
Effects of Intrauterine Growth Restriction (IUGR) on Growth and Body Composition Compared to Constitutionally Small Infants

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
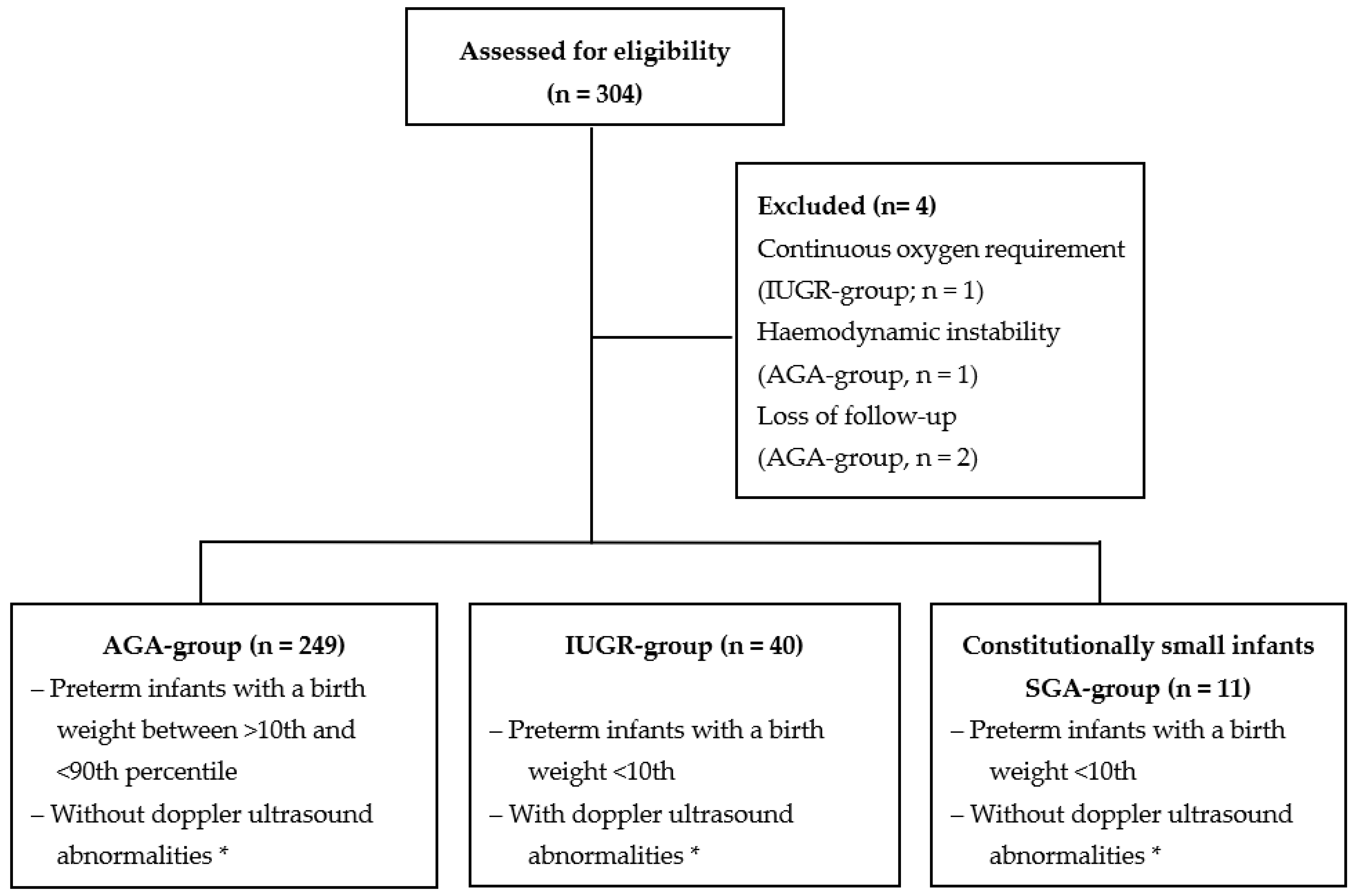
2.2. Patient Groups
2.3. Growth and Body Composition
2.4. Neonatal Morbidities
2.5. Nutritional Management
2.6. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garite, T.J.; Clark, R.; Thorp, J.A. Intrauterine growth restriction increases morbidity and mortality among premature neonates. Am. J. Obstet. Gynecol. 2004, 191, 481–487. [Google Scholar] [CrossRef]
- Sacchi, C.; Marino, C.; Nosarti, C.; Vieno, A.; Visentin, S.; Simonelli, A. Association of Intrauterine Growth Restriction and Small for Gestational Age Status with Childhood Cognitive Outcomes: A Systematic Review and Meta-analysis. JAMA Pediatr. 2020, 174, 772–781. [Google Scholar] [CrossRef]
- Clark, R.H.; Thomas, P.; Peabody, J. Extrauterine growth restriction remains a serious problem in prematurely born neonates. Pediatrics 2003, 111, 986–990. [Google Scholar] [CrossRef]
- Sacchi, C.; O’Muircheartaigh, J.; Batalle, D.; Counsell, S.J.; Simonelli, A.; Cesano, M.; Falconer, S.; Chew, A.; Kennea, N.; Nongena, P.; et al. Neurodevelopmental Outcomes following Intrauterine Growth Restriction and Very Preterm Birth. J. Pediatr. 2021, 238, 135–144.e10. [Google Scholar] [CrossRef]
- Hay, W.W., Jr. Aggressive Nutrition of the Preterm Infant. Curr. Pediatr. Rep. 2013, 1, 229–239. [Google Scholar] [CrossRef]
- Gidi, N.W.; Goldenberg, R.L.; Nigussie, A.K.; McClure, E.; Mekasha, A.; Worku, B.; Siebeck, M.; Genzel-Boroviczeny, O.; Muhe, L.M. Incidence and associated factors of extrauterine growth restriction (EUGR) in preterm infants, a cross-sectional study in selected NICUs in Ethiopia. BMJ Paediatr. Open 2020, 4, e000765. [Google Scholar] [CrossRef]
- Morgan, J.; Young, L.; McGuire, W. Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. 2014, 2014, CD001970. [Google Scholar] [CrossRef]
- Kumar, R.K.; Singhal, A.; Vaidya, U.; Banerjee, S.; Anwar, F.; Rao, S. Optimizing Nutrition in Preterm Low Birth Weight Infants-Consensus Summary. Front. Nutr. 2017, 4, 20. [Google Scholar] [CrossRef]
- Claas, M.J.; de Vries, L.S.; Koopman, C.; Uniken Venema, M.M.; Eijsermans, M.J.; Bruinse, H.W.; Verrijn Stuart, A.A. Postnatal growth of preterm born children </= 750 g at birth. Early Hum. Dev. 2011, 87, 495–507. [Google Scholar] [CrossRef]
- Hack, M.; Breslau, N.; Weissman, B.; Aram, D.; Klein, N.; Borawski, E. Effect of very low birth weight and subnormal head size on cognitive abilities at school age. N. Engl. J. Med. 1991, 325, 231–237. [Google Scholar] [CrossRef]
- Neubauer, V.; Griesmaier, E.; Pehbock-Walser, N.; Pupp-Peglow, U.; Kiechl-Kohlendorfer, U. Poor postnatal head growth in very preterm infants is associated with impaired neurodevelopment outcome. Acta Paediatr. 2013, 102, 883–888. [Google Scholar] [CrossRef]
- Gallagher, D.; Andres, A.; Fields, D.A.; Evans, W.J.; Kuczmarski, R.; Lowe, W.L., Jr.; Lumeng, J.C.; Oken, E.; Shepherd, J.A.; Sun, S.; et al. Body Composition Measurements from Birth through 5 Years: Challenges, Gaps, and Existing & Emerging Technologies—A National Institutes of Health workshop. Obes. Rev. 2020, 21, e13033. [Google Scholar]
- Andrews, E.T.; Beattie, R.M.; Johnson, M.J. Measuring body composition in the preterm infant: Evidence base and practicalities. Clin. Nutr. 2019, 38, 2521–2530. [Google Scholar] [CrossRef]
- Binder, C.; Buchmayer, J.; Thajer, A.; Giordano, V.; Schmidbauer, V.; Harreiter, K.; Klebermass-Schrehof, K.; Berger, A.; Goeral, K. Association between Fat-Free Mass and Brain Size in Extremely Preterm Infants. Nutrients 2021, 13, 4205. [Google Scholar] [CrossRef]
- Ramel, S.E.; Gray, H.L.; Christiansen, E.; Boys, C.; Georgieff, M.K.; Demerath, E.W. Greater Early Gains in Fat-Free Mass, but Not Fat Mass, Are Associated with Improved Neurodevelopment at 1 Year Corrected Age for Prematurity in Very Low Birth Weight Preterm Infants. J. Pediatr. 2016, 173, 108–115. [Google Scholar] [CrossRef]
- Georgieff, M.K.; Ramel, S.E.; Cusick, S.E. Nutritional influences on brain development. Acta Paediatr. 2018, 107, 1310–1321. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Lees, C.C.; Stampalija, T.; Baschat, A.; da Silva Costa, F.; Ferrazzi, E.; Figueras, F.; Hecher, K.; Kingdom, J.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef]
- Gumina, D.L.; Su, E.J. Mechanistic insights into the development of severe fetal growth restriction. Clin. Sci. 2023, 137, 679–695. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef]
- Su, E.J.; Xin, H.; Yin, P.; Dyson, M.; Coon, J.; Farrow, K.N.; Mestan, K.K.; Ernst, L.M. Impaired fetoplacental angiogenesis in growth-restricted fetuses with abnormal umbilical artery doppler velocimetry is mediated by aryl hydrocarbon receptor nuclear translocator (ARNT). J. Clin. Endocrinol. Metab. 2015, 100, E30–E40. [Google Scholar] [CrossRef][Green Version]
- Ji, S.; Xin, H.; Su, E.J. Overexpression of the aryl hydrocarbon receptor nuclear translocator partially rescues fetoplacental angiogenesis in severe fetal growth restriction. Clin. Sci. 2019, 133, 1353–1365. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- de Mendonca, E.; de Lima Macena, M.; Bueno, N.B.; de Oliveira, A.C.M.; Mello, C.S. Premature birth, low birth weight, small for gestational age and chronic non-communicable diseases in adult life: A systematic review with meta-analysis. Early Hum. Dev. 2020, 149, 105154. [Google Scholar] [CrossRef]
- Bruno, C.J.; Bengani, S.; Gomes, W.A.; Brewer, M.; Vega, M.; Xie, X.; Kim, M.; Fuloria, M. MRI Differences Associated with Intrauterine Growth Restriction in Preterm Infants. Neonatology 2017, 111, 317–323. [Google Scholar] [CrossRef]
- Guellec, I.; Marret, S.; Baud, O.; Cambonie, G.; Lapillonne, A.; Roze, J.C.; Fresson, J.; Flamant, C.; Charkaluk, M.L.; Arnaud, C.; et al. Intrauterine Growth Restriction, Head Size at Birth, and Outcome in Very Preterm Infants. J. Pediatr. 2015, 167, 975–981.e2. [Google Scholar] [CrossRef]
- El Ayoubi, M.; Patkai, J.; Bordarier, C.; Desfrere, L.; Moriette, G.; Jarreau, P.H.; Zeitlin, J. Impact of fetal growth restriction on neurodevelopmental outcome at 2 years for extremely preterm infants: A single institution study. Dev. Med. Child. Neurol. 2016, 58, 1249–1256. [Google Scholar] [CrossRef]
- Mamelle, N.; Cochet, C.; Claris, O. Definition of fetal growth restriction according to constitutional growth potential. Biol. Neonate 2001, 80, 277–285. [Google Scholar] [CrossRef]
- Jayawardena, L.; Sheehan, P. Introduction of a customised growth chart protocol increased detection of small for gestational age pregnancies in a tertiary Melbourne hospital. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 493–500. [Google Scholar] [CrossRef]
- Gardosi, J. Customized charts and their role in identifying pregnancies at risk because of fetal growth restriction. J. Obstet. Gynaecol. Can. 2014, 36, 408–415. [Google Scholar] [CrossRef]
- Lan, S.; Fu, H.; Zhang, R.; Zhong, G.; Pan, L.; Bei, F.; Hong, L. Extrauterine growth restriction in preterm infants: Postnatal growth pattern and physical development outcomes at age 3–6 years. Front. Pediatr. 2022, 10, 945422. [Google Scholar] [CrossRef]
- Aggett, P.J.; Agostoni, C.; Axelsson, I.; De Curtis, M.; Goulet, O.; Hernell, O.; Koletzko, B.; Lafeber, H.N.; Michaelsen, K.F.; Puntis, J.W.L.; et al. Feeding preterm infants after hospital discharge: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 596–603. [Google Scholar] [CrossRef]
- Tudehope, D.; Vento, M.; Bhutta, Z.; Pachi, P. Nutritional requirements and feeding recommendations for small for gestational age infants. J Pediatr. 2013, 162, S81–S89. [Google Scholar] [CrossRef]
- Wang, N.; Cui, L.; Liu, Z.; Wang, Y.; Zhang, Y.; Shi, C.; Cheng, Y. Optimizing parenteral nutrition to achieve an adequate weight gain according to the current guidelines in preterm infants with birth weight less than 1500 g: A prospective observational study. BMC Pediatr. 2021, 21, 303. [Google Scholar] [CrossRef]
- Kosmeri, C.; Giapros, V.; Rallis, D.; Balomenou, F.; Serbis, A.; Baltogianni, M. Classification and Special Nutritional Needs of SGA Infants and Neonates of Multiple Pregnancies. Nutrients 2023, 15, 2736. [Google Scholar] [CrossRef]
- Bahlmann, F.; Reinhard, I.; Krummenauer, F.; Neubert, S.; Macchiella, D.; Wellek, S. Blood flow velocity waveforms of the fetal middle cerebral artery in a normal population: Reference values from 18 weeks to 42 weeks of gestation. J. Perinat. Med. 2002, 30, 490–501. [Google Scholar] [CrossRef]
- Khalil, A.; Beune, I.; Hecher, K.; Wynia, K.; Ganzevoort, W.; Reed, K.; Lewi, L.; Oepkes, D.; Gratacos, E.; Thilaganathan, B.; et al. Consensus definition and essential reporting parameters of selective fetal growth restriction in twin pregnancy: A Delphi procedure. Ultrasound Obstet. Gynecol. 2019, 53, 47–54. [Google Scholar] [CrossRef]
- Wagner, S.; Repke, J.T.; Ural, S.H. Overview and Long-term Outcomes of Patients Born with Twin-to-Twin Transfusion Syndrome. Rev. Obstet. Gynecol. 2013, 6, 149–154. [Google Scholar]
- Norris, T.; Ramel, S.E.; Catalano, P.; Caoimh, C.N.; Roggero, P.; Murray, D.; Fields, D.A.; Demerath, E.W.; Johnson, W. New charts for the assessment of body composition, according to air-displacement plethysmography, at birth and across the first 6 mo of life. Am. J. Clin. Nutr. 2019, 109, 1353–1360. [Google Scholar] [CrossRef]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [CrossRef]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group; de Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Walsh, M.C.; Kliegman, R.M. Necrotizing enterocolitis: Treatment based on staging criteria. Pediatr. Clin N. Am. 1986, 33, 179–201. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef]
- Gale, C.; Logan, K.M.; Jeffries, S.; Parkinson, J.R.; Santhakumaran, S.; Uthaya, S.; Durighel, G.; Alavi, A.; Thomas, E.L.; Bell, J.D.; et al. Sexual dimorphism in relation to adipose tissue and intrahepatocellular lipid deposition in early infancy. Int. J. Obes. 2015, 39, 629–632. [Google Scholar] [CrossRef]
- Uthaya, S.; Thomas, E.L.; Hamilton, G.; Dore, C.J.; Bell, J.; Modi, N. Altered adiposity after extremely preterm birth. Pediatr. Res. 2005, 57, 211–215. [Google Scholar] [CrossRef]
- Sharma, D.; Shastri, S.; Sharma, P. Intrauterine Growth Restriction: Antenatal and Postnatal Aspects. Clin. Med. Insights Pediatr. 2016, 10, 67–83. [Google Scholar] [CrossRef]
- Carberry, A.E.; Gordon, A.; Bond, D.M.; Hyett, J.; Raynes-Greenow, C.H.; Jeffery, H.E. Customised versus population-based growth charts as a screening tool for detecting small for gestational age infants in low-risk pregnant women. Cochrane Database Syst. Rev. 2014, 2014, CD008549. [Google Scholar] [CrossRef]
- Malhotra, A.; Allison, B.J.; Castillo-Melendez, M.; Jenkin, G.; Polglase, G.R.; Miller, S.L. Neonatal Morbidities of Fetal Growth Restriction: Pathophysiology and Impact. Front. Endocrinol. 2019, 10, 55. [Google Scholar] [CrossRef]
- Wesolowski, S.R.; Hay, W.W., Jr. Role of placental insufficiency and intrauterine growth restriction on the activation of fetal hepatic glucose production. Mol. Cell. Endocrinol. 2016, 435, 61–68. [Google Scholar] [CrossRef]
- Limesand, S.W.; Rozance, P.J. Fetal adaptations in insulin secretion result from high catecholamines during placental insufficiency. J. Physiol. 2017, 595, 5103–5113. [Google Scholar] [CrossRef]
- Priante, E.; Verlato, G.; Giordano, G.; Stocchero, M.; Visentin, S.; Mardegan, V.; Baraldi, E. Intrauterine Growth Restriction: New Insight from the Metabolomic Approach. Metabolites 2019, 9, 267. [Google Scholar] [CrossRef]
- Chernausek, S.D. Update: Consequences of abnormal fetal growth. J. Clin. Endocrinol. Metab. 2012, 97, 689–695. [Google Scholar] [CrossRef]
- Thorn, S.R.; Rozance, P.J.; Brown, L.D.; Hay, W.W., Jr. The intrauterine growth restriction phenotype: Fetal adaptations and potential implications for later life insulin resistance and diabetes. Semin. Reprod. Med. 2011, 29, 225–236. [Google Scholar] [CrossRef]
- Manapurath, R.; Gadapani, B.; Pereira-da-Silva, L. Body Composition of Infants Born with Intrauterine Growth Restriction: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 1085. [Google Scholar] [CrossRef]
- Morlacchi, L.; Mallardi, D.; Gianni, M.L.; Roggero, P.; Amato, O.; Piemontese, P.; Consonni, D.; Mosca, F. Is targeted fortification of human breast milk an optimal nutrition strategy for preterm infants? An interventional study. J. Transl. Med. 2016, 14, 195. [Google Scholar] [CrossRef]
- Fusch, S.; Fusch, G.; Yousuf, E.I.; Rochow, M.; So, H.Y.; Fusch, C.; Rochow, N. Individualized Target Fortification of Breast Milk: Optimizing Macronutrient Content Using Different Fortifiers and Approaches. Front. Nutr. 2021, 8, 652641. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Ali, A.; Bhatia, A.; So, H.Y.; Iskander, R.; Chessell, L.; El Helou, S.; Fusch, C. Individualized target fortification of breast milk with protein, carbohydrates, and fat for preterm infants: A double-blind randomized controlled trial. Clin. Nutr. 2021, 40, 54–63. [Google Scholar] [CrossRef]
- Parat, S.; Raza, P.; Kamleh, M.; Super, D.; Groh-Wargo, S. Targeted Breast Milk Fortification for Very Low Birth Weight (VLBW) Infants: Nutritional Intake, Growth Outcome and Body Composition. Nutrients 2020, 12, 1156. [Google Scholar] [CrossRef]
- Pereira-da-Silva, L.; Virella, D.; Fusch, C. Nutritional Assessment in Preterm Infants: A Practical Approach in the NICU. Nutrients 2019, 11, 1999. [Google Scholar] [CrossRef]
- Pfister, K.M.; Zhang, L.; Miller, N.C.; Ingolfsland, E.C.; Demerath, E.W.; Ramel, S.E. Early body composition changes are associated with neurodevelopmental and metabolic outcomes at 4 years of age in very preterm infants. Pediatr. Res. 2018, 84, 713–718. [Google Scholar] [CrossRef]
- Embleton, N.D.; Korada, M.; Wood, C.L.; Pearce, M.S.; Swamy, R.; Cheetham, T.D. Catch-up growth and metabolic outcomes in adolescents born preterm. Arch. Dis. Child. 2016, 101, 1026–1031. [Google Scholar] [CrossRef]
- Ou-Yang, M.C.; Sun, Y.; Liebowitz, M.; Chen, C.C.; Fang, M.L.; Dai, W.; Chuang, T.W.; Chen, J.L. Accelerated weight gain, prematurity, and the risk of childhood obesity: A meta-analysis and systematic review. PLoS ONE 2020, 15, e0232238. [Google Scholar] [CrossRef]
- de Fluiter, K.S.; van Beijsterveldt, I.; Breij, L.M.; Acton, D.; Hokken-Koelega, A.C.S. Association Between Fat Mass in Early Life and Later Fat Mass Trajectories. JAMA Pediatr. 2020, 174, 1141–1148. [Google Scholar] [CrossRef]
- Zheng, M.; Lamb, K.E.; Grimes, C.; Laws, R.; Bolton, K.; Ong, K.K.; Campbell, K. Rapid weight gain during infancy and subsequent adiposity: A systematic review and meta-analysis of evidence. Obes. Rev. 2018, 19, 321–332. [Google Scholar] [CrossRef]
- Goossens, G.H. The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function. Obes. Facts 2017, 10, 207–215. [Google Scholar] [CrossRef]
- van de Lagemaat, M.; Rotteveel, J.; Lafeber, H.N.; van Weissenbruch, M.M. Lean mass and fat mass accretion between term age and 6 months post-term in growth-restricted preterm infants. Eur. J. Clin. Nutr. 2014, 68, 1261–1263. [Google Scholar] [CrossRef]
- Villela, L.D.; Meio, M.; Gomes Junior, S.C.S.; de Abranches, A.D.; Soares, F.V.M.; Moreira, M.E.L. Body composition in preterm infants with intrauterine growth restriction: A cohort study. J. Perinat. Med. 2018, 46, 804–810. [Google Scholar] [CrossRef]
- Gianni, M.L.; Roggero, P.; Liotto, N.; Taroni, F.; Polimeni, A.; Morlacchi, L.; Piemontese, P.; Consonni, D.; Mosca, F. Body composition in late preterm infants according to percentile at birth. Pediatr. Res. 2016, 79, 710–715. [Google Scholar] [CrossRef]


{kind=link}
| Variables | AGA Group (n = 249) | IUGR Group (n = 40) | SGA Group (n = 11) | AGA vs. IUGR p-Values | AGA vs. SGA p-Values |
|---|---|---|---|---|---|
| Gestational age, weeks * | 26.9 (25.8, 31.0) | 30.4 (25.9, 35.7) | 28.1 (25.5, 28.9) | <0.001 | 0.21 |
| Male, % (n) | 58 (144/249) | 35 (14/40) | 64 (7/11) | 0.006 | 0.56 |
| Antenatal steroids, % (n) | 43 (107/249) | 58 (23/40) | 82 (9/11) | 0.13 | 0.016 |
| PROM, % (n) | 17 (41/249) | 5 (2/40) | 18 (2/11) | <0.001 | 0.21 |
| Caesarean delivery, % (n) | 69 (171/249) | 83 (33/40) | 73 (8/11) | 0.08 | 0.88 |
| APGAR Score, 5 min * | 9 (8, 9) | 9 (9, 9) | 9 (9, 9) | 0.11 | 0.26 |
| APGAR Score, 10 min * | 9 (9, 9) | 9 (9, 10) | 9 (9, 9) | 0.83 | 0.83 |
| Umbilical artery, pH * | 7.32 (7.29, 7.39) | 7.30 (7.27, 7.36) | 7.31 (7.28, 7.34) | 0.07 | 0.51 |
| Anthropometry at birth | |||||
| Birth weight, gram * | 935 (757, 1399) | 1050 (550, 1835) | 623 (543, 735) | 0.05 | <0.001 |
| Birth weight, Z-Score * | 0.0 (−0.8, 0.3) | −1.6 (−1.8, −1.5) | −1.5 (−2.0, −1.4) | <0.001 | <0.001 |
| Birth length, cm * | 35 (32, 41) | 39 (30, 44) | 31 (30, 33) | 0.09 | <0.001 |
| Birth length, Z-Score * | 0.0 (−0.7, 0.9) | −1.2 (−1.9, −0.7) | −1.7 (−2.5, −1.4) | <0.001 | <0.001 |
| Birth HC, cm * | 24.8 (23.0, 29.0) | 25.5 (21.3, 30.5) | 23.3 (21.5, 25.4) | 0.89 | 0.001 |
| Birth HC, Z-Score * | 0.2 (−0.3, 0.9) | −1.3 (−1.9, −0.9) | −1.1 (−2.0, −0.1) | <0.001 | <0.001 |
| Variables | AGA Group (n = 249) | IUGR Group (n = 40) | SGA Group (n = 11) | IUGR vs. AGA p-Values | SGA vs. AGA p-Values |
|---|---|---|---|---|---|
| PMA at discharge, week * | 38.1 (36.9, 40.0) | 39.7 (37.7, 41.5) | 39.7 (37.6, 45.4) | 0.29 | 0.09 |
| Discharge weight, gram * | 2805 (2442, 3114) | 2333 (1998, 2765) | 2730 (2080, 3190) | <0.001 | 0.67 |
| Weight velocity, g/kg/d * | 22.0 (19.5, 24.5) | 20.3 (18.5, 23.1) | 21.5 (17.7, 24.1) | 0.022 | 0.74 |
| Discharge length, cm * | 46 (44, 48.5) | 44 (41, 46) | 44 (40, 46) | <0.001 | 0.07 |
| Length increase, cm/week * | 0.95 (0.82, 1.07) | 1.03 (0.91, 1.10) | 0.94 (0.83, 1.11) | 0.14 | 0.97 |
| Discharge HC, cm * | 33.0 (31.5, 34) | 32.0 (30.8, 33.8) | 31.5 (30.7, 33.8) | 0.10 | 0.37 |
| HC increase, cm/week * | 0.69 (0.59, 0.78) | 0.72 (0.61, 0.81) | 0.74 (0.58, 0.83) | 0.35 | 0.22 |
| ROP grade II-IV, % (n) | 13 (33/249) | 10 (4/40) | 27 (3/11) | 0.43 | 0.17 |
| IVH (stage ≥ 2), % (n) | 7 (18/249) | 8 (3/40) | 18 (2/11) | 0.90 | 0.18 |
| NEC (stage ≥ 2), % (n) | 8 (19/249) | 3 (1/40) | 9 (1/11) | 0.23 | 0.78 |
| BPD, % (n) | 12 (30/249) | 10 (4/40) | 27 (3/11) | 0.63 | 0.13 |
| Culture-proven sepsis, % (n) | 22 (55/249) | 33 (13/40) | 27 (3/11) | 0.16 | 0.78 |
| Variables | AGA Group (n = 249) | IUGR Group (n = 40) | SGA Group (n = 11) | IUGR vs. AGA p-Values | SGA vs. AGA p-Values |
|---|---|---|---|---|---|
| Parenteral and Enteral Nutrition * | |||||
| Days on PN | 18 (12, 21) | 17 (11, 21) | 24 (16, 33) | 0.68 | 0.07 |
| Total Energy (kcal/kg/d) | 108 (104, 116) | 107 (104, 113) | 114 (110, 120) | 0.31 | 0.14 |
| Total Carbohydrates (mg/kg/min) | 7.9 (6.8, 8.6) | 7.4 (6.2, 8.3) | 6.4 (5.9, 7.9) | 0.73 | 0.29 |
| Total Protein (g/kg/d) | 3.7 (3.5, 3.8) | 3.6 (3.4, 3.6) | 3.3 (3.1, 3.9) | 0.90 | 0.14 |
| Total Fat (g/kg/d) | 3.9 (3.6, 4.5) | 3.5 (3.0, 4.2) | 3.4 (2.8, 4.1) | 0.43 | 0.51 |
| Enteral nutrition, % (n) | |||||
| Human Milk + HMF | 28 (70/249) | 30 (12/40) | 27 (3/11) | 0.80 | 0.95 |
| Human Milk + BMF | 33 (82/249) | 30 (12/40) | 45 (5/11) | 0.71 | 0.38 |
| Formula | 5 (12/249) | 7 (3/40) | 0 (0/11) | 0.47 | 0.45 |
| Mixed | 34 (85/249) | 33 (13/40) | 27 (3/11) | 0.83 | 0.63 |
| Exclusively mother’s own milk at discharge | 61 (152/249) | 60 (24/40) | 73 (8/11) | 0.68 | 0.45 |
| AGA Group (n = 249) | IUGR Group (n = 40) | SGA Group (n = 11) | |
|---|---|---|---|
| PMA at measurement, week | 42.1 (40.0, 46.3) | 43.0 (40.5, 46.9) | 42.1 (39.4, 52.6) |
| Body composition parameters | |||
| FFM, percentage | 77.8 (73.9, 83.6) | 81.9 (73.3, 85.4) | 78.2 (76.6, 81.2) |
| FM, percentage | 22.2 (16.5, 26.1) | 18.2 (14.6, 26.7) | 21.8 (18.8, 23.4) |
| FFM, gram | 2896 (2403, 3412) | 2428 (2147, 2859) | 2510 (2121, 2920) |
| FM, gram | 785 (512, 1174) | 662 (382, 893) | 620 (530, 799) |
| Anthropometric parameters | |||
| Weight, gram | 3681 (2915, 4586) | 3090 (2529, 3752) | 3130 (2651, 3719) |
| Length, cm | 46.0 (44.0, 48.5) | 44.0 (41.0, 46.0) | 44.0 (40.0, 46.0) |
| Head circumference, cm | 33.0 (31.5, 34.0) | 32.0 (30.8, 33.8) | 31.5 (30.7, 33.8) |
| Adjusted Mean | Adjusted Mean Difference | ||||
|---|---|---|---|---|---|
| AGA Group | IUGR Group | SGA Group | IUGR Group | SGA Group | |
| Total (n) | 249 | 40 | 11 | ||
| Weight at scan, gram 1 | 3797 (3745, 3849) | 3667 (3528, 3806) | 3736 (3480, 3992) | −130 (−21, 281) | −46 (−215, 307) |
| p = 0.09 | p = 0.73 | ||||
| FFM, Z-Score | −1.1 (−1.2, −1.0) | −1.5 (−1.8, −1.2) | −1.0 (−1.6, −0.5) | −0.4 (−0.8, −1.0) | −0,1 (−0.5, 0.7) |
| p = 0.017 | p = 0.79 | ||||
| FM, Z-Score | 0.8 (0.7, 0.9) | 0.7 (0.3, 1.0) | 1.2 (0.5, 1.9) | 0.1 (−0.5, 0.3) | 0.4 (−0.3, 1.1) |
| p = 0.48 | p = 0.24 | ||||
| FFM, gram | 2977 (2919, 3035) | 2654 (2502, 2807) | 2823 (2690, 2956) | −323 (−488, −158) | −154 (−229, 79) |
| p < 0.001 | p = 0.09 | ||||
| FM, gram | 843 (817, 868) | 847 (774, 921) | 958 (825, 1092) | 4 (8, 53) | 116 (−21, 252) |
| p = 0.99 | p = 0.09 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calek, E.; Binder, J.; Palmrich, P.; Eibensteiner, F.; Thajer, A.; Kainz, T.; Harreiter, K.; Berger, A.; Binder, C. Effects of Intrauterine Growth Restriction (IUGR) on Growth and Body Composition Compared to Constitutionally Small Infants. Nutrients 2023, 15, 4158. https://doi.org/10.3390/nu15194158
Calek E, Binder J, Palmrich P, Eibensteiner F, Thajer A, Kainz T, Harreiter K, Berger A, Binder C. Effects of Intrauterine Growth Restriction (IUGR) on Growth and Body Composition Compared to Constitutionally Small Infants. Nutrients. 2023; 15(19):4158. https://doi.org/10.3390/nu15194158
Chicago/Turabian StyleCalek, Elisabeth, Julia Binder, Pilar Palmrich, Felix Eibensteiner, Alexandra Thajer, Theresa Kainz, Karin Harreiter, Angelika Berger, and Christoph Binder. 2023. "Effects of Intrauterine Growth Restriction (IUGR) on Growth and Body Composition Compared to Constitutionally Small Infants" Nutrients 15, no. 19: 4158. https://doi.org/10.3390/nu15194158
APA StyleCalek, E., Binder, J., Palmrich, P., Eibensteiner, F., Thajer, A., Kainz, T., Harreiter, K., Berger, A., & Binder, C. (2023). Effects of Intrauterine Growth Restriction (IUGR) on Growth and Body Composition Compared to Constitutionally Small Infants. Nutrients, 15(19), 4158. https://doi.org/10.3390/nu15194158