
Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence

 ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Methods
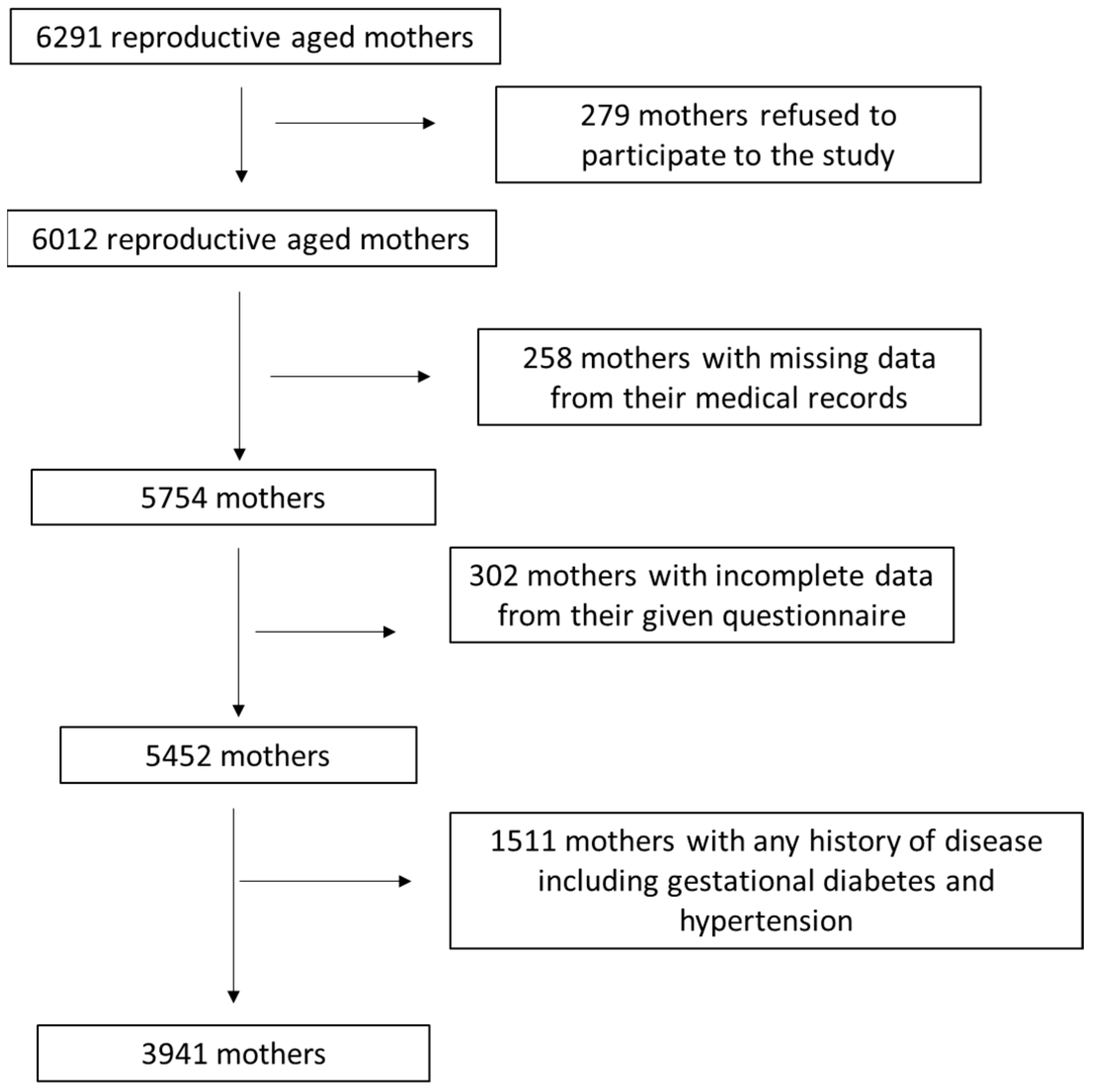
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Study Population
3.2. Associations of Postpartum Depression with Sociodemographic Parameters of the Study Population
3.3. Associations of Postpartum Depression with Anthropometric Parameters and Perinatal Outcomes of the Study Population
3.4. Multivariate Analysis for Postpartum Depression by Adjusting for Several Confounders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, L.J. Postpartum Depression. JAMA 2002, 287, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Front. Neuroendocr. 2019, 52, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Özcan, N.K.; Boyacıoğlu, N.E.; Dinç, H. Postpartum Depression Prevalence and Risk Factors in Turkey: A Systematic Review and Meta-Analysis. Arch. Psychiatr. Nurs. 2017, 31, 420–428. [Google Scholar] [CrossRef]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; Tam, W.W.S.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Li, W.; Xiong, J.; Zheng, X. Prevalence and Risk Factors Associated with Postpartum Depression during the COVID-19 Pandemic: A Literature Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2219. [Google Scholar] [CrossRef] [PubMed]
- Appiah, F.; Fenteng, J.O.D.; Dare, F.; Salihu, T.; Darteh, A.O.; Takyi, M.; Ayerakwah, P.A.; Ameyaw, E.K. Understanding the determinants of postnatal care uptake for babies: A mixed effects multilevel modelling of 2016–18 Papua New Guinea Demographic and Health Survey. BMC Pregnancy Childbirth 2021, 21, 841. [Google Scholar] [CrossRef]
- DelRosario, G.A.; Chang, A.C.; Lee, E.D. Postpartum depression: Symptoms, diagnosis, and treatment approaches. J. Am. Acad. Physician Assist. 2013, 26, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Pouyan, F.; Kamrani, M.A.; Rahimzadeh, M.; Jamshidimanesh, M.; Esmaelzadeh–Saeieh, S. Effect of Interpersonal Psychotherapy Oriented Child Birth Education on Stress and Role Adaption in Mothers with Premature Birth: A Randomized Clinical Trial. Iran. J. Psychiatry Behav. Sci. 2019, 13, e86645. [Google Scholar] [CrossRef]
- Dennis, C.-L.; Grigoriadis, S.; Zupancic, J.; Kiss, A.; Ravitz, P. Telephone-based nurse-delivered interpersonal psychotherapy for postpartum depression: Nationwide randomised controlled trial. Br. J. Psychiatry 2020, 216, 189–196. [Google Scholar] [CrossRef]
- Nusrat, H.; Zehra, N.; Amir, B.; Nasim, C.; Tayyeba, K.; Shehla, Z.; Batool, F.; Meher, H.; Farooq, N. Group interpersonal psychotherapy for maternal depression an exploratory randomized control trial. Eur. Psychiatry 2016, 33, S413–S414. [Google Scholar] [CrossRef]
- Cicchetti, D.; Toth, S.L.; Handley, E.D. Genetic moderation of interpersonal psychotherapy efficacy for low-income mothers with major depressive disorder: Implications for differential susceptibility. Dev. Psychopathol. 2015, 27, 19–35. [Google Scholar] [CrossRef]
- Wang, D.; Li, Y.-L.; Qiu, D.; Xiao, S.-Y. Factors Influencing Paternal Postpartum Depression: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 293, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Bernecker, S.L.; Constantino, M.J.; Pazzaglia, A.M.; Ravitz, P.; McBride, C. Patient Interpersonal and Cognitive Changes and Their Relation to Outcome in Interpersonal Psychotherapy for Depression. J. Clin. Psychol. 2014, 70, 518–527. [Google Scholar] [CrossRef]
- Liu, X.; Wang, S.; Wang, G. Prevalence and Risk Factors of Postpartum Depression in Women: A Systematic Review and Meta-analysis. J. Clin. Nurs. 2022, 31, 2665–2677. [Google Scholar] [CrossRef]
- Hakanen, H.; Flykt, M.; Sinervä, E.; Nolvi, S.; Kataja, E.L.; Pelto, J.; Karlsson, H.; Karlsson, L.; Korja, R. How maternal pre- and postnatal symptoms of depression and anxiety affect early mother-infant interaction? J. Affect. Disord. 2019, 257, 83–90. [Google Scholar] [CrossRef]
- Silva, C.S.; Lima, M.C.; Sequeira-De-Andrade, L.A.; Oliveira, J.S.; Monteiro, J.S.; Lima, N.M.; Santos, R.M.; Lira, P.I. Association between postpartum depression and the practice of exclusive breastfeeding in the first three months of life. J. Pediatr. 2017, 93, 356–364. [Google Scholar] [CrossRef]
- Farías-Antúnez, S.; Xavier, M.O.; Santos, I.S. Effect of maternal postpartum depression on offspring’s growth. J. Affect. Disord. 2018, 228, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of Persistent and Severe Postnatal Depression With Child Outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Kingston, D.; Kehler, H.; Austin, M.-P.; Mughal, M.K.; Wajid, A.; Vermeyden, L.; Benzies, K.; Brown, S.; Stuart, S.; Giallo, R. Trajectories of maternal depressive symptoms during pregnancy and the first 12 months postpartum and child externalizing and internalizing behavior at three years. PLoS ONE 2018, 13, e0195365. [Google Scholar] [CrossRef]
- Zhang, Q.; Dai, X.; Li, W. Comparative efficacy and acceptability of pharmacotherapies for postpartum depression: A systematic review and network meta-analysis. Front. Pharmacol. 2022, 13, 950004. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, Y.; Carlini, S.V.; Deligiannidis, K.M. Advances in pharmacotherapy for postpartum depression: A structured review of standard-of-care antidepressants and novel neuroactive steroid antidepressants. Ther. Adv. Psychopharmacol. 2022, 12, 20451253211065859. [Google Scholar] [CrossRef] [PubMed]
- Yonkers, K.A.; Wisner, K.L.; Stewart, D.E.; Oberlander, T.F.; Dell, D.L.; Stotland, N.; Ramin, S.; Chaudron, L.; Lockwood, C. The management of depression during pregnancy: A report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Gen. Hosp. Psychiatry 2009, 31, 403–413. [Google Scholar] [CrossRef]
- Stewart, D.E.; Vigod, S.N. Postpartum Depression: Pathophysiology, Treatment, and Emerging Therapeutics. Annu. Rev. Med. 2019, 70, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Frieder, A.; Fersh, M.; Hainline, R.; Deligiannidis, K.M. Pharmacotherapy of Postpartum Depression: Current Approaches and Novel Drug Development. CNS Drugs 2019, 33, 265–282. [Google Scholar] [CrossRef]
- Molyneaux, E.; Howard, L.M.; McGeown, H.R.; Karia, A.M.; Trevillion, K. Antidepressant treatment for postnatal depression. Cochrane Database Syst. Rev. 2014, 9, CD002018. [Google Scholar] [CrossRef]
- Stuart, S. Interpersonal Psychotherapy for Postpartum Depression. Clin. Psychol. Psychother. 2012, 19, 134–140. [Google Scholar] [CrossRef]
- Stuart, S.; Pereira, X.V.; Chung, J.P. Transcultural adaptation of interpersonal psychotherapy in Asia. Asia-Pac. Psychiatry 2020, 13, e12439. [Google Scholar] [CrossRef] [PubMed]
- Moot, W.; Crowe, M.; Inder, M.; Eggleston, K.; Frampton, C.; Porter, R.J. Domain-Based Functional Improvements in Bipolar Disorder After Interpersonal and Social Rhythm Therapy. Front. Psychiatry 2022, 13, 767629. [Google Scholar] [CrossRef]
- Amini, S.; Jafarirad, S.; Amani, R.; Bargard, M.S.; Cheraghian, B.; Hemmati, A.A. The relationship between dietary intakes during pregnancy and incidence of postpartum depression: A case-control study. Nutr. Food Sci. 2019, 50, 751–764. [Google Scholar] [CrossRef]
- Ellsworth-Bowers, E.R.; Corwin, E.J. Nutrition and the psychoneuroimmunology of postpartum depression. Nutr. Res. Rev. 2012, 25, 180–192. [Google Scholar] [CrossRef]
- Lanjewar, S.; Nimkar, S.; Jungari, S. Depressed Motherhood: Prevalence and Covariates of Maternal Postpartum Depression among Urban Mothers in India. Asian J. Psychiatry 2021, 57, 102567. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Sparling, T.M.; Nesbitt, R.C.; Henschke, N.; Gabrysch, S. Nutrients and perinatal depression: A systematic review. J. Nutr. Sci. 2017, 6, e61. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Verberne, L.; De Irala, J.; Ruíz-Canela, M.; Toledo, E.; Serra-Majem, L.; Martínez-González, M.A. Dietary Fat Intake and the Risk of Depression: The SUN Project. PLoS ONE 2011, 6, e16268. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Gan, R.-Y.; Li, B.-Y.; Mao, Q.-Q.; Shang, A.; Xu, X.-Y.; Li, H.-Y.; Li, H.-B. Effects and Mechanisms of Tea on Parkinson’s Disease, Alzheimer’s Disease and Depression. Food Rev. Int. 2021, 39, 278–306. [Google Scholar] [CrossRef]
- Ren, Y.; Sun-Waterhouse, D.; Ouyang, F.; Tan, X.; Li, D.; Xu, L.; Li, B.; Wang, Y.; Li, F. Apple phenolic extracts ameliorate lead-induced cognitive impairment and depression- and anxiety-like behavior in mice by abating oxidative stress, inflammation and apoptosis via the miR-22-3p/SIRT1 axis. Food Funct. 2022, 13, 2647–2661. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-X.; Li, J.; Zhou, D.-D.; Xiong, R.-G.; Huang, S.-Y.; Saimaiti, A.; Shang, A.; Li, H.-B. Possible Effects and Mechanisms of Dietary Natural Products and Nutrients on Depression and Anxiety: A Narrative Review. Antioxidants 2022, 11, 2132. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, T.; Yu, Y.; Li, M.; Sun, X.; Song, W.; Wang, Y.; Zhang, C.; Fu, F. The etiology of poststroke-depression: A hypothesis involving HPA axis. BioMedicine 2022, 151, 113146. [Google Scholar] [CrossRef] [PubMed]
- Yahya, N.F.S.; Teng, N.I.M.F.; Das, S.; Juliana, N. Nutrition and physical activity interventions to ameliorate postpartum depression: A scoping review. Asia Pac. J. Clin. Nutr. 2021, 30, 662–674. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, R.; Selvamani, T.Y.; Zahra, A.; Malla, J.; Dhanoa, R.K.; Venugopal, S.; Shoukrie, S.I.; Hamouda, R.K.; Hamid, P. Association between Dietary Habits and Depression: A Systematic Review. Cureus 2022, 14, e32359. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, G.N.; Sanlier, N. The relationship between nutrition and depression in the life process: A mini-review. Exp. Gerontol. 2023, 172, 112072. [Google Scholar] [CrossRef] [PubMed]
- Rudzińska, A.; Perera, I.; Gryglewska, B.; Gąsowski, J.; Piotrowicz, K. Can the Mediterranean diet decrease the risk of depression in older persons—A systematic review. Psychiatr. Polska 2023, 57, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Zielińska, M.; Łuszczki, E.; Michońska, I.; Dereń, K. The Mediterranean Diet and the Western Diet in Adolescent Depression-Current Reports. Nutrients 2022, 14, 4390. [Google Scholar] [CrossRef]
- Riveros, M.E.; Ávila, A.; Schruers, K.; Ezquer, F. Antioxidant Biomolecules and Their Potential for the Treatment of Difficult-to-Treat Depression and Conventional Treatment-Resistant Depression. Antioxidants 2022, 11, 540. [Google Scholar] [CrossRef]
- Keys, A.; Mienotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The Diet and 15-Year Death Rate in The Seven Countries Study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean diet and health: A comprehensive overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef]
- Richardson, L.A.; Izuora, K.; Basu, A. Mediterranean Diet and Its Association with Cardiovascular Disease Risk Factors: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 12762. [Google Scholar] [CrossRef]
- Franco, G.A.; Interdonato, L.; Cordaro, M.; Cuzzocrea, S.; Di Paola, R. Bioactive Compounds of the Mediterranean Diet as Nutritional Support to Fight Neurodegenerative Disease. Int. J. Mol. Sci. 2023, 24, 7318. [Google Scholar] [CrossRef]
- Maggi, S.; Ticinesi, A.; Limongi, F.; Noale, M.; Ecarnot, F. The role of nutrition and the Mediterranean diet on the trajectories of cognitive decline. Exp. Gerontol. 2023, 173, 112110. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef]
- Mantzorou, M.; Vadikolias, K.; Pavlidou, E.; Tryfonos, C.; Vasios, G.; Serdari, A.; Giaginis, C. Mediterranean diet adherence is associated with better cognitive status and less depressive symptoms in a Greek elderly population. Aging Clin. Exp. Res. 2020, 33, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Mantzorou, M.; Vadikolias, K.; Pavlidou, E.; Serdari, A.; Vasios, G.; Tryfonos, C.; Giaginis, C. Nutritional status is associated with the degree of cognitive impairment and depressive symptoms in a Greek elderly population. Nutr. Neurosci. 2018, 23, 201–209. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report: 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006. Available online: https://apps.who.int/iris/handle/10665/43432 (accessed on 20 March 2023).
- James, W.P.T. WHO recognition of the global obesity epidemic. Int. J. Obes. 2008, 32, S120–S126. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Gilmore, L.A.; Redman, L.M. Weight gain in pregnancy and application of the 2009 IOM guidelines: Toward a uniform approach. Obesity 2015, 23, 507–511. [Google Scholar] [CrossRef]
- Mantzorou, M.; Papandreou, D.; Vasios, G.K.; Pavlidou, E.; Antasouras, G.; Psara, E.; Taha, Z.; Poulios, E.; Giaginis, C. Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery. Nutrients 2022, 14, 3599. [Google Scholar] [CrossRef]
- Papandreou, D.; Mantzorou, M.; Tyrovolas, S.; Pavlidou, E.; Antasouras, G.; Psara, E.; Poulios, E.; Vasios, G.K.; Giaginis, C. Pre-Pregnancy Excess Weight Association with Maternal Sociodemographic, Anthropometric and Lifestyle Factors and Maternal Perinatal Outcomes. Nutrients 2022, 14, 3810. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Cox, J. Thirty years with the Edinburgh Postnatal Depression Scale: Voices from the past and recommendations for the future. Br. J. Psychiatry 2019, 214, 127–129. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Arvaniti, F.; Panagiotakos, D.B. Healthy Indexes in Public Health Practice and Research: A Review. Crit. Rev. Food Sci. Nutr. 2008, 48, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, M.-R.; Wei, Y.-J.; Sun, L.; Zhang, J.-X.; Zhang, H.-G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [PubMed]
- Gould, J.F.; Best, K.; Makrides, M. Perinatal nutrition interventions and post-partum depressive symptoms. J. Affect. Disord. 2017, 224, 2–9. [Google Scholar] [CrossRef]
- Fahey, J.O.; Shenassa, E. Understanding and Meeting the Needs of Women in the Postpartum Period: The Perinatal Maternal Health Promotion Model. J. Midwifery Women’s Health 2018, 58, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Barker, E.D.; Kirkham, N.; Ng, J.; Jensen, S.K.G. Prenatal maternal depression symptoms and nutrition, and child cognitive function. Br. J. Psychiatry 2013, 203, 417–421. [Google Scholar] [CrossRef]
- Fowles, E.R.; Bryant, M.; Kim, S.; Walker, L.O.; Ruiz, R.J.; Timmerman, G.M.; Brown, A. Predictors of Dietary Quality in Low-Income Pregnant Women: A Path Analysis. Nurs. Res. 2011, 60, 286–294. [Google Scholar] [CrossRef]
- Zuckerman, B.; Amaro, H.; Bauchner, H.; Cabral, H. Depressive symptoms during pregnancy: Relationship to poor health behaviors. Am. J. Obstet. Gynecol. 1989, 160, 1107–1111. [Google Scholar] [CrossRef]
- Opie, R.S.; Uldrich, A.C.; Ball, K. Maternal Postpartum Diet and Postpartum Depression: A Systematic Review. Matern. Child Health J. 2020, 24, 966–978. [Google Scholar] [CrossRef]
- Teo, C.; Chia, A.-R.; Colega, M.T.; Chen, L.-W.; Fok, D.; Pang, W.W.; Godfrey, K.M.; Tan, K.H.; Yap, F.; Shek, L.P.-C.; et al. Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study. Nutrients 2018, 10, 299. [Google Scholar] [CrossRef]
- Chatzi, L.; Melaki, V.; Sarri, K.; Apostolaki, I.; Roumeliotaki, T.; Georgiou, V.; Vassilaki, M.; Koutis, A.; Bitsios, P.; Kogevinas, M. Dietary patterns during pregnancy and the risk of postpartum depression: The mother–child ‘Rhea’ cohort in Crete, Greece. Public Health Nutr. 2011, 14, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Vilela, A.A.F.; Farias, D.R.; Eshriqui, I.; Vaz, J.d.S.; Franco-Sena, A.B.; Castro, M.B.T.; Olinto, M.T.A.; Machado, S.P.; da Silva, A.A.M.; Kac, G. Prepregnancy Healthy Dietary Pattern Is Inversely Associated with Depressive Symptoms among Pregnant Brazilian Women. J. Nutr. 2014, 144, 1612–1618. [Google Scholar] [CrossRef] [PubMed]
- Pina-Camacho, L.; Jensen, S.K.; Gaysina, D.; Barker, E.D. Maternal depression symptoms, unhealthy diet and child emotional–behavioural dysregulation. Psychol. Med. 2015, 45, 1851–1860. [Google Scholar] [CrossRef]
- Leung, B.M.; Kaplan, B.J.; Field, C.J.; Tough, S.; Eliasziw, M.; Gomez, M.F.; McCargar, L.J.; Gagnon, L.; the APrON Study Team. Prenatal micronutrient supplementation and postpartum depressive symptoms in a pregnancy cohort. BMC Pregnancy Childbirth 2013, 13, 2. [Google Scholar] [CrossRef]
- Hsu, M.-C.; Tung, C.-Y.; Chen, H.-E. Omega-3 polyunsaturated fatty acid supplementation in prevention and treatment of maternal depression: Putative mechanism and recommendation. J. Affect. Disord. 2018, 238, 47–61. [Google Scholar] [CrossRef]
- Firouzabadi, F.D.; Shab-Bidar, S.; Jayedi, A. The effects of omega-3 polyunsaturated fatty acids supplementation in pregnancy, lactation, and infancy: An umbrella review of meta-analyses of randomized trials. Pharmacol. Res. 2022, 177, 106100. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.J.; Murray, L.; Beckmann, M.M.; Kent, T.; Macfarlane, B. Dietary supplements for preventing postnatal depression. Cochrane Database Syst. Rev. 2013, 2013, CD009104. [Google Scholar] [CrossRef]
- Mocking, R.J.T.; Steijn, K.; Roos, C.; Assies, J.; Bergink, V.; Ruhé, H.G.; Schene, A.H. Omega-3 Fatty Acid Supplementation for Perinatal Depression: A Meta-Analysis. J. Clin. Psychiatry 2020, 81, 19r13106. [Google Scholar] [CrossRef]
- Judge, M.P.; Beck, C.T.; Durham, H.; McKelvey, M.M.; Lammi-Keefe, C.J. Pilot trial evaluating maternal docosahexaenoic acid consumption during pregnancy: Decreased postpartum depressive symptomatology. Int. J. Nurs. Sci. 2014, 1, 339–345. [Google Scholar] [CrossRef][Green Version]
- Miyake, Y.; Tanaka, K.; Okubo, H.; Sasaki, S.; Arakawa, M. Fish and fat intake and prevalence of depressive symptoms during pregnancy in Japan: Baseline data from the Kyushu Okinawa Maternal and Child Health Study. J. Psychiatr. Res. 2013, 47, 572–578. [Google Scholar] [CrossRef]
- Flor-Alemany, M.; Migueles, J.H.; Alemany-Arrebola, I.; Aparicio, V.A.; Baena-García, L. Exercise, Mediterranean Diet Adherence or Both during Pregnancy to Prevent Postpartum Depression—GESTAFIT Trial Secondary Analyses. Int. J. Environ. Res. Public Health 2022, 19, 14450. [Google Scholar] [CrossRef]
- Chopra, C.; Mandalika, S.; Kinger, N. Does diet play a role in the prevention and management of depression among adolescents? A narrative review. Nutr. Health 2021, 27, 243–263. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Marx, W.; Dash, S.; Carney, R.; Teasdale, S.B.; Solmi, M.; Stubbs, B.; Schuch, F.B.; Carvalho, A.F.; Jacka, F.; et al. The Effects of Dietary Improvement on Symptoms of Depression and Anxiety: A Meta-Analysis of Randomized Controlled Trials. Psychosom. Med. 2019, 81, 265–280. [Google Scholar] [CrossRef]
- Arouca, A.; Michels, N.; Moreno, L.A.; González-Gil, E.M.; Marcos, A.; Gómez, S.; Díaz, L.E.; Widhalm, K.; Molnár, D.; Manios, Y.; et al. Associations between a Mediterranean diet pattern and inflammatory biomarkers in European adolescents. Eur. J. Nutr. 2017, 57, 1747–1760. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Kifley, A.; Louie, J.C.Y.; Mitchell, P. Association between Carbohydrate Nutrition and Successful Aging Over 10 Years. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1335–1340. [Google Scholar] [CrossRef]
- Tehrani, A.N.; Salehpour, A.; Beyzai, B.; Farhadnejad, H.; Moloodi, R.; Hekmatdoost, A.; Rashidkhani, B. Adherence to Mediterranean dietary pattern and depression, anxiety and stress among high-school female adolescents. Mediterr. J. Nutr. Metab. 2018, 11, 73–83. [Google Scholar] [CrossRef]
- Molendijk, M.; Molero, P.; Sánchez-Pedreño, F.O.; Van der Does, W.; Martínez-González, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.-H.; Zhang, Z.-H. Risk factors for postpartum depression: An evidence-based systematic review of systematic reviews and meta-analyses. Asian J. Psychiatry 2020, 53, 102353. [Google Scholar] [CrossRef] [PubMed]
- Ghaedrahmati, M.; Kazemi, A.; Kheirabadi, G.; Ebrahimi, A.; Bahrami, M. Postpartum depression risk factors: A narrative review. J. Educ. Health Promot. 2017, 6, 60. [Google Scholar]
- Qiu, X.; Zhang, S.; Yan, J. Gestational weight gain and risk of postpartum depression: A meta-analysis of observational studies. Psychiatry Res. 2022, 310, 114448. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.; Luo, J.; Wang, J.; Liang, Y. Association between breastfeeding and postpartum depression: A meta-analysis. J. Affect. Disord. 2022, 308, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Moreira, L.K.S.; Moreira, C.V.L.; Custódio, C.H.X.; Dias, M.L.P.; Rosa, D.A.; Ferreira-Neto, M.L.; Colombari, E.; Costa, E.A.; Fajemiroye, J.O.; Pedrino, G.R. Post-partum depression: From clinical understanding to preclinical assessments. Front. Psychiatry 2023, 14, 1173635. [Google Scholar] [CrossRef]
- Wells, T. Postpartum Depression: Screening and Collaborative Management. Prim. Care 2023, 50, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, I.; Mehendale, A.M.; Malhotra, R. Risk Factors of Postpartum Depression. Cureus 2022, 14, e30898. [Google Scholar] [CrossRef]
- Eurostat Database on Births and Fertility Data. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210224-1 (accessed on 23 August 2023).
- Statista Research Department Data. Available online: https://www.statista.com/statistics/612088/mean-age-of-woman-at-childbirth-europe/ (accessed on 23 August 2023).
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Kanellopoulos, D.; Gourounti, K. Tocophobia and Women’s Desire for a Caesarean Section: A Systematic Review. Maedica 2022, 17, 186–193. [Google Scholar]
- O’Connell, M.A.; Khashan, A.S.; Leahy-Warren, P.; Stewart, F.; O’Neill, S.M. Interventions for fear of childbirth (tocophobia). Cochrane Database Syst. Rev. 2021, 7, CD013321. [Google Scholar] [CrossRef]
- Chan, A.W.; Reid, C.; Skeffington, P.; Marriott, R. A systematic review of EPDS cultural suitability with Indigenous mothers: A global perspective. Arch. Womens Ment. Health 2020, 24, 353–365. [Google Scholar] [CrossRef]
- Chang, M.-W.; Brown, R.; Nitzke, S.; Smith, B.; Eghtedary, K. Stress, Sleep, Depression and Dietary Intakes among Low-Income Overweight and Obese Pregnant Women. Matern. Child Health J. 2014, 19, 1047–1059. [Google Scholar] [CrossRef]
- Silva, N.d.M.L.e.; Lam, M.P.; Soares, C.N.; Munoz, D.P.; Milev, R.; De Felice, F.G. Insulin Resistance as a Shared Pathogenic Mechanism between Depression and Type 2 Diabetes. Front. Psychiatry 2019, 10, 57. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics (n = 3941) | Postpartum Depression (n, %) | ||
|---|---|---|---|
| No 3464 (87.9%) | Yes 477 (12.1%) | p-Value | |
| Age (mean ± SD; years) | 32.7 ± 5.4 | 33.9 ± 53 | p = 0.0012 |
| Education level (n, %) | p ˂ 0.0001 | ||
| Primary education | 643 (18.6%) | 318 (66.7%) | |
| Secondary education | 1484 (42.8%) | 127 (26.6%) | |
| University studies | 1337 (38.6%) | 32 (6.7%) | |
| Family economic status (n, %) | |||
| Low | 1625 (46.9%) | 201 (42.1%) | p = 0.0001 |
| Medium | 1518 (43.8%) | 256 (53.7%) | |
| High | 321 (9.3%) | 20 (4.2%) | |
| Nationality (n, %) | p = 0.0117 | ||
| Greek | 3305 (95.4%) | 467 (97.9%) | |
| Other | 159 (4.6%) | 10 (2.1%) | |
| Marital status (n, %) | p = 0.5698 | ||
| Married | 2661 (76.8%) | 372 (78.0%) | |
| Other | 803 (23.2%) | 105 (22.0%) | |
| Employment (n, %) | p = 0.2276 | ||
| Employed | 2330 (67.3%) | 334 (70.0%) | |
| Unemployed | 1134 (32.7%) | 143 (30.0%) | |
| Smoking habits (n, %) | p = 0.4010 | ||
| No smokers | 2582 (74.5%) | 347 (72.7%) | |
| Smokers | 882 (25.5%) | 130 (27.3%) | |
| Parity (n, %) | p = 0.0307 | ||
| Nulliparity | 2146 (62.0%) | 271 (56.8%) | |
| Multiparity | 1318 (38.0%) | 206 (43.2%) | |
| Pre-pregnancy BMI status (n, %) | p = 0.8239 | ||
| Normal weight | 2618 (75.6%) | 356 (74.6%) | |
| Overweight | 651 (18.8%) | 91 (19.1%) | |
| Obese | 195 (5.6%) | 30 (6.3%) | |
| Postpartum BMI status (n, %) | p ˂ 0.0001 | ||
| Normal weight | 2656 (76.7%) | 323 (67.7%) | |
| Overweight | 539 (15.6%) | 117 (24.5%) | |
| Obese | 269 (7.8%) | 37 (7.8%) | |
| Gestational weight gain (n, %) | p = 0.0051 | ||
| Low | 114 (3.3%) | 10 (2.1%) | |
| Normal | 2474 (71.4%) | 315 (66.0%) | |
| Excess | 876 (25.3%) | 152 (31.9%) | |
| Preterm birth (<37th week, n, %) | p = 0.9999 | ||
| No | 2716 (78.4%) | 374 (78.4%) | |
| Yes | 748 (21.6%) | 103 (21.6%) | |
| Type of delivery (n, %) | p = 0.0001 | ||
| Vaginal | 1569 (45.3%) | 172 (36.1%) | |
| Caesarean section | 1895 (54.7%) | 305 (63.9%) | |
| Exclusive breastfeeding (n, %) | p ˂ 0.0001 | ||
| No | 1674 (48.3%) | 302 (63.3%) | |
| Yes | 1790 (51.7%) | 175 (36.7%) | |
| Mediterranean Diet adherence (n, %) | p ˂ 0.0001 | ||
| Very low | 807 (23.3%) | 174 (36.5%) | |
| Low | 854 (24.6%) | 126 (26.4%) | |
| Moderate | 903 (26.1%) | 103 (21.6%) | |
| High | 900 (26.0%) | 74 (15.5%) | |
| Characteristics | Postpartum Depression (No vs. Yes) | |
|---|---|---|
| RR * (95% CI **) | p-Value | |
| Age (Below vs. Over mean value) | 1.32 (0.62–2.1) | p = 0.0819 |
| Education level (Primary education vs. Secondary education and university studies) | 1.38 (1.02–1.73) | p = 0.0244 |
| Family economic status (High vs. Low or medium) | 1.19 (0.59–1.88) | p = 0.0936 |
| Nationality (Greek vs. Other) | 1.06 (0.39–1.88) | p = 0.3134 |
| Marital status (Married vs. Other) | 0.93 (0.21–1.74) | p = 0.7501 |
| Employment (Employed vs. Unemployed) | 1.05 (0.27–1.83) | p = 0.5812 |
| Smoking habits (No vs. Yes) | 1.16 (0.45–1.98) | p = 0.7129 |
| Parity (Nulliparity vs. Multiparity) | 1.38 (0.67–2.12) | p = 0.2733 |
| Pre-pregnancy BMI status (Normal weight vs. Overweight & obese) | 1.11 (0.27–2.01) | p = 0.8159 |
| Postpartum BMI status (Normal weight vs. Overweight & obese) | 1.95 (1.58–2.23) | p = 0.0198 |
| Gestational weight gain (Low and normal vs. Excess) | 1.44 (1.11–1.79) | p = 0.0107 |
| Preterm birth (No vs. Yes) | 1.06 (0.45–1.89) | p = 0.7897 |
| Type of delivery (Vaginal/Caesarean section) | 1.93 (1.62–2.1.27) | p = 0.0087 |
| Exclusive breastfeeding (Yes/No) | 2.44 (2.25–2.514) | p = 0.0031 |
| Mediterranean Diet adherence (Moderate + High/Very low + Low) | 2.51 (2.33–2.68) | p = 0.0005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoulou, S.K.; Pavlidou, E.; Dakanalis, A.; Antasouras, G.; Vorvolakos, T.; Mentzelou, M.; Serdari, A.; Pandi, A.-L.; Spanoudaki, M.; Alexatou, O.; et al. Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence. Nutrients 2023, 15, 3853. https://doi.org/10.3390/nu15173853
Papadopoulou SK, Pavlidou E, Dakanalis A, Antasouras G, Vorvolakos T, Mentzelou M, Serdari A, Pandi A-L, Spanoudaki M, Alexatou O, et al. Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence. Nutrients. 2023; 15(17):3853. https://doi.org/10.3390/nu15173853
Chicago/Turabian StylePapadopoulou, Sousana K., Eleni Pavlidou, Antonios Dakanalis, Georgios Antasouras, Theofanis Vorvolakos, Maria Mentzelou, Aspasia Serdari, Aimilia-Lynn Pandi, Maria Spanoudaki, Olga Alexatou, and et al. 2023. "Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence" Nutrients 15, no. 17: 3853. https://doi.org/10.3390/nu15173853
APA StylePapadopoulou, S. K., Pavlidou, E., Dakanalis, A., Antasouras, G., Vorvolakos, T., Mentzelou, M., Serdari, A., Pandi, A.-L., Spanoudaki, M., Alexatou, O., Aggelakou, E.-P., & Giaginis, C. (2023). Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence. Nutrients, 15(17), 3853. https://doi.org/10.3390/nu15173853