
Therapeutic Effects of Vitamin D on Vaginal, Sexual, and Urological Functions in Postmenopausal Women


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Background
2. Methodology
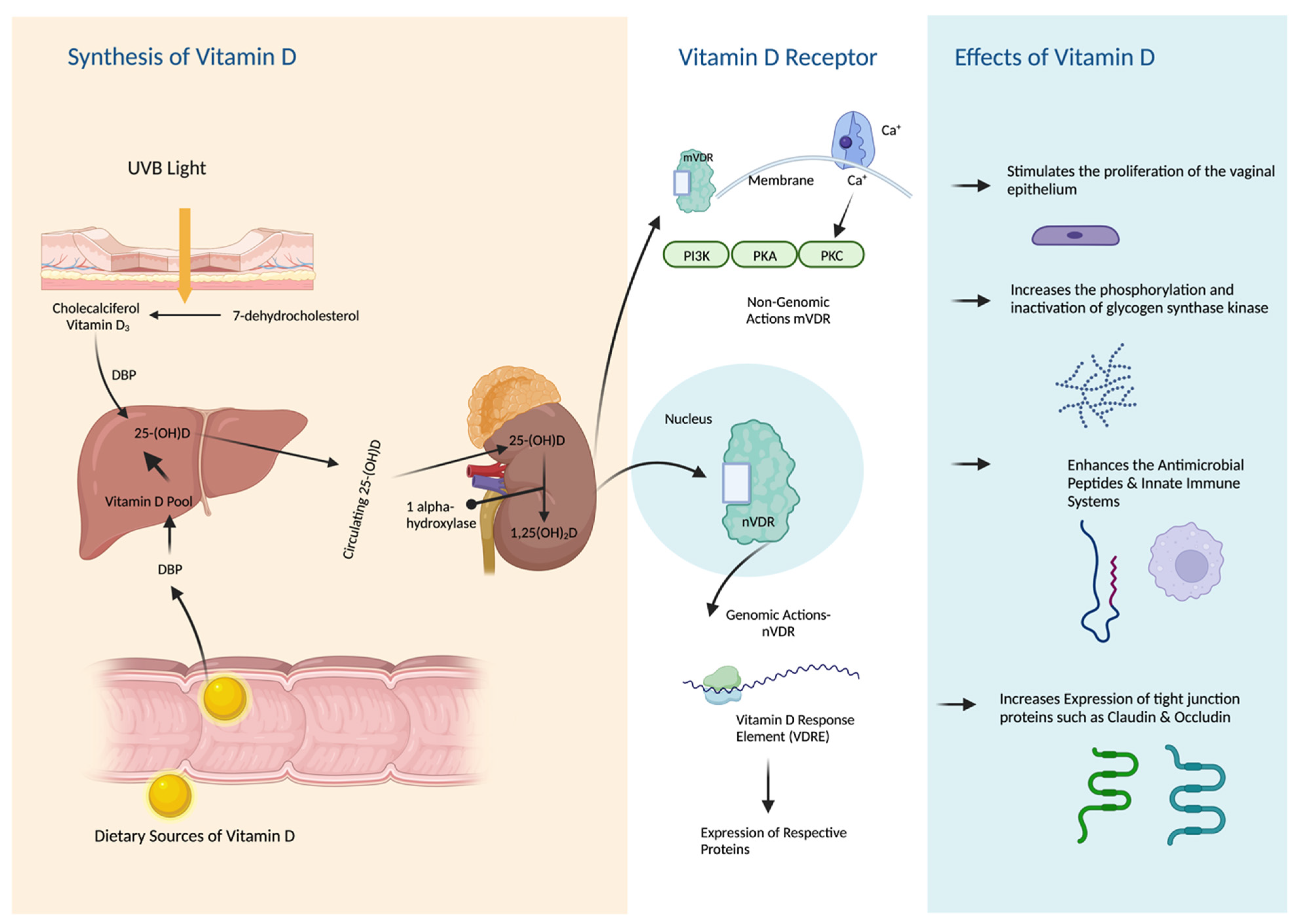
3. The Pharmacology of Vitamin D
3.1. Vitamin D Synthesis
3.2. Vitamin D Metabolism
3.3. Vitamin D Mechanism of Action
3.4. Predictors of Vitamin D Status
3.5. Effect of Estrogen on Vitamin D Metabolism in Postmenopausal Women
4. Genitourinary Syndrome of Menopause
4.1. Urogenital Changes in Postmenopausal Women
4.2. Hormonal Therapy for GSM Symptoms
4.3. Vitamin D Supplementations for GSM Symptoms
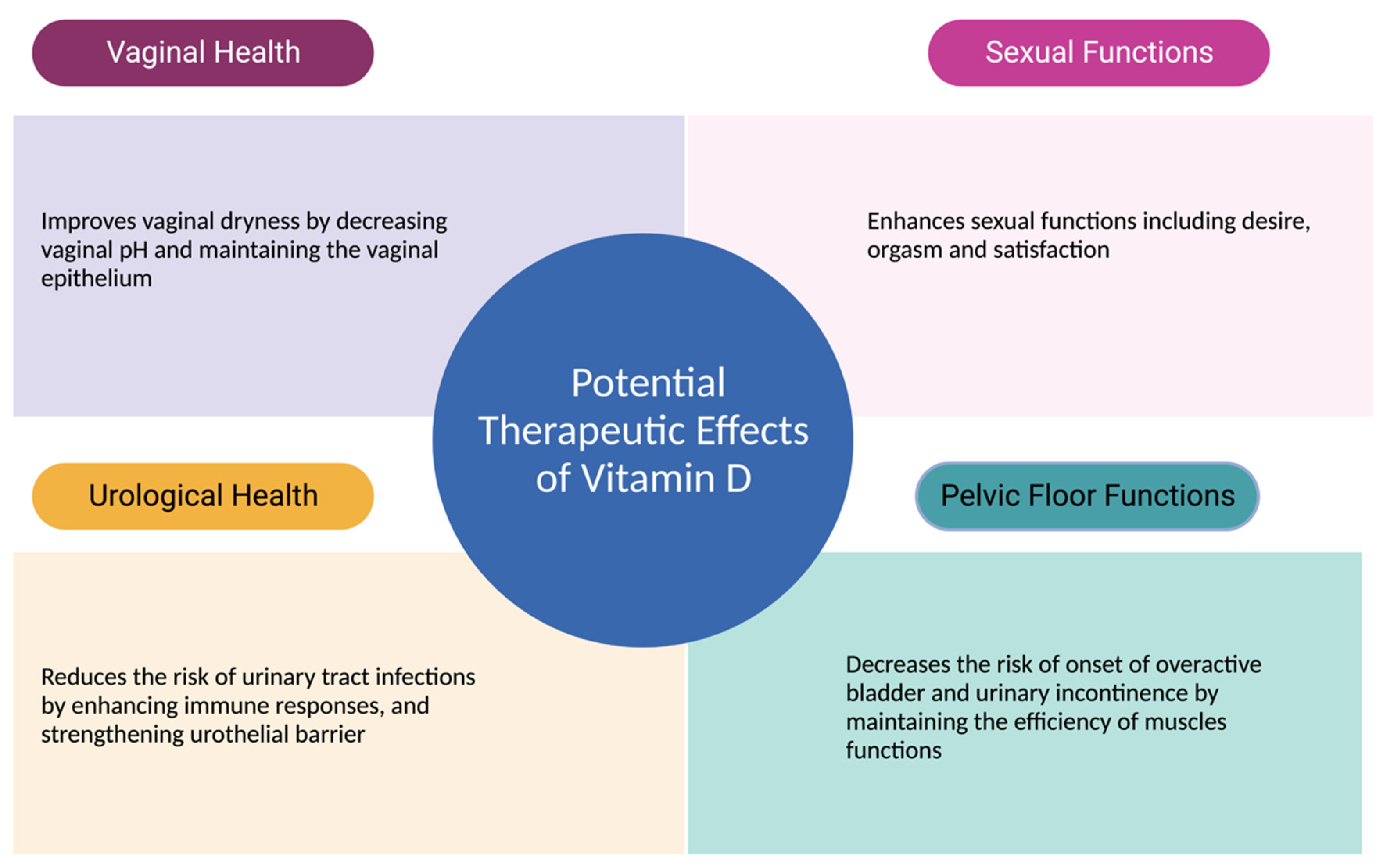
5. Therapeutic Effects of Vitamin D on Urogenital Functions
5.1. Cellular Effects of Vitamin D on Urogenital Tissues
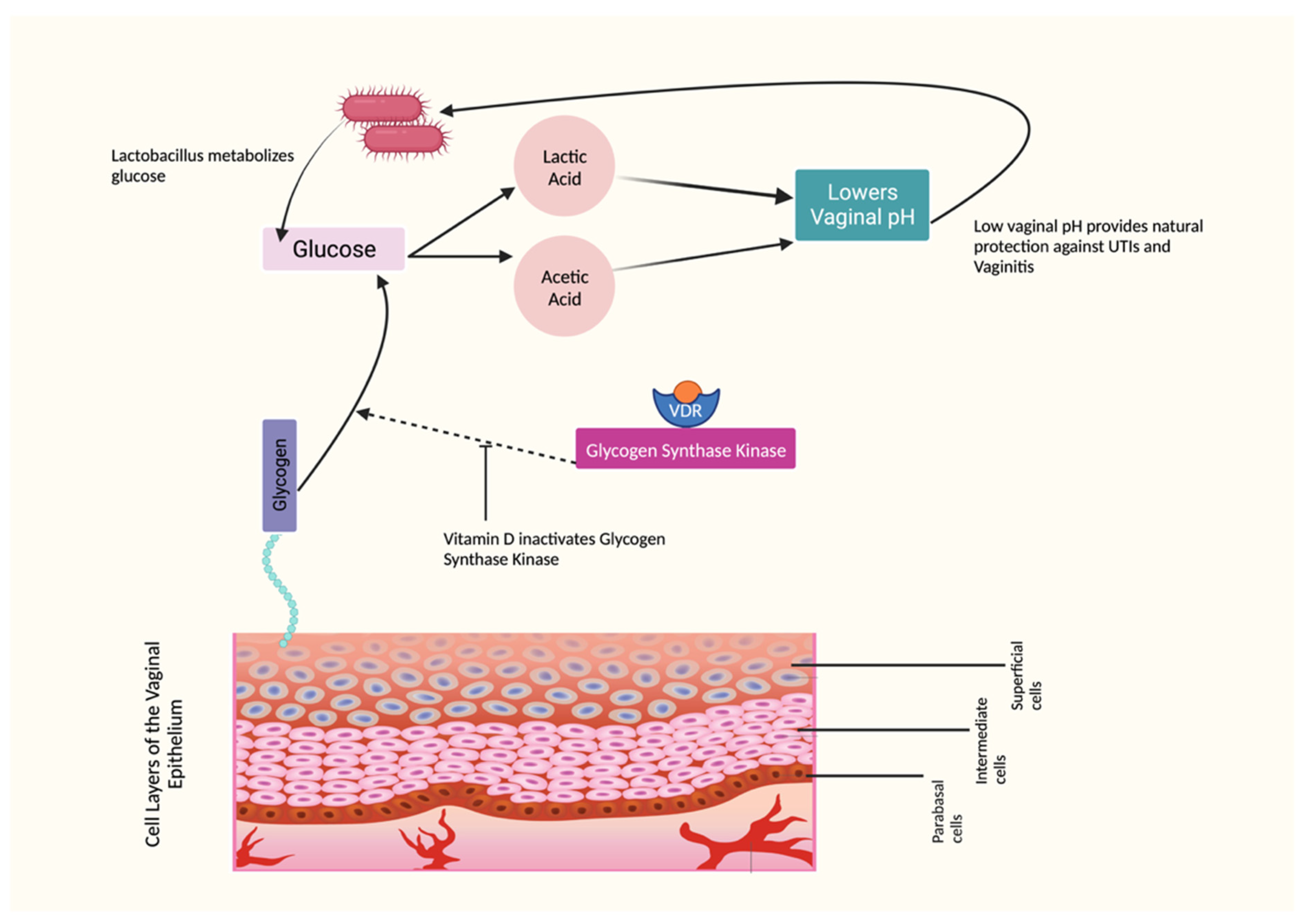
5.2. The Effects of Vitamin D on Vaginal Epithelium and pH
5.3. The Effects of Vitamin D on Vaginal Symptoms
5.4. The Effects of Vitamin D on Vaginal Infections
5.5. The Effects of Vitamin D on Sexual Functions
5.6. The Role of Vitamin D in UTIs: Effects on the Immune Function
5.7. The Role of Vitamin D in UTIs: Effects on Tight Junction Proteins
5.8. The Effects of Vitamin D on Pelvic Floor Disorders
6. Vaginal Dosage Form as Route of Delivery
7. Future Research Directions
8. Conclusions
9. Key Findings
- The role of vitamin D on urogenital and sexual health in postmenopausal women revealed a limited but growing body of research.
- Vitamin D has the potential to support postmenopausal women’s urogenital and sexual health.
- Vitamin D receptors play a significant role in mediating and maintaining the pharmacological effects of vitamin D on urogenital organs.
- Both oral and vaginal vitamin D were shown to improve vulvovaginal symptoms, sexual functioning and reduce the risk of urinary tract infections.
- Further research is needed to fully understand the therapeutic effects of vitamin D supplementation on urogenital and sexual health in postmenopausal women.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gandhi, J.; Chen, A.; Dagur, G.; Suh, Y.; Smith, N.; Cali, B.; Khan, S.A. Genitourinary syndrome of menopause: An overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am. J. Obstet. Gynecol. 2016, 215, 704–711. [Google Scholar] [CrossRef] [PubMed]
- North American Menopause Society. Management of symptomatic vulvovaginal atrophy: 2013 position statement of The North American Menopause Society. Menopause 2013, 20, 888–902. [Google Scholar] [CrossRef] [PubMed]
- Angelou, K.; Grigoriadis, T.; Diakosavvas, M.; Zacharakis, D.; Athanasiou, S. The Genitourinary Syndrome of Menopause: An Overview of the Recent Data. Cureus 2020, 12, e7586. [Google Scholar] [CrossRef]
- Faubion, S.S.; Sood, R.; Kapoor, E. Genitourinary Syndrome of Menopause: Management Strategies for the Clinician. Mayo Clin. Proc. 2017, 92, 1842–1849. [Google Scholar] [CrossRef] [PubMed]
- Hugenholtz, F.; van der Veer, C.; Terpstra, M.L.; Borgdorff, H.; van Houdt, R.; Bruisten, S.; Geerlings, S.E.; van de Wijgert, J. Urine and vaginal microbiota compositions of postmenopausal and premenopausal women differ regardless of recurrent urinary tract infection and renal transplant status. Sci. Rep. 2022, 12, 2698. [Google Scholar] [CrossRef]
- Nappi, R.E.; Martini, E.; Cucinella, L.; Martella, S.; Tiranini, L.; Inzoli, A.; Brambilla, E.; Bosoni, D.; Cassani, C.; Gardella, B. Addressing Vulvovaginal Atrophy (VVA)/Genitourinary Syndrome of Menopause (GSM) for Healthy Aging in Women. Front. Endocrinol. 2019, 10, 561. [Google Scholar] [CrossRef] [PubMed]
- Portman, D.J.; Gass, M.L.; Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: New terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Menopause 2014, 21, 1063–1068. [Google Scholar] [CrossRef]
- Domoney, C.; Short, H.; Particco, M.; Panay, N. Symptoms, attitudes and treatment perceptions of vulvo-vaginal atrophy in UK postmenopausal women: Results from the REVIVE-EU study. Post Reprod. Health 2020, 26, 101–109. [Google Scholar] [CrossRef]
- Krychman, M.; Graham, S.; Bernick, B.; Mirkin, S.; Kingsberg, S.A. The Women’s EMPOWER Survey: Women’s Knowledge and Awareness of Treatment Options for Vulvar and Vaginal Atrophy Remains Inadequate. J. Sex. Med. 2017, 14, 425–433. [Google Scholar] [CrossRef]
- Moral, E.; Delgado, J.L.; Carmona, F.; Caballero, B.; Guillan, C.; Gonzalez, P.M.; Suarez-Almarza, J.; Velasco-Ortega, S.; Nieto, C.; as the writing group of the GENISSE study. Genitourinary syndrome of menopause. Prevalence and quality of life in Spanish postmenopausal women. The GENISSE study. Climacteric 2018, 21, 167–173. [Google Scholar] [CrossRef]
- Nappi, R.E.; de Melo, N.R.; Martino, M.; Celis-Gonzalez, C.; Villaseca, P.; Rohrich, S.; Palacios, S. Vaginal Health: Insights, Views & Attitudes (VIVA-LATAM): Results from a survey in Latin America. Climacteric 2018, 21, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Kingsberg, S.; Maamari, R.; Simon, J. The CLOSER (CLarifying Vaginal Atrophy’s Impact On SEx and Relationships) survey: Implications of vaginal discomfort in postmenopausal women and in male partners. J. Sex. Med. 2013, 10, 2232–2241. [Google Scholar] [CrossRef] [PubMed]
- Palma, F.; Volpe, A.; Villa, P.; Cagnacci, A.; as the writing group of the AGATA study. Vaginal atrophy of women in postmenopause. Results from a multicentric observational study: The AGATA study. Maturitas 2016, 83, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Mac Bride, M.B.; Rhodes, D.J.; Shuster, L.T. Vulvovaginal atrophy. Mayo Clin. Proc. 2010, 85, 87–94. [Google Scholar] [CrossRef]
- Lee, A.; Lee, M.R.; Lee, H.H.; Kim, Y.S.; Kim, J.M.; Enkhbold, T.; Kim, T.H. Vitamin D Proliferates Vaginal Epithelium through RhoA Expression in Postmenopausal Atrophic Vagina tissue. Mol. Cells 2017, 40, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Jalali-Chimeh, F.; Gholamrezaei, A.; Vafa, M.; Nasiri, M.; Abiri, B.; Darooneh, T.; Ozgoli, G. Effect of Vitamin D Therapy on Sexual Function in Women with Sexual Dysfunction and Vitamin D Deficiency: A Randomized, Double-Blind, Placebo Controlled Clinical Trial. J. Urol. 2019, 201, 987–993. [Google Scholar] [CrossRef]
- Askin, M.; Koc, E.M.; Soyoz, M.; Aksun, S.; Aydogmus, S.; Sozmen, K. Relationship between Postmenopausal Vitamin D Level, Menopausal Symptoms and Sexual Functions. J. Coll. Physicians Surg. Pak. 2019, 29, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Hertting, O.; Holm, A.; Luthje, P.; Brauner, H.; Dyrdak, R.; Jonasson, A.F.; Wiklund, P.; Chromek, M.; Brauner, A. Vitamin D induction of the human antimicrobial Peptide cathelicidin in the urinary bladder. PLoS ONE 2010, 5, e15580. [Google Scholar] [CrossRef]
- Lorenzen, M.; Boisen, I.M.; Mortensen, L.J.; Lanske, B.; Juul, A.; Blomberg Jensen, M. Reproductive endocrinology of vitamin D. Mol. Cell. Endocrinol. 2017, 453, 103–112. [Google Scholar] [CrossRef]
- Skowronska, P.; Pastuszek, E.; Kuczynski, W.; Jaszczol, M.; Kuc, P.; Jakiel, G.; Woclawek-Potocka, I.; Lukaszuk, K. The role of vitamin D in reproductive dysfunction in women—A systematic review. Ann. Agric. Environ. Med. 2016, 23, 671–676. [Google Scholar] [CrossRef]
- Kamronrithisorn, T.; Manonai, J.; Vallibhakara, S.A.; Sophonsritsuk, A.; Vallibhakara, O. Effect of Vitamin D Supplement on Vulvovaginal Atrophy of the Menopause. Nutrients 2020, 12, 2876. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, K.K.; Parikh, H.I.; Garcia, E.M.; Edwards, D.J.; Serrano, M.G.; Hewison, M.; Shary, J.R.; Powell, A.M.; Hollis, B.W.; Fettweis, J.M.; et al. Relationship between vitamin D status and the vaginal microbiome during pregnancy. J. Perinatol. 2019, 39, 824–836. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, B.; Kaleli, B.; Duzcan, E.; Topuz, O. The effects of postmenopausal Vitamin D treatment on vaginal atrophy. Maturitas 2004, 49, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Saeideh, Z.; Raziyeh, M.; Soghrat, F. Comparing the effects of continuous hormone replacement therapy and tibolone on the genital tract of menopausal women; a randomized controlled trial. J. Reprod. Infertil. 2010, 11, 183–187. [Google Scholar] [PubMed]
- Rad, P.; Tadayon, M.; Abbaspour, M.; Latifi, S.M.; Rashidi, I.; Delaviz, H. The effect of vitamin D on vaginal atrophy in postmenopausal women. Iran J. Nurs. Midwifery Res. 2015, 20, 211–215. [Google Scholar]
- Mucci, M.; Carraro, C.; Mancino, P.; Monti, M.; Papadia, L.S.; Volpini, G.; Benvenuti, C. Soy isoflavones, lactobacilli, Magnolia bark extract, vitamin D3 and calcium. Controlled clinical study in menopause. Minerva Ginecol. 2006, 58, 323–334. [Google Scholar]
- Checa, M.A.; Garrido, A.; Prat, M.; Conangla, M.; Rueda, C.; Carreras, R. A comparison of raloxifene and calcium plus vitamin D on vaginal atrophy after discontinuation of long-standing postmenopausal hormone therapy in osteoporotic women. A randomized, masked-evaluator, one-year, prospective study. Maturitas 2005, 52, 70–77. [Google Scholar] [CrossRef]
- Bala, R.; Kaur, H.; Nagpal, M. Authenticity of vitamin D in modified vaginal health index in geriatric subjects. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 4119–4122. [Google Scholar] [CrossRef]
- Riazi, H.; Ghazanfarpour, M.; Taebi, M.; Abdolahian, S. Effect of Vitamin D on the Vaginal Health of Menopausal Women: A Systematic Review. J. Menopausal. Med. 2019, 25, 109–116. [Google Scholar] [CrossRef]
- Sarebani, Z.; Chegini, V.; Chen, H.; Aali, E.; Mirzadeh, M.; Abbaspour, M.; Griffiths, M.D.; Alimoradi, Z. Effect of vitamin D vaginal suppository on sexual functioning among postmenopausal women: A three-arm randomized controlled clinical trial. Obstet. Gynecol. Sci. 2023, 66, 208–220. [Google Scholar] [CrossRef]
- Hussain, A.; Ahsan, F. The vagina as a route for systemic drug delivery. J. Control. Release 2005, 103, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, M.M.; Huri, H.Z.; Baig, K.; Abduelkarem, A.R. Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review. Nutrients 2023, 15, 685. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.Q.; Chen, T.C.; Matsuoka, L.Y.; Wortsman, J.; Holick, M.F. Kinetic and thermodynamic studies of the conversion of previtamin D3 to vitamin D3 in human skin. J. Biol. Chem. 1993, 268, 14888–14892. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: A millenium perspective. J. Cell. Biochem. 2003, 88, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; MacLaughlin, J.A.; Clark, M.B.; Holick, S.A.; Potts, J.T., Jr.; Anderson, R.R.; Blank, I.H.; Parrish, J.A.; Elias, P. Photosynthesis of previtamin D3 in human skin and the physiologic consequences. Science 1980, 210, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Bikle, D.D. What is new in vitamin D: 2006–2007. Curr. Opin. Rheumatol. 2007, 19, 383–388. [Google Scholar] [CrossRef]
- Cheng, J.B.; Levine, M.A.; Bell, N.H.; Mangelsdorf, D.J.; Russell, D.W. Genetic evidence that the human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc. Natl. Acad. Sci. USA 2004, 101, 7711–7715. [Google Scholar] [CrossRef]
- Fu, G.K.; Lin, D.; Zhang, M.Y.; Bikle, D.D.; Shackleton, C.H.; Miller, W.L.; Portale, A.A. Cloning of human 25-hydroxyvitamin D-1 alpha-hydroxylase and mutations causing vitamin D-dependent rickets type 1. Mol. Endocrinol. 1997, 11, 1961–1970. [Google Scholar] [CrossRef][Green Version]
- Shinki, T.; Shimada, H.; Wakino, S.; Anazawa, H.; Hayashi, M.; Saruta, T.; DeLuca, H.F.; Suda, T. Cloning and expression of rat 25-hydroxyvitamin D3-1alpha-hydroxylase cDNA. Proc. Natl. Acad. Sci. USA 1997, 94, 12920–12925. [Google Scholar] [CrossRef] [PubMed]
- Takeyama, K.; Kitanaka, S.; Sato, T.; Kobori, M.; Yanagisawa, J.; Kato, S. 25-Hydroxyvitamin D3 1alpha-hydroxylase and vitamin D synthesis. Science 1997, 277, 1827–1830. [Google Scholar] [CrossRef] [PubMed]
- Haussler, M.R.; Whitfield, G.K.; Haussler, C.A.; Hsieh, J.C.; Thompson, P.D.; Selznick, S.H.; Dominguez, C.E.; Jurutka, P.W. The nuclear vitamin D receptor: Biological and molecular regulatory properties revealed. J. Bone Miner. Res. 1998, 13, 325–349. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, S.; Na, S.; Rathnachalam, R. Noncalcemic actions of vitamin D receptor ligands. Endocr. Rev. 2005, 26, 662–687. [Google Scholar] [CrossRef]
- Sutton, A.L.; MacDonald, P.N. Vitamin D: More than a “bone-a-fide” hormone. Mol. Endocrinol. 2003, 17, 777–791. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and human health: Lessons from vitamin D receptor null mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef]
- Lips, P.; van Schoor, N.M.; de Jongh, R.T. Diet, sun, and lifestyle as determinants of vitamin D status. Ann. N. Y. Acad. Sci. 2014, 1317, 92–98. [Google Scholar] [CrossRef]
- Sollid, S.T.; Hutchinson, M.Y.; Fuskevag, O.M.; Joakimsen, R.M.; Jorde, R. Large Individual Differences in Serum 25-Hydroxyvitamin D Response to Vitamin D Supplementation: Effects of Genetic Factors, Body Mass Index, and Baseline Concentration. Results from a Randomized Controlled Trial. Horm. Metab. Res. 2016, 48, 27–34. [Google Scholar] [CrossRef]
- Whiting, S.J.; Bonjour, J.P.; Payen, F.D.; Rousseau, B. Moderate amounts of vitamin D3 in supplements are effective in raising serum 25-hydroxyvitamin D from low baseline levels in adults: A systematic review. Nutrients 2015, 7, 2311–2323. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Yalamanchili, V.; Smith, L.M. The effect of vitamin D supplementation on serum 25(OH)D in thin and obese women. J. Steroid Biochem. Mol. Biol. 2013, 136, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Davies, K.M.; Chen, T.C.; Holick, M.F.; Barger-Lux, M.J. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr. 2003, 77, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, A.K.; Singh, R.J.; Noymer, A. Vitamin D (25OHD) Serum Seasonality in the United States. PLoS ONE 2013, 8, e65785. [Google Scholar] [CrossRef]
- Rees, J.R.; Mott, L.A.; Barry, E.L.; Baron, J.A.; Bostick, R.M.; Figueiredo, J.C.; Bresalier, R.S.; Robertson, D.J.; Peacock, J.L. Lifestyle and Other Factors Explain One-Half of the Variability in the Serum 25-Hydroxyvitamin D Response to Cholecalciferol Supplementation in Healthy Adults. J. Nutr. 2016, 146, 2312–2324. [Google Scholar] [CrossRef] [PubMed]
- Viljakainen, H.T.; Palssa, A.; Karkkainen, M.; Jakobsen, J.; Lamberg-Allardt, C. How much vitamin D3 do the elderly need? J. Am. Coll. Nutr. 2006, 25, 429–435. [Google Scholar] [CrossRef]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An updated systematic review and meta-analysis of the efficacy of vitamin D food fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef]
- Bonjour, J.P.; Dontot-Payen, F.; Rouy, E.; Walrand, S.; Rousseau, B. Evolution of Serum 25OHD in Response to Vitamin D(3)-Fortified Yogurts Consumed by Healthy Menopausal Women: A 6-Month Randomized Controlled Trial Assessing the Interactions between Doses, Baseline Vitamin D Status, and Seasonality. J. Am. Coll. Nutr. 2018, 37, 34–43. [Google Scholar] [CrossRef]
- Talwar, S.A.; Aloia, J.F.; Pollack, S.; Yeh, J.K. Dose response to vitamin D supplementation among postmenopausal African American women. Am. J. Clin. Nutr. 2007, 86, 1657–1662. [Google Scholar] [CrossRef]
- Tjellesen, L.; Hummer, L.; Christiansen, C.; Rodbro, P. Serum concentration of vitamin D metabolites during treatment with vitamin D2 and D3 in normal premenopausal women. Bone Miner. 1986, 1, 407–413. [Google Scholar]
- Trang, H.M.; Cole, D.E.; Rubin, L.A.; Pierratos, A.; Siu, S.; Vieth, R. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am. J. Clin. Nutr. 1998, 68, 854–858. [Google Scholar] [CrossRef]
- Armas, L.A.; Hollis, B.W.; Heaney, R.P. Vitamin D2 is much less effective than vitamin D3 in humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hypponen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Mastaglia, S.R.; Mautalen, C.A.; Parisi, M.S.; Oliveri, B. Vitamin D2 dose required to rapidly increase 25OHD levels in osteoporotic women. Eur. J. Clin. Nutr. 2006, 60, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stocklin, E.; Sidelnikov, E.; Willett, W.C.; Edel, J.O.; Stahelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3 versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef]
- Perez-Castrillon, J.L.; Duenas-Laita, A.; Brandi, M.L.; Jodar, E.; Del Pino-Montes, J.; Quesada-Gomez, J.M.; Cereto Castro, F.; Gomez-Alonso, C.; Gallego Lopez, L.; Olmos Martinez, J.M.; et al. Calcifediol is superior to cholecalciferol in improving vitamin D status in postmenopausal women: A randomized trial. J. Bone Miner. Res. 2021, 36, 1967–1978. [Google Scholar] [CrossRef]
- Webb, A.R.; DeCosta, B.R.; Holick, M.F. Sunlight regulates the cutaneous production of vitamin D3 by causing its photodegradation. J. Clin. Endocrinol. Metab. 1989, 68, 882–887. [Google Scholar] [CrossRef]
- Holick, M.F. High prevalence of vitamin D inadequacy and implications for health. Mayo Clin. Proc. 2006, 81, 353–373. [Google Scholar] [CrossRef]
- Signorello, L.B.; Williams, S.M.; Zheng, W.; Smith, J.R.; Long, J.; Cai, Q.; Hargreaves, M.K.; Hollis, B.W.; Blot, W.J. Blood vitamin d levels in relation to genetic estimation of African ancestry. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2325–2331. [Google Scholar] [CrossRef]
- Aloia, J.F.; Talwar, S.A.; Pollack, S.; Yeh, J. A randomized controlled trial of vitamin D3 supplementation in African American women. Arch. Intern. Med. 2005, 165, 1618–1623. [Google Scholar] [CrossRef]
- Aloia, J.F.; Vaswani, A.; Yeh, J.K.; Flaster, E. Risk for osteoporosis in black women. Calcif. Tissue Int. 1996, 59, 415–423. [Google Scholar] [CrossRef]
- Nesby-O’Dell, S.; Scanlon, K.S.; Cogswell, M.E.; Gillespie, C.; Hollis, B.W.; Looker, A.C.; Allen, C.; Doughertly, C.; Gunter, E.W.; Bowman, B.A. Hypovitaminosis D prevalence and determinants among African American and white women of reproductive age: Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Clin. Nutr. 2002, 76, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Siris, E.S.; Wehren, L.E.; Miller, P.D.; Abbott, T.A.; Berger, M.L.; Santora, A.C.; Sherwood, L.M. Osteoporosis and fracture risk in women of different ethnic groups. J. Bone Miner. Res. 2005, 20, 185–194. [Google Scholar] [CrossRef]
- Bryant, R.J.; Wastney, M.E.; Martin, B.R.; Wood, O.; McCabe, G.P.; Morshidi, M.; Smith, D.L.; Peacock, M.; Weaver, C.M. Racial differences in bone turnover and calcium metabolism in adolescent females. J. Clin. Endocrinol. Metab. 2003, 88, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.S. Vitamin D and African Americans. J. Nutr. 2006, 136, 1126–1129. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhao, L.J.; Zhou, Y.; Badr, R.; Watson, P.; Ye, A.; Zhou, B.; Zhang, J.; Deng, H.W.; Recker, R.R.; et al. SNP rs11185644 of RXRA gene is identified for dose-response variability to vitamin D3 supplementation: A randomized clinical trial. Sci. Rep. 2017, 7, 40593. [Google Scholar] [CrossRef] [PubMed]
- Cheema, C.; Grant, B.F.; Marcus, R. Effects of estrogen on circulating “free” and total 1,25-dihydroxyvitamin D and on the parathyroid-vitamin D axis in postmenopausal women. J. Clin. Investig. 1989, 83, 537–542. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Riggs, B.L.; DeLuca, H.F. Effect of estrogen on calcium absorption and serum vitamin D metabolites in postmenopausal osteoporosis. J. Clin. Endocrinol. Metab. 1980, 51, 1359–1364. [Google Scholar] [CrossRef]
- Bikle, D.D.; Halloran, B.P.; Harris, S.T.; Portale, A.A. Progestin antagonism of estrogen stimulated 1,25-dihydroxyvitamin D levels. J. Clin. Endocrinol. Metab. 1992, 75, 519–523. [Google Scholar] [CrossRef][Green Version]
- Prince, R.L. Counterpoint: Estrogen effects on calcitropic hormones and calcium homeostasis. Endocr. Rev. 1994, 15, 301–309. [Google Scholar] [CrossRef]
- Dick, I.M.; Prince, R.L.; Kelly, J.J.; Ho, K.K. Oestrogen effects on calcitriol levels in post-menopausal women: A comparison of oral versus transdermal administration. Clin. Endocrinol. 1995, 43, 219–224. [Google Scholar] [CrossRef]
- Santoro, A.M.; Simpson, C.A.; Cong, E.; Haas, A.; Sullivan, R.R.; Parziale, S.; Deng, Y.; Insogna, K.L. Differing effects of oral conjugated equine estrogen and transdermal estradiol on vitamin D metabolism in postmenopausal women: A 4-year longitudinal study. Menopause 2022, 29, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, I. Recognizing and treating urogenital atrophy in postmenopausal women. J. Womens Health 2010, 19, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.D.; Oliver, R.H.; Leung, B.S.; Lin, L.Y.; Yeh, J. Estrogen receptor alpha and beta expression in the vaginal walls and uterosacral ligaments of premenopausal and postmenopausal women. Fertil. Steril. 1999, 71, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- North American Menopause Society. The role of local vaginal estrogen for treatment of vaginal atrophy in postmenopausal women: 2007 position statement of The North American Menopause Society. Menopause 2007, 14, 355–369. [Google Scholar] [CrossRef]
- Nappi, R.E.; Palacios, S. Impact of vulvovaginal atrophy on sexual health and quality of life at postmenopause. Climacteric 2014, 17, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Costantino, D.; Guaraldi, C. Effectiveness and safety of vaginal suppositories for the treatment of the vaginal atrophy in postmenopausal women: An open, non-controlled clinical trial. Eur. Rev. Med. Pharmacol. Sci. 2008, 12, 411–416. [Google Scholar]
- Kim, G.W.; Jeong, G.W. Menopause-related brain activation patterns during visual sexual arousal in menopausal women: An fMRI pilot study using time-course analysis. Neuroscience 2017, 343, 449–458. [Google Scholar] [CrossRef]
- Avis, N.E.; Stellato, R.; Crawford, S.; Johannes, C.; Longcope, C. Is there an association between menopause status and sexual functioning? Menopause 2000, 7, 297–309. [Google Scholar] [CrossRef]
- Dennerstein, L.; Dudley, E.; Burger, H. Are changes in sexual functioning during midlife due to aging or menopause? Fertil. Steril. 2001, 76, 456–460. [Google Scholar] [CrossRef]
- Nappi, R.E.; Nijland, E.A. Women’s perception of sexuality around the menopause: Outcomes of a European telephone survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 137, 10–16. [Google Scholar] [CrossRef]
- Altoparlak, U.; Kadanali, A.; Kadanali, S. Correlation of urinary tract infections with the vaginal colonization in postmenopausal women. Mikrobiyol. Bul. 2004, 38, 377–383. [Google Scholar] [PubMed]
- Luthje, P.; Brauner, H.; Ramos, N.L.; Ovregaard, A.; Glaser, R.; Hirschberg, A.L.; Aspenstrom, P.; Brauner, A. Estrogen supports urothelial defense mechanisms. Sci. Transl. Med. 2013, 5, 190ra180. [Google Scholar] [CrossRef] [PubMed]
- Pabich, W.L.; Fihn, S.D.; Stamm, W.E.; Scholes, D.; Boyko, E.J.; Gupta, K. Prevalence and determinants of vaginal flora alterations in postmenopausal women. J. Infect. Dis. 2003, 188, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Raz, R.; Stamm, W.E. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N. Engl. J. Med. 1993, 329, 753–756. [Google Scholar] [CrossRef]
- Cellai, I.; Di Stasi, V.; Comeglio, P.; Maseroli, E.; Todisco, T.; Corno, C.; Filippi, S.; Cipriani, S.; Sorbi, F.; Fambrini, M.; et al. Insight on the Intracrinology of Menopause: Androgen Production within the Human Vagina. Endocrinology 2021, 162, bqaa219. [Google Scholar] [CrossRef]
- Scavello, I.; Maseroli, E.; Di Stasi, V.; Vignozzi, L. Sexual Health in Menopause. Medicina 2019, 55, 559. [Google Scholar] [CrossRef]
- Archer, D.F.; Labrie, F.; Bouchard, C.; Portman, D.J.; Koltun, W.; Cusan, L.; Labrie, C.; Cote, I.; Lavoie, L.; Martel, C.; et al. Treatment of pain at sexual activity (dyspareunia) with intravaginal dehydroepiandrosterone (prasterone). Menopause 2015, 22, 950–963. [Google Scholar] [CrossRef]
- Palacios, S.; Mejia, A.; Neyro, J.L. Treatment of the genitourinary syndrome of menopause. Climacteric 2015, 18 (Suppl. S1), 23–29. [Google Scholar] [CrossRef]
- Baber, R.J.; Panay, N.; Fenton, A.; Group, I.M.S.W. 2016 IMS Recommendations on women’s midlife health and menopause hormone therapy. Climacteric 2016, 19, 109–150. [Google Scholar] [CrossRef]
- North American Menopause Society. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause 2017, 24, 728–753. [Google Scholar] [CrossRef]
- Goldstajn, M.S.; Mikus, M.; Ferrari, F.A.; Bosco, M.; Uccella, S.; Noventa, M.; Torok, P.; Terzic, S.; Lagana, A.S.; Garzon, S. Effects of transdermal versus oral hormone replacement therapy in postmenopause: A systematic review. Arch. Gynecol. Obstet. 2023, 307, 1727–1745. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Baena, M.T.; Perez-Roncero, G.R.; Perez-Lopez, F.R.; Mezones-Holguin, E.; Chedraui, P. Vitamin D, menopause, and aging: Quo vadis? Climacteric 2020, 23, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Delle Monache, S.; Di Fulvio, P.; Iannetti, E.; Valerii, L.; Capone, L.; Nespoli, M.G.; Bologna, M.; Angelucci, A. Body mass index represents a good predictor of vitamin D status in women independently from age. Clin. Nutr. 2019, 38, 829–834. [Google Scholar] [CrossRef]
- Feghaly, J.; Johnson, P.; Kalhan, A. Vitamin D and obesity in adults: A pathophysiological and clinical update. Br. J. Hosp. Med. 2020, 81, 1–5. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Ruban, K.; Bellen, G.; Grinceviciene, S. Pharmacotherapy for the treatment of vaginal atrophy. Expert Opin Pharmacother. 2019, 20, 821–835. [Google Scholar] [CrossRef]
- Duque, G.; El Abdaimi, K.; Macoritto, M.; Miller, M.M.; Kremer, R. Estrogens (E2) regulate expression and response of 1,25-dihydroxyvitamin D3 receptors in bone cells: Changes with aging and hormone deprivation. Biochem. Biophys. Res. Commun. 2002, 299, 446–454. [Google Scholar] [CrossRef]
- Abban, G.; Yildirim, N.B.; Jetten, A.M. Regulation of the vitamin D receptor and cornifin beta expression in vaginal epithelium of the rats through vitamin D3. Eur. J. Histochem. 2008, 52, 107–114. [Google Scholar] [CrossRef]
- Bikle, D.; Teichert, A.; Hawker, N.; Xie, Z.; Oda, Y. Sequential regulation of keratinocyte differentiation by 1,25(OH)2D3, VDR, and its coregulators. J. Steroid Biochem. Mol. Biol. 2007, 103, 396–404. [Google Scholar] [CrossRef]
- Fadiel, A.; Lee, H.H.; Demir, N.; Richman, S.; Iwasaki, A.; Connell, K.; Naftolin, F. Ezrin is a key element in the human vagina. Maturitas 2008, 60, 31–41. [Google Scholar] [CrossRef]
- Carranza-Lira, S.; Amador-Perez, C.; Macgregor-Gooch, A.L.; Estrada-Moscoso, I. Changes in maturation index and vaginal dryness in postmenopausal women who use or not calcitriol. Rev. Med. Inst. Mex. Seguro Soc. 2012, 50, 537–540. [Google Scholar]
- Radnia, N.; Hosseini, S.T.; Vafaei, S.Y.; Pirdehghan, A.; Mehrabadi, N.L. The effect of conjugated estrogens vaginal cream and a combined vaginal cream of vitamins D and E in the treatment of genitourinary syndrome. J. Fam. Med. Prim. Care 2023, 12, 507–516. [Google Scholar] [CrossRef]
- Porterfield, L.; Wur, N.; Delgado, Z.S.; Syed, F.; Song, A.; Weller, S.C. Vaginal Vitamin E for Treatment of Genitourinary Syndrome of Menopause: A Systematic Review of Randomized Controlled Trials. J. Menopausal. Med. 2022, 28, 9–16. [Google Scholar] [CrossRef]
- Hillier, S.L.; Lau, R.J. Vaginal microflora in postmenopausal women who have not received estrogen replacement therapy. Clin. Infect. Dis. 1997, 25 (Suppl. S2), S123–S126. [Google Scholar] [CrossRef] [PubMed]
- Cauci, S.; Driussi, S.; De Santo, D.; Penacchioni, P.; Iannicelli, T.; Lanzafame, P.; De Seta, F.; Quadrifoglio, F.; de Aloysio, D.; Guaschino, S. Prevalence of bacterial vaginosis and vaginal flora changes in peri- and postmenopausal women. J. Clin. Microbiol. 2002, 40, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Dennerstein, G.J.; Ellis, D.H. Oestrogen, glycogen and vaginal candidiasis. Aust. N. Z. J. Obstet. Gynaecol. 2001, 41, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kumar, N.; Singhal, N.; Kaur, R.; Manektala, U. Vaginal microflora in postmenopausal women on hormone replacement therapy. Indian J. Pathol. Microbiol. 2006, 49, 457–461. [Google Scholar]
- Fischer, G.; Bradford, J. Vulvovaginal candidiasis in postmenopausal women: The role of hormone replacement therapy. J. Low. Genit. Tract. Dis. 2011, 15, 263–267. [Google Scholar] [CrossRef]
- Tarry, W.; Fisher, M.; Shen, S.; Mawhinney, M. Candida albicans: The estrogen target for vaginal colonization. J. Surg. Res. 2005, 129, 278–282. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Krohn, M.A.; Simhan, H.N. Maternal vitamin D deficiency is associated with bacterial vaginosis in the first trimester of pregnancy. J. Nutr. 2009, 139, 1157–1161. [Google Scholar] [CrossRef]
- Kaur, H.; Bala, R.; Nagpal, M. Role of Vitamin D in urogenital health of geriatric participants. J. Midlife Health 2017, 8, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Ginkel, P.D.; Soper, D.E.; Bump, R.C.; Dalton, H.P. Vaginal flora in postmenopausal women: The effect of estrogen replacement. Infect. Dis. Obstet. Gynecol. 1993, 1, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Krysiak, R.; Gilowska, M.; Okopien, B. Sexual function and depressive symptoms in young women with low vitamin D status: A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 204, 108–112. [Google Scholar] [CrossRef]
- Inal, Z.O.; Inal, H.A.; Gorkem, U. Sexual function and depressive symptoms in primary infertile women with vitamin D deficiency undergoing IVF treatment. Taiwan J. Obstet. Gynecol. 2020, 59, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Caruso, S.; Rapisarda, A.M.C.; Cianci, S.; Cianci, A. Isoflavones, calcium, vitamin D and inulin improve quality of life, sexual function, body composition and metabolic parameters in menopausal women: Result from a prospective, randomized, placebo-controlled, parallel-group study. Prz. Menopauzalny 2018, 17, 32–38. [Google Scholar] [CrossRef]
- Provvedini, D.M.; Tsoukas, C.D.; Deftos, L.J.; Manolagas, S.C. 1,25-dihydroxyvitamin D3 receptors in human leukocytes. Science 1983, 221, 1181–1183. [Google Scholar] [CrossRef]
- Adorini, L.; Giarratana, N.; Penna, G. Pharmacological induction of tolerogenic dendritic cells and regulatory T cells. Semin. Immunol. 2004, 16, 127–134. [Google Scholar] [CrossRef]
- Wang, T.T.; Nestel, F.P.; Bourdeau, V.; Nagai, Y.; Wang, Q.; Liao, J.; Tavera-Mendoza, L.; Lin, R.; Hanrahan, J.W.; Mader, S.; et al. Cutting edge: 1,25-dihydroxyvitamin D3 is a direct inducer of antimicrobial peptide gene expression. J. Immunol. 2004, 173, 2909–2912. [Google Scholar] [CrossRef]
- Tian, H.; Miao, J.; Zhang, F.; Xiong, F.; Zhu, F.; Li, J.; Wang, X.; Chen, S.; Chen, J.; Huang, N.; et al. Non-histone nuclear protein HMGN2 differently regulates the urothelium barrier function by altering expression of antimicrobial peptides and tight junction protein genes in UPEC J96-infected bladder epithelial cell monolayer. Acta Biochim. Pol. 2018, 65, 93–100. [Google Scholar] [CrossRef]
- Sayeed, I.; Turan, N.; Stein, D.G.; Wali, B. Vitamin D deficiency increases blood-brain barrier dysfunction after ischemic stroke in male rats. Exp. Neurol. 2019, 312, 63–71. [Google Scholar] [CrossRef]
- Won, S.; Sayeed, I.; Peterson, B.L.; Wali, B.; Kahn, J.S.; Stein, D.G. Vitamin D prevents hypoxia/reoxygenation-induced blood-brain barrier disruption via vitamin D receptor-mediated NF-kB signaling pathways. PLoS ONE 2015, 10, e0122821. [Google Scholar] [CrossRef] [PubMed]
- Alperin, M.; Burnett, L.; Lukacz, E.; Brubaker, L. The mysteries of menopause and urogynecologic health: Clinical and scientific gaps. Menopause 2019, 26, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, Z.; He, X.; Liu, Z.; Shen, L.; Long, C.; Wei, G.; Liu, X.; Guo, C. Vitamin D levels and the risk of overactive bladder: A systematic review and meta-analysis. Nutr. Rev. 2023, nuad049. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Uebbing, C.; Schlett, S.; Craiut, D.; Bumbu, G. Stage I and II Stress Incontinence (SIC): High dosed vitamin D may improve effects of local estriol. Dermato-Endocrinology 2016, 8, e1079359. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dallosso, H.M.; McGrother, C.W.; Matthews, R.J.; Donaldson, M.M.; Leicestershire, M.R.C.I.S.G. Nutrient composition of the diet and the development of overactive bladder: A longitudinal study in women. Neurourol. Urodyn. 2004, 23, 204–210. [Google Scholar] [CrossRef]
- Arjmand, M.; Abbasi, H.; Behforouz, A. The effect of vitamin D on urgent urinary incontinence in postmenopausal women. Int. Urogynecol. J. 2023, 34, 1955–1960. [Google Scholar] [CrossRef] [PubMed]
- Brannon-Peppas, L. Novel vaginal drug release applications. Adv. Drug Deliv. Rev. 1993, 11, 169–177. [Google Scholar] [CrossRef]
- Van der Straten, A.; Stadler, J.; Montgomery, E.; Hartmann, M.; Magazi, B.; Mathebula, F.; Schwartz, K.; Laborde, N.; Soto-Torres, L. Women’s experiences with oral and vaginal pre-exposure prophylaxis: The VOICE-C qualitative study in Johannesburg, South Africa. PLoS ONE 2014, 9, e89118. [Google Scholar] [CrossRef]
- Garg, S.; Tambwekar, K.R.; Vermani, K.; Kandarapu, R.; Garg, A.; Waller, D.P.; Zaneveld, L.J. Development pharmaceutics of microbicide formulations. Part II: Formulation, evaluation, and challenges. AIDS Patient Care STDS 2003, 17, 377–399. [Google Scholar] [CrossRef]
- Hull, T.; Hilber, A.M.; Chersich, M.F.; Bagnol, B.; Prohmmo, A.; Smit, J.A.; Widyantoro, N.; Utomo, I.D.; Francois, I.; Tumwesigye, N.M.; et al. Prevalence, motivations, and adverse effects of vaginal practices in Africa and Asia: Findings from a multicountry household survey. J. Womens Health 2011, 20, 1097–1109. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassanein, M.M.; Huri, H.Z.; Abduelkarem, A.R.; Baig, K. Therapeutic Effects of Vitamin D on Vaginal, Sexual, and Urological Functions in Postmenopausal Women. Nutrients 2023, 15, 3804. https://doi.org/10.3390/nu15173804
Hassanein MM, Huri HZ, Abduelkarem AR, Baig K. Therapeutic Effects of Vitamin D on Vaginal, Sexual, and Urological Functions in Postmenopausal Women. Nutrients. 2023; 15(17):3804. https://doi.org/10.3390/nu15173804
Chicago/Turabian StyleHassanein, Mohammed M., Hasniza Zaman Huri, Abduelmula R. Abduelkarem, and Kauser Baig. 2023. "Therapeutic Effects of Vitamin D on Vaginal, Sexual, and Urological Functions in Postmenopausal Women" Nutrients 15, no. 17: 3804. https://doi.org/10.3390/nu15173804
APA StyleHassanein, M. M., Huri, H. Z., Abduelkarem, A. R., & Baig, K. (2023). Therapeutic Effects of Vitamin D on Vaginal, Sexual, and Urological Functions in Postmenopausal Women. Nutrients, 15(17), 3804. https://doi.org/10.3390/nu15173804