
Concordance between Dash Diet and Hypertension: Results from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
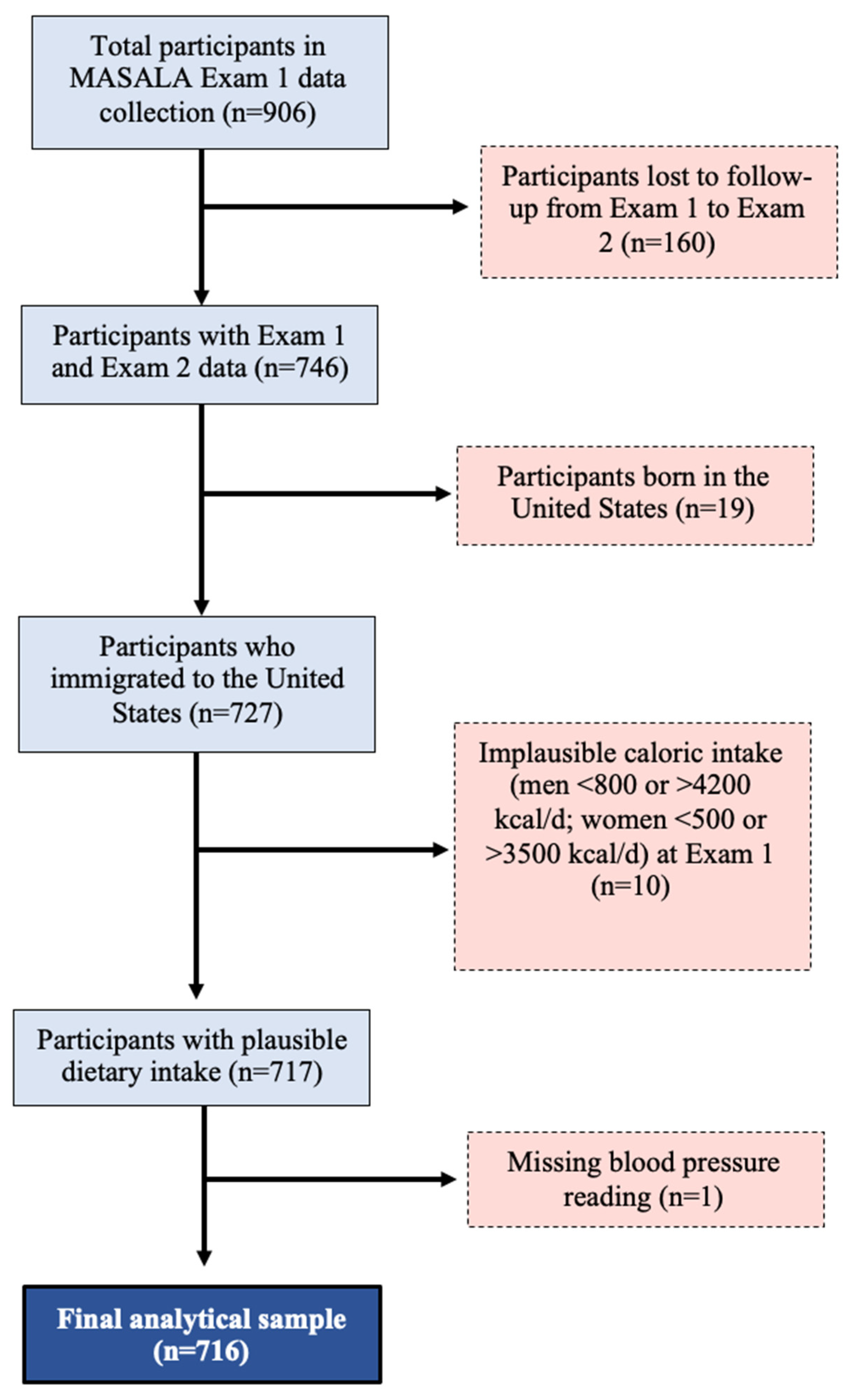
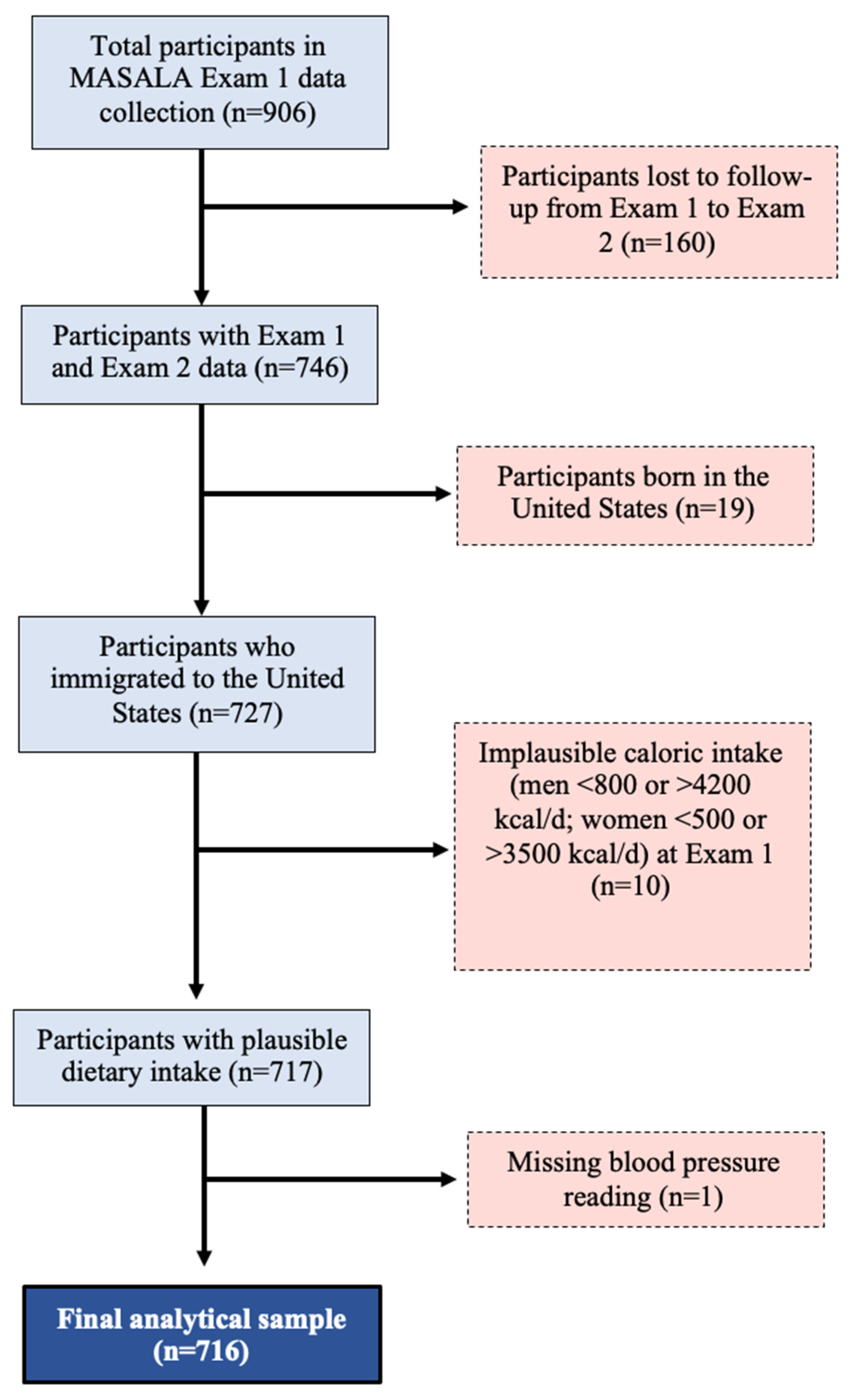
2.1. Study Population
2.2. Analytical Dataset
2.3. Data Collection
2.4. Creation of the DASH Diet Score
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Volgman, A.S.; Palaniappan, L.S.; Aggarwal, N.T.; Gupta, M.; Khandelwal, A.; Krishnan, A.V.; Lichtman, J.H.; Mehta, L.S.; Patel, H.N.; Shah, K.S.; et al. Atherosclerotic Cardiovascular Disease in South Asians in the United States: Epidemiology, Risk Factors, and Treatments: A Scientific Statement from the American Heart Association. Circulation 2018, 138, e1–e34. [Google Scholar] [CrossRef]
- Carey, R.M.; Whelton, P.K.; 2017 ACC/AHA Hypertension Guideline Writing Committee. Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of the 2017 American College of Cardiology/American Heart Association Hypertension Guideline. Ann. Intern. Med. 2018, 168, 351–358. [Google Scholar] [CrossRef]
- King-Shier, K.M.; Dhaliwal, K.K.; Puri, R.; LeBlanc, P.; Johal, J. South Asians’ experience of managing hypertension: A grounded theory study. Patient Prefer. Adherence 2019, 13, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Agyemang, C.; Bhopal, R. Hypertension and cardiovascular disease endpoints by ethnic group: The promise of data linkage. Heart 2013, 99, 675–676. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Akhlaghi, M. Dietary Approaches to Stop Hypertension (DASH): Potential mechanisms of action against risk factors of the metabolic syndrome. Nutr. Res. Rev. 2020, 33, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Svetkey, L.P.; Simons-Morton, D.; Vollmer, W.M.; Appel, L.J.; Conlin, P.R.; Ryan, D.H.; Ard, J.; Kennedy, B.M. Effects of dietary patterns on blood pressure: Subgroup analysis of the Dietary Approaches to Stop Hypertension (DASH) randomized clinical trial. Arch. Intern. Med. 1999, 159, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Theodoridis, X.; Chourdakis, M.; Chrysoula, L.; Chroni, V.; Tirodimos, I.; Dipla, K.; Gkaliagkousi, E.; Triantafyllou, A. Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3261. [Google Scholar] [CrossRef]
- Kanaya, A.M.; Kandula, N.; Herrington, D.; Budoff, M.J.; Hulley, S.; Vittinghoff, E.; Liu, K. Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study: Objectives, Methods, and Cohort Description. Clin. Cardiol. 2013, 36, 713–720. [Google Scholar] [CrossRef]
- Gadgil, M.D.; Anderson, C.A.; Kandula, N.R.; Kanaya, A.M. Dietary Patterns Are Associated with Metabolic Risk Factors in South Asians Living in the United States. J. Nutr. 2015, 145, 1211–1217. [Google Scholar] [CrossRef]
- Kelemen, L.E.; Anand, S.S.; Vuksan, V.; Yi, Q.; Teo, K.K.; Devanesen, S.; Yusuf, S. Development and evaluation of cultural food frequency questionnaires for South Asians, Chinese, and Europeans in North America. J. Am. Diet. Assoc. 2003, 103, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Irwin, M.L.; Addy, C.L.; Whitt, M.C.; Stolarczyk, L.M. Moderate Physical Activity Patterns of Minority Women: The Cross-Cultural Activity Participation Study. J. Women’s Health Gend.-Based Med. 1999, 8, 805–813. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American heart association’s strategic impact goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed]
- Talegawkar, S.A.; Jin, Y.; Kandula, N.R.; Kanaya, A.M. Cardiovascular health metrics among South Asian adults in the United States: Prevalence and associations with subclinical atherosclerosis. Prev. Med. 2017, 96, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-Style Diet and Risk of Coronary Heart Disease and Stroke in Women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Daniel, G.D.; Chen, H.; Bertoni, A.G.; Rapp, S.R.; Fitzpatrick, A.L.; Luchsinger, J.A.; Wood, A.C.; Hughes, T.M.; Burke, G.L.; Hayden, K.M. DASH diet adherence and cognitive function: Multi-ethnic study of atherosclerosis. Clin. Nutr. ESPEN 2021, 46, 223–231. [Google Scholar] [CrossRef]
- Agresti, A. An Introduction to Categorical Data Analysis; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1996. [Google Scholar]
- Hosmer, D.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2000. [Google Scholar]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal Diagrams for Epidemiologic Research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef]
- Duvall, C.; Blumenthal, R.S.; Sharma, G. The CAC Consortium: Highlights from Four Years of Research (Expert Analysis). 2021. Available online: https://www.acc.org/latest-in-cardiology/articles/2021/03/08/13/15/the-cac-consortium (accessed on 8 March 2023).
- Uddin, S.M.I.; Mirbolouk, M.; Kianoush, S.; Orimoloye, O.A.; Dardari, Z.; Whelton, S.P.; Miedema, M.D.; Nasir, K.; Rumberger, J.A.; Shaw, L.J.; et al. Role of Coronary Artery Calcium for Stratifying Cardiovascular Risk in Adults With Hypertension. Hypertension 2019, 73, 983–989. [Google Scholar] [CrossRef]
- Sung, K.-C.; Lee, M.-Y.; Kim, J.-Y.; Park, J.B.; Cho, E.J.; Avolio, A. Prediction of incident hypertension with the coronary artery calcium score based on the 2017 ACC/AHA high blood pressure guidelines. Hypertens. Res. 2020, 43, 1293–1300. [Google Scholar] [CrossRef]
- Vanderweele, T.J.; Vansteelandt, S. Conceptual issues concerning mediation, interventions and composition. Stat. Its Interface 2009, 2, 457–468. [Google Scholar] [CrossRef]
- Shaw, L.J.; Min, J.K.; Nasir, K.; Xie, J.X.; Berman, D.S.; Miedema, M.D.; Whelton, S.P.; A Dardari, Z.; Rozanski, A.; Rumberger, J.; et al. Sex differences in calcified plaque and long-term cardiovascular mortality: Observations from the CAC Consortium. Eur. Heart J. 2018, 39, 3727–3735. [Google Scholar] [CrossRef]
- Stata; Version 16.1; StataCorp LLC: College Station, TX, USA, 2020.
- Tindall, A.M.; Stallings, V.A. Sex differences in cardiovascular risk may be related to sex differences in diet patterns: A narrative review. Ann. Hum. Biol. 2021, 48, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Gujral, U.P.; Narayan, K.V.; Kahn, S.E.; Kanaya, A.M. The relative associations of β-cell function and insulin sensitivity with glycemic status and incident glycemic progression in migrant Asian Indians in the United States: The MASALA study. J. Diabetes Its Complicat. 2014, 28, 45–50. [Google Scholar] [CrossRef]
- Gadgil, M.D.; Anderson, C.A.; Kandula, N.R.; Kanaya, A.M. Dietary Patterns in Asian Indians in the United States: An Analysis of the Metabolic Syndrome and Atherosclerosis in South Asians Living in America Study. J. Acad. Nutr. Diet. 2014, 114, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Karanja, N.M.; Obarzanek, E.; Lin, P.-H.; McCULLOUGH, M.L.; Phillips, K.M.; Swain, J.F.; Champagne, C.M.; Hoben, K.P. Descriptive Characteristics of the Dietary Patterns Used in the Dietary Approaches to Stop Hypertension Trial. J. Am. Diet. Assoc. 1999, 99, S19–S27. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. Int. Rev. J. 2017, 8, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J.; et al. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Francisco, S.C.; Araújo, L.F.; Griep, R.H.; Chor, D.; Molina, M.D.C.B.; Mil, J.G.; Bensenor, I.M.; Matos, S.M.A.; Barreto, S.M.; Giatti, L. Adherence to the Dietary Approaches to Stop Hypertension (DASH) and hypertension risk: Results of the Longitudinal Study of Adult Health (ELSA-Brasil). Br. J. Nutr. 2020, 123, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Bai, G.; Zhang, J.; Zhao, C.; Wang, Y.; Qi, Y.; Zhang, B. Adherence to a healthy lifestyle and a DASH-style diet and risk of hypertension in Chinese individuals. Hypertens. Res. 2017, 40, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Kesse-Guyot, E.; Czernichow, S.; Bertrais, S.; Estaquio, C.; Péneau, S.; Vergnaud, A.-C.; Chat-Yung, S.; Castetbon, K.; Deschamps, V.; et al. Dietary patterns and blood pressure change over 5-y follow-up in the SU.VI.MAX cohort. Am. J. Clin. Nutr. 2007, 85, 1650–1656. [Google Scholar] [CrossRef]
- Lelong, H.; Blacher, J.; Baudry, J.; Adriouch, S.; Galan, P.; Fezeu, L.; Hercberg, S.; Kesse-Guyot, E.; Günther, A.L.; Liese, A.D.; et al. Individual and Combined Effects of Dietary Factors on Risk of Incident Hypertension: Prospective Analysis From the NutriNet-Sante Cohort. Hypertension 2017, 70, 712–720. [Google Scholar] [CrossRef]
- Toledo, E.; de A Carmona-Torre, F.; Alonso, A.; Puchau, B.; A Zulet, M.; Martinez, J.A.; A Martinez-Gonzalez, M. Hypothesis-oriented food patterns and incidence of hypertension: 6-year follow-up of the SUN (Seguimiento Universidad de Navarra) prospective cohort. Public Health Nutr. 2010, 13, 338–349. [Google Scholar] [CrossRef]
- Flint, A.J.; Hu, F.B.; Glynn, R.J.; Jensen, M.K.; Franz, M.; Sampson, L.; Rimm, E.B. Whole grains and incident hypertension in men. Am. J. Clin. Nutr. 2009, 90, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Sun, D.; He, Y. Fruit and vegetables consumption and incident hypertension: Dose–response meta-analysis of prospective cohort studies. J. Hum. Hypertens. 2016, 30, 573–580. [Google Scholar] [CrossRef]
- Jiang, J.; Liu, M.; Troy, L.M.; Bangalore, S.; Hayes, R.B.; Parekh, N. Concordance with DASH diet and blood pressure change: Results from the Framingham Offspring Study (1991–2008). J. Hypertens. 2015, 33, 2223–2230. [Google Scholar] [CrossRef]
- Fidalgo, A.S.Q.; Vollenweider, P.; Marques-Vidal, P. No association between dietary markers and incident hypertension in a population-based sample. Clin. Nutr. ESPEN 2018, 28, 208–213. [Google Scholar] [CrossRef]
- Folsom, A.R.; Parker, E.D.; Harnack, L.J. Degree of Concordance With DASH Diet Guidelines and Incidence of Hypertension and Fatal Cardiovascular Disease. Am. J. Hypertens. 2007, 20, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Chien, L.-C.; Alman, A.C.; Snell-Bergeon, J.K. Associations of dietary patterns and nutrients with coronary artery calcification and pericardial adiposity in a longitudinal study of adults with and without type 1 diabetes. Eur. J. Nutr. 2021, 60, 3911–3925. [Google Scholar] [CrossRef] [PubMed]
- Frölich, S.; Lehmann, N.; Weyers, S.; Wahl, S.; Dragano, N.; Budde, T.; Kälsch, H.; Mahabadi, A.; Erbel, R.; Moebus, S.; et al. Association of dietary patterns with five-year degree and progression of coronary artery calcification in the Heinz Nixdorf Recall study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.-W.; Hao, Q.-Y.; Zhang, H.-F.; Li, X.-Z.; Yuan, Z.-M.; Guo, Y.; Wang, J.-F.; Zhang, S.-L.; Liu, P.-M. Low-Carbohydrate Diet Score and Coronary Artery Calcium Progression. Arter. Thromb. Vasc. Biol. 2020, 41, 491–500. [Google Scholar] [CrossRef]
- Weinberg, R.L.; Rubenfire, M.; Brook, R.D. Coronary artery calcium scoring in patients with hypertension. J. Hum. Hypertens. 2020, 34, 609–616. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Baranowski, T.; Subar, A.F.; Tooze, J.A.; Frongillo, E.A. Best Practices for Conducting and Interpreting Studies to Validate Self-Report Dietary Assessment Methods. J. Acad. Nutr. Diet. 2019, 119, 1801–1816. [Google Scholar] [CrossRef]
- Subar, A.F.; Kushi, L.H.; Lerman, J.L.; Freedman, L.S. Invited Commentary: The Contribution to the Field of Nutritional Epidemiology of the Landmark 1985 Publication by Willett et al. Am. J. Epidemiol. 2017, 185, 1124–1129. [Google Scholar] [CrossRef]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013; Volume 40. [Google Scholar]
- Gadgil, M.D.; Kandula, N.R.; Kanaya, A.M. Acculturation is Associated with Dietary Patterns in South Asians in America. J. Immigr. Minor. Health 2020, 22, 1135–1140. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Total Study Population (n = 716) | DASH Score 13–20 (Lowest) (n = 127) | DASH Score 21–28 (n = 444) | DASH Score 29–35 (Highest) (n = 145) | p Value |
|---|---|---|---|---|---|
| Demographic and Diet Information (Exam 1) | |||||
| Age (y) (mean (SD)) | 55.6 (9.2) | 54.2 (9.6) | 55.9 (9.2) | 55.6 (9.0) | 0.18 |
| Women (n (%)) | 322 (45.0) | 38 (29.9) | 197 (44.4) | 87 (60) | <0.001 |
| Percent of life lived in U.S. (mean (SD)) | 48.6 (16.7) | 51.2 (17.4) | 48.8 (16.8) | 45.8 (15.4) | 0.03 |
| Bachelor’s Degree or Higher (n (%)) | 640 (89.4) | 108 (85.0) | 399 (89.9) | 133 (91.7) | 0.18 |
| Income > $100 K (n (%)) | 461 (66.4) | 85 (67.5) | 276 (64.9) | 100 (69.9) | 0.53 |
| Energy Intake (mean (SD)) | 1681.9 (492.1) | 1631.3 (489.2) | 1655.9 (508.5) | 1805.9 (421.5) | 0.003 |
| Behavioral Risk Factors (Exam 2) | |||||
| Never Smoked (n (%)) | 596 (83.2) | 92 (72.4) | 369 (83.1) | 135 (93.1) | <0.001 |
| No Alcohol Intake (n (%)) | 471 (65.8) | 55 (43.3) | 304 (68.5) | 112 (77.2) | <0.001 |
| Physical Activity * (n (%)) | 0.005 | ||||
| Poor | 102 (14.3) | 22 (17.3) | 67 (15.1) | 13 (9.0) | |
| Intermediate | 140 (19.6) | 35 (27.6) | 84 (18.9) | 21 (14.5) | |
| Ideal | 474 (66.2) | 70 (55.1) | 293 (66.0) | 111 (76.6) | |
| Characteristic | Total Study Population (n = 716) | DASH Score 13–20 (Lowest) (n = 127) | DASH Score 21–28 (n = 444) | DASH Score 29–35 (Highest) (n = 145) | p Value |
|---|---|---|---|---|---|
| Hypertension and Blood Pressure (Exam 2) | |||||
| Incident Hypertension (n (%)) | 0.01 | ||||
| None | 362 (50.6) | 65 (51.2) | 208 (46.9) | 89 (61.4) | |
| Incident (from Exam 1 to Exam 2) | 93 (13.0) | 20 (15.8) | 64 (14.4) | 9 (6.2) | |
| Prevalent/Existing from Exam 1 | 261 (36.5) | 42 (33.1) | 172 (38.7) | 47 (32.4) | |
| Systolic Blood Pressure (mmHg) (mean (SD)) | 127.8 (17.5) | 128.6 (15.6) | 128.3 (17.5) | 125.8 (18.9) | 0.29 |
| Diastolic Blood Pressure (mmHg) (mean (SD)) | 75.1 (9.6) | 77.0 (9.2) | 75.0 (9.7) | 73.6 (9.7) | 0.01 |
| Clinical Measurements (Exam 1) | |||||
| CAC Score Category (Exam 1) (n (%)) | 0.21 | ||||
| 0 | 414 (58.0) | 68 (53.5) | 253 (57.1) | 93 (64.6) | |
| 1–100 | 37 (5.2) | 9 (7.1) | 19 (4.3) | 9 (6.3) | |
| 101–400 | 123 (17.2) | 19 (15.0) | 84 (19.0) | 20 (13.9) | |
| >400 | 140 (19.6) | 31 (24.4) | 87 (19.6) | 22 (15.3) | |
| HDL Cholesterol (mean (SD)) | 49.9 (13.1) | 48.5 (12.6) | 50.1 (13.3) | 50.4 (12.8) | 0.44 |
| LDL Cholesterol (mean (SD)) | 111.3 (32.0) | 112.5 (28.8) | 111.4 (33.7) | 110.0 (29.1) | 0.81 |
| BMI (kg/m2) (mean (SD)) | 25.8 (3.9) | 25.8 (3.8) | 25.9 (4.0) | 25.5 (3.6) | 0.57 |
| Diabetes (n (%)) | 171 (23.9) | 31 (24.4) | 111 (25.0) | 29 (20.0) | 0.33 |
| DASH Score 13–20 (Lowest) (n = 127) | DASH Score 21–28 (n = 444) | DASH Score 29–35 (Highest) (n = 145) | Ptrend * | |||
|---|---|---|---|---|---|---|
| Reference | RRR/β (SE) | 95% CI | RRR/β (SE) | 95% CI | ||
| Incident Hypertension 1 | ||||||
| Unadjusted | 1.00 | 1.00 (0.29) | 0.56, 1.78 | 0.33 (0.14) | 0.14, 0.77 | 0.01 |
| Age Adjusted | 1.00 | 0.92 (0.27) | 0.51, 1.65 | 0.29 (0.13) | 0.12, 0.70 | 0.01 |
| Model 1 + | 1.00 | 0.97 (0.31) | 0.53, 1.80 | 0.32 (0.15) | 0.13, 0.79 | 0.01 |
| Model 2 ++ | 1.00 | 1.00 (0.32) | 0.53, 1.88 | 0.33 (0.16) | 0.13, 0.84 | 0.02 |
| Model 3 +++ | 1.00 | 1.00 (0.32) | 0.53, 1.89 | 0.33 (0.16) | 0.13, 0.85 | 0.02 |
| Prevalent Hypertension 1 | ||||||
| Unadjusted | 1.00 | 1.28 (0.29) | 0.83, 1.98 | 0.82 (0.22) | 0.48, 1.38 | 0.34 |
| Age Adjusted | 1.00 | 1.12 (0.27) | 0.70, 1.80 | 0.68 (0.20) | 0.38, 1.20 | 0.14 |
| Model 1 + | 1.00 | 1.28 (0.33) | 0.77, 2.11 | 0.85 (0.27) | 0.46, 1.57 | 0.47 |
| Model 2 ++ | 1.00 | 1.35 (0.38) | 0.77, 2.36 | 0.97 (0.34) | 0.49, 1.93 | 0.79 |
| Model 3 +++ | 1.00 | 1.36 (0.39) | 0.77, 2.37 | 1.01 (0.36) | 0.50, 2.02 | 0.89 |
| Systolic Blood Pressure | ||||||
| Unadjusted | 0.00 | −0.30 (1.76) | −3.75, 3.16 | −2.77 (2.12) | −6.94, 1.40 | 0.18 |
| Age Adjusted | 0.00 | −1.36 (1.67) | −4.63, 1.91 | −3.67 (2.01) | −7.62, 0.27 | 0.06 |
| Model 1 + | 0.00 | −0.58 (1.72) | −3.96, 2.80 | −2.45 (2.13) | −6.63, 1.74 | 0.24 |
| Model 2 ++ | 0.00 | −0.54 (1.72) | −3.92, 2.84 | −1.87 (2.14) | −6.08, 2.34 | 0.37 |
| Model 3 +++ | 0.00 | −0.58 (1.73) | −3.97, 2.81 | −2.04 (2.18) | −6.32, 2.23 | 0.34 |
| Diastolic Blood Pressure | ||||||
| Unadjusted | 0.00 | −2.02 (0.96) | −3.91, −0.12 | −3.47 (1.16) | −5.76, −1.18 | 0.003 |
| Age Adjusted | 0.00 | −1.83 (0.96) | −3.72, 0.05 | −3.32 (1.16) | −5.59, −1.04 | 0.004 |
| Model 1 + | 0.00 | −0.81 (0.97) | −2.72, 1.09 | −1.51 (1.20) | −3.87, 0.86 | 0.21 |
| Model 2 ++ | 0.00 | −0.87 (0.98) | −2.79, 1.04 | −1.17 (1.21) | −3.55, 1.22 | 0.35 |
| Model 3 +++ | 0.00 | −0.87 (0.98) | −2.79, 1.04 | −1.17 (1.23) | −3.59, 1.25 | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, B.M.; Deierlein, A.L.; Kanaya, A.M.; Talegawkar, S.A.; O’Connor, J.A.; Gadgil, M.D.; Lin, Y.; Parekh, N. Concordance between Dash Diet and Hypertension: Results from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study. Nutrients 2023, 15, 3611. https://doi.org/10.3390/nu15163611
Hussain BM, Deierlein AL, Kanaya AM, Talegawkar SA, O’Connor JA, Gadgil MD, Lin Y, Parekh N. Concordance between Dash Diet and Hypertension: Results from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study. Nutrients. 2023; 15(16):3611. https://doi.org/10.3390/nu15163611
Chicago/Turabian StyleHussain, Bridget Murphy, Andrea L. Deierlein, Alka M. Kanaya, Sameera A. Talegawkar, Joyce A. O’Connor, Meghana D. Gadgil, Yong Lin, and Niyati Parekh. 2023. "Concordance between Dash Diet and Hypertension: Results from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study" Nutrients 15, no. 16: 3611. https://doi.org/10.3390/nu15163611
APA StyleHussain, B. M., Deierlein, A. L., Kanaya, A. M., Talegawkar, S. A., O’Connor, J. A., Gadgil, M. D., Lin, Y., & Parekh, N. (2023). Concordance between Dash Diet and Hypertension: Results from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study. Nutrients, 15(16), 3611. https://doi.org/10.3390/nu15163611