
Clinical Studies on the Supplementation of Manufactured Human Milk Oligosaccharides: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
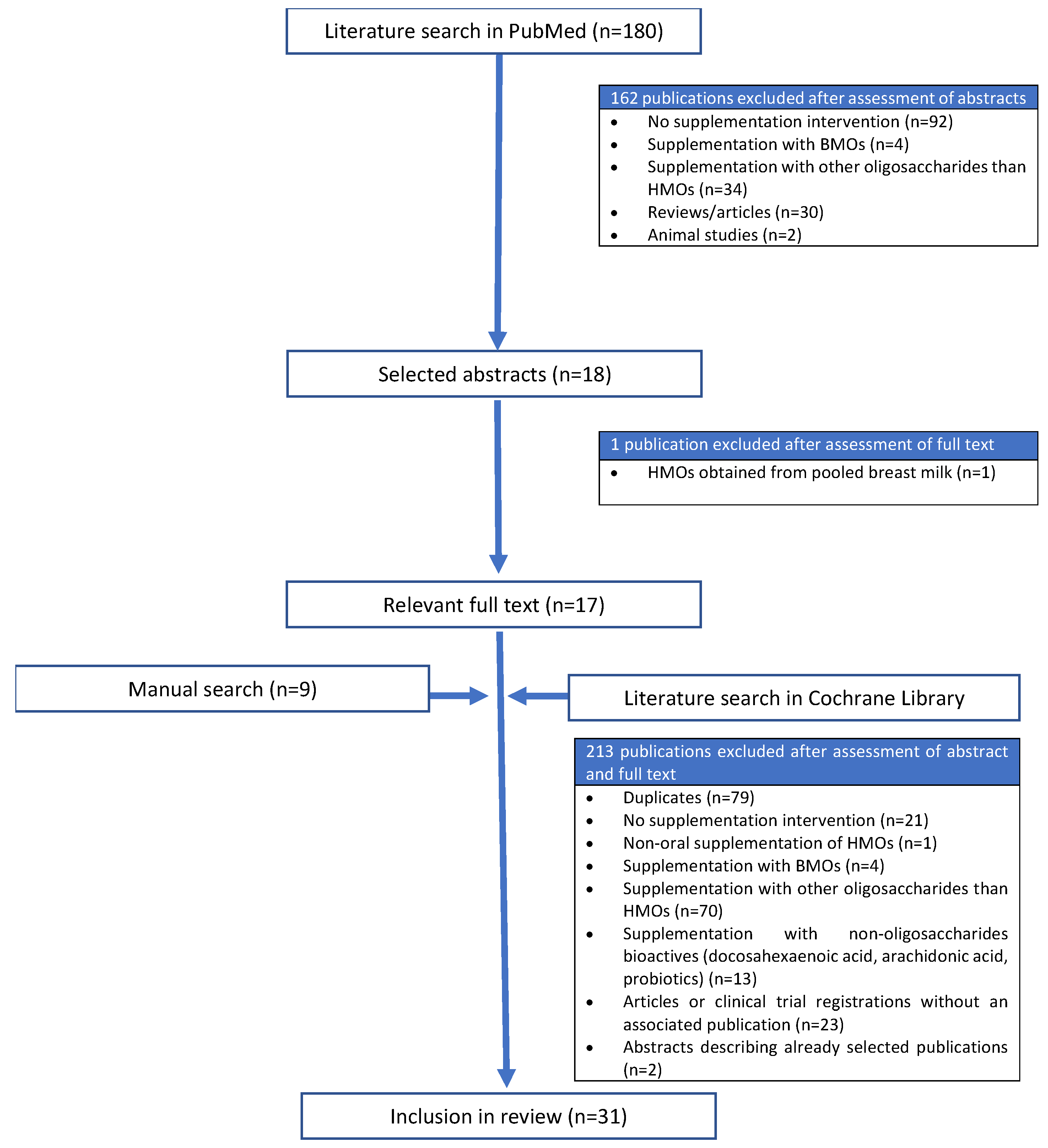
3.1. Overview of the Literature Search
3.2. Description of Studies
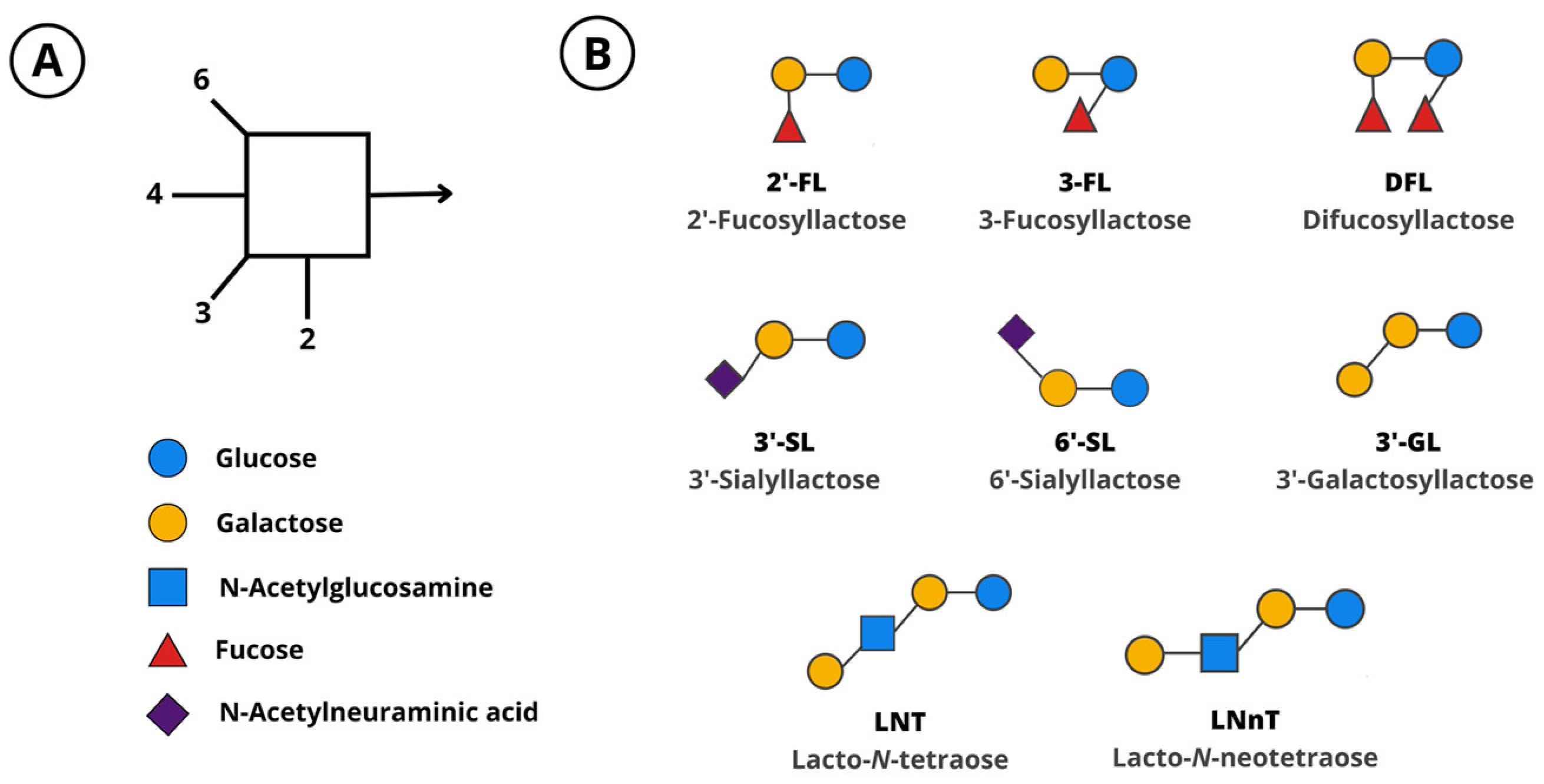
3.3. Investigated HMOs, Doses, and Period of Supplementation

| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Clinical trials Oral supplementation of manufactured HMOs as intervention (individually, in blends, or in combination with other bioactives) HMOs supplemented as pure product or another food product containing manufactured HMOs Individuals of any age Healthy individuals or those with medical conditions Publication available in English language | Non-clinical studies Intake of HMOs from breastfeeding Supplementation of HMO pools isolated from human or bovine milk Supplementation of prebiotics other than HMOs Probiotics or other bioactives as sole intervention Interventions on mothers to evaluate offspring Abstracts duplicating data from other publications |
| Reference | Study Population | Study Design | Intervention Groups | Comparison | Duration of Intervention | Key Findings |
|---|---|---|---|---|---|---|
| [39] | Healthy term infants aged 6–24 months (n = 228) | Randomized, double-blind multicenter, controlled trial | 0.2 g/L LNnT (n = 115) | Control formula without oligosaccharides (n = 113) | 16 weeks | - Safe and well-tolerated - No effect on oropharyngeal colonization with Streptococcus pneumoniae |
| [40] | Healthy term infants < 5 days at inclusion (n = 420) | Randomized, double-blind, multicenter, controlled trial | - Intervention 1: 0.2 g/L 2′-FL + 2.2 g/L GOS (n = 104) - Intervention 2: 1.0 g/L 2′-FL + 1.4 g/L GOS (n = 109) | - Control formula: 2.4 g/L GOS (n = 101) - BF reference group (n = 106) | 17 weeks | - Safe and well tolerated - Supports normal, age-appropriate growth - Similar relative absorption and relative excretion of 2′-FL in intervention and BF groups at DOL 42 and 119 |
| [41] | Follow-up analysis of [40] | - | - Subpopulation from intervention 1: 0.2 g/L 2′-FL + 2.2 g/L GOS (n = 76) - Subpopulation from intervention 2: 1.0 g/L 2′-FL + 1.4 g/L GOS (n = 78) | - Subpopulation from control formula: 2.4 g/L GOS (n = 75) - Subpopulation from BF reference group (n = 86) | - | - Similar cytokine profile and ex vivo stimulation of PBMCs in intervention and BF groups at 6 weeks |
| [42] | Healthy term infants < 8 days at inclusion (n = 119) | Randomized, double-blind, multicenter, controlled trial | 0.2 g/L 2′-FL + 2 g/L scFOS (n = 46) | - Control formula without oligosaccharides (n = 42) - BF reference group (n = 43) | 35 days | - Well tolerated - Supports normal, age-appropriate growth |
| [43] | Healthy term infants < 14 days at inclusion (n = 175) | Randomized, double-blind, multicenter, controlled trial | 1.0 g/L 2′-FL + 0.5 g/L LNnT (n = 88) | - Control formula without oligosaccharides (n = 87) - BF reference group (n = 38) | 6 months (HMO intervention) + follow-up up to 12 months of age (no HMO intervention) | - Safe and well tolerated - Supports normal, age-appropriate growth - Reduced parent-reported cases of bronchitis and medication use during the first 12 months of life - Reduced incidence of infantile colic at 4 months |
| [44] | Healthy term infants 14 ± 5 days at inclusion (n = 79) | Randomized, double-blind, multicenter, controlled trial | 0.25 g/L 2′-FL + Bifidobacterium animalis ssp. lactis. Partially hydrolyzed formula (n = 39) | Control formula without oligosaccharides + Bifidobacterium animalis ssp. lactis (n = 40) | 6 weeks | - Safe and well tolerated - Supports normal, age-appropriate growth - Trend of reduced number of reported infections (not statistically significant) |
| [45] | Follow-up analysis of [43] | - | Subpopulation from intervention: 1.0 g/L 2′-FL + 0.5 g/L LNnT (n = 58) | - Subpopulation from control formula without oligosaccharides (n = 64) - Subpopulation from BF reference group (n = 35) | - | - Gut microbiome composition shifted towards BF infants - Reduced use of antibiotics during the first 12 months of life |
| [46] | Healthy term infants 7 days to 2 months at inclusion (n = 207) | Non-randomized, open-label, multicenter trial | 1.0 g/L 2′-FL + 0.5 g/L LNnT. Partially hydrolyzed formula (n = 66) | - Mixed group: HMO formula + BF - BF reference group (n = 45) | 8 weeks | - Safe and well tolerated - Supports normal, age-appropriate growth |
| [47] | Healthy term infants < 14 days at inclusion (n = 276) | Randomized, double-blind, multicenter, controlled trial | 1.0 g/L 2′-FL + 7.2 g/L GOS + 0.8 g/L FOS, including 0.015 g/L 3′-GL. Partially hydrolyzed formula (n = 108) | - Control formula without 2′-FL and 3′-GL, with 7.2 g/L GOS + 0.8 g/L FOS (n = 107) - BF reference group (n = 61) | 17 weeks | - Safe and well tolerated - Supports normal, age-appropriate growth |
| [48] | Follow-up analysis [43] | - | - | - | - | - Gut microbiome composition shifted towards BF infants - Effect on fecal biomarkers at 3 months |
| [49] | Healthy term infants < 14 days at inclusion (n = 341) | Randomized, double-blind, multicenter, controlled trial | 5.75 g/L HMOs: 2.99 g/L 2′-FL + 0.75 g/L 3-FL + 1.5 g/L LNT + 0.23 g/L 3′-SL + 0.28 g/L 6′-SL (n = 113) | - Control formula without oligosaccharides (n = 112) - BF reference group (n = 116) | 16 weeks (HMO intervention) + 8-week voluntary follow-up (HMO intervention) | - Safe and well tolerated - Supports normal, age-appropriate growth - Stool characteristics shifted towards BF infants |
| [50] | Healthy term infants < 14 days at inclusion (n = 289) | Randomized, double-blind, multicenter, controlled trial | 1.0 g/L 2′-FL + Limosilactobacillus reuteri (n = 144) | - Control formula without oligosaccharides + Limosilactobacillus reuteri (n = 145) - BF reference group (n = 60) | 6 months | - Safe and well tolerated - Supports normal, age-appropriate growth - Gut microbiome composition shifted towards BF infants |
| [51] | Healthy term infants < 21 days at inclusion (n = 535) | Randomized, double-blind, multicenter, controlled trial | - Intervention 1: 1.5 g/L HMOs: 0.87 g/L 2′-FL + 0.10 g/L DFL + 0.29 g/L LNT + 0.11 g/L 3′-SL + 0.14 g/L 6′-SL (n = 153) - Intervention 2: 2.5 g/L HMOs: 1.45 g/L 2′-FL + 0.14 g/L DFL + 0.48 g/L LNT + 0.18 g/L 3′-SL + 0.24 g/L 6′-SL (n = 158) | - Control formula without oligosaccharides (n = 155) - BF reference group (n = 69) | 6 months | - Gut microbiome composition shifted towards BF infants - Effect on fecal biomarkers at 3 and 6 months |
| [52] | Healthy term infants < 14 days at inclusion (n = 363) | Randomized, double-blind, multicenter, controlled trial | 5.75 g/L HMOs: 3.0 g/L 2′-FL + 0.80 g/L 3-FL + 1.5 g/L LNT + 0.20 g/L 3′-SL + 0.30 g/L 6′-SL (n = 130) | - Control formula without oligosaccharides (n = 129) - BF reference group (n = 104) | 4 months | - Safe and well tolerated - Supports normal, age-appropriate growth - Stool characteristics shifted towards BF infants - Reduced number of visits to healthcare professionals |
| [53] | Follow-up analysis [43] | - | - | - | - | - Effect on gut-microbiome fecal co-metabolite profile |
| [54] | Healthy term infants < 28 days at inclusion (n = 221) | Randomized, double-blind, multicenter, controlled trial | 1.0 g/L 2′-FL + FOS (not specified) (n = 66) | - Control formula + GOS + FOS (not specified) (n = 66) - BF reference group (n = 89) | 16 weeks | - Safe - Supports normal, age-appropriate growth - Gut microbiome composition shifted towards BF infants - Increased microbial metabolic capacity to utilize fucosylated HMOs |
| Reference | Study Population | Study Design | Intervention Groups | Comparison | Duration of Intervention | Key Findings |
|---|---|---|---|---|---|---|
| [55] | Infants and children between 2 months and 4 years with diagnosed CMPA (n = 67) | Randomized, double-blind, placebo-controlled food challenge procedure (DBPCFC) and open-label challenge | 1.0 g/L 2′-FL + 0.5 g/L LNnT. Extensively hydrolyzed formula (n = 36 in DBPCFC, n = 62 in open-label challenge) | Control formula without oligosaccharides (n = 31, only in DBPCFC) | 1 week | - Safe and well tolerated - Confirmed hypo-allergenicity |
| [56] | Infants < 60 days at inclusion with suspected food protein allergy/sensitivity (n = 48) | Non-randomized, multicenter, single-arm trial | 0.2 g/L 2′-FL. Extensively hydrolyzed formula (n = 48) | - | 60 days | - Safe and well tolerated - Supports normal, age-appropriate growth - Improved and resolved allergy symptoms |
| [57] | Term infants aged 0–6 months diagnosed with CMPA (n = 194) | Randomized, double-blind, multicenter, controlled trial | 1.0 g/L 2′-FL + 0.5 g/L LNnT. Extensively hydrolyzed formula (n = 94) | Control formula without oligosaccharides (n = 96) | 4 months (HMO intervention) + follow-up up to 12 months of age (no HMO intervention) | - Safe and well tolerated - Supports normal, age-appropriate growth - No effect on allergy symptoms - Reduced frequency of URTIs and risk of otitis media - Reduced use of antipyretics between 4 months and 12 months |
| [58] | Term infants aged 1–8 months diagnosed with moderate-to-severe CMPA (n = 32) | Non-randomized, open-label, multicenter, single-arm trial | 1.0 g/L 2′-FL + 0.5 g/L LNnT. Amino acid-based formula (n = 32) | - | 4 months + voluntarily up to 12 months of age (HMO intervention) | - Safe and well tolerated - Supports normal, age-appropriate growth - Stool characteristics and gut microbiome composition shifted towards BF infants - Effect on SCFA concentrations in feces - Improved allergy symptoms except for two infants, who experienced adverse events associated with the study formula |
| [59] | Preterm infants with very low birth weight < 1700 g (n = 86) | Randomized, double-blind, multicenter, controlled trial | 0.34 g/kg/d 2′-FL + 0.034 g/kg/d LNnT (n = 43) | Glucose placebo (0.140 g/kg/d) (n = 43) | - | - Safe and well tolerated - Increased length-for-age z-score at day 14 and 21 before full enteral feeding - Increased mean head circumference gain at day 21 before full enteral feeding |
| Reference | Study Population | Study Design | Intervention Groups | Comparison | Duration of Intervention | Key Findings |
|---|---|---|---|---|---|---|
| [60] | Healthy children aged 1–2.5 years (n = 461) | Randomized, double-blind, single-center, controlled trial | -Intervention 1: Formula with 3.0 g/L 2′-FL (n = 114) - Intervention 2: Formula with 3.0 g/L 2′-FL + lactoferrin, immunoglobulins, TGF-β and milk fat (n = 114) | - Formula with no supplements (n = 114) - Formula with lactoferrin, immunoglobulins, TGF-β and milk fat (n = 114) | 6 months | - Safe and well tolerated - Supports normal, age-appropriate growth - Reduced number of days with hard stools - Effect on reported duration of URTIs - No effect on gut and nasal microbiome composition |
| [61] | Overweight/obese children aged 6–12 years (n = 75) | Randomized, double-blind, single-center, controlled trial | - Intervention 1: 4.5 g/d 2′-FL (n = 25) - Intervention 2: 4.5 g/d 2′-FL + LNnT at 4:1 ratio (n = 25) | 4.5 g/d glucose placebo (n = 25) | 8 weeks | - Safe and well tolerated - Effect on gut microbiome composition - No effect on stool characteristics, blood, and fecal markers |
| Reference | Study Population | Study Design | Intervention Groups | Comparison | Duration of Intervention | Key Findings |
|---|---|---|---|---|---|---|
| [62] | Adults with diagnosed H. pylori infection (n = 6) | Open-label study | 10 g/d 3′-SL (n = 6) | - | 1 day | - No effects on H. pylori infection - Well tolerated - No effects on blood markers |
| [63] | Adults with diagnosed H. pylori infection (n = 65) | Randomized, double-blind, placebo-controlled trial | Intervention 1: 10 g/d 3′-SL (n = 17) Intervention 2: 20 g/d 3′-SL (n = 22) | Placebo (not specified, n = 21) | 4 weeks | - No effects on H. pylori infection - Well tolerated |
| [64] | Healthy adults (n = 100) | Randomized, double-blind, single-center, controlled trial | - Intervention 1: 5 g/d 2′-FL (n = 10) - Intervention 2: 10 g/d 2′-FL (n = 10) - Intervention 3: 20 g/d 2′-FL (n = 10) - Intervention 4: 5 g/d LNnT (n = 10) - Intervention 5: 10 g/d LNnT (n = 10) - Intervention 6: 20 g/d LNnT (n = 10) - Intervention 7: 5 g/d 2′-FL + LNnT at 2:1 ratio (n = 10) - Intervention 8: 10 g/d 2′-FL + LNnT at 2:1 ratio (n = 10) - Intervention 9: 20 g/d 2′-FL + LNnT at 2:1 ratio (n = 10) | 2 g/d glucose placebo (n = 10) | 2 weeks | - Safe and well tolerated - Reported gastrointestinal symptoms in some higher-dose intervention groups - Effect on gut microbiome composition - No effect on blood and fecal markers |
| [65] | Adults with IBS (n = 61) | Randomized, double-blind, single-center, controlled trial | - Intervention 1: 5 g/d 2′-FL + LNnT at 4:1 ratio (n = 20) - Intervention 2: 10 g/d 2′-FL + LNnT at 4.1 ratio (n = 20) | 5 g/d glucose placebo (n = 21) | 4 weeks supplementation + 4-week follow-up (no HMO intervention) | - Well tolerated - No worsening of IBS symptoms - No effect on gut microbiome composition |
| [66] | Follow-up analysis of [65] | - | - | - | - | - Effect on microbiome composition in fecal and mucosal colonic biopsies samples - Effect on fecal and plasma biomarkers |
| [67] | Adults with IBS (n = 317) | Open-label, multicenter, single-arm trial | 4 g/d 2′-FL + 1 g/d LNnT (n = 317) | - | 12 weeks | - Safe and well tolerated - Improved IBS symptoms - Effect on stool characteristics |
| [68] | Adults with IBS, ulcerative colitis, Crohn’s disease, or celiac disease (n = 20) | Open-label, multicenter, single-arm, pilot trial | 4 g/d 2′-FL (n = 20) | - | 6 weeks | - Improved IBS symptoms - Effect on gut microbiome composition - Effect on SCFA concentrations in feces |
| [69] | Healthy adults (n = 60) | Randomized, triple-blind, single-center, controlled trial | 3 g/d 6′-SL (n = 30) | 3 g/d maltodextrin placebo (n = 30) | 12 weeks | - Safe and well tolerated - No effect on blood markers |
| Study Population | Study Product | Reference | Total HMO | Dosage | Other Bioactive Compounds | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2′-FL | 3-FL | DFL | LNT | LNnT | 3′-GL | 3′-SL | 6′-SL | |||||
| Healthy term infants | Infant formula (g/L) | [39] | 0.2 | 0.2 | ||||||||
| [40] | 0.2 1.0 | 0.2 1.0 | GOS: 2.2 and 1.4 g/L | |||||||||
| [41] | 0.2 | 0.2 | FOS: 2.0 g/L | |||||||||
| [43] | 1.5 | 1.0 | 0.5 | |||||||||
| [44] | 0.25 | 0.25 | Bifidobacterium animalis ssp. lactis (106 CFU/g) | |||||||||
| [46] | 1.5 | 1.0 | 0.5 | Limosilactobacillus reuteri (CFU not specified) | ||||||||
| [47] | 1.0 | 1.0 | 0.015 | GOS: 7.2 g/L FOS: 0.8 | ||||||||
| [49] | 5.75 | 2.99 | 0.75 | 1.5 | 0.23 | 0.28 | ||||||
| [50] | 1.0 | 1.0 | Limosilactobacillus reuteri (107 CFU/g) | |||||||||
| [51] | 1.5 2.5 | 0.87 1.45 | 0.10 0.14 | 0.29 0.48 | 0.11 0.18 | 0.14 0.24 | ||||||
| [52] | 5.75 | 3.0 | 0.8 | 1.5 | 0.20 | 0.30 | ||||||
| [54] | 1.0 | 1.0 | FOS (not specified) | |||||||||
| Infants with diagnosed or suspected allergies | Infant formula (g/L) | [55] | 1.5 | 1.0 | 0.5 | |||||||
| [56] | 0.2 | 0.2 | ||||||||||
| [57] | 1.5 | 1.0 | 0.5 | |||||||||
| [58] | 1.5 | 1.0 | 0.5 | |||||||||
| Pre-term infants | Dietary supplement (g/kg/d) | [59] | 0.374 | 0.34 | 0.034 | |||||||
| Healthy children | Young-child formula (g/L) | [60] | 3.0 | 3.0 | Lactoferrin, immunoglobulins, TGF-β, and milk fat | |||||||
| Obese and overweight children | Dietary supplement (g/d) | [61] | 4.5 | 4.5 3.6 | - 0.9 | |||||||
| Healthy adults | Dietary supplement (g/d) | [64] | 5.0 10.0 20.0 | 5.0 10.0 20.0 - - - 3.33 6.67 13.32 | - - - 5.0 10.0 20.0 1.67 3.32 6.67 | |||||||
| [68] | 4.0 | 4.0 | ||||||||||
| [69] | 3.0 | 3.0 | ||||||||||
| Adults with IBS | Dietary supplement (g/d) | [67] | 5.0 | 4.0 | 1.0 | |||||||
| [65] | 5.0 10.0 | 4.0 8.0 | 1.0 2.0 | |||||||||
| Adults with Helicobacter pylori infection | Supplement (g/d) | [62] | 10.0 | 10.0 | ||||||||
| [63] | 10.0 20.0 | 10.0 20.0 | ||||||||||
3.4. Study Outcomes
3.4.1. Safety
3.4.2. Growth
3.4.3. Tolerance
3.4.4. Stool Characteristics
3.4.5. Infection Incidence
3.4.6. Gut and Nasopharyngeal Microbiome
3.4.7. Biomarkers in Fecal Samples
3.4.8. Blood Analysis
3.4.9. Other Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horta, B.L.; Loret De Mola, C.; Victora, C.G. Long-Term Consequences of Breastfeeding on Cholesterol, Obesity, Systolic Blood Pressure and Type 2 Diabetes: A Systematic Review and Meta-Analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Smith, E.R.; Lee, S.E.; Vargas, A.J.; Bremer, A.A.; Raiten, D.J. The Need to Study Human Milk as a Biological System. Am. J. Clin. Nutr. 2021, 113, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- de Weerth, C.; Aatsinki, A.K.; Azad, M.B.; Bartol, F.F.; Bode, L.; Collado, M.C.; Dettmer, A.M.; Field, C.J.; Guilfoyle, M.; Hinde, K.; et al. Human Milk: From Complex Tailored Nutrition to Bioactive Impact on Child Cognition and Behavior. Crit. Rev. Food Sci. Nutr. 2022, 30, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.M.; Aghaeepour, N.; Andres, A.; Azad, M.B.; Becker, M.; Carlson, S.E.; Järvinen, K.M.; Lin, W.; Lönnerdal, B.; Slupsky, C.M.; et al. Evidence for Human Milk as a Biological System and Recommendations for Study Design-a Report from “Breastmilk Ecology: Genesis of Infant Nutrition (BEGIN)” Working Group 4. Am. J. Clin. Nutr. 2023, 117 (Suppl. 1), S61–S86. [Google Scholar] [CrossRef]
- Urashima, T.; Hirabayashi, J.; Sato, S.; Kobata, A. Human Milk Oligosaccharides as Essential Tools for Basic and Application Studies on Galectins. Trends Glycosci. Glycotechnol. 2018, 30, SE51–SE65. [Google Scholar] [CrossRef]
- Bode, L. Human Milk Oligosaccharides: Every Baby Needs a Sugar Mama. Glycobiology 2012, 22, 1147–1162. [Google Scholar] [CrossRef]
- Zhang, S.; Li, T.; Xie, J.; Zhang, D.; Pi, C.; Zhou, L.; Yang, W. Gold Standard for Nutrition: A Review of Human Milk Oligosaccharide and Its Effects on Infant Gut Microbiota. Microb. Cell Fact. 2021, 20, 108. [Google Scholar] [CrossRef]
- Hanisch, F.-G.; Kunz, C. Novel Class of Human Milk Oligosaccharides Based on 6′-Galactosyllactose Containing N-Acetylglucosamine Branches Extended by Oligogalactoses. J. Proteome Res. 2021, 20, 3865–3874. [Google Scholar] [CrossRef]
- Gnoth, M.J.; Kunz, C.; Kinne-Saffran, E.; Rudloff, S. Human Milk Oligosaccharides Are Minimally Digested In Vitro. J. Nutr. 2000, 130, 3014–3020. [Google Scholar] [CrossRef]
- Engfer, M.B.; Stahl, B.; Finke, B.; Sawatzki, G.; Daniel, H. Human Milk Oligosaccharides Are Resistant to Enzymatic Hydrolysis in the Upper Gastrointestinal Tract. Am. J. Clin. Nutr. 2000, 71, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Mills, D.A.; German, J.B.; Lebrilla, C.B.; Underwood, M.A. Translating Neonatal Microbiome Science into Commercial Innovation: Metabolism of Human Milk Oligosaccharides as a Basis for Probiotic Efficacy in Breast-Fed Infants. Gut Microbes 2023, 15, 2192458. [Google Scholar] [CrossRef]
- Marcobal, A.; Barboza, M.; Froehlich, J.W.; Block, D.E.; German, J.B.; Lebrilla, C.B.; Mills, D.A. Consumption of Human Milk Oligosaccharides by Gut-Related Microbes. J. Agric. Food Chem. 2010, 58, 5334–5340. [Google Scholar] [CrossRef] [PubMed]
- Sela, D.A.; Mills, D.A. Nursing Our Microbiota: Molecular Linkages between Bifidobacteria and Milk Oligosaccharides. Trends Microbiol. 2010, 18, 298–307. [Google Scholar] [CrossRef]
- Laursen, M.F.; Sakanaka, M.; von Burg, N.; Mörbe, U.; Andersen, D.; Moll, J.M.; Pekmez, C.T.; Rivollier, A.; Michaelsen, K.F.; Mølgaard, C.; et al. Bifidobacterium Species Associated with Breastfeeding Produce Aromatic Lactic Acids in the Infant Gut. Nat. Microbiol. 2021, 6, 1367–1382. [Google Scholar] [CrossRef] [PubMed]
- Roager, H.M.; Stanton, C.; Hall, L.J. Microbial Metabolites as Modulators of the Infant Gut Microbiome and Host-Microbial Interactions in Early Life. Gut Microbes 2023, 15, 2192151. [Google Scholar] [CrossRef]
- Triantis, V.; Bode, L.; van Neerven, J.R.J. Immunological Effects of Human Milk Oligosaccharides. Front. Pediatr. 2018, 6, 190. [Google Scholar] [CrossRef]
- Morozov, V.; Hansman, G.; Hanisch, F.G.; Schroten, H.; Kunz, C. Human Milk Oligosaccharides as Promising Antivirals. Mol. Nutr. Food Res. 2018, 62, e1700679. [Google Scholar] [CrossRef]
- Donovan, S.M.; Comstock, S.S. Human Milk Oligosaccharides Influence Neonatal Mucosal and Systemic Immunity. Ann. Nutr. Metab. 2016, 69 (Suppl. 2), 42–51. [Google Scholar] [CrossRef]
- Tarrant, I.; Finlay, B.B. Human Milk Oligosaccharides: Potential Therapeutic Aids for Allergic Diseases. Trends Immunol. 2023, 44, 644–661. [Google Scholar] [CrossRef]
- Carr, L.E.; Virmani, M.D.; Rosa, F.; Munblit, D.; Matazel, K.S.; Elolimy, A.A.; Yeruva, L. Role of Human Milk Bioactives on Infants’ Gut and Immune Health. Front. Immunol. 2021, 12, 604080. [Google Scholar] [CrossRef] [PubMed]
- Berger, P.K.; Plows, J.F.; Jones, R.B.; Alderete, T.L.; Yonemitsu, C.; Poulsen, M.; Ryoo, J.H.; Peterson, B.S.; Bode, L.; Goran, M.I. Human Milk Oligosaccharide 2′-Fucosyllactose Links Feedings at 1 Month to Cognitive Development at 24 Months in Infants of Normal and Overweight Mothers. PLoS ONE 2020, 15, e0228323. [Google Scholar] [CrossRef] [PubMed]
- Oliveros, E.; Martín, M.J.; Torres-Espínola, F.J.; Segura-Moreno, T.; Ramírez, M.; Santos, A.; Buck, R.; Rueda, R.; Escudero, M.; Catena, A.; et al. Human Milk Levels of 2´-Fucosyllactose and 6´-Sialyllactose Are Positively Associated with Infant Neurodevelopment and Are Not Impacted by Maternal BMI or Diabetic Status. J. Nutr. Food Sci. 2021, 4, 100024. [Google Scholar]
- Jantscher-Krenn, E.; von Schirnding, L.; Trötzmüller, M.; Köfeler, H.; Kurtovic, U.; Fluhr, H.; Müller, A.; Bagci, S. Human Milk Oligosaccharides Are Present in Amniotic Fluid and Show Specific Patterns Dependent on Gestational Age. Nutrients 2022, 14, 2065. [Google Scholar] [CrossRef]
- Lu, M.; Mosleh, I.; Abbaspourrad, A. Engineered Microbial Routes for Human Milk Oligosaccharides Synthesis. ACS Synth. Biol. 2021, 10, 923–938. [Google Scholar] [CrossRef]
- Bode, L.; Contractor, N.; Barile, D.; Pohl, N.; Prudden, A.R.; Boons, G.J.; Jin, Y.S.; Jennewein, S. Overcoming the Limited Availability of Human Milk Oligosaccharides: Challenges and Opportunities for Research and Application. Nutr. Rev. 2016, 74, 635–644. [Google Scholar] [CrossRef]
- Biel-Nielsen, T.L.; Li, K.; Sørensen, S.O.; Sejberg, J.J.P.; Meyer, A.S.; Holck, J. Utilization of Industrial Citrus Pectin Side Streams for Enzymatic Production of Human Milk Oligosaccharides. Carbohydr. Res. 2022, 519, 108627. [Google Scholar] [CrossRef]
- Salminen, S.; Stahl, B.; Vinderola, G.; Szajewska, H. Infant Formula Supplemented with Biotics: Current Knowledge and Future Perspectives. Nutrients 2020, 12, 1952. [Google Scholar] [CrossRef]
- Dinleyici, M.; Barbieur, J.; Dinleyici, E.C.; Vandenplas, Y. Functional Effects of Human Milk Oligosaccharides (HMOs). Gut Microbes 2023, 15, 2186115. [Google Scholar] [CrossRef]
- Sprenger, N.; Tytgat, H.L.P.; Binia, A.; Austin, S.; Singhal, A. Biology of Human Milk Oligosaccharides: From Basic Science to Clinical Evidence. J. Hum. Nutr. Diet. 2022, 35, 280–299. [Google Scholar] [CrossRef]
- Walsh, C.; Lane, J.A.; van Sinderen, D.; Hickey, R.M. From Lab Bench to Formulated Ingredient: Characterization, Production, and Commercialization of Human Milk Oligosaccharides. J. Funct. Foods 2020, 72, 104052. [Google Scholar] [CrossRef]
- Szajewska, H. Selected Human Milk Oligosaccharides Added to Infant Formulas for Term Infants. Nestle Nutr. Inst. Workshop Ser. 2021, 96, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Reverri, E.J.; Devitt, A.A.; Kajzer, J.A.; Baggs, G.E.; Borschel, M.W. Review of the Clinical Experiences of Feeding Infants Formula Containing the Human Milk Oligosaccharide 2′-Fucosyllactose. Nutrients 2018, 10, 1346. [Google Scholar] [CrossRef]
- Sanz Morales, P.; Wijeyesekera, A.; Robertson, M.D.; Jackson, P.P.J.; Gibson, G.R. The Potential Role of Human Milk Oligosaccharides in Irritable Bowel Syndrome. Microorganisms 2022, 10, 2338. [Google Scholar] [CrossRef] [PubMed]
- Button, J.E.; Autran, C.A.; Reens, A.L.; Cosetta, C.M.; Smriga, S.; Ericson, M.; Pierce, J.V.; Cook, D.N.; Lee, M.L.; Sun, A.K.; et al. Dosing a Synbiotic of Human Milk Oligosaccharides and B. Infantis Leads to Reversible Engraftment in Healthy Adult Microbiomes without Antibiotics. Cell Host Microbe 2022, 30, 712–725.e7. [Google Scholar] [CrossRef]
- Steenhout, P.; Sperisen, P.; Martin, F.-P.; Sprenger, N.; Wernimont, S.; Pecquet, S.; Berger, B. Term Infant Formula Supplemented with Human Milk Oligosaccharides (2′Fucosyllactose and Lacto-N-Neotetraose) Shifts Stool Microbiota and Metabolic Signatures Closer to That of Breastfed Infants. FASEB J. 2016, 30, 275.7. [Google Scholar]
- Vigsnæs, L.K.; Iribarren, C.; Magnusson, M.K.; Amundsen, I.D.; McConnell, B.; Seitzberg, D.; Ohman, L.; Simren, M. Impact of Human Milk Oligosaccharides on the Gut Microbiota Composition from Irritable Bowel Syndrome Parients: A Dparallel Double-Blind, Placebo Controlled Trial. Gastroenterology 2020, 158, S-848. [Google Scholar] [CrossRef]
- Ukkonen, P.; Varis, K.; Jernfors, M.; Herva, E.; Jokinen, J.; Ruokokoski, E.; Zopf, D.; Kilpi, T. Treatment of Acute Otitis Media with an Antiadhesive Oligosaccharide: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2000, 356, 1398–1402. [Google Scholar] [CrossRef]
- Prieto, A.P. Vitro and Clinical Experiences with a Human Milk Oligosaccharide, Lacto-NneoTetraose, and Fructooligosaccharides. Foods Food Ingred. J. Jpn. 2005, 210, 1018–1030. [Google Scholar]
- Marriage, B.J.; Buck, R.H.; Goehring, K.C.; Oliver, J.S.; Williams, J.A. Infants Fed a Lower Calorie Formula with 2′FL Show Growth and 2′FL Uptake Like Breast-Fed Infants. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 649–658. [Google Scholar] [CrossRef]
- Goehring, K.C.; Marriage, B.J.; Oliver, J.S.; Wilder, J.A.; Barrett, E.G.; Buck, R.H. Similar to Those Who Are Breastfed, Infants Fed a Formula Containing 2′-Fucosyllactose Have Lower Inflammatory Cytokines in a Randomized Controlled Trial. J. Nutr. 2016, 146, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Kajzer, J.; Oliver, J.; Marriage, B. Gastrointestinal Tolerance of Formula Supplemented with Oligosaccharides. FASEB J. 2016, 30, 671.4. [Google Scholar]
- Puccio, G.; Alliet, P.; Cajozzo, C.; Janssens, E.; Corsello, G.; Sprenger, N.; Wernimont, S.; Egli, D.; Gosoniu, L.; Steenhout, P. Effects of Infant Formula with Human Milk Oligosaccharides on Growth and Morbidity: A Randomized Multicenter Trial. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 624–631. [Google Scholar] [CrossRef]
- Storm, H.M.; Shepard, J.; Czerkies, L.M.; Kineman, B.; Cohen, S.S.; Reichert, H.; Carvalho, R. 2′-Fucosyllactose Is Well Tolerated in a 100% Whey, Partially Hydrolyzed Infant Formula with Bifidobacterium Lactis: A Randomized Controlled Trial. Glob. Pediatr. Health 2019, 6. [Google Scholar] [CrossRef]
- Berger, B.; Porta, N.; Foata, F.; Grathwohl, D.; Delley, M.; Moine, D.; Charpagne, A.; Siegwald, L.; Descombes, P.; Alliet, P.; et al. Linking Human Milk Oligosaccharides, Infant Fecal Community Types, and Later Risk To Require Antibiotics. mBio 2020, 11, e03196-19. [Google Scholar] [CrossRef]
- Román Riechmann, E.; Moreno Villares, J.M.; Domínguez Ortega, F.; Carmona Martínez, A.; Picó Sirvent, L.; Santana Sandoval, L.; Casas Rivero, J.; Alshweki, A.; Cercamondi, C.; Dahbane, S.; et al. Real-World Study in Infants Fed with an Infant Formula with Two Human Milk Oligosaccharydes. Nutr. Hosp. 2020, 37, 698–706. [Google Scholar] [CrossRef]
- Vandenplas, Y.; de Halleux, V.; Arciszewska, M.; Lach, P.; Pokhylko, V.; Klymenko, V.; Schoen, S.; Abrahamse-Berkeveld, M.; Mulder, K.A.; Rubio, R.P. A Partly Fermented Infant Formula with Postbiotics Including 3′-GL, Specific Oligosaccharides, 2′-FL, and Milk Fat Supports Adequate Growth, Is Safe and Well-Tolerated in Healthy Term Infants: A Double-Blind, Randomised, Controlled, Multi-Country Trial. Nutrients 2020, 12, 3560. [Google Scholar] [CrossRef]
- Dogra, S.K.; Martin, F.P.; Donnicola, D.; Julita, M.; Berger, B.; Sprenger, N. Human Milk Oligosaccharide-Stimulated Bifidobacterium Species Contribute to Prevent Later Respiratory Tract Infections. Microorganisms 2021, 9, 1939. [Google Scholar] [CrossRef]
- Parschat, K.; Melsaether, C.; Jäpelt, K.R.; Jennewein, S. Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth. Nutrients 2021, 13, 2871. [Google Scholar] [CrossRef]
- Alliet, P.; Vandenplas, Y.; Roggero, P.; Jespers, S.N.J.; Peeters, S.; Stalens, J.P.; Kortman, G.A.M.; Amico, M.; Berger, B.; Sprenger, N.; et al. Safety and Efficacy of a Probiotic-Containing Infant Formula Supplemented with 2′-Fucosyllactose: A Double-Blind Randomized Controlled Trial. Nutr. J. 2022, 21, 11. [Google Scholar] [CrossRef]
- Bosheva, M.; Tokodi, I.; Krasnow, A.; Pedersen, H.K.; Lukjancenko, O.; Eklund, A.C.; Grathwohl, D.; Sprenger, N.; Berger, B.; Cercamondi, C.I. Infant Formula with a Specific Blend of Five Human Milk Oligosaccharides Drives the Gut Microbiota Development and Improves Gut Maturation Markers: A Randomized Controlled Trial. Front. Nutr. 2022, 9, 920362. [Google Scholar] [CrossRef]
- Lasekan, J.; Choe, Y.; Dvoretskiy, S.; Devitt, A.; Zhang, S.; Mackey, A.; Wulf, K.; Buck, R.; Steele, C.; Johnson, M.; et al. Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial. Nutrients 2022, 14, 2625. [Google Scholar] [CrossRef]
- Martin, F.P.; Tytgat, H.L.P.; Krogh Pedersen, H.; Moine, D.; Eklund, A.C.; Berger, B.; Sprenger, N. Host-Microbial Co-Metabolites Modulated by Human Milk Oligosaccharides Relate to Reduced Risk of Respiratory Tract Infections. Front. Nutr. 2022, 9, 935711. [Google Scholar] [CrossRef] [PubMed]
- Wallingford, J.C.; Neve Myers, P.; Barber, C.M. Effects of Addition of 2-Fucosyllactose to Infant Formula on Growth and Specific Pathways of Utilization by Bifidobacterium in Healthy Term Infants. Front. Nutr. 2022, 9, 961526. [Google Scholar] [CrossRef] [PubMed]
- Nowak-Wegrzyn, A.; Czerkies, L.; Reyes, K.; Collins, B.; Heine, R.G. Confirmed Hypoallergenicity of a Novel Whey-Based Extensively Hydrolyzed Infant Formula Containing Two Human Milk Oligosaccharides. Nutrients 2019, 11, 1447. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Farias, C.; Baggs, G.E.; Marriage, B.J. Growth, Tolerance, and Compliance of Infants Fed an Extensively Hydrolyzed Infant Formula with Added 2′-Fl Fucosyllactose (2′-Fl) Human Milk Oligosaccharide. Nutrients 2021, 13, 186. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Żołnowska, M.; Canani, R.B.; Ludman, S.; Tengelyi, Z.; Moreno-álvarez, A.; Goh, A.E.N.; Gosoniu, M.L.; Kirwan, B.A.; Tadi, M.; et al. Effects of an Extensively Hydrolyzed Formula Supplemented with Two Human Milk Oligosaccharides on Growth, Tolerability, Safety and Infection Risk in Infants with Cow’s Milk Protein Allergy: A Randomized, Multi-Center Trial. Nutrients 2022, 14, 530. [Google Scholar] [CrossRef]
- Gold, M.S.; Quinn, P.J.; Campbell, D.E.; Peake, J.; Smart, J.; Robinson, M.; O’sullivan, M.; Vogt, J.K.; Pedersen, H.K.; Liu, X.; et al. Effects of an Amino Acid-Based Formula Supplemented with Two Human Milk Oligosaccharides on Growth, Tolerability, Safety, and Gut Microbiome in Infants with Cow’s Milk Protein Allergy. Nutrients 2022, 14, 2297. [Google Scholar] [CrossRef]
- Hascoët, J.M.; Chevallier, M.; Gire, C.; Brat, R.; Rozé, J.C.; Norbert, K.; Chen, Y.; Hartweg, M.; Billeaud, C. Use of a Liquid Supplement Containing 2 Human Milk Oligosaccharides: The First Double-Blind, Randomized, Controlled Trial in Pre-Term Infants. Front. Pediatr. 2022, 10, 858380. [Google Scholar] [CrossRef]
- Leung, T.F.; Ulfman, L.H.; Chong, M.K.C.; Hon, K.L.; Khouw, I.M.S.L.; Chan, P.K.S.; Delsing, D.J.; Kortman, G.A.M.; Bovee-Oudenhoven, I.M.J. A Randomized Controlled Trial of Different Young Child Formulas on Upper Respiratory and Gastrointestinal Tract Infections in Chinese Toddlers. Pediatr. Allergy Immunol. 2020, 31, 745–754. [Google Scholar] [CrossRef]
- Fonvig, C.E.; Amundsen, I.D.; Vigsnæs, L.K.; Sørensen, N.; Frithioff-Bøjsøe, C.; Christiansen, M.; Hedley, P.L.; Holm, L.A.; McConnell, B.; Holm, J.C. Human Milk Oligosaccharides Modulate Fecal Microbiota and Are Safe for Use in Children with Overweight: A Randomized Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Opekun, A.R.; El-Zaimaity, H.M.T.; Osato, M.S.; Gilger, M.A.; Malaty, H.M.; Terry, M.; Headon, D.R.; Graham, D.Y. Novel Therapies for Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 1999, 13, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Parente, F.; Cucino, C.; Anderloni, A.; Grandinetti, G.; Bianchi Porro, G. Treatment Oi Helicobacter Pylori Infection Using. a Novel Antiadhesion Compound (3′sialyllactose Sodium Salt). A Double Blind, Placebo-Controlled Clinical Study. Helicobacter 2003, 8, 252–256. [Google Scholar] [CrossRef]
- Elison, E. Oral Supplementation of Healthy Adults with 2′-O-Fucosyllactose and Lacto-N-Neotetraose Is Well Tolerated and Shifts the Intestinal Microbiota. Br. J. Nutr. 2016, 116, 1356–1368. [Google Scholar] [CrossRef]
- Iribarren, C.; Törnblom, H.; Aziz, I.; Magnusson, M.K.; Sundin, J.; Vigsnæs, L.K.; Amundsen, I.D.; McConnell, B.; Seitzberg, D.; Öhman, L.; et al. Human Milk Oligosaccharide Supplementation in Irritable Bowel Syndrome Patients: A Parallel, Randomized, Double-Blind, Placebo-Controlled Study. Neurogastroenterol. Motil. 2020, 32, e13920. [Google Scholar] [CrossRef] [PubMed]
- Iribarren, C.; Magnusson, M.K.; Vigsnæs, L.K.; Aziz, I.; Amundsen, I.D.; Šuligoj, T.; Juge, N.; Patel, P.; Sapnara, M.; Johnsen, L.; et al. The Effects of Human Milk Oligosaccharides on Gut Microbiota, Metabolite Profiles and Host Mucosal Response in Patients with Irritable Bowel Syndrome. Nutrients 2021, 13, 3836. [Google Scholar] [CrossRef]
- Palsson, O.S.; Peery, A.; Seitzberg, D.; Amundsen, I.D.; McConnell, B.; Simrén, M. Human Milk Oligosaccharides Support Normal Bowel Function and Improve Symptoms of Irritable Bowel Syndrome: A Multicenter, Open-Label Trial. Clin. Transl. Gastroenterol. 2020, 11, e00276. [Google Scholar] [CrossRef]
- Ryan, J.J.; Monteagudo-Mera, A.; Contractor, N.; Gibson, G.R. Impact of 2′-Fucosyllactose on Gut Microbiota Composition in Adults with Chronic Gastrointestinal Conditions: Batch Culture Fermentation Model and Pilot Clinical Trial Findings. Nutrients 2021, 13, 938. [Google Scholar] [CrossRef]
- Kim, J.H.; Yong, S.Y.; Kim, S.H.; Baek, A.; Go, T.H.; Kang, D.R. Randomized, Triple-Blind, Placebo-Controlled Study to Evaluate the Safety of 6′-Sialyllactose in Healthy Adults. Regul. Toxicol. Pharmacol. 2022, 129, 105110. [Google Scholar] [CrossRef]
- American Academy of Pediatrics; Committee on Nutrition. Hypoallergenic Infant Formulas. Pediatrics 2000, 106, 346–349. [Google Scholar] [CrossRef]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Mysonhimer, A.R.; Holscher, H.D. Gastrointestinal Effects and Tolerance of Nondigestible Carbohydrate Consumption. Adv. Nutr. 2022, 13, 2237–2276. [Google Scholar] [CrossRef]
- Shanahan, F.; Ghosh, T.S.; O’Toole, P.W. The Healthy Microbiome-What Is the Definition of a Healthy Gut Microbiome? Gastroenterology 2021, 160, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.J. 2022 Fleming Prize Lecture: Diet-Microbe-Host Interaction in Early Life. J. Med. Microbiol. 2023, 72, 001662. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, P.A.; Goossens, D.A.M.; Staiano, A. Stool Characteristics of Infants Receiving Short-Chain Galacto-Oligosaccharides and Long-Chain Fructo-Oligosaccharides: A Review. World J. Gastroenterol. 2014, 20, 13446–13452. [Google Scholar] [CrossRef]
- Skórka, A.; Pieścik-Lech, M.; Kołodziej, M.; Szajewska, H. Infant Formulae Supplemented with Prebiotics: Are They Better than Unsupplemented Formulae? An Updated Systematic Review. Br. J. Nutr. 2018, 119, 810–825. [Google Scholar] [CrossRef]
- Lönnerdal, B. Infant Formula and Infant Nutrition: Bioactive Proteins of Human Milk and Implications for Composition of Infant Formulas. Am. J. Clin. Nutr. 2014, 99, 712S–717S. [Google Scholar] [CrossRef]
- Zuurveld, M.; Ayechu-Muruzabal, V.; Folkerts, G.; Garssen, J.; van‘t Land, B.; Willemsen, L.E.M. Specific Human Milk Oligosaccharides Differentially Promote Th1 and Regulatory Responses in a CpG-Activated Epithelial/Immune Cell Coculture. Biomolecules 2023, 13, 263. [Google Scholar] [CrossRef]
- Rousseaux, A.; Brosseau, C.; Le Gall, S.; Piloquet, H.; Barbarot, S.; Bodinier, M. Human Milk Oligosaccharides: Their Effects on the Host and Their Potential as Therapeutic Agents. Front. Immunol. 2021, 12, 680911. [Google Scholar] [CrossRef]
- Rudloff, S.; Pohlentz, G.; Borsch, C.; Lentze, M.J.; Kunz, C. Urinary Excretion of in Vivo 13C-Labelled Milk Oligosaccharides in Breastfed Infants. Br. J. Nutr. 2012, 107, 957–963. [Google Scholar] [CrossRef]
- Goehring, K.C.; Kennedy, A.D.; Prieto, P.A.; Buck, R.H. Direct Evidence for the Presence of Human Milk Oligosaccharides in the Circulation of Breastfed Infants. PLoS ONE 2014, 9, e101692. [Google Scholar] [CrossRef] [PubMed]
- Ruhaak, L.R.; Stroble, C.; Underwood, M.A.; Lebrilla, C.B. Detection of Milk Oligosaccharides in Plasma of Infants. Anal. Bioanal. Chem. 2014, 406, 5775–5784. [Google Scholar] [CrossRef] [PubMed]
- Bode, L. Human Milk Oligosaccharides: Structure and Functions. Nestle Nutr. Inst. Workshop Ser. 2020, 94, 115–123. [Google Scholar] [CrossRef] [PubMed]
- BfR. Gesundheitliche Vorteile von Säuglingsanfangs- Und Folgenahrung Mit Humanen Milcholigo- Und/Oder Galaktooligosacchariden Noch Nicht Belegt. BfR-Stellungnahmen 2022, 2022, 1–42. [Google Scholar] [CrossRef]
- Bührer, C.; Ensenauer, R.; Jochum, F.; Kalhoff, H.; Koletzko, B.; Lawrenz, B.; Mihatsch, W.; Posovszky, C.; Rudloff, S. Infant Formulas with Synthetic Oligosaccharides and Respective Marketing Practices. Mol. Cell Pediatr. 2022, 9, 14. [Google Scholar] [CrossRef]
- Donovan, S.M.; Abrams, S.A.; Azad, M.B.; Belfort, M.B.; Bode, L.; Carlson, S.E.; Dallas, D.C.; Hettinga, K.; Järvinen, K.; Kim, J.H.; et al. Summary of the Joint National Institutes of Health and the Food and Drug Administration Workshop Titled “Exploring the Science Surrounding the Safe Use of Bioactive Ingredients in Infant Formula: Considerations for an Assessment Framework”. J. Pediatr. 2022, 255, 30–41.e1. [Google Scholar] [CrossRef]
- Autran, C.A.; Kellman, B.P.; Kim, J.H.; Asztalos, E.; Blood, A.B.; Spence, E.C.H.; Patel, A.L.; Hou, J.; Lewis, N.E.; Bode, L. Human Milk Oligosaccharide Composition Predicts Risk of Necrotising Enterocolitis in Preterm Infants. Gut 2018, 67, 1064–1070. [Google Scholar] [CrossRef]
- Sodhi, C.P.; Wipf, P.; Yamaguchi, Y.; Fulton, W.B.; Kovler, M.; Niño, D.F.; Zhou, Q.; Banfield, E.; Werts, A.D.; Ladd, M.R.; et al. The Human Milk Oligosaccharides 2′-Fucosyllactose and 6′-Sialyllactose Protect against the Development of Necrotizing Enterocolitis by Inhibiting Toll-like Receptor 4 Signaling. Pediatr. Res. 2021, 89, 91–101. [Google Scholar] [CrossRef]
- Holst, A.Q.; Myers, P.; Rodríguez-García, P.; Hermes, G.D.A.; Melsaether, C.; Baker, A.; Jensen, S.R.; Parschat, K. Infant Formula Supplemented with Five Human Milk Oligosaccharides Shifts the Fecal Microbiome of Formula-Fed Infants Closer to That of Breastfed Infants. Nutrients 2023, 15, 3087. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, P.; Vogt, J.K.; Moll, J.M.; Bauer, V.; Arciszewska, M.; Tarneva, M.; Dosev, S.; Dimitrova, S.; Nikolova, O.; Nowak, M.; et al. Supplementation with 5-HMOs from Birth to 15 Months Shifts the Gut Microbiome Developmental Trajectory of Caesarean. Section Born Infants towards a Reference of Breastfed, Vaginally-Delivered Infants. In Proceedings of the ESPGHAN Conference, Vienna, Austria, 17–20 May 2023. AS03 Nutrition. [Google Scholar]
- Boulangé, C.L.; Pedersen, H.K.; Martin, F.P.; Siegwald, L.; Pallejà Caro, A.; Eklund, A.C.; Jia, W.; Zhang, H.; Berger, B.; Sprenger, N.; et al. An Extensively Hydrolyzed Formula Supplemented with Two Human Milk Oligosaccharides Modifies the Fecal Microbiome and Metabolome in Infants with Cow’s Milk Protein Allergy. Int. J. Mol. Sci. 2023, 24, 11422. [Google Scholar] [CrossRef]
- Hill, D.R.; Buck, R.H. Infants Fed Breastmilk or 2′-FL Supplemented Formula Have Similar Systemic Levels of Microbiota-Derived Secondary Bile Acids. Nutrients 2023, 15, 2339. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schönknecht, Y.B.; Moreno Tovar, M.V.; Jensen, S.R.; Parschat, K. Clinical Studies on the Supplementation of Manufactured Human Milk Oligosaccharides: A Systematic Review. Nutrients 2023, 15, 3622. https://doi.org/10.3390/nu15163622
Schönknecht YB, Moreno Tovar MV, Jensen SR, Parschat K. Clinical Studies on the Supplementation of Manufactured Human Milk Oligosaccharides: A Systematic Review. Nutrients. 2023; 15(16):3622. https://doi.org/10.3390/nu15163622
Chicago/Turabian StyleSchönknecht, Yannik Bernd, María Virginia Moreno Tovar, Stina Rikke Jensen, and Katja Parschat. 2023. "Clinical Studies on the Supplementation of Manufactured Human Milk Oligosaccharides: A Systematic Review" Nutrients 15, no. 16: 3622. https://doi.org/10.3390/nu15163622
APA StyleSchönknecht, Y. B., Moreno Tovar, M. V., Jensen, S. R., & Parschat, K. (2023). Clinical Studies on the Supplementation of Manufactured Human Milk Oligosaccharides: A Systematic Review. Nutrients, 15(16), 3622. https://doi.org/10.3390/nu15163622