

Machine Learning-Based Prediction of Complications and Prolonged Hospitalization with the GLIM Criteria Combinations Containing Calf Circumference in Elderly Asian Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
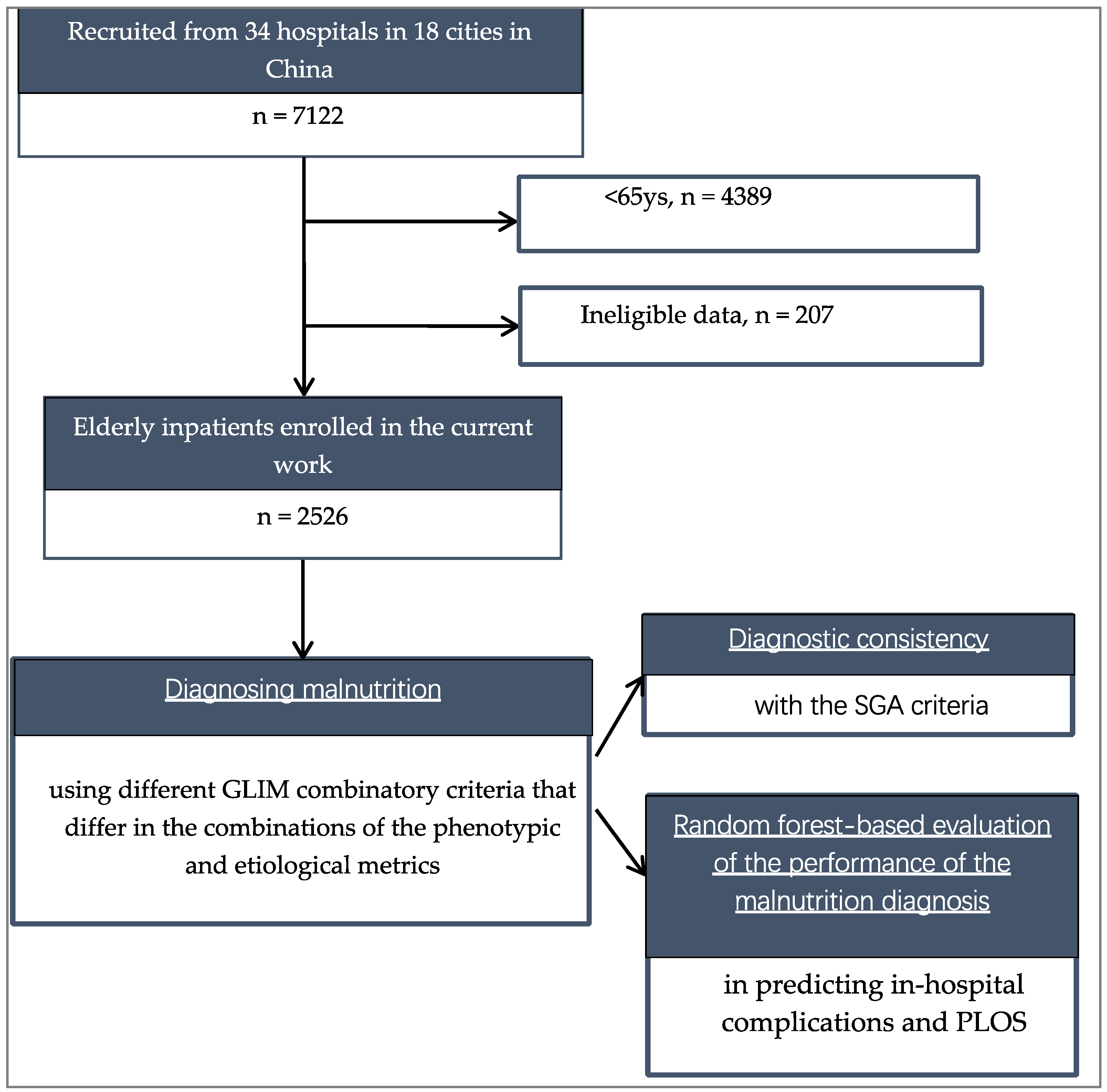
2.1. Population
2.2. Data Collection
2.3. Adverse Clinical Outcomes
2.4. Diagnostic Criteria for Malnutrition
2.4.1. The SGA Criteria
2.4.2. The GLIM Criteria
2.5. Statistical Analysis
2.6. Machine Learning Algorithm
3. Results
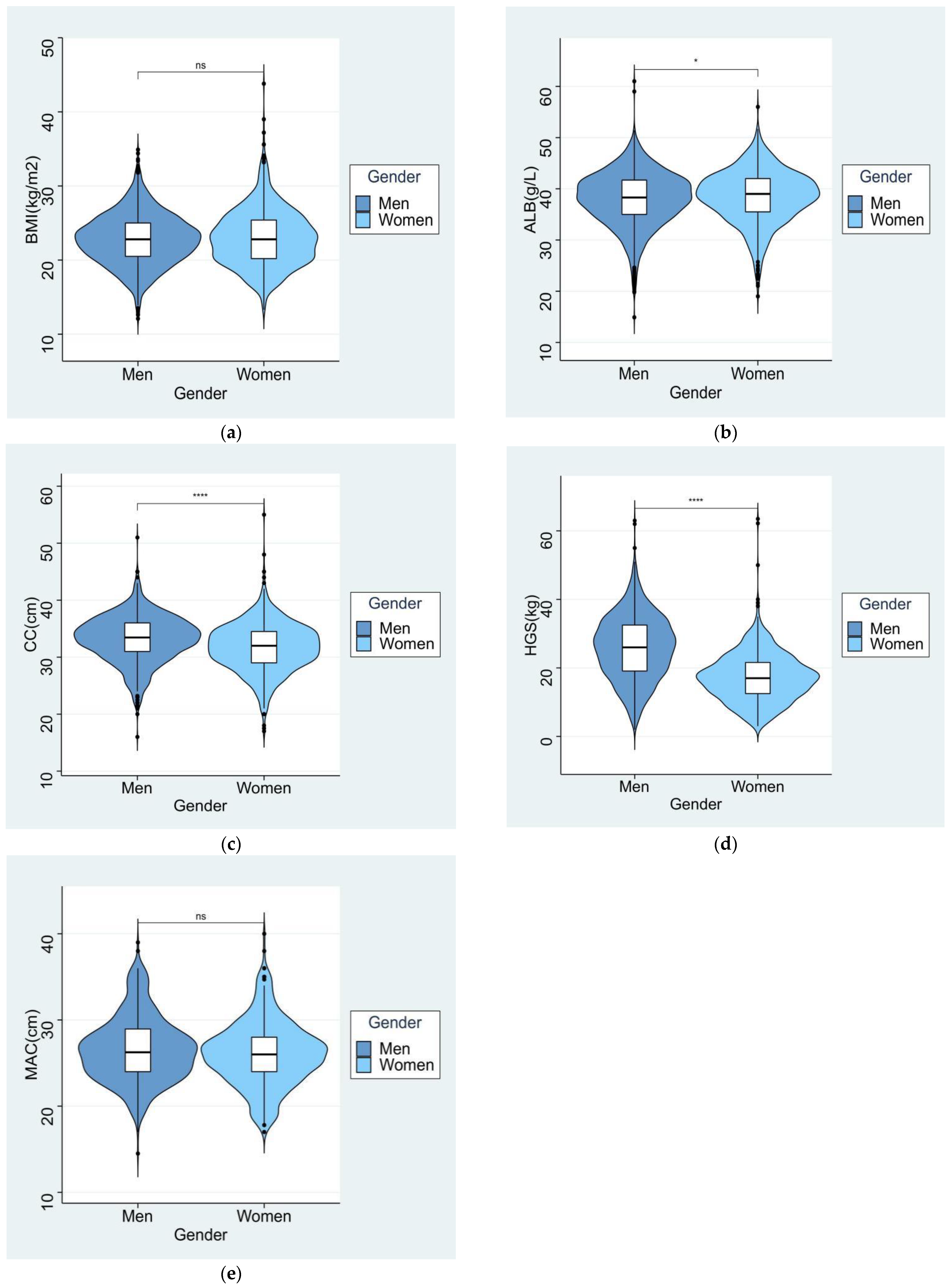
3.1. Baseline Characteristics of the Subjects
3.2. Prevalence of the Single GLIM Phenotypic and Etiological Criteria in the Subjects
3.3. Prevalence of Malnutrition Diagnosed with the 33 GLIM Criteria Combinations and Their Diagnostic Consistency with the SGA Criteria
3.4. Associations of Malnutrition Diagnosed with the 33 GLIM Criteria Combinations with the Total 30-Day IHC and PLOS in Elderly Patients
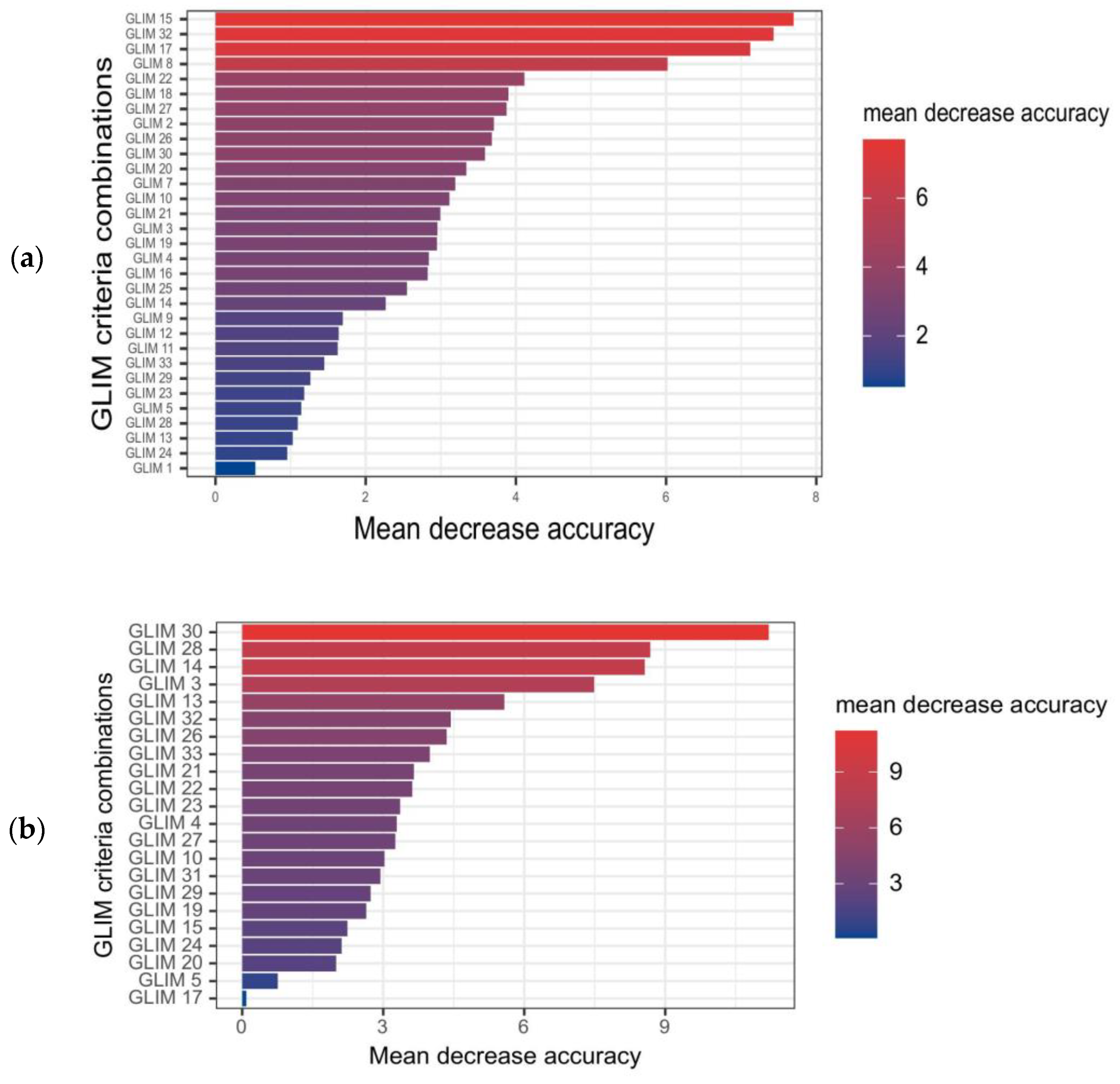
3.5. Performance of Malnutrition Defined by Different GLIM Criteria Combinations in Predicting Total IHC and PLOS in Elderly Inpatients
4. Discussion
4.1. Principal Findings
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cederholm, T.; Barazzoni, R. A year with the GLIM diagnosis of malnutrition—Does it work for older persons? Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Simpson, F.; Doig, G.S. Bedside nutrition evaluation and physical assessment techniques in critical illness. Curr. Opin. Crit. Care 2016, 22, 303–307. [Google Scholar] [CrossRef]
- Kiss, N.; Steer, B.; de van der Schueren, M.; Loeliger, J.; Alizadehsani, R.; Edbrooke, L.; Deftereos, I.; Laing, E.; Khosravi, A. Comparison of the prevalence of 21 GLIM phenotypic and etiologic criteria combinations and association with 30-day outcomes in people with cancer: A retrospective observational study. Clin. Nutr. 2022, 41, 1102–1111. [Google Scholar] [CrossRef]
- Santos, B.C.; Fonseca, A.L.F.; Ferreira, L.G.; Ribeiro, H.S.; Correia, M.; Lima, A.S.; Penna, F.G.C.; Anastácio, L.R. Different combinations of the GLIM criteria for patients awaiting a liver transplant: Poor performance for malnutrition diagnosis but a potentially useful prognostic tool. Clin. Nutr. 2022, 41, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Henrique, J.R.; Pereira, R.G.; Ferreira, R.S.; Keller, H.; de Van der Schueren, M.; Gonzalez, M.C.; Meira, W., Jr.; Toulson, M.I.; Correia, D. Pilot study GLIM criteria for categorization of a malnutrition diagnosis of patients undergoing elective gastrointestinal operations: A pilot study of applicability and validation. Nutrition 2020, 79–80, 110961. [Google Scholar] [CrossRef]
- Barazzoni, R.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Higashiguchi, T.; Shi, H.P.; Bischoff, S.C.; Boirie, Y.; Carrasco, F.; Cruz-Jentoft, A.; et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition (GLIM) diagnosis of malnutrition. Clin. Nutr. 2022, 41, 1425–1433. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.-Y.; Chen, L.-Y.; Hsu, P.-S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Abreo, A.P.; Bailey, S.R.; Abreo, K. Associations between calf, thigh, and arm circumference and cardiovascular and all-cause mortality in NHANES 1999–2004. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1410–1415. [Google Scholar] [CrossRef]
- Ishida, Y.; Maeda, K.; Nonogaki, T.; Shimizu, A.; Yamanaka, Y.; Matsuyama, R.; Kato, R.; Mori, N. Impact of edema on length of calf circumference in older adults. Geriatr. Gerontol. Int. 2019, 19, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Kakita, D.; Matsuzawa, R.; Yamamoto, S.; Suzuki, Y.; Harada, M.; Imamura, K.; Yoshikoshi, S.; Imai, H.; Osada, S.; Shimokado, K.; et al. Simplified discriminant parameters for sarcopenia among patients undergoing haemodialysis. J. Cachexia Sarcopenia Muscle 2022, 13, 2898–2907. [Google Scholar] [CrossRef] [PubMed]
- de van der Schueren, M.A.E.; Keller, H.; Consortium, G.; Cederholm, T.; Barazzoni, R.; Compher, C.; Correia, M.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M.; et al. Global Leadership Initiative on Malnutrition (GLIM): Guidance on validation of the operational criteria for the diagnosis of protein-energy malnutrition in adults. Clin. Nutr. 2020, 39, 2872–2880. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, K.; Fahling, K.; Roubaud-Baudron, C.; Sanchez-Rodriguez, D.; Bauer, J.; Gasowski, J. Highlights of the 14th International Congress of the European Geriatric Medicine Society. Eur. Geriatr. Med. 2019, 10, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lu, Z.; Li, Z.; Xu, J.; Cui, H.; Zhu, M. Influence of Malnutrition According to the GLIM Criteria on the Clinical Outcomes of Hospitalized Patients with Cancer. Front. Nutr. 2021, 8, 774636. [Google Scholar] [CrossRef]
- Ren, S.S.; Zhu, M.W.; Zhang, K.W.; Chen, B.W.; Yang, C.; Xiao, R.; Li, P.G. Machine Learning-Based Prediction of In-Hospital Complications in Elderly Patients Using GLIM-, SGA-, and ESPEN 2015-Diagnosed Malnutrition as a Factor. Nutrients 2022, 14, 3035. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M.; Educational. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enteral. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Weaving, G.; Batstone, G.F.; Jones, R.G. Age and sex variation in serum albumin concentration: An observational study. Ann. Clin. Biochem. 2016, 53, 106–111. [Google Scholar] [CrossRef]
- Munoz Fernandez, S.S.; Garcez, F.B.; Alencar, J.C.G.; Cederholm, T.; Aprahamian, I.; Morley, J.E.; de Souza, H.P.; da Silva, T.J.A.; Ribeiro, S.M.L. Applicability of the GLIM criteria for the diagnosis of malnutrition in older adults in the emergency ward: A pilot validation study. Clin. Nutr. 2021, 40, 5447–5456. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, D.; Locquet, M.; Bruyere, O.; Lengele, L.; Cavalier, E.; Reginster, J.Y.; Beaudart, C. Prediction of 5-year mortality risk by malnutrition according to the GLIM format using seven pragmatic approaches to define the criterion of loss of muscle mass. Clin. Nutr. 2021, 40, 2188–2199. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.C.; Mehrnezhad, A.; Razaviarab, N.; Barbosa-Silva, T.G.; Heymsfield, S.B. Calf circumference: Cutoff values from the NHANES 1999–2006. Am. J. Clin. Nutr. 2021, 113, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Shang, Y.; Fratiglioni, L.; Johnell, K.; Welmer, A.K.; Marseglia, A.; Xu, W. Individual changes in anthropometric measures after age 60 years: A 15-year longitudinal population-based study. Age Ageing 2021, 50, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.E.; Chen, W.L. Calf circumference refines sarcopenia in correlating with mortality risk. Age Ageing 2022, 51, afab239. [Google Scholar] [CrossRef]
- Contreras-Bolivar, V.; Sanchez-Torralvo, F.J.; Ruiz-Vico, M.; Gonzalez-Almendros, I.; Barrios, M.; Padin, S.; Alba, E.; Olveira, G. GLIM Criteria Using Hand Grip Strength Adequately Predict Six-Month Mortality in Cancer Inpatients. Nutrients 2019, 11, 2043. [Google Scholar] [CrossRef]
- Zhang, F.M.; Chen, X.L.; Wu, Q.; Dong, W.X.; Dong, Q.T.; Shen, X.; Shi, H.-P.; Yu, Z.; Zhuang, C.-L. Development and validation of nomograms for the prediction of low muscle mass and radiodensity in gastric cancer patients. Am. J. Clin. Nutr. 2021, 113, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Lin, X.; Zhao, Z.; Li, N.; He, X.; Zhang, M.; Yang, J.; Guo, Z.; Li, Z.; Wang, K.; et al. Is hand grip strength a necessary supportive index in the phenotypic criteria of the GLIM-based diagnosis of malnutrition in patients with cancer? Support Care Cancer 2021, 29, 4001–4013. [Google Scholar] [CrossRef]
- Yin, L.; Cheng, N.; Chen, P.; Zhang, M.; Li, N.; Lin, X.; He, X.; Wang, Y.; Xu, H.; Guo, W.; et al. Association of Malnutrition, as Defined by the PG-SGA, ESPEN 2015, and GLIM Criteria, With Complications in Esophageal Cancer Patients After Esophagectomy. Front. Nutr. 2021, 8, 632546. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men | Women | Total | p |
|---|---|---|---|---|
| n | 1495(59.18) | 1031(40.82) | 2526 | 0.000 |
| General characteristics | ||||
| Age (year) | 74.73 ± 7.31 | 74.49 ± 6.82 | 74.63 ± 7.12 | 0.383 |
| Married (%) | 1401(93.7) | 976(94.7) | 2377(94.2) | 0.318 |
| Height * (cm) | 168.91 ± 6.09 | 157.47 ± 6.00 | 164.24 ± 8.26 | 0.000 |
| Weight * (kg) | 65.11 ± 10.95 | 57.06 ± 10.43 | 61.83 ± 11.45 | 0.000 |
| BMI (kg/m2) | 22.78 ± 3.40 | 22.98 ± 3.81 | 22.86 ± 3.57 | 0.179 |
| Education level * | ||||
| Primary school and lower | 1013(67.8) | 800(77.6) | 1813(71.8) | 0.000 |
| High school | 220(14.7) | 111(10.8) | 331(13.1) | |
| Bachelor’s degree or above | 262(17.5) | 120(11.6) | 382(15.1) | |
| Hospitalization reasons | ||||
| Endocrine diseases | 33(2.2) | 30(2.9) | 63(2.5) | 0.266 |
| Nervous system diseases | 249(16.7) | 181(17.6) | 430(17.0) | 0.554 |
| Osteoarthropathy * | 49(3.3) | 92(8.9) | 141(5.6) | 0.000 |
| Digestive diseases * | 238(15.9) | 225(21.8) | 463(18.3) | 0.001 |
| Respiratory diseases | 143(9.6) | 80(7.8) | 223(8.8) | 0.116 |
| Cardiovascular diseases | 80(5.4) | 58(5.6) | 138(5.5) | 0.765 |
| Tumors * | 615(41.1) | 333(32.3) | 948(37.5) | 0.000 |
| Kidney diseases | 6(0.4) | 4(0.4) | 10(0.4) | 0.958 |
| Nutritional status according to the SGA criteria | ||||
| A(%) | 983(65.8) | 714(69.3) | 1697(67.2) | 0.180 |
| B(%) | 437(29.2) | 269(26.1) | 706(27.9) | |
| C(%) | 75(5.0) | 48(4.7) | 123(4.9) | |
| Blood parameters | ||||
| Total protein * (g/L) | 65.04 ± 6.90 | 66.06 ± 6.94 | 65.45 ± 6.93 | 0.001 |
| Triglyceride * (mmol/L) | 1.17(0.46) | 1.36(0.61) | 1.24(0.50) | 0.000 |
| Total cholesterol * (mmol/L) | 3.96 ± 1.40 | 4.28 ± 1.53 | 4.08 ± 1.46 | 0.000 |
| Hemoglobin * (g/L) | 125.64 ± 21.34 | 117.81 ± 18.10 | 122.43 ± 20.44 | 0.000 |
| Lymphocytes * (109/L) | 1.45(0.53) | 1.58(0.55) | 1.57(0.59) | 0.001 |
| Men | Women | Total | p | |
|---|---|---|---|---|
| Phenotypic criteria | ||||
| Weight loss * | 349(23.3) | 203(19.7) | 552(21.9) | 0.029 |
| BMI reduction | 243(16.3) | 187(18.1) | 430(17.0) | 0.216 |
| CC reduction * | 691(46.2) | 550(53.3) | 1241(49.1) | 0.000 |
| CC reduction+HGS reduction | 483(32.3) | 335(32.5) | 818(32.4) | 0.922 |
| Etiological criteria | ||||
| Low food intake or absorption | 718(48.0) | 503(48.8) | 1221(48.3) | 0.707 |
| Disease burden or inflammation * | 687(46.0) | 428(41.5) | 1115(44.1) | 0.027 |
| GLIM Criteria Combinations | Malnourished Patients, n (%) | Kappa vs. SGA | 95% CI |
|---|---|---|---|
| Combinations with 1 phenotypic and 1 etiological criterion | |||
| GLIM 1 (W+F) | 409 (16.2) | 0.567 | (0.532–0.602) |
| GLIM 2 (W+D) | 408 (16.2) | 0.581 | (0.546–0.616) |
| GLIM 3 (B+F) | 269 (10.6) | 0.566 | (0.531–0.601) |
| GLIM 4 (B+D) | 319 (12.6) | 0.429 | (0.397–0.460) |
| GLIM 5 (M1+F) | 686 (27.2) | 0.866 | (0.827–0.904) |
| GLIM 6 (M2+F) | 479 (19.0) | 0.648 | (0.611–0.684) |
| GLIM 7 (M1+D) | 653 (25.9) | 0.833 | (0.795–0.871) |
| GLIM 8 (M2+D) | 453 (17.9) | 0.618 | (0.582–0.654) |
| Combinations with 2 phenotypic and 1 etiological criterion | |||
| GLIM 9 (WF+D) | 327 (12.9) | 0.467 | (0.434–0.500) |
| GLIM 10 (BF+D) | 219 (8.7) | 0.325 | (0.297–0.354) |
| GLIM 11 (M1+FD) | 445 (17.6) | 0.609 | (0.573–0.645) |
| GLIM 12 (M2+FD) | 315 (12.5) | 0.452 | (0.419–0.484) |
| GLIM 13 (WB+F) | 142 (5.6) | 0.217 | (0.193–0.242) |
| GLIM 14 (WB+D) | 171 (6.8) | 0.259 | (0.233–0.285) |
| GLIM 15 (WM1+D) | 264 (10.5) | 0.386 | (0.355–0.417) |
| GLIM 16 (WM2+D) | 197 (7.8) | 0.341 | (0.311–0.371) |
| GLIM 17 (WM1+F) | 257 (10.2) | 0.376 | (0.346–0.407) |
| GLIM 18 (WM2+F) | 186 (7.4) | 0.280 | (0.253–0.307) |
| GLIM 19 (BM1+F) | 226 (8.9) | 0.335 | (0.306–0.364) |
| GLIM 20 (BM2+F) | 172 (6.8) | 0.260 | (0.234–0.287) |
| GLIM 21 (BM1+D) | 265 (10.5) | 0.396 | (0.365–0.428) |
| GLIM 22 (BM2+D) | 199 (7.9) | 0.298 | (0.270–0.326) |
| Combinations with 2 phenotypic and 2 etiological criteria | |||
| GLIM 23 (WB+FD) | 128 (5.1) | 0.197 | (0.174–0.220) |
| GLIM 24 (WM1+FD) | 287 (11.4) | 0.416 | (0.384–0.447) |
| GLIM 25 (WM2+FD) | 166 (6.6) | 0.252 | (0.226–0.278) |
| GLIM 26 (BM1+FD) | 182 (7.2) | 0.274 | (0.248–0.301) |
| GLIM 27 (BM2+FD) | 141 (5.6) | 0.216 | (0.192–0.240) |
| Combinations with 3 phenotypic and 1 etiological criterion | |||
| GLIM 28 (WBM1+F) | 121 (4.8) | 0.187 | (0.164–0.209) |
| GLIM 29 (WBM2+F) | 91 (3.6) | 0.142 | (0.122–0.162) |
| GLIM 30 (WBM1+D) | 130 (5.1) | 0.200 | (0.177–0.223) |
| GLIM 31 (WBM2+D) | 99 (3.9) | 0.154 | (0.133–0.175) |
| Combinations with 3 phenotypic and 2 etiological criteria | |||
| GLIM 32 (WBM1+FD) | 142 (5.6) | 0.217 | (0.193–0.242) |
| GLIM 33 (WBM2+FD) | 83 (3.3) | 0.130 | (0.111–0.149) |
| GLIM Criteria Combinations | In-Hospital Complications | PLOS | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| GLIM 1 | 2.220 | 1.428–3.450 | 0.000 | 1.199 | 0.966–1.489 | 0.100 |
| GLIM 2 | 2.579 | 1.676–3.969 | 0.000 | 1.241 | 0.999–1.541 | 0.051 |
| GLIM 3 | 2.155 | 1.290–3.602 | 0.003 | 1.354 | 1.046–1.752 | 0.021 |
| GLIM 4 | 2.074 | 1.275–3.375 | 0.003 | 1.288 | 1.013–1.637 | 0.039 |
| GLIM 5 | 2.076 | 1.351–3.040 | 0.001 | 1.217 | 1.016–1.458 | 0.033 |
| GLIM 6 | 1.537 | 0.972–2.431 | 0.066 | 1.118 | 0.962–1.450 | 0.112 |
| GLIM 7 | 2.710 | 1.806–4.065 | 0.000 | 1.182 | 0.983–1.421 | 0.075 |
| GLIM 8 | 1.849 | 1.176–2.908 | 0.008 | 1.094 | 0.885–1.351 | 0.407 |
| GLIM 9 | 2.827 | 1.804–4.432 | 0.000 | 1.219 | 0.962–1.546 | 0.101 |
| GLIM 10 | 2.380 | 1.395–4.061 | 0.001 | 1.398 | 1.055–1.852 | 0.020 |
| GLIM 11 | 2.849 | 1.869–4.344 | 0.000 | 1.234 | 1.000–1.521 | 0.050 |
| GLIM 12 | 2.224 | 1.375–3.597 | 0.001 | 1.138 | 0.983–1.450 | 0.297 |
| GLIM 13 | 2.369 | 1.259–4.458 | 0.007 | 1.864 | 1.321–2.630 | 0.000 |
| GLIM 14 | 2.081 | 1.134–3.822 | 0.018 | 1.891 | 1.379–2.593 | 0.000 |
| GLIM 15 | 3.336 | 2.100–5.299 | 0.000 | 1.364 | 1.053–1.767 | 0.019 |
| GLIM 16 | 2.097 | 1.185–3.714 | 0.011 | 1.273 | 0.947–1.711 | 0.109 |
| GLIM 17 | 3.074 | 1.915–4.935 | 0.000 | 1.376 | 1.059–1.787 | 0.017 |
| GLIM 18 | 2.241 | 1.264–3.975 | 0.006 | 1.311 | 0.968–1.775 | 0.080 |
| GLIM 19 | 2.668 | 1.589–4.481 | 0.000 | 1.520 | 1.151–2.008 | 0.003 |
| GLIM 20 | 2.698 | 1.528–4.763 | 0.001 | 1.457 | 1.063–1.997 | 0.019 |
| GLIM 21 | 2.473 | 1.502–4.072 | 0.000 | 1.480 | 1.142–1.918 | 0.003 |
| GLIM 22 | 2.228 | 1.268–3.916 | 0.005 | 1.437 | 1.070–1.930 | 0.016 |
| GLIM 23 | 2.676 | 1.419–5.047 | 0.002 | 1.851 | 1.290–2.656 | 0.001 |
| GLIM 24 | 3.557 | 2.267–5.582 | 0.000 | 1.319 | 1.027–1.694 | 0.030 |
| GLIM 25 | 2.372 | 1.314–4.280 | 0.004 | 1.086 | 0.786–1.502 | 0.617 |
| GLIM 26 | 2.983 | 1.729–5.117 | 0.000 | 1.667 | 1.228–2.265 | 0.001 |
| GLIM 27 | 2.839 | 1.560–5.169 | 0.001 | 1.605 | 1.137–2.266 | 0.007 |
| GLIM 28 | 2.876 | 1.520–5.439 | 0.001 | 2.160 | 1.485–3.142 | 0.000 |
| GLIM 29 | 2.378 | 1.114–5.075 | 0.025 | 2.104 | 1.370–3.229 | 0.001 |
| GLIM 30 | 2.880 | 1.557–5.328 | 0.001 | 2.173 | 1.514–3.121 | 0.000 |
| GLIM 31 | 2.120 | 0.997–4.511 | 0.051 | 1.999 | 1.328–3.011 | 0.001 |
| GLIM 32 | 3.082 | 1.718–5.530 | 0.000 | 1.577 | 1.118–2.224 | 0.009 |
| GLIM 33 | 2.647 | 1.237–5.665 | 0.012 | 2.073 | 1.326–3.241 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, S.-S.; Zhang, K.-W.; Chen, B.-W.; Yang, C.; Xiao, R.; Li, P.-G.; Zhu, M.-W. Machine Learning-Based Prediction of Complications and Prolonged Hospitalization with the GLIM Criteria Combinations Containing Calf Circumference in Elderly Asian Patients. Nutrients 2023, 15, 4146. https://doi.org/10.3390/nu15194146
Ren S-S, Zhang K-W, Chen B-W, Yang C, Xiao R, Li P-G, Zhu M-W. Machine Learning-Based Prediction of Complications and Prolonged Hospitalization with the GLIM Criteria Combinations Containing Calf Circumference in Elderly Asian Patients. Nutrients. 2023; 15(19):4146. https://doi.org/10.3390/nu15194146
Chicago/Turabian StyleRen, Shan-Shan, Kai-Wen Zhang, Bo-Wen Chen, Chun Yang, Rong Xiao, Peng-Gao Li, and Ming-Wei Zhu. 2023. "Machine Learning-Based Prediction of Complications and Prolonged Hospitalization with the GLIM Criteria Combinations Containing Calf Circumference in Elderly Asian Patients" Nutrients 15, no. 19: 4146. https://doi.org/10.3390/nu15194146
APA StyleRen, S.-S., Zhang, K.-W., Chen, B.-W., Yang, C., Xiao, R., Li, P.-G., & Zhu, M.-W. (2023). Machine Learning-Based Prediction of Complications and Prolonged Hospitalization with the GLIM Criteria Combinations Containing Calf Circumference in Elderly Asian Patients. Nutrients, 15(19), 4146. https://doi.org/10.3390/nu15194146