

Antihypertensive Effects of an Optimized Aged Garlic Extract in Subjects with Grade I Hypertension and Antihypertensive Drug Therapy: A Randomized, Triple-Blind Controlled Trial
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Intervention
2.3. Study Population
2.4. Sample Size Determination
2.5. Outcomes
2.5.1. Blood Pressure
2.5.2. Endothelial Function
2.5.3. Nitric Oxide
2.5.4. Antioxidant Capacity
2.5.5. Inflammatory Cytokines
2.5.6. Angiotensin-Converting Enzyme (ACE) Activity
2.5.7. Statistical Analysis
3. Results
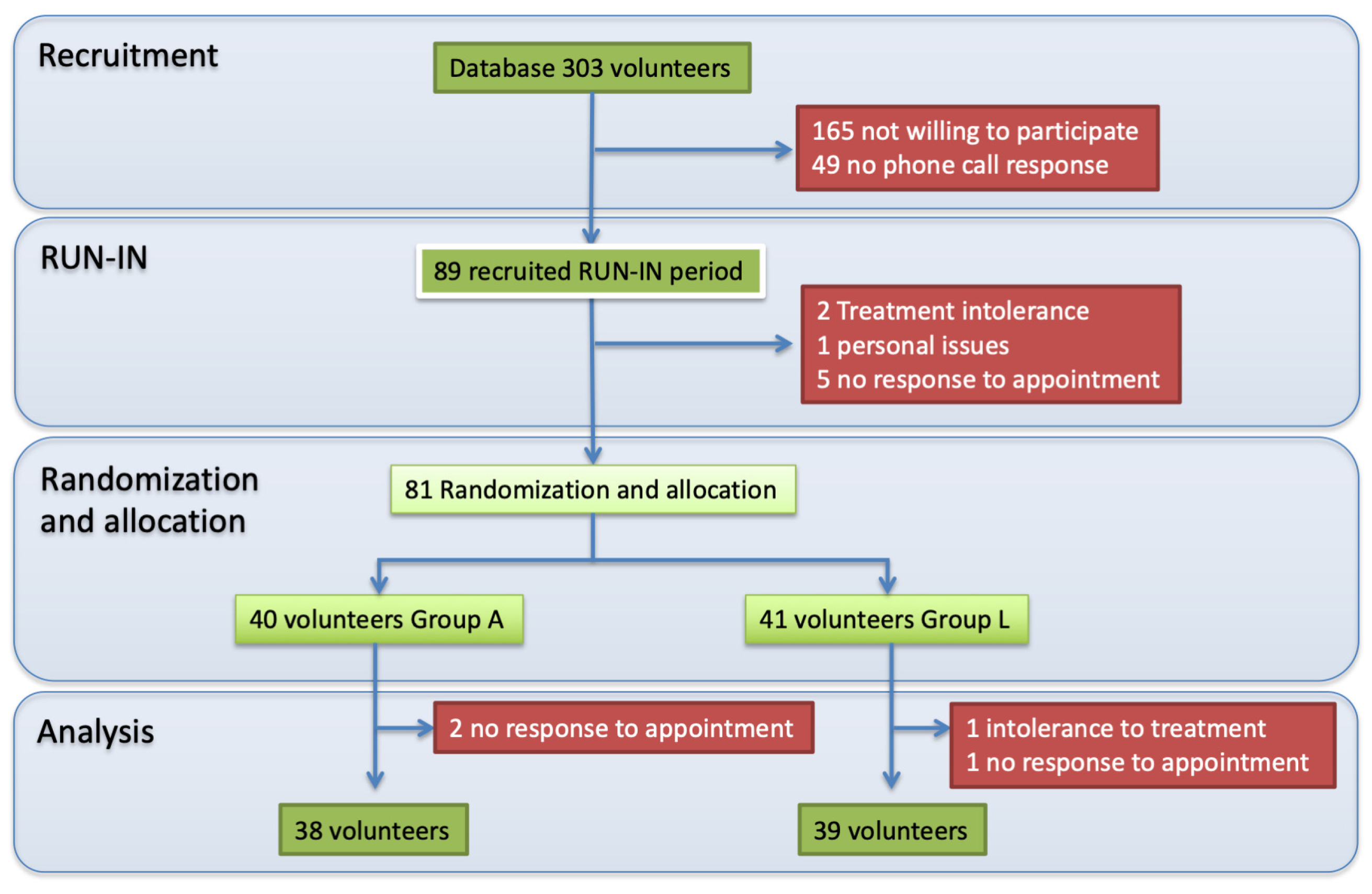
3.1. Study Design
3.2. Compliance and Reported Adverse Events
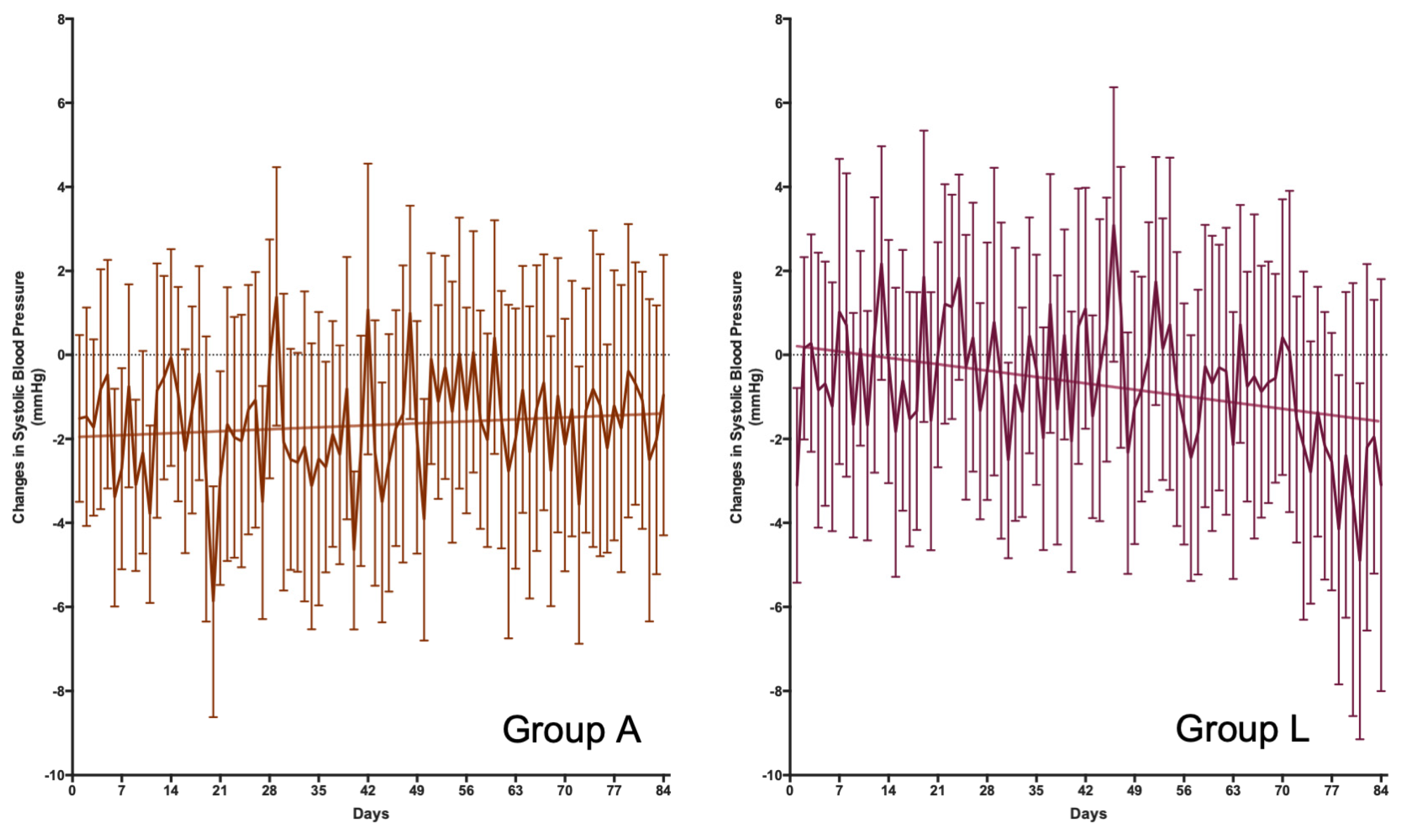
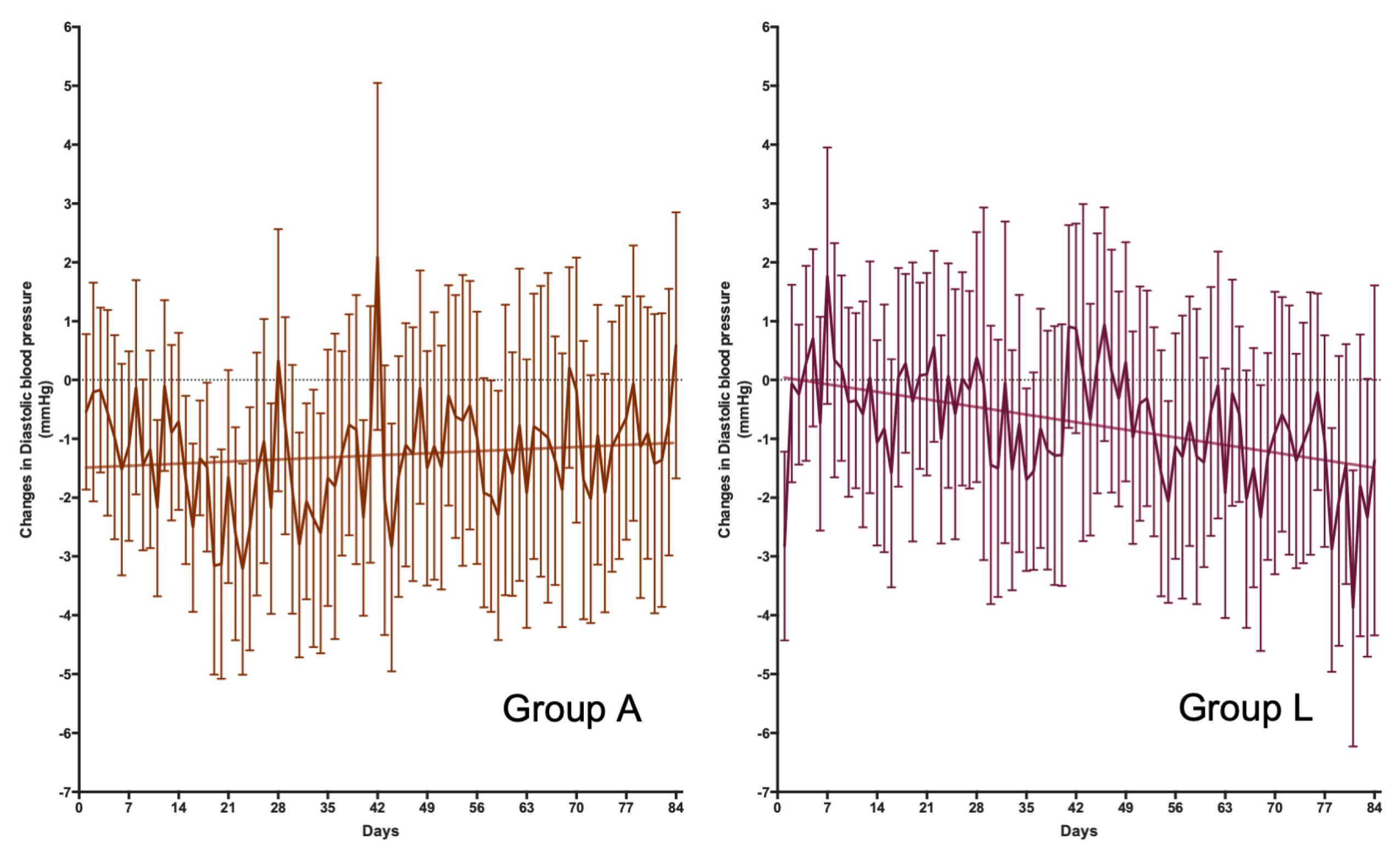
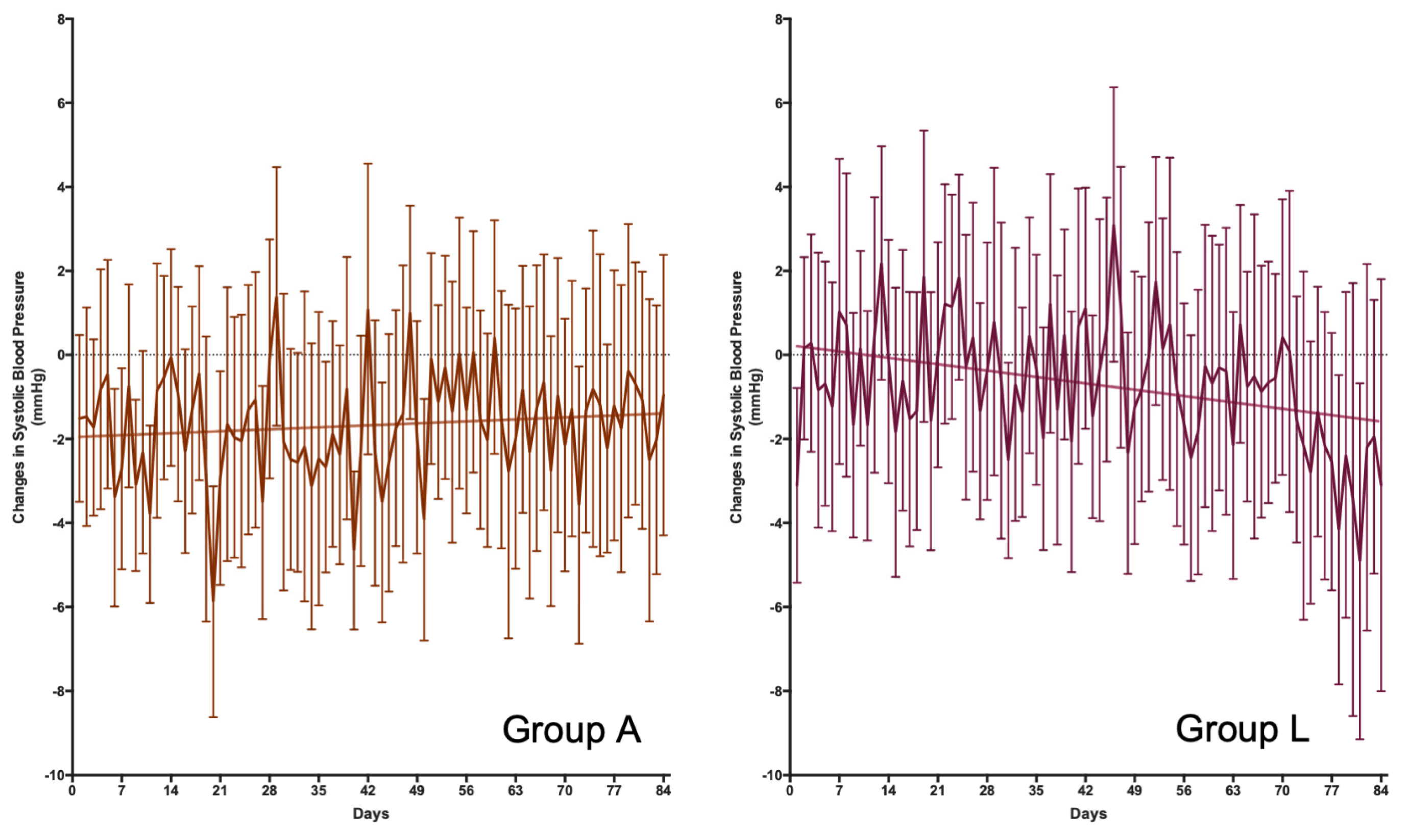
3.3. Blood Pressure, Endothelial Function, and Related Variables
3.4. Confounding Variables Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood Pressure Lowering for Prevention of Cardiovascular Disease and Death: A Systematic Review and Meta-Analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R.; et al. Prevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High-, Middle-, and Low-Income Countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Lamirault, G.; Artifoni, M.; Daniel, M.; Barber-Chamoux, N.; Nantes University Hospital Working Group on Hypertension. Resistant Hypertension: Novel Insights. Curr. Hypertens. Rev. 2020, 16, 61–72. [Google Scholar] [CrossRef]
- Borghi, C.; Cicero, A.F.G. Nutraceuticals with a Clinically Detectable Blood Pressure-Lowering Effect: A Review of Available Randomized Clinical Trials and Their Meta-Analyses. Br. J. Clin. Pharmacol. 2017, 83, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Prieto, M.A.; Miatello, R.M. Organosulfur Compounds and Cardiovascular Disease. Mol. Aspects Med. 2010, 31, 540–545. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Hecker, K.D.; Bonanome, A.; Coval, S.M.; Binkoski, A.E.; Hilpert, K.F.; Griel, A.E.; Etherton, T.D. Bioactive Compounds in Foods: Their Role in Preventing Cardiovascular Disease and Cancer. Am. J. Med. 2002, 113, 71–88. [Google Scholar] [CrossRef]
- Ried, K. Garlic Lowers Blood Pressure in Hypertensive Individuals, Regulates Serum Cholesterol, and Stimulates Immunity: An Updated Meta-Analysis and Review. J. Nutr. 2016, 146, 389S–396S. [Google Scholar] [CrossRef]
- Piragine, E.; Citi, V.; Lawson, K.; Calderone, V.; Martelli, A. Regulation of Blood Pressure by Natural Sulfur Compounds: Focus on Their Mechanisms of Action. Biochem. Pharmacol. 2022, 206, 115302. [Google Scholar] [CrossRef]
- Recinella, L.; Chiavaroli, A.; Masciulli, F.; Fraschetti, C.; Filippi, A.; Cesa, S.; Cairone, F.; Gorica, E.; De Leo, M.; Braca, A.; et al. Protective Effects Induced by a Hydroalcoholic Allium sativum Extract in Isolated Mouse Heart. Nutrients 2021, 13, 2332. [Google Scholar] [CrossRef]
- Recinella, L.; Gorica, E.; Chiavaroli, A.; Fraschetti, C.; Filippi, A.; Cesa, S.; Cairone, F.; Martelli, A.; Calderone, V.; Veschi, S.; et al. Anti-Inflammatory and Antioxidant Effects Induced by Allium sativum L. Extracts on an Ex Vivo Experimental Model of Ulcerative Colitis. Foods 2022, 11, 3559. [Google Scholar] [CrossRef] [PubMed]
- García-Villalón, A.L.; Amor, S.; Monge, L.; Fernández, N.; Prodanov, M.; Muñoz, M.; Inarejos-García, A.M.; Granado, M. In Vitro Studies of an Aged Black Garlic Extract Enriched in S-Allylcysteine and Polyphenols with Cardioprotective Effects. J. Funct. Foods 2016, 27, 189–200. [Google Scholar] [CrossRef]
- Lu, X.; Li, N.; Qiao, X.; Qiu, Z.; Liu, P. Composition Analysis and Antioxidant Properties of Black Garlic Extract. J. Food Drug Anal. 2017, 25, 340–349. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, G.; Cong, X.; Wen, C. Black Garlic Improves Heart Function in Patients With Coronary Heart Disease by Improving Circulating Antioxidant Levels. Front. Physiol. 2018, 9, 1435. [Google Scholar] [CrossRef]
- Czompa, A.; Szoke, K.; Prokisch, J.; Gyongyosi, A.; Bak, I.; Balla, G.; Tosaki, A.; Lekli, I. Aged (Black) versus Raw Garlic against Ischemia/Reperfusion-Induced Cardiac Complications. Int. J. Mol. Sci. 2018, 19, 1017. [Google Scholar] [CrossRef] [PubMed]
- Groenland, E.H.; Bots, M.L.; Visseren, F.L.J.; McManus, R.J.; Spiering, W. Number of Measurement Days Needed for Obtaining a Reliable Estimate of Home Blood Pressure and Hypertension Status. Blood Press. 2022, 31, 100–108. [Google Scholar] [CrossRef]
- Ried, K. Garlic Lowers Blood Pressure in Hypertensive Subjects, Improves Arterial Stiffness and Gut Microbiota: A Review and Meta-Analysis. Exp. Ther. Med. 2020, 19, 1472–1478. [Google Scholar] [CrossRef]
- Wang, H.P.; Yang, J.; Qin, L.Q.; Yang, X.J. Effect of Garlic on Blood Pressure: A Meta-Analysis. J. Clin. Hypertens. 2015, 17, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Howard, S.C.; Dolan, E.; O’Brien, E.; Dobson, J.E.; Dahlöf, B.; Sever, P.S.; Poulter, N.R. Prognostic Significance of Visit-to-Visit Variability, Maximum Systolic Blood Pressure, and Episodic Hypertension. Lancet 2010, 375, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.J.; Wang, P.Q.; Li, S.J.; Li, X.K.; Zhang, Y.Q.; Wang, J. Garlic for Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytomedicine 2015, 22, 352–361. [Google Scholar] [CrossRef]
- Nakasone, Y.; Nakamura, Y.; Yamamoto, T.; Yamaguchi, H. Effect of a Traditional Japanese Garlic Preparation on Blood Pressure in Prehypertensive and Mildly Hypertensive Adults. Exp. Ther. Med. 2013, 5, 399–405. [Google Scholar] [CrossRef]
- Borrelli, F.; Capasso, R.; Izzo, A.A. Garlic (Allium sativum L.): Adverse Effects and Drug Interactions in Humans. Mol. Nutr. Food Res. 2007, 51, 1386–1397. [Google Scholar] [CrossRef] [PubMed]
- Vaes, L.P.J.; Chyka, P.A. Interactions of Warfarin with Garlic, Ginger, Ginkgo, or Ginseng: Nature of the Evidence. Ann. Pharmacother. 2000, 34, 1478–1482. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Kang, D. Physicochemical Properties, Biological Activity, Health Benefits, and General Limitations of Aged Black Garlic: A Review. Molecules 2017, 22, 919. [Google Scholar] [CrossRef]
- Pamukcu, B.; Lip, G.Y.H.; Snezhitskiy, V.; Shantsila, E. The CD40-CD40L System in Cardiovascular Disease. Ann. Med. 2011, 43, 331–340. [Google Scholar] [CrossRef]
- Bliziotis, I.A.; Destounis, A.; Stergiou, G.S. Home versus Ambulatory and Office Blood Pressure in Predicting Target Organ Damage in Hypertension: A Systematic Review and Meta-Analysis. J. Hypertens. 2012, 30, 1289–1299. [Google Scholar] [CrossRef]
- Canoy, D.; Nazarzadeh, M.; Copland, E.; Bidel, Z.; Rao, S.; Li, Y.; Rahimi, K. How Much Lowering of Blood Pressure Is Required to Prevent Cardiovascular Disease in Patients With and Without Previous Cardiovascular Disease? Curr. Cardiol. Rep. 2022, 24, 851. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-Specific Relevance of Usual Blood Pressure to Vascular Mortality: A Meta-Analysis of Individual Data for One Million Adults in 61 Prospective Studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Valls, R.M.; Companys, J.; Calderón-Pérez, L.; Salamanca, P.; Pla-Pagà, L.; Sandoval-Ramírez, B.A.; Bueno, A.; Puzo, J.; Crescenti, A.; Del Bas, J.M.; et al. Effects of an Optimized Aged Garlic Extract on Cardiovascular Disease Risk Factors in Moderate Hypercholesterolemic Subjects: A Randomized, Crossover, Double-Blind, Sustainedand Controlled Study. Nutrients 2022, 14, 405. [Google Scholar] [CrossRef]
- Baik, J.S.; Min, J.H.; Ju, S.M.; Ahn, J.H.; Ko, S.H.; Chon, H.S.; Kim, M.S.; Shin, Y. Il Effects of Fermented Garlic Extract Containing Nitric Oxide Metabolites on Blood Flow in Healthy Participants: A Randomized Controlled Trial. Nutrients 2022, 14, 5238. [Google Scholar] [CrossRef]
- Leitão, R.; de Oliveira, G.V.; Rezende, C.; Volino-Souza, M.; Mesquita, J.; de Carvalho, L.L.; Alvares, T.S. Improved Microvascular Reactivity after Aged Garlic Extract Intake Is Not Mediated by Hydrogen Sulfide in Older Adults at Risk for Cardiovascular Disease: A Randomized Clinical Trial. Eur. J. Nutr. 2022, 61, 3357–3366. [Google Scholar] [CrossRef]
- Gruenwald, J.; Bongartz, U.; Bothe, G.; Uebelhack, R. Effects of Aged Garlic Extract on Arterial Elasticity in a Placebo-Controlled Clinical Trial Using EndoPATTM Technology. Exp. Ther. Med. 2020, 19, 1490–1499. [Google Scholar] [CrossRef]
- Kim, D.G.; Kang, M.J.; Hong, S.S.; Choi, Y.H.; Shin, J.H. Antiinflammatory Effects of Functionally Active Compounds Isolated from Aged Black Garlic. Phytother. Res. 2017, 31, 53–61. [Google Scholar] [CrossRef]
- Kim, H.O.; Kim, H.S.; Youn, J.C.; Shin, E.C.; Park, S. Serum Cytokine Profiles in Healthy Young and Elderly Population Assessed Using Multiplexed Bead-Based Immunoassays. J. Transl. Med. 2011, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Paz, M.A.; De-La-Sierra, A.; Sáez, M.; Barceló, M.A.; Rodríguez, J.J.; Castro, S.; Lagarón, C.; Garrido, J.M.; Vera, P.; Coll-De-Tuero, G. Treatment Efficacy of Anti-Hypertensive Drugs in Monotherapy or Combination: ATOM Systematic Review and Meta-Analysis of Randomized Clinical Trials According to PRISMA Statement. Medicine 2016, 95, e4071. [Google Scholar] [CrossRef]
- Shouk, R.; Abdou, A.; Shetty, K.; Sarkar, D.; Eid, A.H. Mechanisms Underlying the Antihypertensive Effects of Garlic Bioactives. Nutr. Res. 2014, 34, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Smolensky, M.H.; Hermida, R.C.; Ayala, D.E.; Tiseo, R.; Portaluppi, F. Administration-Time-Dependent Effects of Blood Pressure-Lowering Medications: Basis for the Chronotherapy of Hypertension. Blood Press. Monit. 2010, 15, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Frank, O.R.; Stocks, N.P. Aged Garlic Extract Reduces Blood Pressure in Hypertensives: A Dose-Response Trial. Eur. J. Clin. Nutr. 2013, 67, 64–70. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Group A Placebo (mg per Tablet) | Group L ABG Extract (mg per Tablet) | |
|---|---|---|
| ABG extract | - | 250 |
| Maltodextrin | 250 | - |
| Microcrystalline cellulose | 90 | 90 |
| Dicalcic phosphate | 157 | 157 |
| Sodium croscarmellose | 10 | 10 |
| Magnesium stearate | 7 | 7 |
| Sodium Alginate | 3.06 | 3.06 |
| Stearic acid | 0.03 | 0.03 |
| Oleic acid | 1.54 | 1.54 |
| Medium-chain triglycerides | 2.80 | 2.80 |
| Ethylcellulose | 13.17 | 13.17 |
| Hydroxypropyl methylcellulose | 4.86 | 4.86 |
| Hydroxypropyl cellulose | 4.86 | 4.86 |
| Talc | 2.88 | 2.88 |
| Titanium oxide | 1.80 | 1.80 |
| Garlic flavor | 1.00 | 1.00 |
| Group A (Placebo) | Group L (ABG Extract) | p-Value | |
|---|---|---|---|
| No. of volunteers | 38 | 39 | |
| Gender | Male: 20; Female: 18 | Male: 20; Female 19 | 0.9057 |
| Age (years) | 64.1 ± 5.9 | 63.7 ± 5.8 | 0.8018 |
| Systolic blood pressure (mmHg) | 145.5 ± 17.2 | 148.8 ± 22.9 | 0.4876 |
| Diastolic blood pressure (mmHg) | 85.3 ± 10.8 | 85.7 ± 11.2 | 0.8765 |
| Pulse pressure (mmHg) | 60.0 ± 12.9 | 62.7 ± 15.7 | 0.4300 |
| Years of diagnosis | 15.4 ± 8.5 | 14.8 ± 11.2 | 0.8192 |
| Antihypertensive drug number | |||
| 1 type | 13 | 13 | 0.6219 |
| Two types | 13 | 10 | |
| Three or more types | 12 | 16 | |
| Antihypertensive drug type | |||
| Thiazides | 25 | 27 | 0.9811 |
| β-blockers | 11 | 14 | |
| Angiotensin II receptor blocker | 15 | 16 | |
| Calcium channel blockers | 14 | 17 | |
| Other types of drugs | |||
| Statins | 15 | 17 | 0.7826 |
| Benzodiazepines | 10 | 9 | |
| Anticoagulants | 8 | 10 | |
| Proton pump inhibitors | 12 | 8 | |
| Nonsteroidal anti-inflammatory drug | 14 | 10 | |
| Antidiabetic | 2 | 4 | |
| Treatment adherence | 96.7 ± 4.7 | 97.8 ± 6.8 | 0.4396 |
| Minimum | 85% | 72% | |
| Maximum | 108% | 112% | |
| Treatment blinding | |||
| Yes/No | 17/21 | 9/30 | 0.0559 |
| Group A (Placebo) (n = 38) | Group L (ABG Extract) (n = 39) | ||||||
|---|---|---|---|---|---|---|---|
| Basal | 12 Weeks | Sidak’s p-Value | Basal | 12 Weeks | Sidak’s p-Value | Two-Way ANOVA p-Value | |
| Blood pressure (office) | |||||||
| Systolic (mmHg) | 144 ± 13 | 138 ± 14 | 0.0169 | 146 ± 21 | 143 ± 18 | 0.3011 | 0.3011 |
| Diastolic (mmHg) | 85 ± 7 | 83 ± 10 | 0.2497 | 85 ± 10 | 83 ± 9 | 0.2889 | 0.9219 |
| Pulse pressure (mmHg) | 59 ± 12 | 55 ± 14 | 0.0632 | 61 ± 16 | 60 ± 14 | 0.6126 | 0.2011 |
| Endothelial function | |||||||
| RHI | 2.059 ± 0.414 | 2.033 ± 0.597 | 0.9583 | 2.016 ± 0.569 | 2.068 ± 0.728 | 0.8276 | 0.9753 |
| AI75 | 30.4 ± 14.9 | 26.7 ± 17.2 | 0.1767 | 25.0 ± 17.0 | 21.1 ± 15.1 | 0.1139 | 0.1185 |
| Blood lipid profile | |||||||
| Total cholesterol (mg/dL) | 188 ± 43 | 188 ± 43 | >0.9999 | 209 ± 40 | 209 ± 39 | 0.9984 | 0.9759 |
| Triacylglycerides (mg/dL) | 107 ± 53 | 107 ± 55 | 0.9986 | 122 ± 53 | 117 ± 43 | 0.8725 | 0.1394 |
| HDL-cholesterol (mg/dL) | 58 ± 15 | 58 ± 15 | 0.9939 | 59 ± 17 | 61 ± 21 | 0.8892 | 0.4172 |
| Inflammatory cytokines | |||||||
| IL-2 (pg/mL) | 0.190 ± 0.657 | 0.223 ± 0.790 | 0.9021 | 0.894 ± 1.844 | 1.022 ± 2.043 | 0.2236 | 0.0282 |
| IL-4 (pg/mL) | 113 ± 541 | 121 ± 566 | 0.4704 | 213 ± 708 | 215 ± 705 | 0.9556 | 0.5079 |
| IL-5 (pg/mL) | 3.8 ± 10.5 | 3.6 ± 10.4 | 0.8234 | 6.4 ± 16.1 | 6.5 ± 16.0 | 0.9021 | 0.3859 |
| IL-8 (pg/mL) | 20.0 ± 29.8 | 21.6 ± 33.7 | 0.2054 | 25.0 ± 31.6 | 26.7 ± 33.0 | 0.2018 | 0.4948 |
| IP-10 (pg/mL) | 490 ± 252 | 446 ± 231 | 0.3753 | 450 ± 202 | 539 ± 332 | 0.0218 | 0.6238 |
| sCD40L (pg/mL) | 3856 ± 3927 | 2322 ± 2512 | 0.0543 | 3742 ± 3001 | 3211 ± 3337 | 0.6710 | 0.4978 |
| Other variables | |||||||
| Nitric oxide (µM) | 88 ± 23 | 90 ± 27 | 0.9188 | 87 ± 19 | 97 ± 31 | 0.0254 | 0.5101 |
| ACE activity (U/L) | 78 ± 44 | 71 ± 41 | 0.1495 | 78 ± 40 | 69 ± 38 | 0.0398 | 0.9560 |
| Uric acid (mg/dL) | 5.6 ± 1.4 | 5.6 ± 1.3 | 0.9987 | 6.0 ± 1.4 | 5.7 ± 1.3 | 0.0483 | 0.3986 |
| FRAP (µM TE/min) | 0.111 ± 0.034 | 0.113 ± 0.029 | 0.6479 | 0.105 ± 0.036 | 0.113 ± 0.043 | 0.0161 | 0.6972 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano, J.C.E.; Castro-Boqué, E.; García-Carrasco, A.; Morán-Valero, M.I.; González-Hedström, D.; Bermúdez-López, M.; Valdivielso, J.M.; Espinel, A.E.; Portero-Otín, M. Antihypertensive Effects of an Optimized Aged Garlic Extract in Subjects with Grade I Hypertension and Antihypertensive Drug Therapy: A Randomized, Triple-Blind Controlled Trial. Nutrients 2023, 15, 3691. https://doi.org/10.3390/nu15173691
Serrano JCE, Castro-Boqué E, García-Carrasco A, Morán-Valero MI, González-Hedström D, Bermúdez-López M, Valdivielso JM, Espinel AE, Portero-Otín M. Antihypertensive Effects of an Optimized Aged Garlic Extract in Subjects with Grade I Hypertension and Antihypertensive Drug Therapy: A Randomized, Triple-Blind Controlled Trial. Nutrients. 2023; 15(17):3691. https://doi.org/10.3390/nu15173691
Chicago/Turabian StyleSerrano, José C. E., Eva Castro-Boqué, Alicia García-Carrasco, María Inés Morán-Valero, Daniel González-Hedström, Marcelino Bermúdez-López, José Manuel Valdivielso, Alberto E. Espinel, and Manuel Portero-Otín. 2023. "Antihypertensive Effects of an Optimized Aged Garlic Extract in Subjects with Grade I Hypertension and Antihypertensive Drug Therapy: A Randomized, Triple-Blind Controlled Trial" Nutrients 15, no. 17: 3691. https://doi.org/10.3390/nu15173691
APA StyleSerrano, J. C. E., Castro-Boqué, E., García-Carrasco, A., Morán-Valero, M. I., González-Hedström, D., Bermúdez-López, M., Valdivielso, J. M., Espinel, A. E., & Portero-Otín, M. (2023). Antihypertensive Effects of an Optimized Aged Garlic Extract in Subjects with Grade I Hypertension and Antihypertensive Drug Therapy: A Randomized, Triple-Blind Controlled Trial. Nutrients, 15(17), 3691. https://doi.org/10.3390/nu15173691