
Dietary Interventions in Ulcerative Colitis: A Systematic Review of the Evidence with Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
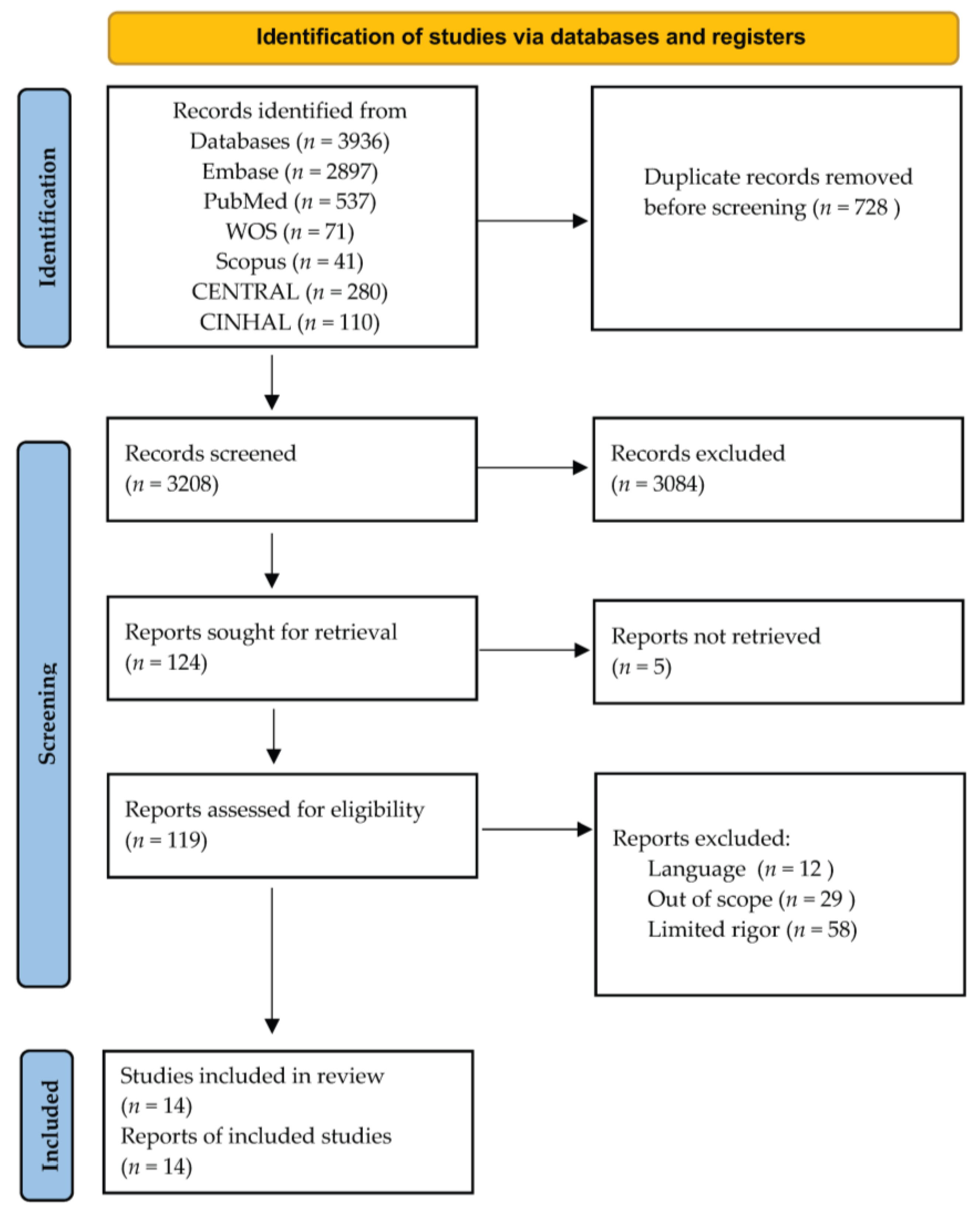
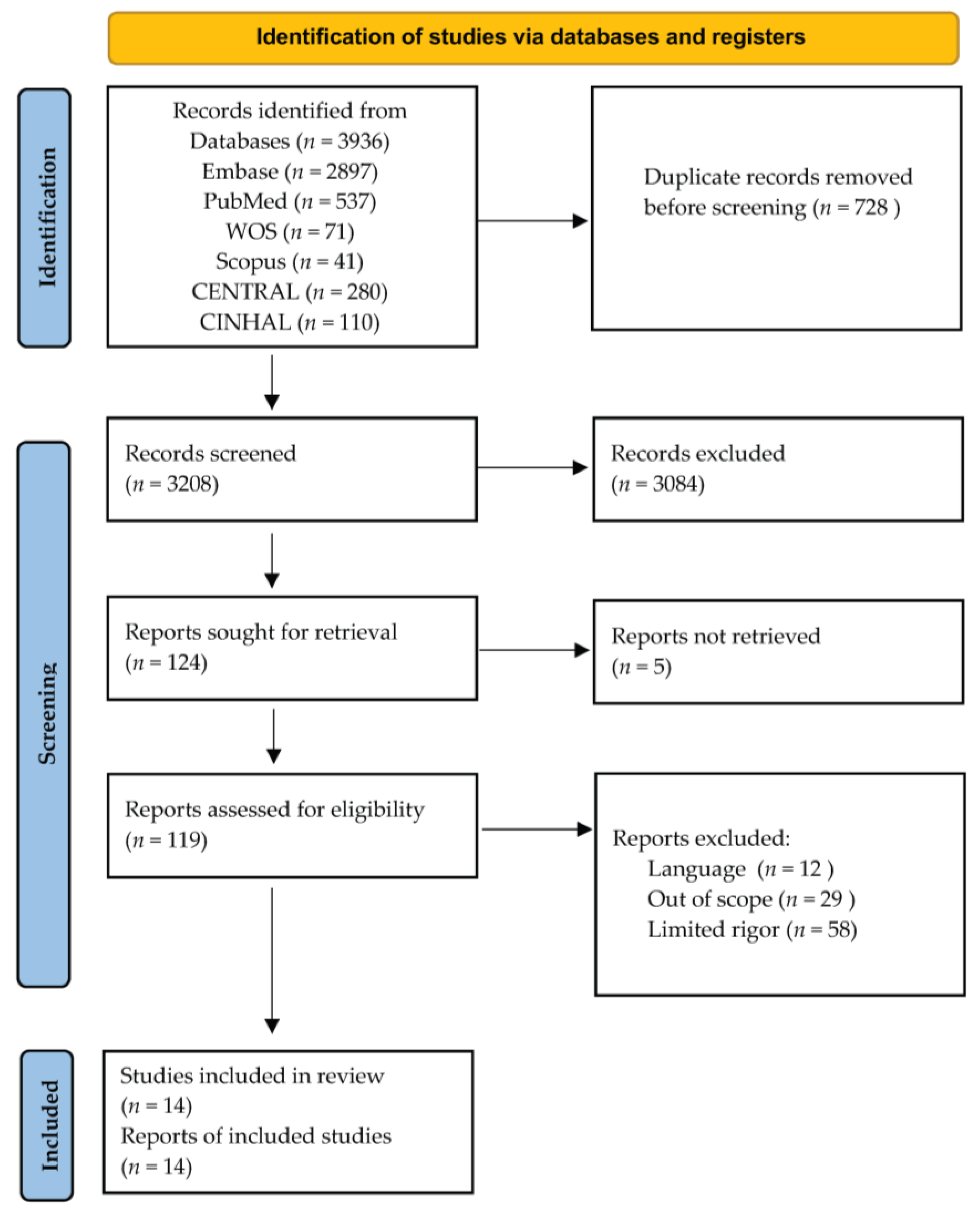
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Assessment of Risk of Bias and GRADE
2.4. Statistical Analysis
3. Results
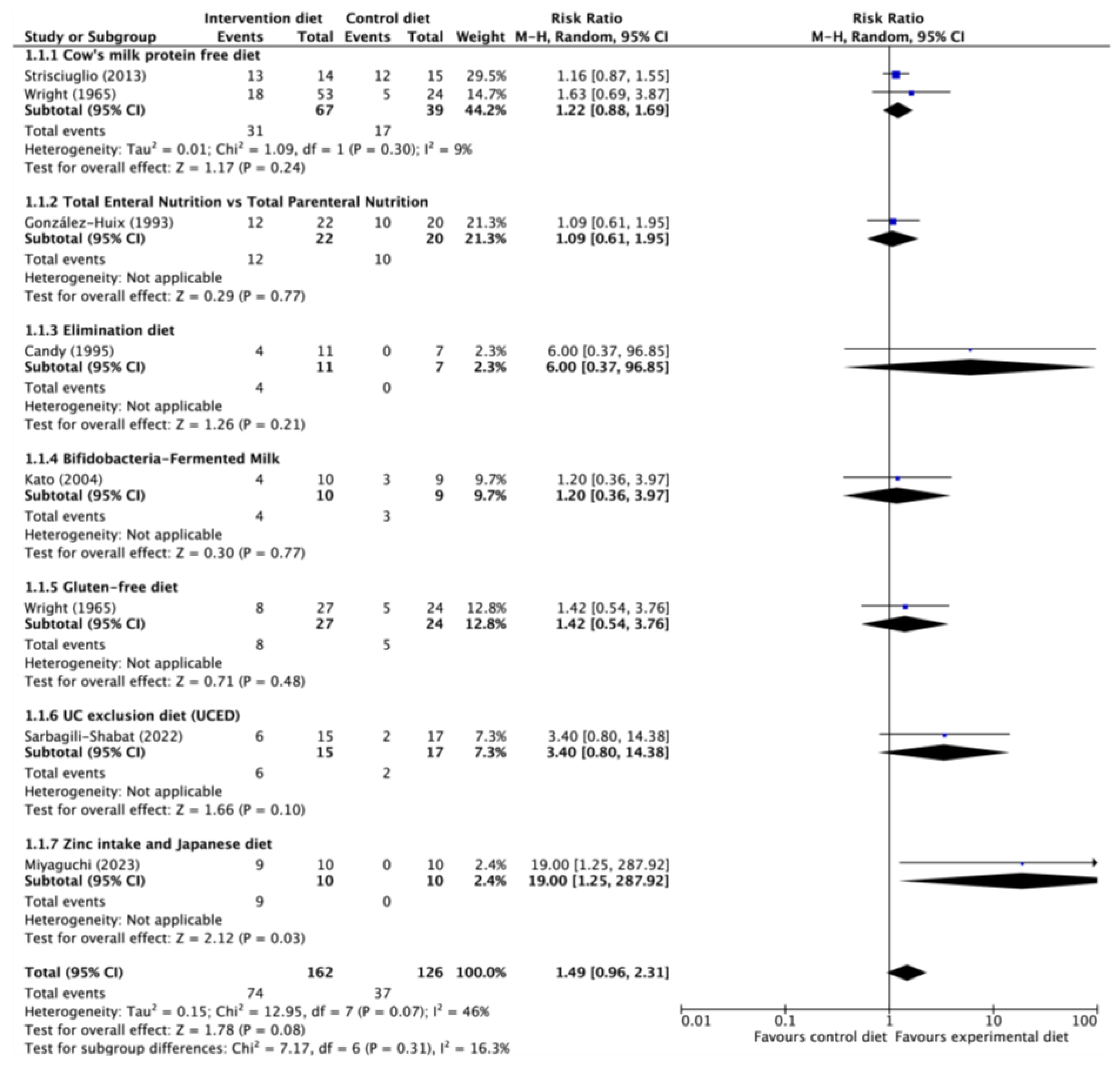
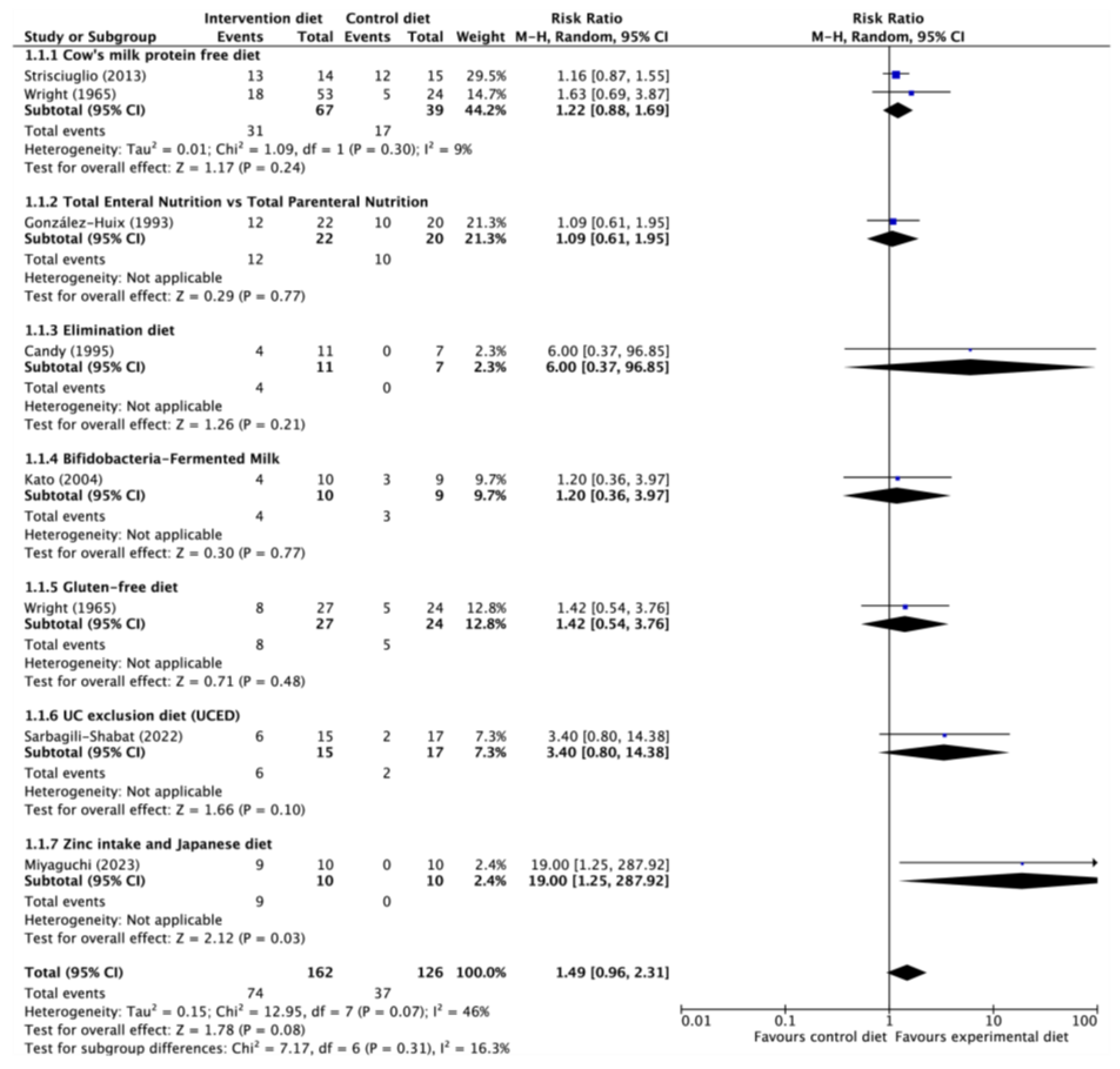
3.1. Induction of Remission in Ulcerative Colitis
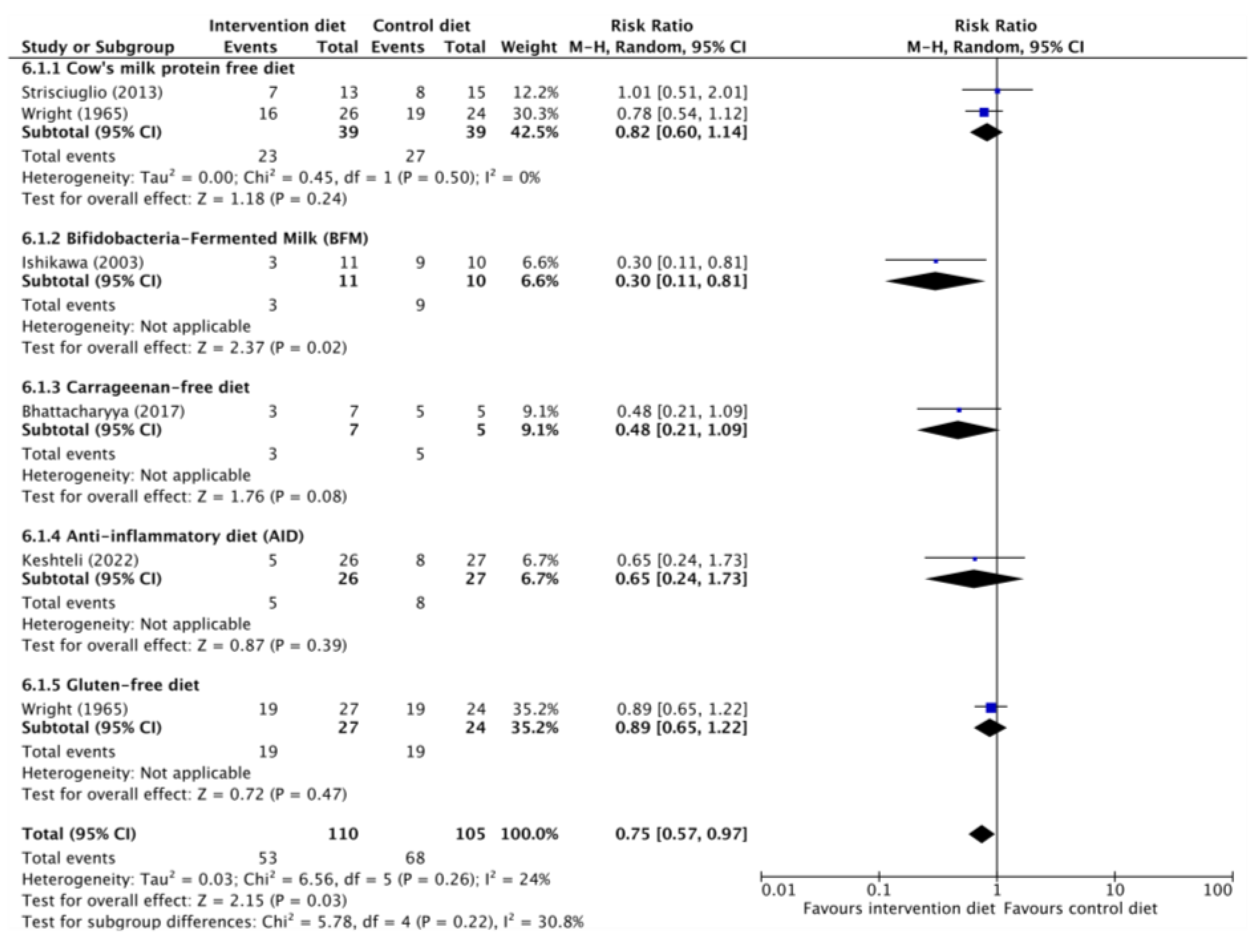
3.2. Maintenance of Remission in Ulcerative Colitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, A.; Rhodes, J.M.; Lindsay, J.O.; Abreu, M.T.; Kamm, M.A.; Gibson, P.R.; Gasche, C.; Silverberg, M.S.; Mahadevan, U.; Boneh, R.S.; et al. Dietary Guidance from the International Organization for the Study of Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; Jess, T. Implications of the Changing Epidemiology of Inflammatory Bowel Disease in a Changing World. United Eur. Gastroenterol. J. 2022, 10, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, C.; Cavalieri, D.; Di Paola, M.; Ramazzotti, M.; Poullet, J.B.; Massart, S.; Collini, S.; Pieraccini, G.; Lionetti, P. Impact of Diet in Shaping Gut Microbiota Revealed by a Comparative Study in Children from Europe and Rural Africa. Proc. Natl. Acad. Sci. USA 2010, 107, 14691–14696. [Google Scholar] [CrossRef] [PubMed]
- Agus, A.; Denizot, J.; Thévenot, J.; Martinez-Medina, M.; Massier, S.; Sauvanet, P.; Bernalier-Donadille, A.; Denis, S.; Hofman, P.; Bonnet, R.; et al. Western Diet Induces a Shift in Microbiota Composition Enhancing Susceptibility to Adherent-Invasive E. Coli Infection and Intestinal Inflammation. Sci. Rep. 2016, 6, 19032. [Google Scholar] [CrossRef]
- Sun, M.; Wu, W.; Liu, Z.; Cong, Y. Microbiota Metabolite Short Chain Fatty Acids, GPCR, and Inflammatory Bowel Diseases. J. Gastroenterol. 2017, 52, 1–8. [Google Scholar] [CrossRef]
- Ji, Y.; Yang, Y.; Sun, S.; Dai, Z.; Ren, F.; Wu, Z. Insights into Diet-Associated Oxidative Pathomechanisms in Inflammatory Bowel Disease and Protective Effects of Functional Amino Acids. Nutr. Rev. 2022, 81, 95–113. [Google Scholar] [CrossRef]
- Werner, T.; Wagner, S.J.; Martinez, I.; Walter, J.; Chang, J.-S.; Clavel, T.; Kisling, S.; Schuemann, K.; Haller, D. Depletion of Luminal Iron Alters the Gut Microbiota and Prevents Crohn’s Disease-like Ileitis. Gut 2011, 60, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Roy, B.; Khan, S.; Septer, S.; Umar, S. Microbiome, Metabolome and Inflammatory Bowel Disease. Microorganisms 2016, 4, 20. [Google Scholar] [CrossRef]
- Reich, K.M. Vitamin D Improves Inflammatory Bowel Disease Outcomes: Basic Science and Clinical Review. World J. Gastroenterol. 2014, 20, 4934. [Google Scholar] [CrossRef]
- John, S.; Luben, R.; Shrestha, S.S.; Welch, A.; Khaw, K.-T.; Hart, A.R. Dietary N-3 Polyunsaturated Fatty Acids and the Aetiology of Ulcerative Colitis: A UK Prospective Cohort Study. Eur. J. Gastroenterol. Hepatol. 2010, 22, 602–606. [Google Scholar] [CrossRef]
- Jowett, S.L. Influence of Dietary Factors on the Clinical Course of Ulcerative Colitis: A Prospective Cohort Study. Gut 2004, 53, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, X.; Wang, W.; Zhang, D. Consumption of Vegetables and Fruit and the Risk of Inflammatory Bowel Disease: A Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2015, 27, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Abraham, B.; El-Serag, H. Dietary Intake and Risk of Developing Inflammatory Bowel Disease: A Systematic Review of the Literature. Am. J. Gastroenterol. 2011, 106, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Haskey, N.; Gibson, D.L. An Examination of Diet for the Maintenance of Remission in Inflammatory Bowel Disease. Nutrients 2017, 9, 259. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; Chan, S.S.M.; Lochhead, P.; Ananthakrishnan, A.N.; Hart, A.R.; Chan, A.T. The Role of Diet in the Aetiopathogenesis of Inflammatory Bowel Disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 525–535. [Google Scholar] [CrossRef]
- Sugihara, K.; Morhardt, T.L.; Kamada, N. The Role of Dietary Nutrients in Inflammatory Bowel Disease. Front. Immunol. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Sicilia, B.; García-López, S.; González-Lama, Y.; Zabana, Y.; Hinojosa, J.; Gomollón, F. Guía GETECCU 2020 para el tratamiento de la colitis ulcerosa. Elaborada con metodología GRADE. Gastroenterol. Hepatol. 2020, 43, 1–57. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.; Petticrew, M.; Tugwell, P.; Moher, D.; O’Neill, J.; Waters, E.; White, H.; the PRISMA-Equity Bellagio Group. PRISMA-Equity 2012 Extension: Reporting Guidelines for Systematic Reviews with a Focus on Health Equity. PLoS Med. 2012, 9, e1001333. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Shumard, T.; Xie, H.; Dodda, A.; Varady, K.A.; Feferman, L.; Halline, A.G.; Goldstein, J.L.; Hanauer, S.B.; Tobacman, J.K. A Randomized Trial of the Effects of the No-Carrageenan Diet on Ulcerative Colitis Disease Activity. Nutr. Healthy Aging 2017, 4, 181–192. [Google Scholar] [CrossRef]
- Bodini, G.; Zanella, C.; Crespi, M.; Lo Pumo, S.; Demarzo, M.G.; Savarino, E.; Savarino, V.; Giannini, E.G. A Randomized, 6-Wk Trial of a Low FODMAP Diet in Patients with Inflammatory Bowel Disease. Nutrion 2019, 67–68, 110542. [Google Scholar] [CrossRef] [PubMed]
- Candy, S.; Borok, G.; Wright, J.P.; Boniface, V.; Goodman, R. The Value of an Elimination Diet in the Management of Patients with Ulcerative Colitis. S. Afr. Med. J. 1995, 85, 1176–1179. [Google Scholar] [PubMed]
- Fritsch, J.; Garces, L.; Quintero, M.A.; Pignac-Kobinger, J.; Santander, A.M.; Fernández, I.; Ban, Y.J.; Kwon, D.; Phillips, M.C.; Knight, K.; et al. Low-Fat, High-Fiber Diet Reduces Markers of Inflammation and Dysbiosis and Improves Quality of Life in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2021, 19, 1189–1199.e30. [Google Scholar] [CrossRef]
- González-Huix, F.; Fernández-Bañares, F.; Esteve-Comas, M.; Abad-Lacruz, A.; Cabré, E.; Acero, D.; Figa, M.; Guilera, M.; Humbert, P.; de León, R. Enteral versus Parenteral Nutrition as Adjunct Therapy in Acute Ulcerative Colitis. Am. J. Gastroenterol. 1993, 88, 227–232. [Google Scholar]
- Ishikawa, H.; Akedo, I.; Umesaki, Y.; Tanaka, R.; Imaoka, A.; Otani, T. Randomized Controlled Trial of the Effect of Bifidobacteria-Fermented Milk on Ulcerative Colitis. J. Am. Coll. Nutr. 2003, 22, 56–63. [Google Scholar] [CrossRef]
- Kato, K.; Mizuno, S.; Umesaki, Y.; Ishii, Y.; Sugitani, M.; Imaoka, A.; Otsuka, M.; Hasunuma, O.; Kurihara, R.; Iwasaki, A.; et al. Randomized Placebo-Controlled Trial Assessing the Effect of Bifidobacteria-Fermented Milk on Active Ulcerative Colitis. Aliment. Pharmacol. Ther. 2004, 20, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Keshteli, A.H.; Valcheva, R.; Nickurak, C.; Park, H.; Mandal, R.; Van Diepen, K.; Kroeker, K.I.; Van Zanten, S.V.; Halloran, B.; Wishart, D.S.; et al. Anti-Inflammatory Diet Prevents Subclinical Colonic Inflammation and Alters Metabolomic Profile of Ulcerative Colitis Patients in Clinical Remission. Nutrients 2022, 14, 3294. [Google Scholar] [CrossRef]
- Kyaw, M.H.; Moshkovska, T.; Mayberry, J. A Prospective, Randomized, Controlled, Exploratory Study of Comprehensive Dietary Advice in Ulcerative Colitis: Impact on Disease Activity and Quality of Life. Eur. J. Gastroenterol. Hepatol. 2014, 26, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Miyaguchi, K.; Tsuzuki, Y.; Ichikawa, Y.; Shiomi, R.; Ohgo, H.; Nakamoto, H.; Imaeda, H. Positive Zinc Intake and a Japanese Diet Rich in N-3 Fatty Acids Induces Clinical Remission in Patients with Mild Active Ulcerative Colitis: A Randomized Interventional Pilot Study. J. Clin. Biochem. Nutr. 2023, 72, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Sarbagili Shabat, C.; Scaldaferri, F.; Zittan, E.; Hirsch, A.; Mentella, M.C.; Musca, T.; Cohen, N.A.; Ron, Y.; Fliss Isakov, N.; Pfeffer, J.; et al. Use of Faecal Transplantation with a Novel Diet for Mild to Moderate Active Ulcerative Colitis: The CRAFT UC Randomised Controlled Trial. J. Crohns Colitis 2022, 16, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Strisciuglio, C.; Giannetti, E.; Martinelli, M.; Sciorio, E.; Staiano, A.; Miele, E. Does Cow’s Milk Protein Elimination Diet Have a Role on Induction and Maintenance of Remission in Children with Ulcerative Colitis? Acta Paediatr. Int. J. Paediatr. 2013, 102, e273–e278. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.; Truelove, S.C. A Controlled Therapeutic Trial of Various Diets in Ulcerative Colitis. BMJ 1965, 2, 138–141. [Google Scholar] [CrossRef]
- Wright, R.; Truelove, S.R. Serial Rectal Biopsy in Ulcerative Colitis during the Course of a Controlled Therapeutic Trial of Various Diets. Am. J. Dig. Dis. 1966, 11, 847–857. [Google Scholar] [CrossRef]
- Herrador-López, M.; Martín-Masot, R.; Navas-López, V.M. EEN Yesterday and Today … CDED Today and Tomorrow. Nutrients 2020, 12, 3793. [Google Scholar] [CrossRef]
- McMaster University and Evidence Prime GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. 2022. Available online: https://www.gradepro.org/ (accessed on 15 May 2023).
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target Strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Martín-Masot, R.; Herrador-López, M.; Navas-López, V.M. Dietary Habit Modifications in Paediatric Patients after One Year of Treatment with the Crohn’s Disease Exclusion Diet. Nutrients 2023, 15, 554. [Google Scholar] [CrossRef]
- Sarbagili-Shabat, C.; Albenberg, L.; Van Limbergen, J.; Pressman, N.; Otley, A.; Yaakov, M.; Wine, E.; Weiner, D.; Levine, A. A Novel UC Exclusion Diet and Antibiotics for Treatment of Mild to Moderate Pediatric Ulcerative Colitis: A Prospective Open-Label Pilot Study. Nutrients 2021, 13, 3736. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| First Author (Year Publication) [Ref.] | Study Population | Intervention | Duration | Variables | Outcomes | Conclusions |
|---|---|---|---|---|---|---|
| Wright (1965) [35] | 77 active UC adult patients (26 milk-free diet, 24 dummy diet and 27 gluten free diet). GFD was not milk-free diet. | Milk free, low-roughage diet vs. dummy diet or gluten-free and milk-free diet (1) | 12 months | Clinical course (number of relapses during the trial period). Clinical remission | Milk free diet vs. dummy diet Clinical remission: 18/53 (33.9%) vs. (20.8%). [RR = 1.63 (CI 95% 0.69–3.87)] No relapses: 10/26 (38.4%) vs. 5/24 (20.8%). [RR = 1.84 (IC 95% 0.73–4.62)] Gluten free diet vs. dummy diet Clinical remission: 8/27 (29.6%) vs. 5/24 (20.8%). RR = 1.42 (CI 95% 0.54–3.76)] No relapses: 8/27 (29.6%) vs. 5/24 (20.8%). [RR = 1.42 (IC 95% 0.54–3.76)] | The milk-free diet and the gluten-free diet were superior to dummy diet to avoid relapses in patients with UC |
| Wright (1966) [36] | 77 active UC adult patients (26 milk-free diet, 24 dummy diet and 27 gluten free-diet). GFD was not milk-free diet. | Milk free diet vs. Milk Milk free, low-roughage diet vs. dummy diet or gluten-free and milk-free diet (1) | 12 months | Sigmoidoscopic remission, histologic remission | Milk free diet vs. dummy diet
| The milk-free and gluten-free diet were superior to dummy diet in inducing endoscopic and histologic remission |
| González-Huix (1993) [27] | 42 active UC adult patients (22 steroids and TEN vs. 20 steroids and TPN) | TEN vs. TPN | Until remission or colectomy | Clinical remission (Truelove’s index) | Remission rates: 54.5% vs. 50.0%. p = 0.764. [RR = 1.09 (IC 95% 0.61–1.95)] More complications after colectomy and related with artificial nutritional support in TPN group | TEN is safe and effective in patients with severe UC. Compared with TPN, is cheaper and is associated with a lower complication rate. |
| Candy (1995) [25] | 18 active UC adult patients (11 intervention and 7 in control group). | Elimination diet (2) | 6 weeks | Remission and improvement rates. Sigmoidoscopy and biopsy findings. |
| Patients with mild to moderate UC may be brought into remission by the manipulation of dietary intake. |
| Ishikawa (2003) [28] | 21 UC adult patients in remission BFM GROUP: 11 CONTROL: 10 | Bifidobacterium-Fermented Milk (BFM, 100 mL per day) + conventional treatment vs. conventional treatment | 12 months | Relapse during the follow-up | Exacerbations of symptoms was seen in 27.3% of subjects in the BFM vs. 90% of control group. Cumulative exacerbation rates were higher in the control group RR: 3.3 (CI 95%, 1.23–8.85), p = 0.0075. Log rank = 0.0184 | Supplementation with the BFM product was successful in maintaining remission and had possible preventive effects on the relapse of ulcerative colitis. |
| Kato (2004) [29] | 20 active UC adult patients: BFM GROUP: 10 CONTROL: 10 | Bifidobacterium-Fermented Milk (BFM, 100 mL per day) + conventional treatment vs. conventional treatment | 12 weeks | Clinical response Clinical remission Endoscopic outcomes Histologic outcomes |
| Supplementation with this bifidobacteria-fermented milk product is safe and more effective than conventional treatment alone, suggesting possible beneficial effects in managing active ulcerative colitis. |
| Strisciuglio (2013) [34] | 29 pediatric patients newly diagnosis of UC. 14 received CMP elimination diet and 15 free diet. | Cow’s milk protein-free diet vs. usual diet plus conventional treatment: If PUCAI < 35: 5-ASA treatment If PUCAI ≥ 35: steroids and 5-ASA | 12 months | Clinical remission (PUCAI) |
| The elimination of cow’s milk proteins from the diet has no relevant role in the induction and maintenance of remission of UC in children. |
| Kyaw (2014) [31] | 112 active UC adult patients | Specific dietary Guidelines for UC (61 patients) vs. usual diet (51 patients) | 4–6 weeks | Disease activity (SCCAI), HR-QOL (IBDQ) | Significant reduction in SCCAI in the intervention group (p = 0.0108) compared to control. No significant changes in quality of life | Probable association between specific dietary advice for UC and symptom improvement |
| Bhattacharyya (2017) [23] | 12 adult UC patients in clinical remission | Carrageenan-free diet vs. Carrageenan-free diet with capsules containing 200 mg food-grade carrageenan | 12 months | Clinical relapse (SCCAI), calprotectin, SIBDQ | Fewer relapses in the placebo group (0% vs. 60%, p = 0.046). Increased levels of IL-6 (p = 0.02) and faecal calprotectin (p = 0.06) in the carrageenan group. No differences in quality of life. | Carrageenan intake contributed to higher relapse frequency in UC patients in remission |
| Bodini (2019) [24] | 20 adult UC patients (clinical remission or mild disease) | Low FODMAPsdiet | 6 weeks | Clinical remission (PMS), calprotectin, HRQOL(IBD-Q) | At baseline 14 (70%) patients were in remission and 6 (30%) had mild disease. After 6 weeks 17 (85%) were in clinical remission and 3 (15%) had mild disease. No significant differences in PMS from baseline to 6 weeks in both groups. After the 6-wk dietary intervention, a statistically significant decrease in median calprotectin values in the LFD group was observed (p = 0.004). After the 6-wk dietary intervention, a modest but statistically significant increase in median IBD-Q in the LFD group was observed. | A short-term low FODMAP diet (LFD) is safe for UC patients and is linked to improved fecal inflammatory markers and quality of life, even in those with mainly quiescent disease. It can also induce clinical remission in patients with mild disease. |
| Fritsch (2021) [26] | 18 adult patients with inactive or mild UC | Low fiber, high-fiber diet (LFD) vs. An improved standard American Diet (iSAD) | 10 weeks 2 weeks of washout between 2 periods of 4 weeks | Clinical remission (PMS), CRP, calprotectin, HR-QOL (SIBDQ) | Significant improvement in quality of life according to SIBDQ in the LFD diet (p = 0.02) and iSAD (p = 0.001). Significant improvement in SF-36 with both diets. Decrease in CRP (p = 0.07) and serum amyloid A protein (p = 0.02) in LFD. After LFD, the relative abundance of Actinobacteria decreased (p = 0.017), while that of Bacteroidetes increased (p = 0.015). | Both diets are well tolerated with improvements in quality of life. The low-fat, high-fibre diet decreased markers of inflammation, gut dysbiosis and PMS. |
| Keshteli (2022) [30] | 53 adults with UC in CR (PMS ≤ 2 points with a rectal bleeding subscore ≤ 1) in the previous 18 months | Anti-inflammatory diet (AID) n = 26 vs. Canada’s Food Guide (CFG) n = 27 | 6 months | Clinical relapse (PMS), Subclinical response (Fcal < 150 μg/g) HR-QOL (SIBDQ) |
| The AID was effective in preventing subclinical inflammation. |
| Sarbagili-Shabat (2022) [33] | Adults with active and refractory established UC. Arm 1 (n = 17) Arm 2 (n = 19) Arm 3 (n = 15) | Arm 1: free diet and standard FT without dietary conditioning of the donor. Arm 2: FT with dietary pre-conditioning of the donor for 14 days and UCED Arm 3: UCED without FT | 12 weeks | Clinical remission (SCCAI), Clinical improvement, endoscopic remission. |
| UCED alone appeared to achieve higher clinical remission and mucosal healing than single donor FT with or without diet. |
| Miyaguchi (2023) [32] | Teenagers and adults with mild UC | Unrestricted diet (UD) vs. promotion of zinc intake and Japanese diet (JD) | 24 weeks | Clinical (CAI), Endoscopic (UCEIS) and histological (GHS) remissions |
| Promotion of zinc intake and a Japanese diet rich in n-3 fatty acids may induce clinical remission in patients with mild active UC |
| Certainty Assessment | № of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design [Ref.] | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Intervention Diet | Control Diet | Relative (95% CI) | Absolute (95% CI) | ||
| DIET: Elimination diet | ||||||||||||
| 1 | RCT [19] | serious a | not serious | not serious | very serious b | none | 7/11 (63.6%) | 0/7 (0.0%) | RR 1.66 (0.85 to 3.23) | 0 fewer per 1000 (from 0 fewer to 0 fewer) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Cow’s milk protein free diet | ||||||||||||
| 2 | RCT [28,29] | serious a | not serious | not serious | very serious b | none | 31/67 (46.3%) | 0.0% | RR 1.16 (0.87 to 1.55) | 0 fewer per 1000 (from 0 fewer to 0 fewer) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Gluten-free diet | ||||||||||||
| 1 | RCT [29] | serious a | not serious | not serious | very serious b | none | 8/27 (29.6%) | 5/24 (20.8%) | RR 1.09 (0.61 to 1.95) | 19 more per 1000 (from 81 fewer to 198 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Total Enteral Nutrition vs. Total Parenteral Nutrition | ||||||||||||
| 1 | RCT [21] | very serious c | serious d | not serious | very serious b | none | 12/22 (54.5%) | 10/20 (50.0%) | RR 6.00 (0.37 to 96.85) | 1000 more per 1000 (from 315 fewer to 1000 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Bifidobacteria-Fermented Milk | ||||||||||||
| 1 | RCT [23] | very serious c | not serious | not serious | very serious d | none | 4/10 (40.0%) | 3/9 (33.3%) | RR 1.20 (0.36 to 3.97) | 67 more per 1000 (from 213 fewer to 990 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: UC exclusion diet (UCED) | ||||||||||||
| 1 | RCT [27] | not serious | not serious | not serious | serious e | none | 6/15 (40.0%) | 2/17 (11.8%) | RR 3.40 (0.80 to 14.38) | 282 more per 1000 (from 24 fewer to 1000 more) | ⨁⨁⨁◯ Moderate | IMPORTANT |
| DIET: Zinc intake and Japanese diet vs. unrestricted diet | ||||||||||||
| 1 | RCT [26] | not serious | not serious | not serious | serious e | none | 9/10 (90.0%) | 0/10 (0.0%) | RR 19.00 (1.25 to 287.92) | 0 fewer per 1000 (from 0 fewer to 0 fewer) | ⨁⨁⨁◯ Moderate | IMPORTANT |
| DIET: Low fat, low carbohydrate, low fiber, high protein and probiotics (DMF) | ||||||||||||
| 1 | RCT [32] | not serious | serious d | not serious | very serious b | none | 61 | 51 | - | mean 1.304 points from baseline more (0.21 more to 2.398 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Low FODMAPs | ||||||||||||
| 1 | RCT [18] | not serious | serious d | not serious | very serious b | none | PMS decreased after the 6-wk dietary intervention, although not significantly, in the Low FODMAPs Diet group (n = 8 patients vs. 12 patients in the control group). | ⨁◯◯◯ Very low | IMPORTANT | |||
| DIET: Low fat, high fiber | ||||||||||||
| 1 | RCT [33] | not serious | serious d | not serious | very serious b | none | PMS decreased after the 4-wk dietary intervention although not significantly, in the low fat and high fiber diet group (n = 18 patients) | ⨁◯◯◯ Very low | IMPORTANT | |||
| Certainty Assessment | № of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Clinical Relapse in Ulcerative Colitis | Placebo | Relative (95% CI) | Absolute (95% CI) | ||
| DIET: Cow’s milk protein free diet | ||||||||||||
| 2 | RCT [28,29] | serious a | not serious | not serious | very serious b | none | 23/39 (59.0%) | 27/39 (69.2%) | RR 0.82 (0.60 to 1.14) | 125 fewer per 1000 (from 277 fewer to 97 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Bifidobacteria-Fermented Milk (BFM) | ||||||||||||
| 1 | RCT [22] | very serious c | not serious | not serious | very serious b | none | 3/11 (27.3%) | 9/10 (90.0%) | RR 0.30 (0.11 to 0.81) | 630 fewer per 1000 (from 801 fewer to 171 fewer) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Carrageenan-free diet | ||||||||||||
| 1 | RCT [17] | very serious c | very serious b | not serious | serious d | none | 3/7 (42.9%) | 5/5 (100.0%) | RR 0.48 (0.21 to 1.09) | 520 fewer per 1000 (from 790 fewer to 90 more) | ⨁◯◯◯ Very low | IMPORTANT |
| DIET: Anti-inflammatory diet (AID) | ||||||||||||
| 1 | RCT [24] | serious a | not serious | not serious | serious d | none | 5/26 (19.2%) | 8/27 (29.6%) | RR 0.65 (0.24 to 1.73) | 104 fewer per 1000 (from 225 fewer to 216 more) | ⨁⨁◯◯ Low | IMPORTANT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrador-López, M.; Martín-Masot, R.; Navas-López, V.M. Dietary Interventions in Ulcerative Colitis: A Systematic Review of the Evidence with Meta-Analysis. Nutrients 2023, 15, 4194. https://doi.org/10.3390/nu15194194
Herrador-López M, Martín-Masot R, Navas-López VM. Dietary Interventions in Ulcerative Colitis: A Systematic Review of the Evidence with Meta-Analysis. Nutrients. 2023; 15(19):4194. https://doi.org/10.3390/nu15194194
Chicago/Turabian StyleHerrador-López, Marta, Rafael Martín-Masot, and Víctor Manuel Navas-López. 2023. "Dietary Interventions in Ulcerative Colitis: A Systematic Review of the Evidence with Meta-Analysis" Nutrients 15, no. 19: 4194. https://doi.org/10.3390/nu15194194
APA StyleHerrador-López, M., Martín-Masot, R., & Navas-López, V. M. (2023). Dietary Interventions in Ulcerative Colitis: A Systematic Review of the Evidence with Meta-Analysis. Nutrients, 15(19), 4194. https://doi.org/10.3390/nu15194194