
Stance4Health Nutritional APP: A Path to Personalized Smart Nutrition

 ,
,  , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Development and Characteristics of the S4H APP
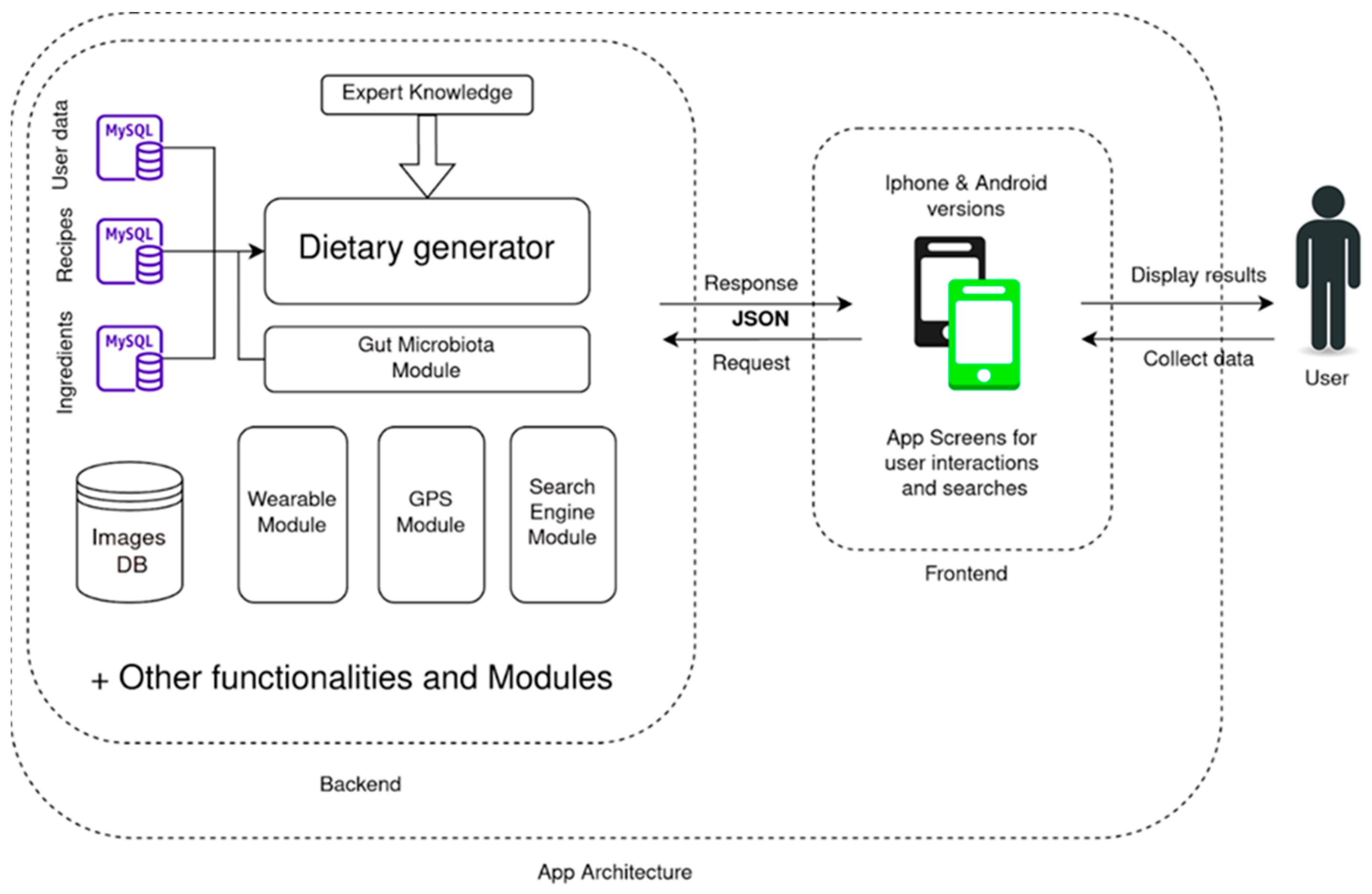
2.2. APP Architecture
2.3. Sources of Data
- User data: We store the main aspects of the user in a MySQL database, including information about biometrics, restrictions and behavior. This information allows us to calculate the nutrient levels we are aiming to recommend. At the same time, it also lets us filter several items in the dietary database that are not suited for the user, either due to age (as coffee or tea recipes in children) or to food allergies (not recommending milk-based products to users allergic to milk proteins). Other than hard restrictions, we also allow the users to check whether they dislike or like specific products and recipes in the dataset. The presence of preferences allows us to choose one recipe over the other when suggesting the menu. In this section, the user’s clinical history is also considered. Currently only the weight section (normal weight, overweight and obesity) and the allergy and intolerances are operational. This section can also take into account pathologies such as diabetes and hypertension. However, these options are currently inoperative as these options are not necessary for the target population of the nutritional interventions performed along the Stance4Health research project.
- Nutritional references: These data are summarized in tables that are used as rules to generate a healthy menu. They contain recommendations for a Mediterranean and sustainable diet [26]. The EU Dietary Reference Values (DRVs) are the reference values on which the nutritional recommendations of the APP are based [27]. This module, therefore, establishes basic rules such as portions of food groups needed per week, or micronutrient intake for a healthy diet.
- Ingredients data: The S4H APP contains multiple nutrient information from many stakeholders. Moreover, some of these data could be updated as new analysis and reviews are made. For that reason, nutritional information for every single ingredient is stored as another set of MySQL tables. Specifically, for this APP, we used the S4H food composition database (FCDB) developed within the framework of the project [28]. In summary, the S4H FCDB consists of more than 2600 foods with nutritional information on approximately 880 elements, including bioactive compounds. However, multiple elements can differ from one country to another. Moreover, several products are not consumed raw, but they undergo some kind of thermal processing. For that reason, our dataset contains a Branded Food Products Database consisting of food from supermarkets and hypermarkets of different countries (this is likely to be a significant percentage of the food already purchased and consumed by consumers). We specifically have detailed data from three different countries: Spain (with 89,385 foods products) provided by AECOC (Spanish Association of Manufacturers and Distributors), Germany (with 211,014 foods products) provided by ATRIFY and Greece (with 3312 foods products) provided by researchers [29]. We also included 670 different items from fast food restaurants obtained from the publications of the restaurant chains. These fast food items could be a recipe themselves, but as it is rare to solely eat one of them, we stored them as ingredients, to give the user more flexibility when entering the different menus which they could have eaten.
- Recipe data: S4H APP, unlike recent approaches in food recommendations, follows recipe-centered meal planning. This means that our system recommends to the user a specific recipe for a specific time of the day. Unlike a single combination of ingredients, recipes give ingredients a context/relationship and a procedure. This allows the user to know “what to eat” and “how to cook it”. This selection has its drawbacks, too, which are analyzed in the discussion section. The recipes were reviewed by inhabitants from each country: it started with the analysis of more than 150,000 recipes from all countries to obtain a set of some 20,000 appropriate recipes (in terms of nutritional value, cultural traditions and diversity in all the possible meal plans). This dataset of recipes was then evaluated in terms of its ingredients’ names, weight, retention factors and yield factors according to the cooking technique described for each recipe. Finally, we obtained the nutritional composition of each recipe [28]. Additionally, users can create their own recipes, with ingredients from the ingredients database. Those users’ recipes will only be available for the users that have created them.
- Expert knowledge: Despite recent trends in computational nutrition (that aims to provide automatic recommendations), having a source of expert knowledge has been proven as an excellent way to manage/rank all the nutritional goals and levels. Within this source, the APP includes:
- Food constraints related to health issues.
- Food levels related to age and biometrics.
- Food patterns that ensure a diverse diet.
- How several factors affect the previous items such as meal distribution, physical exercise and portion size.
2.4. Physical Activity
2.5. Portion Sizes
2.6. Additional Data Sources: Images, Barcodes and User Interaction
- Allows the user to see how a recipe looks when finished.
- Allows the user to identify ingredients easily.
- Allows the user to quickly check if they are using the correct product.
2.7. Generator
2.8. Gut Microbiota Module
2.9. Search Engine
- Camera-based interactions were primarily developed to allow users to have a quick interaction with commercial products as they may be the main source of deviation from the diet. This can be achieved through a comprehensive database linked to the commercial barcodes in the system. A user can easily scan a barcode with their smartphone and automatically find the product data in the APP database.
- Text-based interactions are based on similarity metrics of the text-chains introduced.
- Voice-based interaction runs on Google Voice recognition API.
2.10. Wearable
2.11. Shopping List and GPS Module
2.12. APP Testing and Validation
2.13. Security and Ethical Aspects of APP
2.14. Statistical Analysis
3. Results
3.1. Integration between Modules
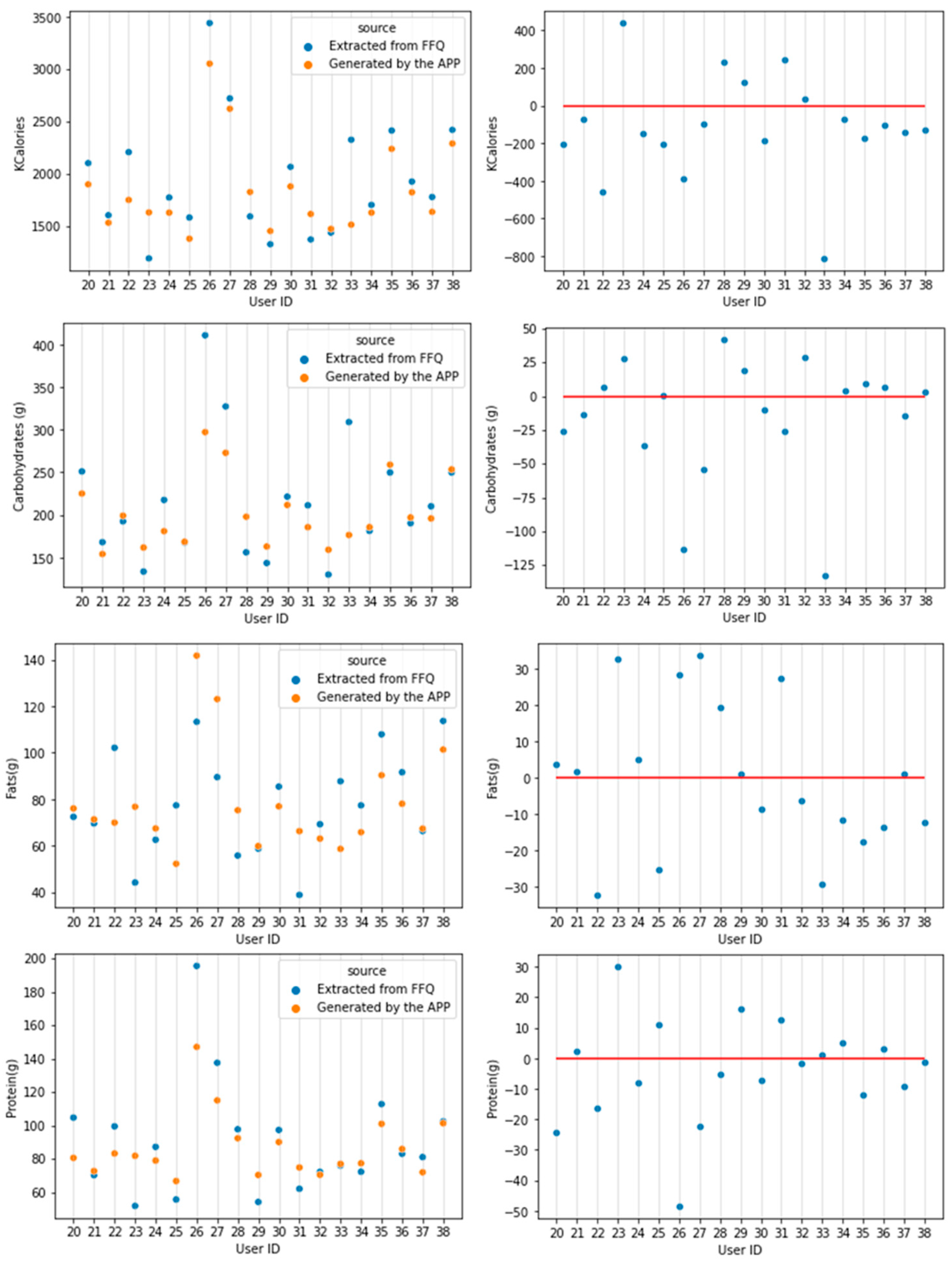
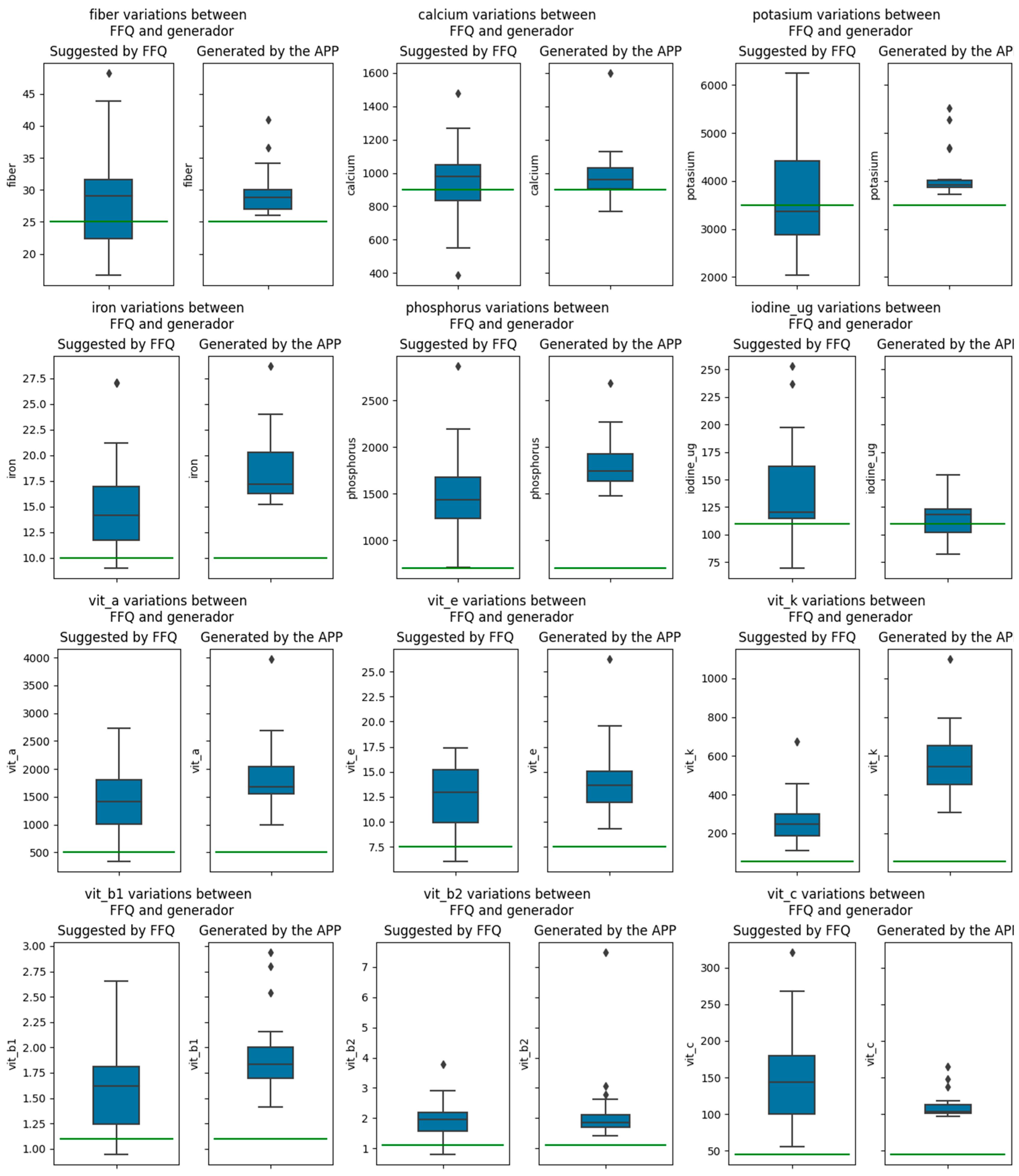
3.2. Testing the APP with Real Subjects
4. Discussion
4.1. Comparison of S4H APP with the Current Situation
4.2. S4H APP Security and Quality
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bzikowska-Jura, A.; Sobieraj, P.; Raciborski, F. Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study. Nutrients 2021, 13, 2868. [Google Scholar] [CrossRef] [PubMed]
- Röttger-Wirtz, S.; Alie, D. Personalised Nutrition: The EU’s Fragmented Legal Landscape and the Overlooked Implications of EU Food Law. Eur. J. Risk Regul. 2021, 12, 212–235. [Google Scholar] [CrossRef]
- Zarnowiecki, D.; Mauch, C.E.; Middleton, G.; Matwiejczyk, L.; Watson, W.L.; Dibbs, J.; Dessaix, A.; Golley, R.K. A Systematic Evaluation of Digital Nutrition Promotion Websites and Apps for Supporting Parents to Influence Children’s Nutrition. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ding, J.; Wang, Y.; Tang, C.; Zhang, P. Nutrition-Related Mobile Apps in the China App Store: Assessment of Functionality and Quality. JMIR MHealth UHealth 2019, 7, e13261. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Chung, C.; Woo, H. Diet-Related Mobile Apps to Promote Healthy Eating and Proper Nutrition: A Content Analysis and Quality Assessment. Int. J. Environ. Res. Public Health 2021, 18, 3496. [Google Scholar] [CrossRef]
- Sempionatto, J.R.; Montiel, V.R.-V.; Vargas, E.; Teymourian, H.; Wang, J. Wearable and Mobile Sensors for Personalized Nutrition. ACS Sens. 2021, 6, 1745–1760. [Google Scholar] [CrossRef]
- Pérez-Troncoso, D.; Epstein, D.M.; Castañeda-García, J.A. Consumers’ Preferences and Willingness to Pay for Personalised Nutrition. Appl. Health Econ. Health Policy 2021, 19, 757–767. [Google Scholar] [CrossRef]
- Vasiloglou, M.F.; Christodoulidis, S.; Reber, E.; Stathopoulou, T.; Lu, Y.; Stanga, Z.; Mougiakakou, S. What Healthcare Professionals Think of “Nutrition & Diet” Apps: An International Survey. Nutrients 2020, 12, 2214. [Google Scholar]
- Schoeppe, S.; Alley, S.; Rebar, A.L.; Hayman, M.; Bray, N.A.; Van Lippevelde, W.; Gnam, J.-P.; Bachert, P.; Direito, A.; Vandelanotte, C. Apps to Improve Diet, Physical Activity and Sedentary Behaviour in Children and Adolescents: A Review of Quality, Features and Behaviour Change Techniques. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–10. [Google Scholar] [CrossRef]
- Tomazic, T.; Jerkovic, O.S. Online Interventions for the Selective Prevention of Illicit Drug Use in Young Drug Users: Exploratory Study. J. Med. Internet Res. 2020, 22, e17688. [Google Scholar] [CrossRef]
- Robles, N.; Puig, E.P.; Gómez-Calderón, C.; Saigí-Rubió, F.; Cambra, G.C.; Zamora, A.; Moharra, M.; Paluzié, G.; Balfegó, M.; Carrion, C. Evaluation Criteria for Weight Management Apps: Validation Using a Modified Delphi Process. JMIR MHealth UHealth 2020, 8, e16899. [Google Scholar] [CrossRef] [PubMed]
- König, L.M.; Attig, C.; Franke, T.; Renner, B. Barriers to and Facilitators for Using Nutrition Apps: Systematic Review and Conceptual Framework. JMIR MHealth UHealth 2021, 9, e20037. [Google Scholar] [CrossRef] [PubMed]
- Vasiloglou, M.F.; Christodoulidis, S.; Reber, E.; Stathopoulou, T.; Lu, Y.; Stanga, Z.; Mougiakakou, S. Perspectives and Preferences of Adult Smartphone Users Regarding Nutrition and Diet Apps: Web-Based Survey Study. JMIR MHealth UHealth 2021, 9, e27885. [Google Scholar] [CrossRef] [PubMed]
- Mistura, L.; Comendador Azcarraga, F.J.; D’Addezio, L.; Martone, D.; Turrini, A. An Italian Case Study for Assessing Nutrient Intake through Nutrition-Related Mobile Apps. Nutrients 2021, 13, 3073. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Mauldin, K.; Manitius, N.; Jalilian, L.; Salonen, B.R. The Age of Artificial Intelligence: Use of Digital Technology in Clinical Nutrition. Curr. Surg. Rep. 2021, 9, 1–13. [Google Scholar] [CrossRef]
- Chen, J.; Allman-Farinelli, M. Impact of Training and Integration of Apps into Dietetic Practice on Dietitians’ Self-Efficacy with Using Mobile Health Apps and Patient Satisfaction. JMIR MHealth UHealth 2019, 7, e12349. [Google Scholar] [CrossRef]
- Eicher-Miller, H.A.; Prapkree, L.; Palacios, C. Expanding the Capabilities of Nutrition Research and Health Promotion through Mobile-Based Applications. Adv. Nutr. 2021, 12, 1032–1041. [Google Scholar] [CrossRef]
- West, J.H.; Belvedere, L.M.; Andreasen, R.; Frandsen, C.; Hall, P.C.; Crookston, B.T. Controlling Your “App” Etite: How Diet and Nutrition-Related Mobile Apps Lead to Behavior Change. JMIR MHealth UHealth 2017, 5, e7410. [Google Scholar] [CrossRef]
- Vasiloglou, M.F.; van der Horst, K.; Stathopoulou, T.; Jaeggi, M.P.; Tedde, G.S.; Lu, Y.; Mougiakakou, S. The Human Factor in Automated Image-Based Nutrition Apps: Analysis of Common Mistakes Using the GoFOOD Lite App. JMIR MHealth UHealth 2021, 9, e24467. [Google Scholar] [CrossRef]
- Jospe, M.R.; Fairbairn, K.A.; Green, P.; Perry, T.L. Diet App Use by Sports Dietitians: A Survey in Five Countries. JMIR MHealth UHealth 2015, 3, e3345. [Google Scholar] [CrossRef]
- Fallaize, R.; Franco, R.Z.; Pasang, J.; Hwang, F.; Lovegrove, J.A. Popular Nutrition-Related Mobile Apps: An Agreement Assessment against a UK Reference Method. JMIR MHealth UHealth 2019, 7, e9838. [Google Scholar] [CrossRef] [PubMed]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A Review and Content Analysis of Engagement, Functionality, Aesthetics, Information Quality, and Change Techniques in the Most Popular Commercial Apps for Weight Management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.L.; Khambalia, A.Z.; Perry, R.; Carty, D.; Hendrie, G.A.; Allman-Farinelli, M.A.; Garnett, S.P.; McNaughton, S.A.; Rangan, A.M.; Truby, H. Great ‘Appeal’but Not There yet: A Review of IPhone Nutrition Applications Relevant to Child Weight Management. Nutr. Diet. 2015, 72, 363–367. [Google Scholar] [CrossRef]
- Burillo, S.P.; Nogueira, D.H.; de la Cueva, S.P.; Henares, J.A.R. Nutrición Personalizada Inteligente. Aliment. Rev. Tecnol. E Hig. Los Aliment. 2019, 500, 25–29. [Google Scholar]
- Dello Russo, M.; Russo, P.; Rufián-Henares, J.Á.; Hinojosa-Nogueira, D.; Pérez-Burillo, S.; de la Cueva, S.P.; Rohn, S.; Fatouros, A.; Douros, K.; González-Vigil, V. The Stance4Health Project: Evaluating a Smart Personalised Nutrition Service for Gut Microbiota Modulation in Normal-and Overweight Adults and Children with Obesity, Gluten-Related Disorders or Allergy/Intolerance to Cow’s Milk. Foods 2022, 11, 1480. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; Ngo de la Cruz, J.; Bach-Faig, A.; Donini, L.M.; Medina, F.-X.; Belahsen, R. Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef]
- Dietary Reference Values|DRV Finder. Available online: https://multimedia.efsa.europa.eu/drvs/index.htm (accessed on 14 September 2022).
- Hinojosa-Nogueira, D.; Pérez-Burillo, S.; Navajas-Porras, B.; Ortiz-Viso, B.; de la Cueva, S.P.; Lauria, F.; Fatouros, A.; Priftis, K.N.; González-Vigil, V.; Rufián-Henares, J.Á. Development of an Unified Food Composition Database for the European Project “Stance4Health”. Nutrients 2021, 13, 4206. [Google Scholar] [CrossRef]
- Katidi, A.; Vlassopoulos, A.; Kapsokefalou, M. Development of the Hellenic Food Thesaurus (HelTH), a Branded Food Composition Database: Aims, Design and Preliminary Findings. Food Chem. 2021, 347, 129010. [Google Scholar] [CrossRef]
- United Nations University; World Health Organization. Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation: Rome (Italy), 17–24 October 2001; Food & Agriculture Org.: Rome, Italy, 2004; Volume 1, ISBN 92-5-105212-3. [Google Scholar]
- Al Marzooqi, H.M.; Burke, S.J.; Al Ghazali, M.R.; Duffy, E.; Al Yousuf, M.H.S. The Development of a Food Atlas of Portion Sizes for the United Arab Emirates. J. Food Compos. Anal. 2015, 43, 140–148. [Google Scholar] [CrossRef]
- Marcos Suarez, V.; Rubio Mañas, J.; Sanchidrián Fernández, R.; Robledo de Dios, T. Spanish National Dietary Survey on Children and Adolescents. EFSA Support. Publ. 2015, 12, 900E. [Google Scholar] [CrossRef]
- Marcos, S.V.; Rubio, M.J.; Sanchidrián, F.R.; de Robledo, D. Spanish National Dietary Survey in Adults, Elderly and Pregnant Women. EFSA Support. Publ. 2016, 13, 1053E. [Google Scholar] [CrossRef]
- Hinojosa-Nogueira, D. Elaboración y Manipulación de Formularios Creados con Google Forms en el Ámbito de la Investigación; Universidad de Granada: Granada, Spain, 2022. [Google Scholar] [CrossRef]
- Ortiz Viso, B. Evolutionary Approach in Recommendation Systems for Complex Structured Objects. In Proceedings of the 14th ACM Conference on Recommender Systems, Virtual, 22–26 September 2020; pp. 776–781. [Google Scholar]
- Blasco, T.; Pérez-Burillo, S.; Balzerani, F.; Hinojosa-Nogueira, D.; Lerma-Aguilera, A.; Pastoriza, S.; Cendoya, X.; Rubio, Á.; Gosalbes, M.J.; Jiménez-Hernández, N. An Extended Reconstruction of Human Gut Microbiota Metabolism of Dietary Compounds. Nat. Commun. 2021, 12, 4728. [Google Scholar] [CrossRef] [PubMed]
- Balzerani, F.; Hinojosa-Nogueira, D.; Cendoya, X.; Blasco, T.; Pérez-Burillo, S.; Apaolaza, I.; Francino, M.P.; Rufián-Henares, J.Á.; Planes, F.J. Prediction of Degradation Pathways of Phenolic Compounds in the Human Gut Microbiota through Enzyme Promiscuity Methods. NPJ Syst. Biol. Appl. 2022, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bertemes-Filho, P.; Morcelles, K.F. Wearable Bioimpedance Measuring Devices. In Medicine-Based Informatics and Engineering; Springer: Berlin/Heidelberg, Germany, 2022; pp. 81–101. [Google Scholar]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR MHealth UHealth 2015, 3, e3422. [Google Scholar] [CrossRef] [PubMed]
- DiFilippo, K.N.; Huang, W.; Chapman-Novakofski, K.M. A New Tool for Nutrition App Quality Evaluation (AQEL): Development, Validation, and Reliability Testing. JMIR MHealth UHealth 2017, 5, e7441. [Google Scholar] [CrossRef]
- Stoyanov, S.; Hides, L.; Kavanagh, D.; Wilson, H. Development and Validation of the User Version of the Mobile Application Rating Scale (UMARS). JMIR MHealth UHealth 2016, 4, e72. [Google Scholar] [CrossRef]
- Béjar, L.M.; García-Perea, M.D.; Reyes, Ó.A.; Vázquez-Limón, E. Relative Validity of a Method Based on a Smartphone App (Electronic 12-Hour Dietary Recall) to Estimate Habitual Dietary Intake in Adults. JMIR MHealth UHealth 2019, 7, e11531. [Google Scholar] [CrossRef]
- EUR-Lex—32016R0679—EN—EUR-Lex. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 14 September 2022).
- Team, T.P.D. Pandas-Dev/Pandas: Pandas 2022. Available online: https://github.com/pandas-dev/pandas (accessed on 5 December 2022).
- McKinney, W. Data Structures for Statistical Computing in Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; pp. 56–61. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- Waskom, M. Seaborn: Statistical Data Visualization. J. Open Source Softw. 2021, 6, 3021. [Google Scholar] [CrossRef]
- Hunter, J.D. Matplotlib: A 2D Graphics Environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Khazen, W.; Jeanne, J.-F.; Demaretz, L.; Schäfer, F.; Fagherazzi, G. Rethinking the Use of Mobile Apps for Dietary Assessment in Medical Research. J. Med. Internet Res. 2020, 22, e15619. [Google Scholar] [CrossRef] [PubMed]
- Mauch, C.E.; Wycherley, T.P.; Laws, R.A.; Johnson, B.J.; Bell, L.K.; Golley, R.K. Mobile Apps to Support Healthy Family Food Provision: Systematic Assessment of Popular, Commercially Available Apps. JMIR MHealth UHealth 2018, 6, e11867. [Google Scholar] [CrossRef] [PubMed]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The Effectiveness of App-based Mobile Interventions on Nutrition Behaviours and Nutrition-related Health Outcomes: A Systematic Review and Meta-analysis. Obes. Rev. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [PubMed]
- DiFilippo, K.N.; Huang, W.-H.; Andrade, J.E.; Chapman-Novakofski, K.M. The Use of Mobile Apps to Improve Nutrition Outcomes: A Systematic Literature Review. J. Telemed. Telecare 2015, 21, 243–253. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, C.F.; Karavetian, M.; Halfens, R.J.; Crutzen, R.; Khoja, L.; Schols, J.M. The Effects of Dietary Mobile Apps on Nutritional Outcomes in Adults with Chronic Diseases: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2019, 119, 626–651. [Google Scholar] [CrossRef] [PubMed]
- Bracken, M.L.; Waite, B.M. Self-Efficacy and Nutrition-Related Goal Achievement of MyFitnessPal Users. Health Educ. Behav. 2020, 47, 677–681. [Google Scholar] [CrossRef]
- Verónica, G.-V. i-Diet un Innovador y Sencillo Software para la Elaboración y Estimación de Dietas Personalizadas; Verónica González-Vigil: Oviedo, Spain, 2022. [Google Scholar]
- Carter, M.C.; Hancock, N.; Albar, S.A.; Brown, H.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S.; Wark, P.A.; Cade, J.E. Development of a New Branded UK Food Composition Database for an Online Dietary Assessment Tool. Nutrients 2016, 8, 480. [Google Scholar] [CrossRef]
- Gurinović, M.; Milešević, J.; Kadvan, A.; Nikolić, M.; Zeković, M.; Djekić-Ivanković, M.; Dupouy, E.; Finglas, P.; Glibetić, M. Development, Features and Application of DIET ASSESS & PLAN (DAP) Software in Supporting Public Health Nutrition Research in Central Eastern European Countries (CEEC). Food Chem. 2018, 238, 186–194. [Google Scholar]
- Braz, V.N.; de Moraes Lopes, M.H.B. Evaluation of Mobile Applications Related to Nutrition. Public Health Nutr. 2019, 22, 1209–1214. [Google Scholar] [CrossRef]
- Mandracchia, F.; Llauradó, E.; Tarro, L.; Valls, R.M.; Solà, R. Mobile Phone Apps for Food Allergies or Intolerances in App Stores: Systematic Search and Quality Assessment Using the Mobile App Rating Scale (MARS). JMIR MHealth UHealth 2020, 8, e18339. [Google Scholar] [CrossRef]
- Javadi, B.; Calheiros, R.N.; Matawie, K.M.; Ginige, A.; Cook, A. Smart Nutrition Monitoring System Using Heterogeneous Internet of Things Platform; Springer: Berlin/Heidelberg, Germany, 2017; pp. 63–74. [Google Scholar]
- Spector, T.; Asnicar, F.; Berry, S.; Valdes, A.; Franks, P.; Wolf, J.; Hadjigeorgiou, G.; Roy, C.L.; Leeming, E.; Drew, D. Microbiome Signatures of Nutrients, Foods and Dietary Patterns: Potential for Personalized Nutrition from The PREDICT 1 Study. Curr. Dev. Nutr. 2020, 4, 1587. [Google Scholar] [CrossRef]
- Berry, S.; Valdes, A.; Segata, N.; Chan, A.; Davies, R.; Drew, D.; Franks, P.; Spector, T. Personal Metabolic Responses to Food Predicted Using Multi-Omics Machine Learning in 1,100 Twins and Singletons: The PREDICT I Study. Proc. Nutr. Soc. 2020, 79. [Google Scholar] [CrossRef]
- Navajas-Porras, B.; Pérez-Burillo, S.; Hinojosa-Nogueira, D.; Douros, K.; Pastoriza, S.; Rufián-Henares, J.Á. The Gut Microbiota of Obese Children Releases Lower Antioxidant Capacity from Food than That of Lean Children. Nutrients 2022, 14, 2829. [Google Scholar] [CrossRef] [PubMed]
- Asnicar, F.; Berry, S.E.; Valdes, A.M.; Nguyen, L.H.; Piccinno, G.; Drew, D.A.; Leeming, E.; Gibson, R.; Le Roy, C.; Khatib, H.A. Microbiome Connections with Host Metabolism and Habitual Diet from 1098 Deeply Phenotyped Individuals. Nat. Med. 2021, 27, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Camblor-Álvarez, M.; Ocón-Bretón, M.-J.; Luengo-Pérez, L.-M.; Virizuela, J.-A.; Sendrós-Madroño, M.-J.; Cervera-Peris, M.; Grande, E.; Álvarez-Hernández, J.; Jiménez-Fonseca, P. Soporte Nutricional y Nutrición Parenteral En El Paciente Oncológico: Informe de Consenso de Un Grupo de Expertos. Nutr. Hosp. 2018, 35, 224–233. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kcal | Carbohydrates (g) | Fats (g) | Proteins (g) | |
|---|---|---|---|---|
| Average | −111.7 | −14.6 | −0.1 | −4.0 |
| Standard deviation | 273.2 | 45.1 | 20.5 | 17.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hinojosa-Nogueira, D.; Ortiz-Viso, B.; Navajas-Porras, B.; Pérez-Burillo, S.; González-Vigil, V.; de la Cueva, S.P.; Rufián-Henares, J.Á. Stance4Health Nutritional APP: A Path to Personalized Smart Nutrition. Nutrients 2023, 15, 276. https://doi.org/10.3390/nu15020276
Hinojosa-Nogueira D, Ortiz-Viso B, Navajas-Porras B, Pérez-Burillo S, González-Vigil V, de la Cueva SP, Rufián-Henares JÁ. Stance4Health Nutritional APP: A Path to Personalized Smart Nutrition. Nutrients. 2023; 15(2):276. https://doi.org/10.3390/nu15020276
Chicago/Turabian StyleHinojosa-Nogueira, Daniel, Bartolomé Ortiz-Viso, Beatriz Navajas-Porras, Sergio Pérez-Burillo, Verónica González-Vigil, Silvia Pastoriza de la Cueva, and José Ángel Rufián-Henares. 2023. "Stance4Health Nutritional APP: A Path to Personalized Smart Nutrition" Nutrients 15, no. 2: 276. https://doi.org/10.3390/nu15020276
APA StyleHinojosa-Nogueira, D., Ortiz-Viso, B., Navajas-Porras, B., Pérez-Burillo, S., González-Vigil, V., de la Cueva, S. P., & Rufián-Henares, J. Á. (2023). Stance4Health Nutritional APP: A Path to Personalized Smart Nutrition. Nutrients, 15(2), 276. https://doi.org/10.3390/nu15020276