

Changes in the Sodium Content in Branded Foods in the Slovenian Food Supply (2011–2020)

 ,
,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Datasets and Methods
2.1. Datasets, Data Collection, and Processing
2.2. Sodium Content in Foods
- ci … sodium content in specific food (i), included in the food (sub)category;
- mi … yearly amount of sold specific food (i);
- i … 1 → n (for all products in selected food (sub)category).
2.3. Major Sodium Sources in Branded Foods
- k … 1 → n (for all included food categories).
2.4. Foods with Excessive Sodium Content
2.5. Data Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef]
- WHO. Fact Sheets: Cardiovascular Diseases (CVDs). Available online: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 25 July 2022).
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- WHO. Fact Sheets: Salt Reduction. Available online: https://www.who.int/news-room/fact-sheets/detail/salt-reduction (accessed on 25 July 2022).
- Bhat, S.; Marklund, M.; Henry, M.E.; Appel, L.J.; Croft, K.D.; Neal, B.; Wu, J.H.Y. A Systematic Review of the Sources of Dietary Salt Around the World. Adv. Nutr. 2020, 11, 677–686. [Google Scholar] [CrossRef]
- Kloss, L.; Meyer, J.D.; Graeve, L.; Vetter, W. Sodium intake and its reduction by food reformulation in the European Union—A review. NFS J. 2015, 1, 9–19. [Google Scholar] [CrossRef]
- Kwong, E.J.L.; Whiting, S.; Bunge, A.C.; Leven, Y.; Breda, J.; Rakovac, I.; Cappuccio, F.P.; Wickramasinghe, K. Population-level salt intake in the WHO European Region in 2022: A systematic review. Public Health Nutr. 2022, 1–14. [Google Scholar] [CrossRef]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [PubMed]
- Stuckler, D.; McKee, M.; Ebrahim, S.; Basu, S. Manufacturing Epidemics: The Role of Global Producers in Increased Consumption of Unhealthy Commodities Including Processed Foods, Alcohol, and Tobacco. PLoS Med. 2012, 9, e1001235. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Noncommunicable Diseases. Available online: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf (accessed on 25 July 2022).
- WHO. The SHAKE Technical Package for Salt Reduction. Available online: https://apps.who.int/iris/bitstream/handle/10665/250135/9789241511346-eng.pdf (accessed on 25 July 2022).
- WHO. WHO Global Sodium Benchmarks for Different Food Categories. Available online: https://apps.who.int/iris/rest/bitstreams/1344511/retrieve (accessed on 25 July 2022).
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N.; Rodriguez-Fernandez, R.; Legetic, B.; McLaren, L.; Barberio, A.; Webster, J. Salt Reduction Initiatives around the World—A Systematic Review of Progress towards the Global Target. PLoS ONE 2015, 10, e0130247. [Google Scholar] [CrossRef] [PubMed]
- Hope, S.F.; Webster, J.; Trieu, K.; Pillay, A.; Ieremia, M.; Bell, C.; Snowdon, W.; Neal, B.; Moodie, M. A systematic review of economic evaluations of population-based sodium reduction interventions. PLoS ONE 2017, 12, e0173600. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Global Report on Sodium Intake Reduction; WHO: Geneva, Switzerland, 2023; p. 99. ISBN 978-92-4-006998-5. Available online: https://www.who.int/publications/i/item/9789240069985 (accessed on 5 September 2023).
- Santos, J.A.; Sparks, E.; Thout, S.R.; McKenzie, B.; Trieu, K.; Hoek, A.; Johnson, C.; McLean, R.; Arcand, J.; Campbell, N.R.C.; et al. The Science of Salt: A global review on changes in sodium levels in foods. J. Clin. Hypertens. 2019, 21, 1043–1056. [Google Scholar] [CrossRef]
- Mhurchu, C.N.; Capelin, C.; Dunford, E.K.; Webster, J.L.; Neal, B.C.; Jebb, S.A. Sodium content of processed foods in the United Kingdom: Analysis of 44,000 foods purchased by 21,000 households. Am. J. Clin. Nutr. 2011, 93, 594–600. [Google Scholar] [CrossRef]
- Coyle, D.H.; Wu, J.H.; Di Tanna, G.L.; Shahid, M.; Taylor, F.; Neal, B.; Trevena, H. The Effects of a Supermarket-Based Intervention on the Nutritional Quality of Private-Label Foods: A Prospective Study. Nutrients 2020, 12, 1692. [Google Scholar] [CrossRef] [PubMed]
- George Institute for Global Health. Food Composition Database, Version 2014; The George Institute for Global Health Sydney: Newtown, Australia, 2014. [Google Scholar]
- Ribic, C.H.; Zakotnik, J.M.; Vertnik, L.; Vegnuti, M.; Cappuccio, F.P. Salt intake of the Slovene population assessed by 24 h urinary sodium excretion. Public Health Nutr. 2010, 13, 1803–1809. [Google Scholar] [CrossRef]
- MZ. National Action Plan for Reducing the Consumption of Salt in the Diet of the Population of Slovenia for the Period 2010–2020 (In Slovenian: Nacionalni Akcijski Načrt za Zmanjševanje Uživanja Soli v Prehrani Prebivalcev Slovenije za Obdobje 2010–2020). Available online: http://www.mz.gov.si/fileadmin/mz.gov.si/pageuploads/mz_dokumenti/delovna_podrocja/javno_zdravje/petric/Nacio_akcijski_nacrt_za_zmanj_uziv_soli_v_prehrani_preb_Slo_2010-2010.pdf (accessed on 27 June 2017).
- WHO. Mapping Salt Reduction Initiatives in the WHO European Region. Available online: https://www.euro.who.int/__data/assets/pdf_file/0009/186462/Mapping-salt-reduction-initiatives-in-the-WHO-European-Region-final.pdf (accessed on 25 July 2022).
- RS. National Program on Nutrition and Health Enhancing Physical Activity 2015–2025; Uradni list Republike Slovenije: Ljubljana, Slovenia, 2015. [Google Scholar]
- Korosec, Z.; Pravst, I. Assessing the average sodium content of prepacked foods with nutrition declarations: The importance of sales data. Nutrients 2014, 6, 3501–3515. [Google Scholar] [CrossRef] [PubMed]
- Pravst, I.; Lavriša, Ž.; Kušar, A.; Miklavec, K.; Žmitek, K. Changes in Average Sodium Content of Prepacked Foods in Slovenia during 2011–2015. Nutrients 2017, 9, 952. [Google Scholar] [CrossRef]
- Pravst, I.; Hribar, M.; Žmitek, K.; Blažica, B.; Korousic Seljak, B.; Kušar, A. Branded foods databases as a tool to support nutrition research and monitoring of the food supply: Insights from the Slovenian Composition and Labelling Information System (CLAS). Front. Nutr. 2022, 8, 798576. [Google Scholar] [CrossRef]
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Ni Mhurchu, C.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.K.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef]
- Pan American Health Organization (PAHO). Pan American Health Organization Nutrient Profile Model. Available online: https://iris.paho.org/bitstream/handle/10665.2/18621/9789275118733_eng.pdf (accessed on 8 September 2020).
- Clapp, J.E.; Niederman, S.A.; Leonard, E.; Curtis, C.J. Changes in Serving Size, Calories, and Sodium Content in Processed Foods From 2009 to 2015. Prev. Chronic Dis. 2018, 15, E33. [Google Scholar] [CrossRef]
- Beltrá, M.; Borrás, F.; Ropero, A.B. Sodium Content of Foods Sold in the Spanish Market. Results from the BADALI Project. Nutrients 2021, 13, 3410. [Google Scholar] [CrossRef] [PubMed]
- Inguglia, E.S.; Zhang, Z.; Tiwari, B.K.; Kerry, J.P.; Burgess, C.M. Salt reduction strategies in processed meat products—A review. Trends Food Sci. Technol. 2017, 59, 70–78. [Google Scholar] [CrossRef]
- Duranton, F.; Guillou, S.; Simonin, H.; Chéret, R.; de Lamballerie, M. Combined use of high pressure and salt or sodium nitrite to control the growth of endogenous microflora in raw pork meat. Innov. Food Sci. Emerg. Technol. 2012, 16, 373–380. [Google Scholar] [CrossRef]
- Petit, G.; Jury, V.; de Lamballerie, M.; Duranton, F.; Pottier, L.; Martin, J.-L. Salt Intake from Processed Meat Products: Benefits, Risks and Evolving Practices. Compr. Rev. Food Sci. Food Saf. 2019, 18, 1453–1473. [Google Scholar] [CrossRef]
- Shan, L.C.; Regan, Á.; Monahan, F.J.; Li, C.; Lalor, F.; Murrin, C.; Wall, P.G.; McConnon, Á. Consumer preferences towards healthier reformulation of a range of processed meat products. Br. Food J. 2017, 119, 2013–2026. [Google Scholar] [CrossRef]
- Guàrdia, M.D.; Guerrero, L.; Gelabert, J.; Gou, P.; Arnau, J. Consumer attitude towards sodium reduction in meat products and acceptability of fermented sausages with reduced sodium content. Meat Sci. 2006, 73, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Zhekov, Z.G.; Owens, C.M.; Kim, M.; Meullenet, J.F. Effects of Partial and Complete Replacement Of Sodium Chloride With Potassium Chloride On The Texture, Flavor And Water-Holding Capacity of Marinated Broiler Breast Fillets. J. Texture Stud. 2012, 43, 124–132. [Google Scholar] [CrossRef]
- Hao, Z.; Liang, L.; Pu, D.; Yuyu, Z. Analysis of Sodium Content in 4082 Kinds of Commercial Foods in China. Nutrients 2022, 14, 2908. [Google Scholar] [CrossRef]
- Allemandi, L.; Tiscornia, M.V.; Guarnieri, L.; Castronuovo, L.; Martins, E. Monitoring Sodium Content in Processed Foods in Argentina 2017–2018: Compliance with National Legislation and Regional Targets. Nutrients 2019, 11, 1474. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.A.; de Sousa, A.A.; Veiros, M.B.; González-Chica, D.A.; Proença, R.P.d.C. Sodium content and labelling of processed and ultra-processed food products marketed in Brazil. Public Health Nutr. 2014, 18, 1206–1214. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Dunford, E.; Ware, L.J.; Harris, T.; Walker, A.; Wicks, M.; Van Zyl, T.; Swanepoel, B.; Charlton, K.E.; Woodward, M.; et al. The Sodium Content of Processed Foods in South Africa during the Introduction of Mandatory Sodium Limits. Nutrients 2017, 9, 404. [Google Scholar] [CrossRef]
- IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. In Red Meat and Processed Meat; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Bansal, V.; Mishra, S.K. Reduced-sodium cheeses: Implications of reducing sodium chloride on cheese quality and safety. Compr. Rev. Food Sci. Food Saf. 2020, 19, 733–758. [Google Scholar] [CrossRef]
- Luzzi, G.; Brinks, E.; Fritsche, J.; Franz, C. Effect of reduction of sodium content on the microbial ecology of Edam cheese samples. AMB Express 2021, 11, 28. [Google Scholar] [CrossRef]
- Rýdlová, L.; Hrubá, M.; Škorpilová, T.; Pivoňka, J.; Tobolka, A.; Suchopárová, M.; Rajchl, A. Sodium content of foods sold in the Czech market. Int. J. Gastron. Food Sci. 2022, 28, 100526. [Google Scholar] [CrossRef]
- EC. Farm to Fork Strategy. Available online: https://food.ec.europa.eu/system/files/2020-05/f2f_action-plan_2020_strategy-info_en.pdf (accessed on 25 June 2022).
- Hlastan Ribič, C.; Zakotnik, J.M.; Seljak, K.B.; Poličnik, R.; Blaznik, U.; Mis, F.N.; Eržen, I.; Ji, C.; Cappucio, F.P. Estimation of sodium availability in food in Slovenia: Results from household food purchase data from 2000 to 2009. Slov. J. Publ. Health 2014, 53, 209. [Google Scholar] [CrossRef]
- Pérez Farinós, N.; Santos Sanz, S.; Dal Re, M.Á.; Yusta Boyo, J.; Robledo, T.; Castrodeza, J.J.; Campos Amado, J.; Villar, C. Salt content in bread in Spain, 2014. Nutr. Hosp. 2018, 35, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Vega-Solano, J.; Blanco-Metzler, A.; Benavides-Aguilar, K.F.; Arcand, J. An Evaluation of the Sodium Content and Compliance with the National Sodium Reduction Targets among Packaged Foods Sold in Costa Rica in 2015 and 2018. Nutrients 2019, 11, 2226. [Google Scholar] [CrossRef] [PubMed]
- Coyne, K.J.; Baldridge, A.S.; Huffman, M.D.; Jenner, K.; Xavier, D.; Dunford, E.K. Differences in the sodium content of bread products in the USA and UK: Implications for policy. Public Health Nutr. 2017, 21, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Carcea, M.; Narducci, V.; Turfani, V.; Aguzzi, A. A Survey of Sodium Chloride Content in Italian Artisanal and Industrial Bread. Foods 2018, 7, 181. [Google Scholar] [CrossRef]
- Gregorič, M.; Hristov, H.; Blaznik, U.; Koroušič Seljak, B.; Delfar, N.; Pravst, I. Dietary Intakes of Slovenian Adults and Elderly: Design and Results of National Dietary Study SI.Menu 2017/18. Nutrients 2022, 14, 3618. [Google Scholar] [CrossRef]
- CBL. National Agreement to Improve Product Composition 2014–2020. Available online: http://www.akkoordverbeteringproductsamenstelling.nl/en (accessed on 30 April 2020).
- Batenburg, M.; Landrieu, E.; van der Velden, R. Chapter 108—Compensation of Salt Reduction with Aroma Compounds. In Flavour Science; Ferreira, V., Lopez, R., Eds.; Academic Press: San Diego, CA, USA, 2014; pp. 589–595. [Google Scholar]
- Kuhar, A.; Korosec, M.; Bolha, A.; Pravst, I.; Hristov, H. Is a Consumer Perception of Salt Modification a Sensory or a Behavioural Phenomenon? Insights from a Bread Study. Foods 2020, 9, 1172. [Google Scholar] [CrossRef]
- Riis, N.L.; Bjoernsbo, K.S.; Toft, U.; Trolle, E.; Hyldig, G.; Hartley, I.E.; Keast, R.; Lassen, A.D. Impact of salt reduction interventions on salt taste sensitivity and liking, a cluster randomized controlled trial. Food Qual. Prefer. 2021, 87, 104059. [Google Scholar] [CrossRef]
- Dunteman, A.; Yang, Y.; McKenzie, E.; Lee, Y.; Lee, S.-Y. Sodium reduction technologies applied to bread products and their impact on sensory properties: A review. Int. J. Food Sci. Technol. 2021, 56, 4396–4407. [Google Scholar] [CrossRef]
- Gressier, M.; Sassi, F.; Frost, G. Healthy Foods and Healthy Diets. How Government Policies Can Steer Food Reformulation. Nutrients 2020, 12, 1992. [Google Scholar] [CrossRef]
- Vargas-Meza, J.; Gonzalez-Rocha, A.; Campos-Nonato, I.; Nilson, E.A.F.; Basto-Abreu, A.; Barquera, S.; Denova-Gutiérrez, E. Effective and Scalable Interventions to Reduce Sodium Intake: A Systematic Review and Meta-Analysis. Curr. Nutr. Rep. 2023, 12, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Rosewarne, E.; Santos, J.A.; Trieu, K.; Tekle, D.; Mhurchu, C.N.; Jones, A.; Ide, N.; Yamamoto, R.; Nishida, C.; Webster, J. A Global Review of National Strategies to Reduce Sodium Concentrations in Packaged Foods. Adv. Nutr. 2022, 13, 1820–1833. [Google Scholar] [CrossRef] [PubMed]
- Van der Westhuizen, B.; Frank, T.; Karim, S.A.; Swart, R.E.C. Determining food industry compliance to mandatory sodium limits: Successes and challenges from the South African experience. Public Health Nutr. 2023, 1–8. [Google Scholar] [CrossRef]
- Strauss-Kruger, M.; Wentzel-Viljoen, E.; Ware, L.J.; Van Zyl, T.; Charlton, K.; Ellis, S.; Schutte, A.E. Early evidence for the effectiveness of South Africa s legislation on salt restriction in foods: The African-PREDICT study. J. Hum. Hypertens. 2023, 37, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Rosewarne, E.; Santos, J.A.; Di Tanna, G.L.; Shahid, M.; Grimes, C.; Bolton, K.A.; Webster, J.; Neal, B.; Woodward, M.; Coyle, D.; et al. Changes in sodium levels in Australian packaged foods between 2014 and 2019: An interrupted time series analysis of the impact of the Victorian Salt Reduction Partnership’s media advocacy strategy. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 71. [Google Scholar] [CrossRef]
- Bandy, L.K.; Hollowell, S.; Jebb, S.A.; Scarborough, P. Changes in the salt content of packaged foods sold in supermarkets between 2015-2020 in the United Kingdom: A repeated cross-sectional study. PLoS Med. 2022, 19, e1004114. [Google Scholar] [CrossRef]
- EC. Regulation (EU) no 1169/2011 on the Provision of Food Information to Consumers. Available online: http://data.europa.eu/eli/reg/2011/1169/2018-01-01 (accessed on 27 September 2021).
- Hafner, E.; Lavrisa, A.; Hribar, M.; Krusic, S.; Kusar, A.; Zmitek, K.; Skrt, M.; Ulrih, N.P.; Pravst, I. Verifying the Use of Food Labeling Data for Compiling Branded Food Databases: A Case Study of Sugars in Beverages. Front. Nutr. 2022, 9, 794468. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Food Factory | 2020 | 2017 | Median Diff. 2020/2017 p-Value | SSC Ratio 2020/2017 (%) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % LSC | Sodium Content (mg per 100 g/mL) | High Na (%) | SW High Na (%) | STSS (%) | N | % LSC | Sodium Content (mg per 100 g/mL) | High Na (%) | SW High Na (%) | STSS (%) | |||||||||
| P25 | Med. | P75 | SSC | P25 | Med. | P75 | SSC | |||||||||||||
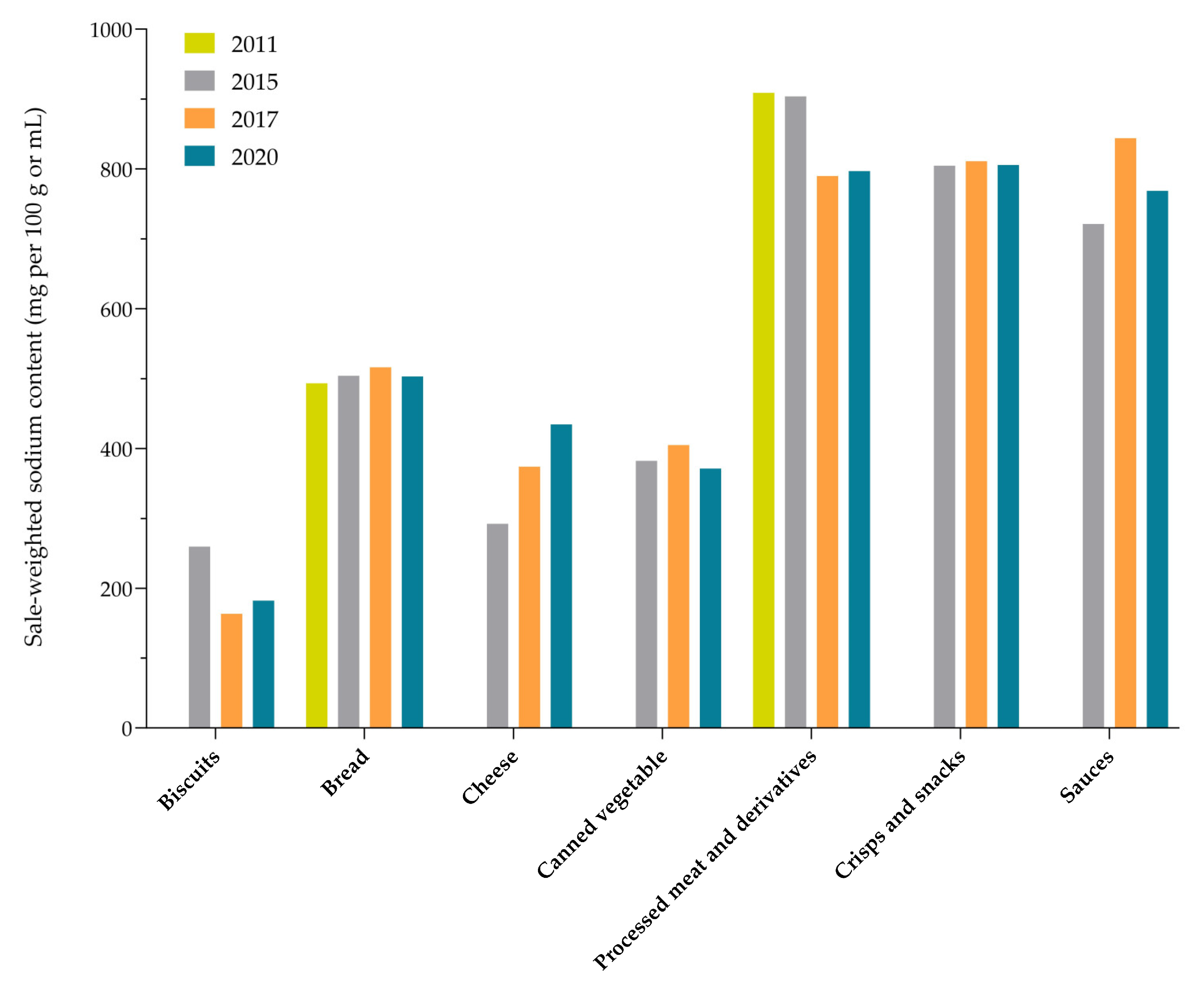
| Bread | 413 | 93 | 440 | 520 | 720 | 504 | 90 | 97 | 8.6 | 361 | 98 | 440 | 520 | 700 | 517 | 89 | 96 | 9 | 0.499 | 97 |
| - Plain bread | 169 | 91 | 440 | 480 | 520 | 486 | 99 | 100 | 6.3 | 134 | 97 | 440 | 480 | 520 | 489 | 95 | 99 | 5.3 | 0.855 | 100 |
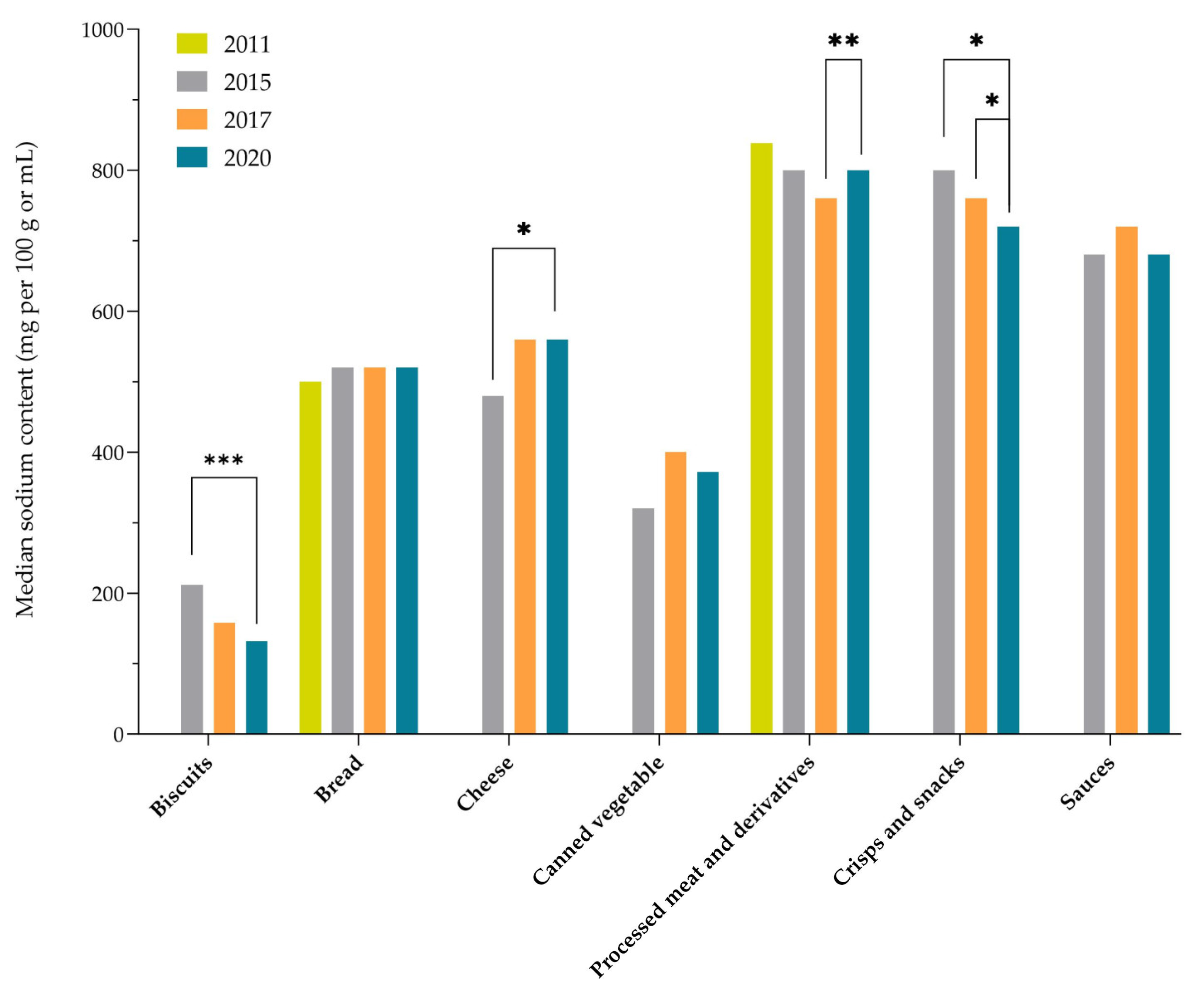
| Biscuits | 770 | 98 | 64 | 132 | 240 | 182 | 4 | 3 | 2.3 | 707 | 95 | 80 | 152 | 260 | 163 | 5 | 3 | 3 | 0.091 | 112 |
| Cakes, muffins, and pastries | 376 | 98 | 92 | 188 | 320 | 191 | 17 | 12 | 0.9 | 344 | 92 | 80 | 180 | 280 | 214 | 13 | 18 | 1.4 | 0.477 | 90 |
| Breakfast cereals | 418 | 99 | 16 | 96 | 212 | 193 | 7 | 16 | 1.0 | 320 | 95 | 16 | 100 | 254 | 218 | 13 | 22 | 1.4 | 0.654 | 89 |
| Pasta | 744 | 97 | 4 | 10.2 | 110 | 123 | 18 | 20 | 1.8 | 633 | 94 | 4 | 12 | 88 | 129 | 21 | 22 | 2.2 | 0.916 | 96 |
| - Noodles | 62 | 98 | 12 | 40 | 400 | 370 | 23 | 40 | 0.5 | 87 | 92 | 16 | 40 | 720 | 263 | 29 | 28 | 0.7 | 0.866 | 141 |
| - Dry pasta | 569 | 96 | 2.8 | 4 | 40 | 30 | 5 | 2 | 0.3 | 445 | 95 | 2.8 | 5.2 | 32 | 31 | 5 | 3 | 0.4 | 0.393 | 96 |
| Pizza | 25 | 100 | 440 | 520 | 560 | 494 | 100 | 100 | 0.1 | 26 | 100 | 480 | 514 | 572 | 523 | 100 | 100 | 0.2 | 0.921 | 94 |
| Soup (prepared) | 197 | 100 | 312 | 360 | 400 | 369 | NA | NA | 0.5 | 206 | 99 | 338 | 374 | 409 | 380 | NA | NA | 0.9 | 0.018 * | 97 |
| Ready meals | 212 | 83 | 288 | 400 | 520 | 442 | 88 | 98 | 1.4 | 187 | 89 | 320 | 400 | 520 | 441 | 98 | 100 | 2 | 0.886 | 100 |
| Preprepared salads and sandwiches | 85 | 94 | 356 | 528 | 600 | 511 | 85 | 82 | 0.5 | 39 | 95 | 360 | 520 | 600 | 530 | 97 | 100 | 0.4 | 0.400 | 96 |
| Cheese and imitates | 523 | 98 | 300 | 560 | 760 | 434 | 79 | 62 | 6.6 | 475 | 96 | 320 | 560 | 800 | 374 | 83 | 56 | 5.6 | 0.176 | 116 |
| - Cheese | 302 | 98 | 400 | 600 | 760 | 597 | 81 | 82 | 4.7 | 266 | 97 | 400 | 600 | 760 | 568 | 88 | 79 | 3.4 | 0.236 | 105 |
| - Spreads and processed cheese | 135 | 98 | 320 | 440 | 890 | 570 | 94 | 97 | 1.5 | 155 | 96 | 350 | 480 | 90 | 554 | 93 | 98 | 1.8 | 0.905 | 103 |
| - Cheese imitates a | 33 | 100 | 680 | 720 | 920 | 915 | 97 | 100 | 0.1 | NA | NA | |||||||||
| Butter and margarine | 91 | 95 | 4 | 40 | 200 | 65 | 14 | 1 | 0.4 | 92 | 91 | 4.2 | 42 | 200 | 77 | 8 | 1 | 0.6 | 0.885 | 84 |
| - Canned vegetables | 497 | 100 | 200 | 372 | 608 | 371 | 93 | 96 | 7.1 | 515 | 93 | 244 | 400 | 780 | 405 | 95 | 96 | 9.7 | 0.099 | 92 |
| Processed meat and derivatives | 732 | 92 | 640 | 800 | 1320 | 797 | 95 | 94 | 16.8 | 703 | 91 | 580 | 748 | 1000 | 780 | 94 | 96 | 21.4 | 0.005 ** | 102 |
| Meat alternatives | 122 | 98 | 176 | 544 | 760 | 324 | 76 | 53 | 0.1 | 90 | 93 | 60 | 352 | 700 | 353 | 69 | 51 | 0.1 | 0.089 | 92 |
| Crisps and snacks | 432 | 100 | 520 | 720 | 960 | 805 | 78 | 87 | 4.8 | 340 | 98 | 600 | 768 | 988 | 811 | 86 | 83 | 5.7 | 0.035 * | 99 |
| Sauces | 686 | 98 | 440 | 680 | 1200 | 768 | 92 | 94 | 4.9 | 581 | 91 | 440 | 720 | 1280 | 844 | 94 | 99 | 6.4 | 0.486 | 91 |
| - Pasta sauces | 131 | 100 | 400 | 532 | 800 | 541 | 98 | 100 | 0.8 | 149 | 89 | 400 | 520 | 920 | 740 | 94 | 100 | 1 | 0.807 | 73 |
| Mayonnaise/dressings | 76 | 99 | 400 | 560 | 600 | 467 | 40 | 7 | 0.9 | 70 | 100 | 440 | 560 | 640 | 466 | 40 | 12 | 1.3 | 0.874 | 100 |
| Spreads | 265 | 97 | 40 | 200 | 480 | 142 | 43 | 19 | 0.4 | 174 | 90 | 48 | 332 | 560 | 143 | 47 | 15 | 0.5 | 0.469 | 99 |
| - Vegetable spreads | 104 | 96 | 400 | 472 | 520 | 467 | 86 | 99 | 0.2 | 60 | 93 | 480 | 560 | 600 | 540 | 95 | 99 | 0.3 | 0.001 ** | 86 |
| Waters | 95 | 88 | 0.28 | 0.76 | 5.1 | 58 | NA | NA | 5.7 | 99 | 88 | 0.24 | 0.76 | 4.8 | 36 | NA | NA | 6.7 | 0.946 | 160 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krušič, S.; Hristov, H.; Hribar, M.; Lavriša, Ž.; Žmitek, K.; Pravst, I. Changes in the Sodium Content in Branded Foods in the Slovenian Food Supply (2011–2020). Nutrients 2023, 15, 4304. https://doi.org/10.3390/nu15194304
Krušič S, Hristov H, Hribar M, Lavriša Ž, Žmitek K, Pravst I. Changes in the Sodium Content in Branded Foods in the Slovenian Food Supply (2011–2020). Nutrients. 2023; 15(19):4304. https://doi.org/10.3390/nu15194304
Chicago/Turabian StyleKrušič, Sanja, Hristo Hristov, Maša Hribar, Živa Lavriša, Katja Žmitek, and Igor Pravst. 2023. "Changes in the Sodium Content in Branded Foods in the Slovenian Food Supply (2011–2020)" Nutrients 15, no. 19: 4304. https://doi.org/10.3390/nu15194304
APA StyleKrušič, S., Hristov, H., Hribar, M., Lavriša, Ž., Žmitek, K., & Pravst, I. (2023). Changes in the Sodium Content in Branded Foods in the Slovenian Food Supply (2011–2020). Nutrients, 15(19), 4304. https://doi.org/10.3390/nu15194304