
| ISF Supplements (n = 19) | ISF Diet (n = 21) | Control (n = 22) | p Value | |
| Duration since previous mammogram in years, median (IQR) | 5.4 (2.1) | 6.7 (1.5) | 6.0 (2.1) | 0.103 |
| Menopause status at previous mammogram, n (%) | ||||
| Pre-menopause | 8 (42.1) | 4 (19.0) | 8 (36.4) | 0.593 |
| Peri-menopause | 3 (15.8) | 5 (23.8) | 4 (18.2) | |
| Post-menopause | 7 (36.8) | 11 (52.4) | 9 (40.9) | |
| Dense area in previous mammogram, cm2, median (IQR) | 29.3 (24.3) | 32.6 (27.5) | 33.7 (31.0) | 0.901 |
| Absolute change in dense area (cm2), median (IQR) | ||||
| Change prior to intervention | −6.5 (8.4) | −8.3 (14.6) | −9.4 (11.7) | 0.470 |
| Change during intervention | −1.9 (7.4) | −0.7 (5.0) | 0.1 (6.8) | 0.225 |
| Relative change in dense area (%), median (IQR) | ||||
| Change prior to intervention | −11.8 (57.9) | −39.7 (31.8) | −33.0 (30.3) | 0.292 |
| Change during intervention | −15.5 (35.4) | −7.4 (34.7) | −2.5 (32.9) | 0.460 |
| Distribution of Participants by Study Arm | |||||
|---|---|---|---|---|---|
| Adverse Events | Overall (n = 118) | ISF Supplements (n = 41) | ISF Diet (n = 38) | Control (n = 39) | p Value |
| Overall | 74 (62.7) | 32 (78.0) | 31 (81.6) | 11 (28.2) | <0.001 |
| Probably related | |||||
| Gastrointestinal complaints | 23 (19.5) | 10 (24.4) | 12 (31.6) | 1 (2.6) | 0.001 |
| Skin rash | 12 (10.2) | 4 (9.8) | 7 (18.4) | 1 (2.6) | 0.070 |
| Joint pains | 9 (7.6) | 5 (12.2) | 4 (10.5) | 0 (0) | 0.062 |
| Weight gain | 8 (6.8) | 2 (4.9) | 5 (13.2) | 1 (2.6) | 0.169 |
| Numbness | 3 (2.5) | 3 (7.3) | 0 (0) | 0 (0) | 0.106 |
| Uncertain | |||||
| High blood uric acid | 4 (3.4) | 3 (7.3) | 1 (2.6) | 0 (0) | 0.268 |
| Back pain | 4 (3.4) | 3 (7.3) | 1 (2.6) | 0 (0) | 0.268 |
| Headache | 3 (2.5) | 1 (2.4) | 2 (5.3) | 0 (0) | 0.422 |
| High blood glucose | 2 (1.7) | 0 (0) | 1 (2.6) | 1 (2.6) | 0.542 |
| High liver function tests | 2 (1.7) | 2 (4.9) | 0 (0) | 0 (0) | 0.328 |
| Changes to the breast | 2 (1.7) | 0 (0) | 1 (2.6) | 1 (2.6) | 0.543 |
| Vaginal discharge | 2 (1.7) | 2 (4.9) | 0 (0) | 0 (0) | 0.328 |
| Sleep disturbance | 2 (1.7) | 2 (4.9) | 0 (0) | 0 (0) | 0.328 |
| Uncertain, serious | |||||
| Brain aneurysm | 2 (1.7) | 2 (4.9) | 0 (0) | 0 (0) | 0.328 |
| Breast cancer | 1 (0.8) | 1 (2.4) | 0 (0) | 0 (0) | 0.322 |
| Post-menopausal bleeding | 1 (0.8) | 0 (0) | 1 (2.6) | 0 (0) | 0.322 |
| Unrelated | |||||
| Infection | 26 (22.0) | 10 (24.4) | 9 (23.7) | 7 (17.9) | 0.788 |
| Surgery | 6 (5.1) | 2 (4.9) | 2 (5.3) | 2 (5.1) | 0.999 |
| High blood pressure | 5 (4.2) | 2 (4.9) | 1 (2.6) | 2 (5.1) | 0.999 |
| Injury/accident | 3 (2.5) | 1 (2.4) | 1 (2.6) | 1 (2.6) | 0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajaram, N.; Yap, B.; Eriksson, M.; Mariapun, S.; Tan, L.M.; Sa’at, H.; Ho, E.L.M.; Taib, N.A.M.; Khor, G.L.; Yip, C.H.; et al. A Randomized Controlled Trial of Soy Isoflavone Intake on Mammographic Density among Malaysian Women. Nutrients 2023, 15, 299. https://doi.org/10.3390/nu15020299
Rajaram N, Yap B, Eriksson M, Mariapun S, Tan LM, Sa’at H, Ho ELM, Taib NAM, Khor GL, Yip CH, et al. A Randomized Controlled Trial of Soy Isoflavone Intake on Mammographic Density among Malaysian Women. Nutrients. 2023; 15(2):299. https://doi.org/10.3390/nu15020299
Chicago/Turabian StyleRajaram, Nadia, Beverley Yap, Mikael Eriksson, Shivaani Mariapun, Lee Mei Tan, Hamizah Sa’at, Evelyn Lai Ming Ho, Nur Aishah Mohd Taib, Geok Lin Khor, Cheng Har Yip, and et al. 2023. "A Randomized Controlled Trial of Soy Isoflavone Intake on Mammographic Density among Malaysian Women" Nutrients 15, no. 2: 299. https://doi.org/10.3390/nu15020299
APA StyleRajaram, N., Yap, B., Eriksson, M., Mariapun, S., Tan, L. M., Sa’at, H., Ho, E. L. M., Taib, N. A. M., Khor, G. L., Yip, C. H., Ho, W. K., Hall, P., & Teo, S. H. (2023). A Randomized Controlled Trial of Soy Isoflavone Intake on Mammographic Density among Malaysian Women. Nutrients, 15(2), 299. https://doi.org/10.3390/nu15020299