

Evaluation of Dietary Intake in Individuals with Mild Cognitive Impairment

Abstract
:1. Introduction
2. Materials and Methods
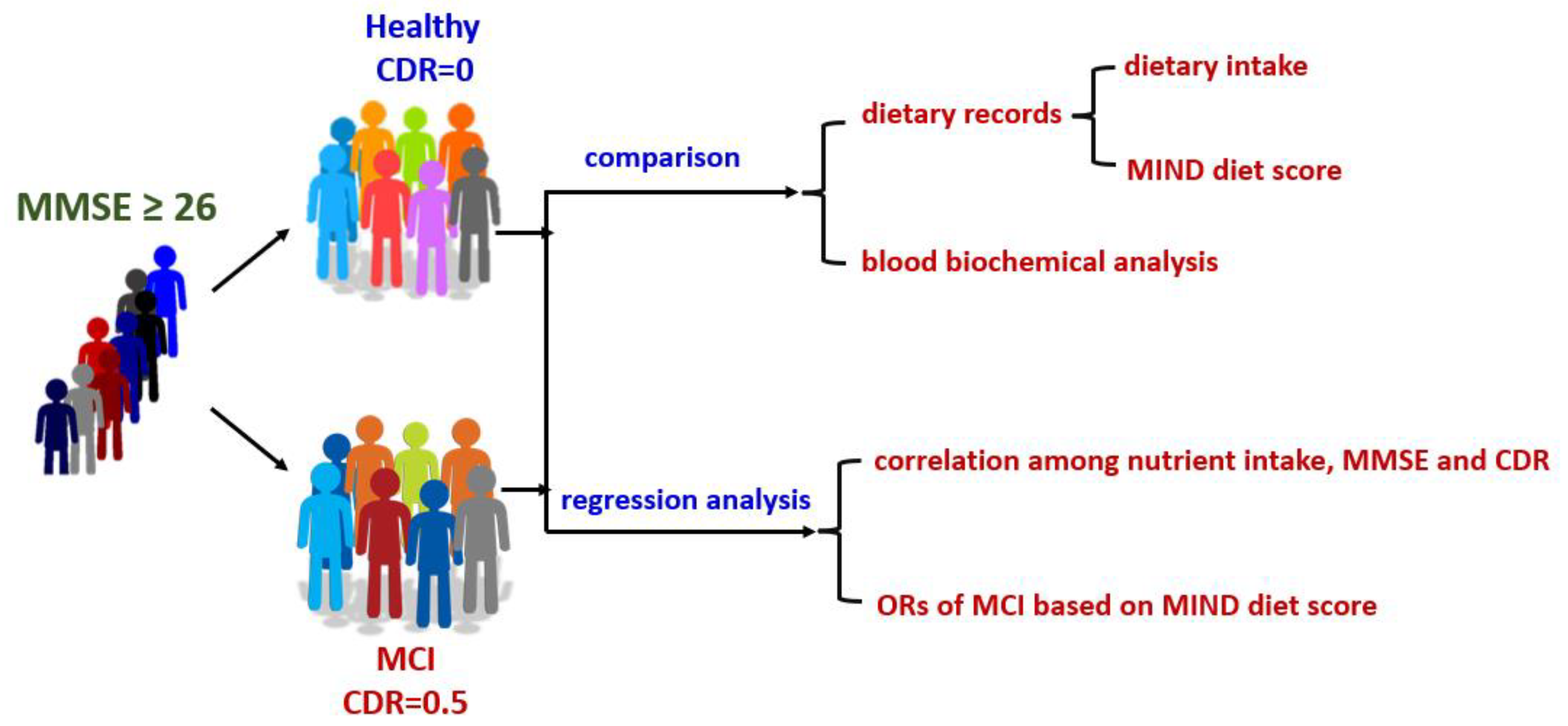
2.1. Study Design and Participants
2.2. Data Collection of Dietary Intake
2.3. Measurement Items
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Nutrient Intake
3.3. Dietary Intake
3.4. MIND Diet Score
3.5. Regression Analysis
3.5.1. Nutrient Intake and Cognitive Function
3.5.2. Dietary Intake and Cognitive Function
3.5.3. MIND Diet Score and Cognitive Function
3.6. Blood Biochemical Parameters
4. Discussion
4.1. Basic Characteristics of Participants
4.2. Nutrients and Cognitive Impairment
4.3. Food Categories and Cognitive Function
4.4. MIND Diet and Cognitive Function
4.5. Body Composition and Blood Biochemical Parameters
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet. Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Dementia Association. Understanding Dementia-Dementia in Taiwan. Available online: http://tada2002.ehosting.com.tw/eng/dementia.html (accessed on 11 April 2023).
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Overman, A.; Chuang, C.C.; McIntosh, M. Quercetin attenuates inflammation in human macrophages and adipocytes exposed to macrophage-conditioned media. Int. J. Obes. 2011, 35, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Jiang, H.; Wu, X.; Fang, J. Therapeutic Effects of Quercetin on Inflammation, Obesity, and Type 2 Diabetes. Mediat. Inflamm. 2016, 2016, 9340637. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND diet slows cognitive decline with aging. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2015, 11, 1015–1022. [Google Scholar] [CrossRef]
- Berendsen, A.A.M.; Kang, J.H.; van de Rest, O.; Feskens, E.J.M.; de Groot, L.; Grodstein, F. The Dietary Approaches to Stop Hypertension Diet, Cognitive Function, and Cognitive Decline in American Older Women. J. Am. Med. Dir. Assoc. 2017, 18, 427–432. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2015, 11, 1007–1014. [Google Scholar] [CrossRef]
- Berendsen, A.M.; Kang, J.H.; Feskens, E.J.M.; de Groot, C.; Grodstein, F.; van de Rest, O. Association of Long-Term Adherence to the MIND Diet with Cognitive Function and Cognitive Decline in American Women. J. Nutr. Health Aging 2018, 22, 222–229. [Google Scholar] [CrossRef]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease-A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef]
- Luciano, M.; Corley, J.; Cox, S.R.; Valdés Hernández, M.C.; Craig, L.C.; Dickie, D.A.; Karama, S.; McNeill, G.M.; Bastin, M.E.; Wardlaw, J.M.; et al. Mediterranean-type diet and brain structural change from 73 to 76 years in a Scottish cohort. Neurology 2017, 88, 449–455. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; Mchugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Ernesto, C.; Schafer, K.; Coats, M.; Leon, S.; Sano, M.; Thal, L.J.; Woodbury, P. Clinical Dementia Rating training and reliability in multicenter studies. Am. Acad. Neurol. 1997, 48, 1508. [Google Scholar] [CrossRef]
- Lin, I.H.; Duong, T.V.; Nien, S.W.; Tseng, I.H.; Wang, H.H.; Chiang, Y.J.; Chen, C.Y.; Wong, T.C. Dietary Diversity Score: Implications for Obesity Prevention and Nutrient Adequacy in Renal Transplant Recipients. Int. J. Environ. Res. Public Health 2020, 17, 5083. [Google Scholar] [CrossRef]
- Taiwan Food and Drug Administration; Ministry of Health and Welfare, Taiwan. Taiwanese Food Composition and Nutrient Database. 2017. Available online: https://consumer.fda.gov.tw/Food/TFND.aspx?nodeID=178 (accessed on 7 December 2018).
- Aronow, W.S. Hypertension and cognitive impairment. Ann. Transl. Med. 2017, 5, 259. [Google Scholar] [CrossRef]
- Longstreth, W.T., Jr.; Manolio, T.A.; Arnold, A.; Burke, G.L.; Bryan, N.; Jungreis, C.A.; Enright, P.L.; O’Leary, D.; Fried, L. Clinical correlates of white matter findings on cranial magnetic resonance imaging of 3301 elderly people. The Cardiovascular Health Study. Stroke 1996, 27, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Liao, D.; Cooper, L.; Cai, J.; Toole, J.F.; Bryan, N.R.; Hutchinson, R.G.; Tyroler, H.A. Presence and severity of cerebral white matter lesions and hypertension, its treatment, and its control. The ARIC Study. Atherosclerosis Risk in Communities Study. Stroke 1996, 27, 2262–2270. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Mayeux, R. Dietary factors and Alzheimer’s disease. Lancet. Neurol. 2004, 3, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Zou, L.; Kong, Z.; Yang, L. Cognitive Impact of Calorie Restriction: A Narrative Review. J. Am. Med. Dir. Assoc. 2020, 21, 1394–1401. [Google Scholar] [CrossRef]
- Berrino, F. Western diet and Alzheimer’s disease. Epidemiol. E Prev. 2002, 26, 107–115. [Google Scholar]
- Roberts, R.O.; Roberts, L.A.; Geda, Y.E.; Cha, R.H.; Pankratz, V.S.; O’Connor, H.M.; Knopman, D.S.; Petersen, R.C. Relative intake of macronutrients impacts risk of mild cognitive impairment or dementia. J. Alzheimer’s Dis. JAD 2012, 32, 329–339. [Google Scholar] [CrossRef]
- Hernanz, A.; De la Fuente, M.; Navarro, M.; Frank, A. Plasma aminothiol compounds, but not serum tumor necrosis factor receptor II and soluble receptor for advanced glycation end products, are related to the cognitive impairment in Alzheimer’s disease and mild cognitive impairment patients. Neuroimmunomodulation 2007, 14, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.P.; Zhu, X.; Perry, G.; Smith, M.A. Oxidative stress in diabetes and Alzheimer’s disease. J. Alzheimer’s Dis. JAD 2009, 16, 763–774. [Google Scholar] [CrossRef]
- Phillips, P. Omega 3 fatty acids for the treatment of dementia: A Cochrane review summary. Int. J. Nurs. Stud. 2017, 67, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Kang, S.A.; Lee, H.O.; Lee, B.H.; Park, J.S.; Kim, J.H.; Jung, I.K.; Park, Y.J.; Lee, J.E. Relationships between dietary intake and cognitive function level in Korean elderly people. Public Health 2001, 115, 133–138. [Google Scholar] [CrossRef]
- van der Zwaluw, N.L.; van de Rest, O.; Tieland, M.; Adam, J.J.; Hiddink, G.J.; van Loon, L.J.; de Groot, L.C. The impact of protein supplementation on cognitive performance in frail elderly. Eur. J. Nutr. 2014, 53, 803–812. [Google Scholar] [CrossRef]
- Morris, M.C. The role of nutrition in Alzheimer’s disease: Epidemiological evidence. Eur. J. Neurol. 2009, 16 (Suppl. S1), 1–7. [Google Scholar] [CrossRef]
- Bolling, B.W.; Chen, C.Y.; McKay, D.L.; Blumberg, J.B. Tree nut phytochemicals: Composition, antioxidant capacity, bioactivity, impact factors. A systematic review of almonds, Brazils, cashews, hazelnuts, macadamias, pecans, pine nuts, pistachios and walnuts. Nutr. Res. Rev. 2011, 24, 244–275. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Duarte, G.B.S.; Reis, B.Z.; Cozzolino, S.M.F. Brazil nuts: Nutritional composition, health benefits and safety aspects. Food Res. Int. 2017, 100, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Benefits of Nut Consumption on Insulin Resistance and Cardiovascular Risk Factors: Multiple Potential Mechanisms of Actions. Nutrients 2017, 9, 1271. [Google Scholar] [CrossRef]
- Wang, X.; Hjorth, E.; Vedin, I.; Eriksdotter, M.; Freund-Levi, Y.; Wahlund, L.O.; Cederholm, T.; Palmblad, J.; Schultzberg, M. Effects of n-3 FA supplementation on the release of proresolving lipid mediators by blood mononuclear cells: The OmegAD study. J. Lipid Res. 2015, 56, 674–681. [Google Scholar] [CrossRef]
- Agarwal, P.; Wang, Y.; Buchman, A.S.; Holland, T.M.; Bennett, D.A.; Morris, M.C. MIND Diet Associated with Reduced Incidence and Delayed Progression of ParkinsonismA in Old Age. J. Nutr. Health Aging 2018, 22, 1211–1215. [Google Scholar] [CrossRef]
- Narayan, S.K.; Saxby, B.K.; Firbank, M.J.; O’Brien, J.T.; Harrington, F.; McKeith, I.G.; Hansrani, M.; Stansby, G.; Ford, G.A. Plasma homocysteine and cognitive decline in older hypertensive subjects. Int. Psychogeriatr. 2011, 23, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.; Nelson, V.A.; Davila, H.; Ratner, E.; Fink, H.A.; Hemmy, L.S.; McCarten, J.R.; Barclay, T.R.; Brasure, M.; Kane, R.L. Over-the-Counter Supplement Interventions to Prevent Cognitive Decline, Mild Cognitive Impairment, and Clinical Alzheimer-Type Dementia: A Systematic Review. Ann. Intern. Med. 2018, 168, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Kwok, T.; Wu, Y.; Lee, J.; Lee, R.; Yung, C.Y.; Choi, G.; Lee, V.; Harrison, J.; Lam, L.; Mok, V. A randomized placebo-controlled trial of using B vitamins to prevent cognitive decline in older mild cognitive impairment patients. Clin. Nutr. 2020, 39, 2399–2405. [Google Scholar] [CrossRef]
- Li, S.; Sun, W.; Zhang, D. Association of Zinc, Iron, Copper, and Selenium Intakes with Low Cognitive Performance in Older Adults: A Cross-Sectional Study from National Health and Nutrition Examination Survey (NHANES). J. Alzheimer’s Dis. JAD 2019, 72, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Odai, T.; Terauchi, M.; Suzuki, R.; Kato, K.; Hirose, A.; Miyasaka, N. Severity of subjective forgetfulness is associated with high dietary intake of copper in Japanese senior women: A cross-sectional study. Food Sci. Nutr. 2020, 8, 4422–4431. [Google Scholar] [CrossRef]
- Safer, U.; Safer, V.B.; Demir, S.O.; Yanikoglu, I. Effects of Bisphosphonates and Calcium plus Vitamin-D Supplements on Cognitive Function in Postmenopausal Osteoporosis§. Endocr. Metab. Immune Disord. Drug Targets 2016, 16, 56–60. [Google Scholar] [CrossRef]
- Zhang, H.; Hardie, L.; Bawajeeh, A.O.; Cade, J. Meat Consumption, Cognitive Function and Disorders: A Systematic Review with Narrative Synthesis and Meta-Analysis. Nutrients 2020, 12, 1528. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, J.; Qiu, J.; Li, Y.; Wang, J.; Jiao, J. Intakes of fish and polyunsaturated fatty acids and mild-to-severe cognitive impairment risks: A dose-response meta-analysis of 21 cohort studies. Am. J. Clin. Nutr. 2016, 103, 330–340. [Google Scholar] [CrossRef]
- Jiang, Y.W.; Sheng, L.T.; Pan, X.F.; Feng, L.; Yuan, J.M.; Pan, A.; Koh, W.P. Meat consumption in midlife and risk of cognitive impairment in old age: The Singapore Chinese Health Study. Eur. J. Nutr. 2020, 59, 1729–1738. [Google Scholar] [CrossRef]
- Pastor-Valero, M.; Furlan-Viebig, R.; Menezes, P.R.; da Silva, S.A.; Vallada, H.; Scazufca, M. Education and WHO recommendations for fruit and vegetable intake are associated with better cognitive function in a disadvantaged Brazilian elderly population: A population-based cross-sectional study. PLoS ONE 2014, 9, e94042. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Fanelli-Kuczmarski, M.T.; Kitner-Triolo, M.H.; Beydoun, H.A.; Kaufman, J.S.; Mason, M.A.; Evans, M.K.; Zonderman, A.B. Dietary antioxidant intake and its association with cognitive function in an ethnically diverse sample of US adults. Psychosom. Med. 2015, 77, 68–82. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Xiao, R.; Cai, C.; Xu, Z.; Wang, S.; Pan, L.; Yuan, L. Diet, lifestyle and cognitive function in old Chinese adults. Arch. Gerontol. Geriatr. 2016, 63, 36–42. [Google Scholar] [CrossRef]
- Mottaghi, T.; Amirabdollahian, F.; Haghighatdoost, F. Fruit and vegetable intake and cognitive impairment: A systematic review and meta-analysis of observational studies. Eur. J. Clin. Nutr. 2018, 72, 1336–1344. [Google Scholar] [CrossRef]
- Hosking, D.E.; Eramudugolla, R.; Anstey, K.J. [P4–363]: The mind diet is associated with reduced incidence of 12-year cognitive impairment in an australian setting. Alzheimer’s Dement. 2017, 13, P1429–P1430. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, L.G.; Wu, Q.J.; Ma, X.; Xiang, Y.B. Association between dietary fiber and lower risk of all-cause mortality: A meta-analysis of cohort studies. Am. J. Epidemiol. 2015, 181, 83–91. [Google Scholar] [CrossRef]
- van de Rest, O.; Wang, Y.; Barnes, L.L.; Tangney, C.; Bennett, D.A.; Morris, M.C. APOE ε4 and the associations of seafood and long-chain omega-3 fatty acids with cognitive decline. Neurology 2016, 86, 2063–2070. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knüppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Malek Rivan, N.F.; Shahar, S.; Fakhruddin, N.N.I.N.M.; You, Y.X.; Che Din, N.; Rajikan, R. The effect of dietary patterns on mild cognitive impairment and dementia incidence among community-dwelling older adults. Front. Nutr. 2022, 9, 901750. [Google Scholar] [CrossRef]
- Wu, W.; Li, Y.; Wu, Y.; Zhang, Y.; Wang, Z.; Liu, X. Lutein suppresses inflammatory responses through Nrf2 activation and NF-κB inactivation in lipopolysaccharide-stimulated BV-2 microglia. Mol. Nutr. Food Res. 2015, 59, 1663–1673. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Rizzuto, D.; Larsson, S.C.; Faxén-Irving, G.; Fratiglioni, L.; Xu, W.L. The Nordic Prudent Diet Reduces Risk of Cognitive Decline in the Swedish Older Adults: A Population-Based Cohort Study. Nutrients 2018, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Suemoto, C.K.; Gilsanz, P.; Mayeda, E.R.; Glymour, M.M. Body mass index and cognitive function: The potential for reverse causation. Int. J. Obes. 2015, 39, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, Y.; Park, S.M. Body Mass Index and Decline of Cognitive Function. PLoS ONE 2016, 11, e0148908. [Google Scholar] [CrossRef] [PubMed]
- Lalithambika, C.V.; Arun, C.S.; Saraswathy, L.A.; Bhaskaran, R. Cognitive Impairment and its Association with Glycemic Control in Type 2 Diabetes Mellitus Patients. Indian J. Endocrinol. Metab. 2019, 23, 353–356. [Google Scholar] [CrossRef]
- Khullar, S.; Dhillon, H.; Kaur, G.; Sharma, R.; Mehta, K.; Aggarwal, R.; Singh, M.; Singh, P. The Prevalence and Predictors of Depression in Type 2 Diabetic Population of Punjab. Community Ment. Health J. 2016, 52, 479–483. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | All (n = 40) | Healthy (n = 19) | MCI (n = 21) | p |
|---|---|---|---|---|
| Age, years | 71.4 ± 6.6 | 72.4 ± 7.0 | 70.5 ± 6.3 | 0.42 |
| Male, n (%) | 15 (37.5%) | 6 (31.6%) | 9 (42.9%) | 0.48 |
| Female, n (%) | 25 (62.5%) | 13 (68.4%) | 12 (57.1%) | 0.48 |
| SBP, mmHg | 139.5 ± 19.3 | 137.9 ± 23.5 | 140.9 ± 15 | 0.61 |
| DBP, mmHg | 77.3 ± 12.7 | 78.9 ± 12.5 | 75.8 ± 13 | 0.47 |
| MMSE | 27.5 ± 1.7 | 27.7 ± 1.9 | 27.3 ± 1.5 | 0.32 |
| CDR | 0.3 ± 0.3 | 0.0 ± 0.0 | 0.5 ± 0.0 | <0.0001 * |
| Overweight, n (%) | 16 (40.0%) | 7 (36.8%) | 9 (42.9%) | 0.71 |
| Obesity, n (%) | 9 (22.5%) | 5 (26.3%) | 4 (19.0%) | 0.60 |
| DM, n (%) | 13 (32.5%) | 5 (26.3%) | 8 (38.1%) | 0.44 |
| HTN, n (%) | 21 (52.5%) | 11 (57.9%) | 10 (47.6%) | 0.53 |
| Hyperlipidemia, n (%) | 12 (30.0%) | 5 (26.3%) | 7 (33.3%) | 0.65 |
| Nutrients | Healthy (n = 19) | MCI (n = 21) | p |
|---|---|---|---|
| Energy, kcal | 1678.7 ± 305.2 | 1695.8 ± 278.3 | 0.72 |
| CHO, g | 188.6 ± 34.1 | 194.5 ± 33.4 | 0.59 |
| CHO, % | 45.4 ± 7.2 | 46.5 ± 6.3 | |
| Protein, g | 70.3 ± 16.4 | 70.1 ± 13.2 | 1.00 |
| Protein, % | 16.8 ± 2.6 | 16.5 ± 2.1 | |
| Fat, g | 72.5 ± 22.9 | 71.3 ± 22.0 | 0.72 |
| Fat, % | 38.3 ± 7.6 | 37.2 ± 7.1 | |
| MUFAs, g | 27.6 ± 9.8 | 28.1 ± 11.7 | 0.91 |
| MUFAs, % | 14.5 ± 3.2 | 14.9 ± 4.8 | |
| PUFAs, g | 23.0 ± 10.3 | 19.2 ± 8.2 | 0.18 |
| PUFAs, % | 12.2 ± 4.8 | 9.7 ± 2.7 | |
| n-3 FAs, g | 3.1 ± 1.6 | 2.2 ± 1.1 | 0.09 |
| n-6 FAs, g | 19.9 ± 9.3 | 17.0 ± 8.6 | 0.22 |
| SFAs, g | 19.6 ± 7.0 | 20.8 ± 6.8 | 0.61 |
| SFAs, % | 10.4 ± 2.7 | 10.8 ± 2.4 | |
| Cholesterol, mg | 249.6 ± 108.0 | 321.8 ± 138.3 | 0.10 |
| Fiber, g | 13.1 ± 6.8 | 14.2 ± 3.8 | 0.18 |
| Vitamin A, μg | 730.1 ± 343.8 | 962.4 ± 502.2 | 0.13 |
| Vitamin E, mg | 9.4 ± 7.1 | 18.9 ± 24.6 | 0.29 |
| Vitamin C, mg | 110.9 ± 64.2 | 110.8 ± 45.2 | 0.66 |
| Vitamin B1, mg | 1.1 ± 0.4 | 1.3 ± 0.6 | 0.37 |
| Vitamin B2, mg | 1.0 ± 0.3 | 1.0 ± 0.3 | 0.75 |
| Niacin, mg | 13.1 ± 3.7 | 14.2 ± 3.4 | 0.18 |
| Vitamin B6, mg | 1.5 ± 0.5 | 1.5 ± 0.4 | 0.63 |
| Vitamin B12, μg | 6.8 ± 10.3 | 3.0 ± 1.2 | 0.55 |
| Folic acid, μg | 250.6 ± 112.6 | 280.8 ± 82.5 | 0.18 |
| Sodium, mg | 1116.9 ± 935.0 | 832.3 ± 411.9 | 0.23 |
| Potassium, mg | 2151.6 ± 999.5 | 2089.0 ± 434.9 | 0.53 |
| Calcium, mg | 543.7 ± 415.5 | 508.5 ± 185.8 | 0.65 |
| Magnesium, mg | 261.9 ± 137.8 | 249.8 ± 63.5 | 0.42 |
| Phosphate, mg | 931.9 ± 280.1 | 927.5 ± 192.7 | 0.63 |
| Iron, mg | 11.1 ± 7.4 | 9.5 ± 2.3 | 0.68 |
| Zinc, mg | 9.7 ± 3.0 | 8.5 ± 2.2 | 0.30 |
| Copper, mg | 58.0 ± 42.8 | 106.9 ± 79.2 | 0.01 * |
| Alcohol, g | 0.0 ± 0.0 | 1.8 ± 4.6 | 0.10 |
| Food component | Health (n = 19) | MCI (n = 21) | p |
|---|---|---|---|
| Whole grains (servings) | 9.4 ± 2.1 | 9.7 ± 2.1 | 0.89 |
| Soybeans, fish, eggs, and low-fat meat (servings) | 2.8 ± 1.2 | 1.8 ± 1.1 | 0.03 * |
| Soybeans, fish, eggs, and medium-fat meat (servings) | 2.6 ± 1.3 | 3.3 ± 1.5 | 0.23 |
| Soybeans, fish, eggs, and high-fat meat (servings) | 0.1 ± 0.3 | 0.4 ± 0.6 | 0.18 |
| Soybeans, fish, eggs, and super high-fat meat (servings) | 0.6 ± 0.8 | 0.5 ± 0.6 | 0.70 |
| Vegetables (servings) | 1.1 ± 0.8 | 1.4 ± 1.0 | 0.51 |
| Fruit (servings) | 2.1 ± 1.0 | 2.6 ± 0.8 | 0.15 |
| Oils, fats, nuts, and seeds (servings) | 7.8 ± 3.6 | 6.5 ± 2.5 | 0.33 |
| Dairy products (low fat) (servings) | 0.1 ± 0.2 | 0.1 ± 0.2 | 0.84 |
| Dairy products (whole fat) (servings) | 0.3 ± 0.3 | 0.2 ± 0.3 | 0.61 |
| Healthy (n = 19) | MCI (n = 21) | p | |
|---|---|---|---|
| Green leafy vegetables score | 0.8 ± 0.3 | 0.8 ± 0.2 | 1.00 |
| Other vegetables score | 0.5 ± 0.5 | 0.6 ± 0.5 | 0.79 |
| Berries score | 0.0 ± 0.0 | 0.0 ± 0.0 | 1.00 |
| Nuts score | 0.4 ± 0.4 | 0.4 ± 0.4 | 1.00 |
| Olive oil score | 0.2 ± 0.4 | 0.4 ± 0.5 | 0.15 |
| Butter and margarine score | 1.0 ± 0.1 | 1.0 ± 0.0 | 0.32 |
| Cheese score | 0.9 ± 0.2 | 1.0 ± 0.2 | 0.32 |
| Whole grains score | 0.2 ± 0.3 | 0.5 ± 0.5 | 0.06 |
| Fish (not fried) score | 0.8 ± 0.4 | 0.9 ± 0.4 | 0.59 |
| Soybeans score | 0.7 ± 0.4 | 0.6 ± 0.5 | 0.78 |
| Poultry (not fried) score | 0.6 ± 0.5 | 0.6 ± 0.5 | 0.81 |
| Red meat and products score | 0.1 ± 0.3 | 0.2 ± 0.3 | 0.28 |
| Fast and fried foods score | 0.9 ± 0.2 | 0.9 ± 0.3 | 0.76 |
| Pastries and sweets score | 0.8 ± 0.4 | 0.7 ± 0.5 | 0.35 |
| Wine score | 0.0 ± 0.0 | 0.0 ± 0.2 | 0.37 |
| MIND diet score | 8.0 ± 1.5 | 8.6 ± 1.2 | 0.17 |
| MMSE | CDR | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| β | p | β | p | β | p | β | p | |
| Dietary intake levels | ||||||||
| Energy, kcal | <0.001 | 0.10 | −0.09 | 0.36 | <0.001 | 0.85 | −0.01 | 0.47 |
| CHO, g | 0.02 | 0.06 | 0.02 | 0.16 | <0.001 | 0.59 | 0.04 | 0.43 |
| Protein, g | 0.02 | 0.22 | 0.47 | 0.31 | <−0.001 | 0.96 | 0.03 | 0.63 |
| Fat, g | 0.01 | 0.41 | 0.39 | 0.67 | <−0.001 | 0.87 | 0.07 | 0.5 |
| MUFAs, g | 0.03 | 0.29 | 0.57 | 0.21 | <0.001 | 0.88 | 0.01 | 0.88 |
| PUFAs, g | <0.001 | 0.93 | −6.50 | 0.44 | −0.01 | 0.20 | −0.11 | 0.22 |
| n-3 PUFAs, g | −0.05 | 0.81 | 6.56 | 0.44 | −0.06 | 0.04 * | −0.01 | 0.64 |
| n-6 PUFAs, g | <0.001 | 0.88 | 6.87 | 0.43 | <−0.001 | 0.32 | 0.13 | 0.18 |
| SFAs, g | 0.03 | 0.51 | 0.30 | 0.40 | <0.001 | 0.60 | 0.02 | 0.5 |
| Cholesterol, mg | <0.001 | 0.18 | 0.01 | 0.59 | <0.001 | 0.08 | <0.001 | 0.42 |
| Fiber, g | 0.05 | 0.35 | 0.17 | 0.61 | <0.001 | 0.54 | 0.03 | 0.46 |
| Vitamins | ||||||||
| Vitamin A, RE | <0.001 | 0.02 * | <0.001 | 0.71 | <0.001 | 0.10 | <0.001 | 0.87 |
| Vitamin E, mg | 0.02 | 0.11 | 0.14 | 0.13 | <0.001 | 0.11 | −0.004 | 0.46 |
| Vitamin C, mg | 0.01 | 0.008 * | 0.01 | 0.07 | <−0.001 | 0.99 | −0.0009 | 0.68 |
| Vitamin B1, mg | 0.75 | 0.16 | 1.10 | 0.73 | 0.09 | 0.29 | 0.63 | 0.12 |
| Vitamin B2, mg | 1.64 | 0.06 | 0.71 | 0.58 | 0.05 | 0.73 | 0.26 | 0.71 |
| Niacin, mg | 0.08 | 0.31 | −0.01 | 0.95 | 0.01 | 0.31 | 0.05 | 0.08 |
| Vitamin B6, mg | 0.86 | 0.16 | 0.79 | 0.73 | −0.01 | 0.93 | −0.7 | 0.05 |
| Vitamin B12, μg | −0.01 | 0.82 | 0.01 | 0.98 | −0.01 | 0.09 | <0.001 | 0.88 |
| Folic acid, μg | <0.001 | 0.08 | −0.006 | 0.18 | <0.001 | 0.34 | −0.0007 | 0.71 |
| Minerals | ||||||||
| Sodium, mg | <0.001 | 0.56 | <0.001 | 0.65 | <−0.001 | 0.21 | −0.0001 | 0.82 |
| Potassium, mg | <0.001 | 0.10 | −0.004 | 0.25 | <−0.001 | 0.80 | <0.001 | 0.58 |
| Calcium, mg | <0.001 | 0.004 * | 0.002 | 0.04 * | <−0.001 | 0.73 | −0.0009 | 0.15 |
| Magnesium, mg | <0.001 | 0.17 | 0.02 | 0.58 | <−0.001 | 0.72 | −0.002 | 0.61 |
| Phosphate, mg | <0.001 | 0.48 | −0.01 | 0.54 | <−0.001 | 0.95 | <0.001 | 0.88 |
| Iron, mg | 0.07 | 0.16 | 0.12 | 0.77 | −0.01 | 0.35 | 0.04 | 0.49 |
| Zinc, mg | 0.12 | 0.23 | −0.51 | 0.44 | −0.02 | 0.18 | −0.04 | 0.54 |
| Copper, mg | <0.001 | 0.24 | −0.05 | 0.13 | <0.001 | 0.02 * | 0.002 | 0.02 * |
| Alcohol, equivalent | 0.04 | 0.59 | 0.27 | 0.31 | 0.02 | 0.10 | 0.05 | 0.17 |
| MMSE | CDR | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| β | p | β | p | β | p | β | p | |
| Food component | ||||||||
| Whole grains (ex) | 0.02 | 0.86 | 0.19 | 0.26 | 0.01 | 0.61 | −0.02 | 0.55 |
| Soybeans, fish, eggs, and meat (low fat) (ex) | −0.08 | 0.73 | −0.11 | 0.7 | −0.08 | 0.01 * | −0.07 | 0.03 * |
| Soybeans, fish, eggs, and meat (medium fat) (ex) | 0.12 | 0.52 | −0.01 | 0.96 | 0.04 | 0.15 | 0.05 | 0.17 |
| Soybeans, fish, eggs, and meat (high fat) (ex) | 0.07 | 0.90 | −0.16 | 0.83 | 0.14 | 0.12 | 0.15 | 0.16 |
| Soybeans, fish, eggs, and meat (super high fat) (ex) | −0.18 | 0.65 | −0.24 | 0.62 | −0.02 | 0.68 | 0.02 | 0.77 |
| Vegetables (ex) | 0.01 | 0.97 | 0.15 | 0.69 | 0.07 | 0.14 | 0.04 | 0.45 |
| Fruit (ex) | 0.76 | 0.01 * | 0.73 | 0.01 * | 0.04 | 0.33 | 0.03 | 0.59 |
| Oils, fats, nuts, and seeds (ex) | 0.09 | 0.30 | 0.15 | 0.18 | −0.02 | 0.21 | −0.03 | 0.06 |
| Dairy products (low fat) (ex) | −0.38 | 0.76 | 0.21 | 0.89 | 0.10 | 0.62 | 0.08 | 0.71 |
| Dairy products (whole fat) (ex) | 1.26 | 0.12 | 1.75 | 0.07 | −0.05 | 0.68 | 0.01 | 0.96 |
| Low-MIND Diet Score | High-MIND Diet Score | ||
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | p | |
| MCI | 1 (Reference) | 0.20 (0.04–0.99) | 0.04 * |
| All (n = 40) | Healthy (n = 19) | MCI (n = 21) | p | |
|---|---|---|---|---|
| BUN, mg/dL | 17.2 ± 6.7 | 17.0 ± 8.1 | 17.3 ± 5.3 | 0.46 |
| Serum Cr, mg/dL | 0.8 ± 0.3 | 0.8 ± 0.4 | 0.8 ± 0.3 | 0.69 |
| Albumin, mg/dL | 4.4 ± 0.3 | 4.4 ± 0.2 | 4.3 ± 0.4 | 1.00 |
| FPG, mg/dL | 104.6 ± 26.3 | 107.6 ± 34.2 | 102.1 ± 18.2 | 0.86 |
| HbA1c, % | 6.2 ± 0.9 | 6.4 ± 1.3 | 6.1 ± 0.6 | 0.89 |
| TC, mg/dL | 181.3 ± 34.9 | 177.4 ± 28.7 | 184.1 ± 39.3 | 0.72 |
| HDL-C, mg/dL | 54.9 ± 13.1 | 52.8 ± 12.9 | 56.5 ± 13.4 | 0.37 |
| LDL-C, mg/dL | 107.0 ± 30.7 | 104.7 ± 26.1 | 108.9 ± 34.7 | 0.88 |
| TGs, mg/dL | 104.6 ± 24.9 | 110.6 ± 30.2 | 100.4 ± 20.3 | 0.44 |
| Folate | 14.2 ± 8.0 | 13.0 ± 7.7 | 15.3 ± 8.3 | 0.33 |
| Vitamin B12 | 857.5 ± 438.8 | 743.1 ± 406.1 | 966.2 ± 451.0 | 0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nien, S.-W.; Lin, I.-H.; Wu, H.-C.; Chen, Y.-H.; Yang, S.-C. Evaluation of Dietary Intake in Individuals with Mild Cognitive Impairment. Nutrients 2023, 15, 3694. https://doi.org/10.3390/nu15173694
Nien S-W, Lin I-H, Wu H-C, Chen Y-H, Yang S-C. Evaluation of Dietary Intake in Individuals with Mild Cognitive Impairment. Nutrients. 2023; 15(17):3694. https://doi.org/10.3390/nu15173694
Chicago/Turabian StyleNien, Shih-Wei, I-Hsin Lin, Hsiu-Chuan Wu, Yi-Hsiu Chen, and Suh-Ching Yang. 2023. "Evaluation of Dietary Intake in Individuals with Mild Cognitive Impairment" Nutrients 15, no. 17: 3694. https://doi.org/10.3390/nu15173694
APA StyleNien, S.-W., Lin, I.-H., Wu, H.-C., Chen, Y.-H., & Yang, S.-C. (2023). Evaluation of Dietary Intake in Individuals with Mild Cognitive Impairment. Nutrients, 15(17), 3694. https://doi.org/10.3390/nu15173694