
Differences in Dietary Intake, Eating Occasion Timings and Eating Windows between Chronotypes in Adults Living with Type 2 Diabetes Mellitus
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chronotype
2.2. Dietary Assessment
2.3. Anthropometric, Demographic and Cardio-Metabolic Measures
2.4. Sleep Behaviours
2.5. Index of Multiple Deprivation
2.6. Statistical Analysis
3. Results
3.1. Chronotype
3.2. Dietary Intake
3.3. Caffeine Intake and Timing
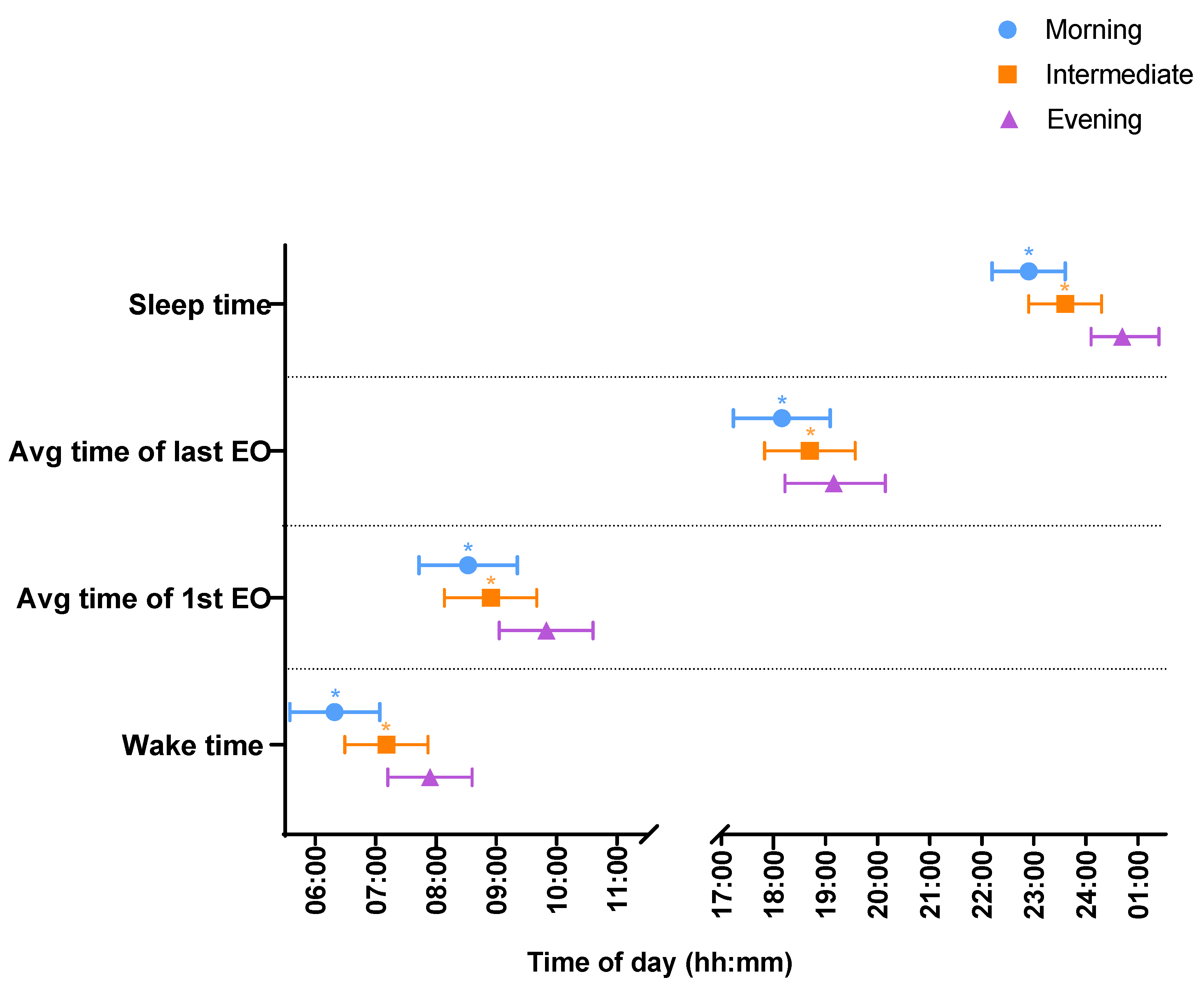
3.4. Wake Times and Sleep Onset
3.5. Eating Window and Timing of Eating Occasions
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flanagan, A.; Bechtold, D.A.; Pot, G.K.; Johnston, J.D. Chrono-Nutrition: From Molecular and Neuronal Mechanisms to Human Epidemiology and Timed Feeding Patterns. J. Neurochem. 2021, 157, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Tang, Q.; Chen, G.; Xie, M.; Yu, S.; Zhao, J.; Chen, L. New Insights into the Circadian Rhythm and Its Related Diseases. Front. Physiol. 2019, 10, 682. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse Metabolic and Cardiovascular Consequences of Circadian Misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef]
- Ruddick-Collins, L.C.; Johnston, J.D.; Morgan, P.J.; Johnstone, A.M. The Big Breakfast Study: Chrono-Nutrition Influence on Energy Expenditure and Bodyweight. Nutr. Bull. 2018, 43, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Challet, E. The Circadian Regulation of Food Intake. Nat. Rev. Endocrinol. 2019, 15, 393–405. [Google Scholar] [CrossRef]
- Adan, A.; Archer, S.N.; Hidalgo, M.P.; Di Milia, L.; Natale, V.; Randler, C. Circadian Typology: A Comprehensive Review. Chronobiol. Int. 2012, 29, 1153–1175. [Google Scholar] [CrossRef]
- van der Merwe, C.; Münch, M.; Kruger, R. Chronotype Differences in Body Composition, Dietary Intake and Eating Behavior Outcomes: A Scoping Systematic Review. Adv. Nutr. 2022, 13, 2357–2405. [Google Scholar] [CrossRef]
- Teixeira, G.P.; Guimarães, K.C.; Soares, A.G.N.S.; Marqueze, E.C.; Moreno, C.R.C.; Mota, M.C.; Crispim, C.A. Role of Chronotype in Dietary Intake, Meal Timing, and Obesity: A Systematic Review. Nutr. Rev. 2023, 81, 75–90. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and Nutritional Approaches for Prevention and Management of Type 2 Diabetes. BMJ 2018, 361, k2234. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.-M.; Knüppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Prospective Studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef]
- National Institute for Heath and Care Excellence (NICE). Type 2 Diabetes in Adults: Management. 2015. Available online: https://www.nice.org.uk/guidance/ng28 (accessed on 31 August 2023).
- Osonoi, Y.; Mita, T.; Osonoi, T.; Saito, M.; Tamasawa, A.; Nakayama, S.; Someya, Y.; Ishida, H.; Kanazawa, A.; Gosho, M.; et al. Morningness–Eveningness Questionnaire Score and Metabolic Parameters in Patients with Type 2 Diabetes Mellitus. Chronobiol. Int. 2014, 31, 1017–1023. [Google Scholar] [CrossRef]
- Iwasaki, M.; Hirose, T.; Mita, T.; Sato, F.; Ito, C.; Yamamoto, R.; Someya, Y.; Yoshihara, T.; Tamura, Y.; Kanazawa, A.; et al. Morningness–Eveningness Questionnaire Score Correlates with Glycated Hemoglobin in Middle-aged Male Workers with Type 2 Diabetes Mellitus. J. Diabetes Investig. 2013, 4, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Kalsbeek, A.; la Fleur, S.; Fliers, E. Circadian Control of Glucose Metabolism. Mol. Metab. 2014, 3, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.K.W.; Huggins, C.E.; Bonham, M.P. Effect of Meal Timing on Postprandial Glucose Responses to a Low Glycemic Index Meal: A Crossover Trial in Healthy Volunteers. Clin. Nutr. Edinb. Scotl. 2019, 38, 465–471. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Qian, J.; Vujovic, N.; Morris, C.J.; Nedeltcheva, A.; Nguyen, H.; Rahman, N.; Heng, S.W.; Kelly, L.; Kerlin-Monteiro, K.; et al. Daytime Eating Prevents Internal Circadian Misalignment and Glucose Intolerance in Night Work. Sci. Adv. 2021, 7, eabg9910. [Google Scholar] [CrossRef]
- Popp, C.J.; Curran, M.; Wang, C.; Prasad, M.; Fine, K.; Gee, A.; Nair, N.; Perdomo, K.; Chen, S.; Hu, L.; et al. Temporal Eating Patterns and Eating Windows among Adults with Overweight or Obesity. Nutrients 2021, 13, 4485. [Google Scholar] [CrossRef] [PubMed]
- Che, T.; Yan, C.; Tian, D.; Zhang, X.; Liu, X.; Wu, Z. Time-Restricted Feeding Improves Blood Glucose and Insulin Sensitivity in Overweight Patients with Type 2 Diabetes: A Randomised Controlled Trial. Nutr. Metab. 2021, 18, 88. [Google Scholar] [CrossRef]
- Moon, S.; Kang, J.; Kim, S.H.; Chung, H.S.; Kim, Y.J.; Yu, J.M.; Cho, S.T.; Oh, C.-M.; Kim, T. Beneficial Effects of Time-Restricted Eating on Metabolic Diseases: A Systemic Review and Meta-Analysis. Nutrients 2020, 12, 1267. [Google Scholar] [CrossRef]
- Pellegrini, M.; Cioffi, I.; Evangelista, A.; Ponzo, V.; Goitre, I.; Ciccone, G.; Ghigo, E.; Bo, S. Effects of Time-Restricted Feeding on Body Weight and Metabolism. A Systematic Review and Meta-Analysis. Rev. Endocr. Metab. Disord. 2020, 21, 17–33. [Google Scholar] [CrossRef]
- Galindo Muñoz, J.S.; Gómez Gallego, M.; Díaz Soler, I.; Barberá Ortega, M.C.; Martínez Cáceres, C.M.; Hernández Morante, J.J. Effect of a Chronotype-Adjusted Diet on Weight Loss Effectiveness: A Randomized Clinical Trial. Clin. Nutr. Edinb. Scotl. 2020, 39, 1041–1048. [Google Scholar] [CrossRef]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L. The Relationship Between Breakfast Skipping, Chronotype, and Glycemic Control in Type 2 Diabetes. Chronobiol. Int. 2014, 31, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Nimitphong, H.; Siwasaranond, N.; Saetung, S.; Thakkinstian, A.; Ongphiphadhanakul, B.; Reutrakul, S. The Relationship among Breakfast Time, Morningness–Eveningness Preference and Body Mass Index in Type 2 Diabetes. Diabet. Med. 2018, 35, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L.; Van Cauter, E. Chronotype Is Independently Associated With Glycemic Control in Type 2 Diabetes. Diabetes Care 2013, 36, 2523–2529. [Google Scholar] [CrossRef]
- Brady, E.M.; Hall, A.P.; Baldry, E.; Chatterjee, S.; Daniels, L.J.; Edwardson, C.; Khunti, K.; Patel, M.I.; Henson, J.J.; Rowlands, A.; et al. Rationale and Design of a Cross-Sectional Study to Investigate and Describe the Chronotype of Patients with Type 2 Diabetes and the Effect on Glycaemic Control: The CODEC Study. BMJ Open 2019, 9, e027773. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A Self-Assessment Questionnaire to Determine Morningness-Eveningness in Human Circadian Rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Taillard, J.; Philip, P.; Chastang, J.-F.; Bioulac, B. Validation of Horne and Ostberg Morningness-Eveningness Questionnaire in a Middle-Aged Population of French Workers. J. Biol. Rhythms 2004, 19, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Gibney, M.J.; Wolever, T.M.S. Periodicity of Eating and Human Health: Present Perspective and Future Directions. Br. J. Nutr. 1997, 77 (Suppl. S1), S3–S5. [Google Scholar] [CrossRef]
- Migueles, J.H.; Rowlands, A.V.; Huber, F.; Sabia, S.; Hees, V.T. van. GGIR: A Research Community–Driven Open Source R Package for Generating Physical Activity and Sleep Outcomes From Multi-Day Raw Accelerometer Data. J. Meas. Phys. Behav. 2019, 2, 188–196. [Google Scholar] [CrossRef]
- van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, Open Access Method to Assess Sleep Duration Using a Wrist-Worn Accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef]
- Fitt, E.; Pell, D.; Cole, D. Assessing Caffeine Intake in the United Kingdom Diet. Food Chem. 2013, 140, 421–426. [Google Scholar] [CrossRef]
- Lucassen, E.A.; Zhao, X.; Rother, K.I.; Mattingly, M.S.; Courville, A.B.; de Jonge, L.; Csako, G.; Cizza, G. Evening Chronotype Is Associated with Changes in Eating Behavior, More Sleep Apnea, and Increased Stress Hormones in Short Sleeping Obese Individuals. PLoS ONE 2013, 8, e56519. [Google Scholar] [CrossRef] [PubMed]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Kronholm, E.; Konttinen, H.; Wennman, H.; Männistö, S. The Associations between Chronotype, a Healthy Diet and Obesity. Chronobiol. Int. 2016, 33, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, K.; Oustric, P.; Alkahtani, S.; Alhussain, M.; Pedersen, H.; Salling Quist, J.; Færch, K.; Finlayson, G. Impact of Meal Timing and Chronotype on Food Reward and Appetite Control in Young Adults. Nutrients 2020, 12, 1506. [Google Scholar] [CrossRef] [PubMed]
- Mota, M.C.; Waterhouse, J.; De-Souza, D.A.; Rossato, L.T.; Silva, C.M.; Araújo, M.B.J.; Tufik, S.; de Mello, M.T.; Crispim, C.A. Association between Chronotype, Food Intake and Physical Activity in Medical Residents. Chronobiol. Int. 2016, 33, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, T.; Komatsu, T.; Tada, Y.; Hida, A.; Kawano, Y.; Togo, F. Association of Habitual Dietary Intake with Morningness-Eveningness and Rotating Shift Work in Japanese Female Nurses. Chronobiol. Int. 2018, 35, 1–13. [Google Scholar] [CrossRef]
- Baron, K.G.; Reid, K.J.; Horn, L.V.; Zee, P.C. Contribution of Evening Macronutrient Intake to Total Caloric Intake and Body Mass Index. Appetite 2013, 60, 246–251. [Google Scholar] [CrossRef]
- Vera, B.; Dashti, H.S.; Gómez-Abellán, P.; Hernández-Martínez, A.M.; Esteban, A.; Scheer, F.A.J.L.; Saxena, R.; Garaulet, M. Modifiable Lifestyle Behaviors, but Not a Genetic Risk Score, Associate with Metabolic Syndrome in Evening Chronotypes. Sci. Rep. 2018, 8, 945. [Google Scholar] [CrossRef]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Kronholm, E.; Tapanainen, H.; Kontto, J.; Männistö, S. Chronotype Differences in Timing of Energy and Macronutrient Intakes: A Population-Based Study in Adults. Obesity 2017, 25, 608–615. [Google Scholar] [CrossRef]
- Teixeira, G.P.; Mota, M.C.; Crispim, C.A. Eveningness Is Associated with Skipping Breakfast and Poor Nutritional Intake in Brazilian Undergraduate Students. Chronobiol. Int. 2018, 35, 358–367. [Google Scholar] [CrossRef]
- Sato-Mito, N.; Sasaki, S.; Murakami, K.; Okubo, H.; Takahashi, Y.; Shibata, S.; Yamada, K.; Sato, K. The Midpoint of Sleep Is Associated with Dietary Intake and Dietary Behavior among Young Japanese Women. Sleep Med. 2011, 12, 289–294. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Safety of Caffeine. EFSA J. 2015, 13, 4102. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiong, Y.; Dong, J.; Guo, T.; Tang, X.; Zhao, Y. Caffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index among Medical Students in Chongqing, China: A Multiple Mediation Model. Int. J. Environ. Res. Public. Health 2018, 15, 1721. [Google Scholar] [CrossRef] [PubMed]
- Bodur, M.; Baspinar, B.; Özçelik, A.Ö. Do Sleep Quality and Caffeine Consumption Mediate the Relationship between Late Chronotype and Body Mass Index? Food Funct. 2021, 12, 5959–5966. [Google Scholar] [CrossRef] [PubMed]
- Penolazzi, B.; Natale, V.; Leone, L.; Russo, P.M. Individual Differences Affecting Caffeine Intake. Analysis of Consumption Behaviours for Different Times of Day and Caffeine Sources. Appetite 2012, 58, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Tsitsou, S.; Zacharodimos, N.; Poulia, K.-A.; Karatzi, K.; Dimitriadis, G.; Papakonstantinou, E. Effects of Time-Restricted Feeding and Ramadan Fasting on Body Weight, Body Composition, Glucose Responses, and Insulin Resistance: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 4778. [Google Scholar] [CrossRef] [PubMed]
- Gontijo, C.A.; Cabral, B.B.M.; Balieiro, L.C.T.; Teixeira, G.P.; Fahmy, W.M.; de Paiva Maia, Y.C.; Crispim, C.A. Time-Related Eating Patterns and Chronotype Are Associated with Diet Quality in Pregnant Women. Chronobiol. Int. 2019, 36, 75–84. [Google Scholar] [CrossRef]
- Xiao, Q.; Garaulet, M.; Scheer, F.A.J.L. Meal Timing and Obesity: Interactions with Macronutrient Intake and Chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef]
- Chamorro, R.; Basfi-fer, K.; Sepúlveda, B.; Farías, R.; Rojas, P.; Carrasco, F.; Codoceo, J.; Inostroza, J.; Ruz, M. Meal Timing across the Day Modulates Daily Energy Intake in Adult Patients with Type 2 Diabetes. Eur. J. Clin. Nutr. 2022, 76, 1470–1477. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 411) | Morning (n = 131) (32.3 %) | Intermediate (n = 195) (48%) | Evening (n = 80) (19.7%) | |
|---|---|---|---|---|
| Demographic variables | ||||
| Age (years) (mean ± SD) | 65.2 ± 7.6 | 64.8 ± 7.8 | 66.3 ± 6.8 | 62.9 ± 9.0 |
| Sex (%female) | 136 (33) | 47 (35.6) | 56 (28.7) | 32 (40) |
| Current smokers (n%) | 18 (4.4) | 5 (3.8) | 9 (4.6) | 4 (5.0) |
| IMD | 19,877.6 ± 8942 | 20,919.3 ± 8415.9 | 19,944.3 ± 8704.2 | 18,014.6 ± 10,229 |
| Ethnicity (%) | ||||
| White European | 380 (92.2) | 126 (95.5) | 178 (91.3) | 72 (90) |
| South Asian | 16 (3.9) | 2 (1.5) | 10 (5.1) | 4 (5.0) |
| Black | 7 (1.7) | 2 (1.5) | 4 (2.0) | 1 (1.3) |
| Other | 9 (2.2) | 2 (1.5) | 3 (1.5) | 3 (3.8) |
| Employment (%) | ||||
| Employed | 115 (27.8) | 52 (39.4) | 44 (22.6) | 18 (22.5) |
| Retired | 269 (65.2) | 76 (57.6) | 139 (71.3) | 50 (62.5) |
| Unemployed | 16 (3.8) | 1 (0.8) | 5 (2.6) | 10 (12.5) |
| Other | 12 (2.9) | 3 (2.3) | 7 (3.6) | 2 (2.6) |
| Number of T2DM medications | 1.3 ± 0.9 | 1.1 ± 0.9 | 1.4 ± 1.0 | 1.3 ± 0.9 |
| Anthropometric variables | ||||
| BMI (kg/m2) | 30.6 ± 5.2 | 30.6 ± 4.9 | 30.5 ± 5.1 | 30.9 ± 5.6 |
| Cardio-metabolic variables | ||||
| HbA1c (%) | 6.9 ± 1.3 | 6.7 ± 1.2 | 6.9 ± 1.2 | 7.0 ± 1.4 |
| HbA1c (mmol/mol) | 51.9 ± 14.2 | 49.7 ± 13.2 | 51.9 ± 13.2 | 53.0 ± 15.3 |
| Duration of T2DM (years) | 10.9 ± 7.4 | 9.7 ± 6.3 | 11.3 ± 7.6 | 11.9 ± 8.0 |
| Variable | Morning | Intermediate | Evening | Main Effect for Chronotype |
|---|---|---|---|---|
| Energy intake (kcal/d) | 1530 (1246.0 to 1814.1) | 1544.6 (1277.7 to 1811.5) | 1504.5 (1233.2 to 1775.8) | 0.428 |
| Energy intake (kcal/kg) | 22.7 (18.8 to 26.6) | 22.3 (18.6 to 25.9) | 21.3 (17.6 to 25.1) | 0.257 |
| Carbohydrates (g/day) | 189.4 (155.9 to 223.0) | 194.5 (163.3 to 226.3) | 184.5 (152.4 to 216.5) | 0.547 |
| Fat (g/d) | 57.9 (42.8 to 72.9) | 56.2 (42.1 to 70.3) | 57.4 (43.1 to 71.8) | 0.507 |
| Protein (g/d) | 62.6 (48.5 to 76.7) | 63.7 (50.4 to 77.0) | 64.5 (51.0 to 77.9) | 0.564 |
| Caffeine (mg) | 62.3 (16.5 to 108.1) * | 78.1 (35.1 to 121.2) | 99.1 (55.4 to 142.9) | 0.048 |
| Timing of first EO (hrs:min) | 08:32 (07:47 to 09:21) * | 08:54 (08:08 to 09:40) * | 09:49 (09:03 to 10:36) | <0.001 |
| Timing of last EO (hrs:min) | 18:09 (17:14 to 19:05) * | 18:42 (17:50 to 19:34) * | 19:16 (18:22 to 20:09) | <0.001 |
| EW (hrs:min) | 09:35 (8:26 to 10:45) | 09:46 (08:40 to 10:51) | 09:21 (08:15 to 10:28) | 0.595 |
| Timing of first caffeine intake | 10:31 (08:41 to 12:20) | 11:13 (09:31 to 12:55) | 11:19 (09:35 to 13:03) | 0.297 |
| Timing of last caffeine intake | 12:33 (10:18 to 14:47) * | 13:26 (11:20 to 15:33) | 14:21 (12:13 to 16:29) | 0.037 |
| Time duration between waking and first EO (hrs:min) | 02:11 (01:25 to 02:56) | 01:58 (01:16 to 02:40) | 01:53 (01:10 to 02:37) | 0.570 |
| Time duration between last EO and sleep onset (hrs:min) | 04:50 (03:48 to 05:51) | 04:53 (03:56 to 05:51) | 05:21 (04:22 to 06:19) | 0.309 |
| Time duration between waking and first caffeine intake | 04:10 (02:18 to 06:03) | 04:05 (02:21 to 05:49) | 03:22 (01:35 to 05:08) | 0.284 |
| Time duration between last caffeine intake and sleep onset | 10:40 (08:24 to 12:55) | 10:15 (08:09 to 12:21) | 10:29 (08:21 to 12:38) | 0.899 |
| Wake time (hrs:min) | 06:19 (05:35 to 07:04) * | 07:11 (06:29 to 07:52) * | 07:56 (07:13 to 08:38) | <0.001 |
| Sleep onset (hrs:min) | 22:58 (22:16 to 23:40) * | 23:38 (22:59 to 00:18) * | 00:46 (00:06 to 01:26) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsarova, S.S.; Redman, E.; Arsenyadis, F.; Brady, E.M.; Rowlands, A.V.; Edwardson, C.L.; Goff, L.M.; Khunti, K.; Yates, T.; Hall, A.P.; et al. Differences in Dietary Intake, Eating Occasion Timings and Eating Windows between Chronotypes in Adults Living with Type 2 Diabetes Mellitus. Nutrients 2023, 15, 3868. https://doi.org/10.3390/nu15183868
Katsarova SS, Redman E, Arsenyadis F, Brady EM, Rowlands AV, Edwardson CL, Goff LM, Khunti K, Yates T, Hall AP, et al. Differences in Dietary Intake, Eating Occasion Timings and Eating Windows between Chronotypes in Adults Living with Type 2 Diabetes Mellitus. Nutrients. 2023; 15(18):3868. https://doi.org/10.3390/nu15183868
Chicago/Turabian StyleKatsarova, Stanislava S., Emma Redman, Franciskos Arsenyadis, Emer M. Brady, Alex V. Rowlands, Charlotte L. Edwardson, Louise M. Goff, Kamlesh Khunti, Thomas Yates, Andrew P. Hall, and et al. 2023. "Differences in Dietary Intake, Eating Occasion Timings and Eating Windows between Chronotypes in Adults Living with Type 2 Diabetes Mellitus" Nutrients 15, no. 18: 3868. https://doi.org/10.3390/nu15183868
APA StyleKatsarova, S. S., Redman, E., Arsenyadis, F., Brady, E. M., Rowlands, A. V., Edwardson, C. L., Goff, L. M., Khunti, K., Yates, T., Hall, A. P., Davies, M. J., & Henson, J. (2023). Differences in Dietary Intake, Eating Occasion Timings and Eating Windows between Chronotypes in Adults Living with Type 2 Diabetes Mellitus. Nutrients, 15(18), 3868. https://doi.org/10.3390/nu15183868