

Relationship between Nutritional Risk, Clinical and Demographic Characteristics, and Pressure Ulcers in Patients with Severe Acquired Brain Injuries Attending a Rehabilitative Program

 , , ,
, , ,  , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
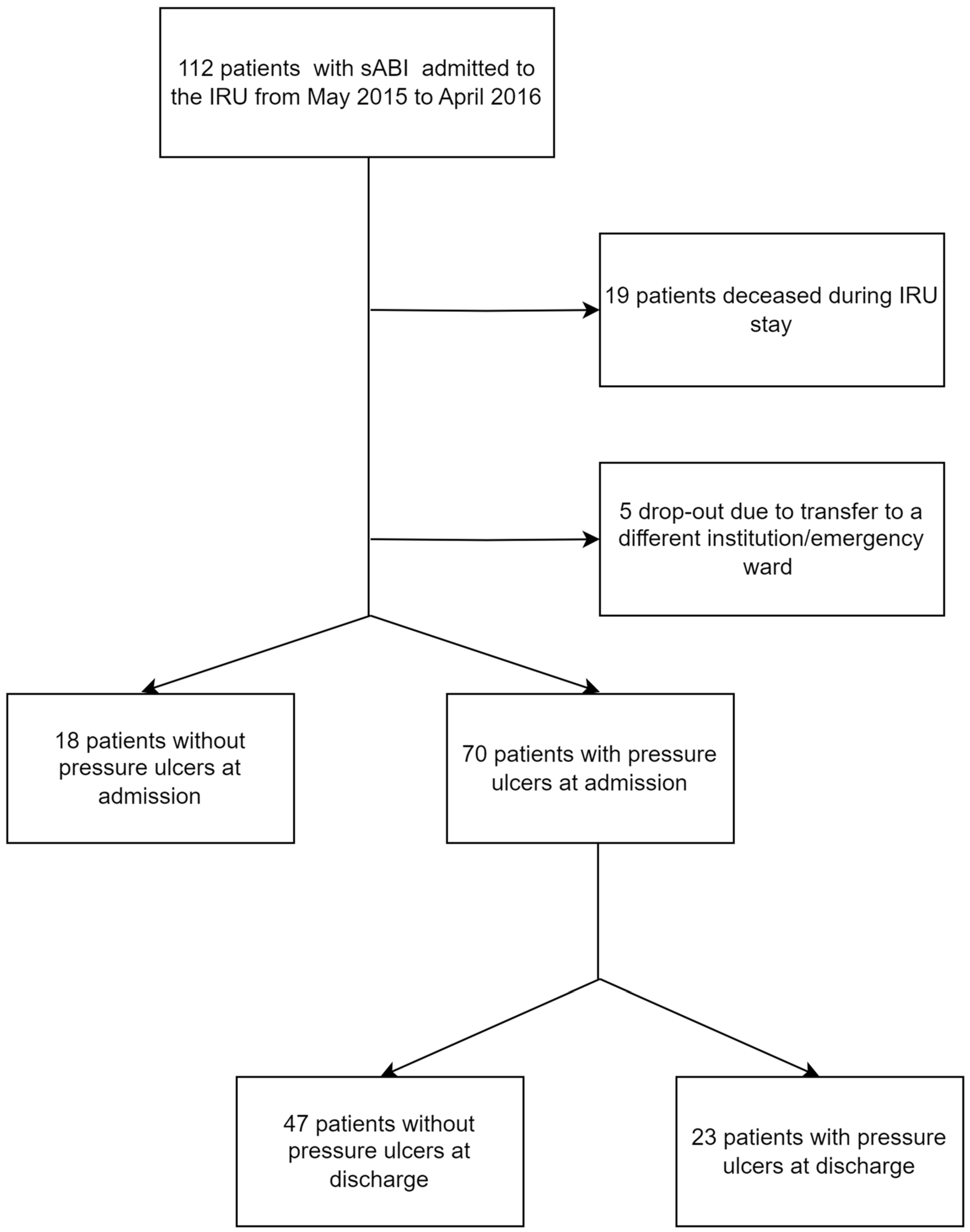
2.2. Study Population
2.3. Clinical Evaluation
2.4. Nutritional Risk and Anthropometric Measures Assessment
2.5. Biochemical Data, Nutritional Risk, and Inflammatory Status Assessment
2.6. Demographical and Clinical Data
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Patients with and without PU at Admission
3.2. Characteristics of Patients with and without PU at Discharge
3.3. Association between the Presence of PU at Discharge and Clinical Characteristics at Admission
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavezzi, S.; Bargellesi, S.; Cassio, A.; DE Tanti, A.; Gatta, G.; Hakiki, B.; Lombardi, F.; Montis, A.; Posteraro, F.; Scarponi, F.; et al. Redefining a minimal rehabili-tation assessment protocol for severe acquired brain injuries. Eur. J. Phys. Rehabil. Med. 2022, 58, 584–591. [Google Scholar] [CrossRef]
- Hakiki, B.; Donnini, I.; Romoli, A.M.; Draghi, F.; Maccanti, D.; Grippo, A.; Scarpino, M.; Maiorelli, A.; Sterpu, R.; Atzori, T.; et al. Clinical, Neurophysiological, and Genetic Predictors of Recovery in Patients with Severe Acquired Brain Injuries (PRABI): A Study Protocol for a Longitudinal Observational Study. Front. Neurol. 2022, 13, 711312. [Google Scholar] [CrossRef]
- de Almeida Medeiros, A.B.; da Conceição Dias Fernandes, M.I.; de Sá Tinôco, J.D.; Cossi, M.S.; de Oliveira Lopes, M.V.; de Carvalho Lira, A.L.B. Predictors of pressure ulcer risk in adult intensive care patients: A retrospective case-control study. Intensive Crit. Care Nurs. 2018, 45, 6–10. [Google Scholar] [CrossRef]
- Kopp Lugli, A.; de Watteville, A.; Hollinger, A.; Goetz, N.; Heidegger, C. Medical Nutrition Therapy in Critically Ill Patients Treated on Intensive and Intermediate Care Units: A Literature Review. J. Clin. Med. 2019, 8, 1395. [Google Scholar] [CrossRef]
- Zarei, E.; Madarshahian, E.; Nikkhah, A.; Khodakarim, S. Incidence of pressure ulcers in intensive care units and direct costs of treatment: Evidence from Iran. J. Tissue Viability 2019, 28, 70–74. [Google Scholar] [CrossRef]
- Wong, A.; Goh, G.; Banks, M.D.; Bauer, J.D. Economic Evaluation of Nutrition Support in the Prevention and Treatment of Pressure Ulcers in Acute and Chronic Care Settings: A Systematic Review. J. Parenter. Enter. Nutr. 2019, 43, 376–400. [Google Scholar] [CrossRef]
- Osis, S.L.; Diccini, S. Incidence and risk factors associated with pressure injury in patients with traumatic brain injury. Int. J. Nurs. Pract. 2020, 26, e12821. [Google Scholar] [CrossRef]
- Gaspar, S.; Peralta, M.; Marques, A.; Budri, A.; Gaspar de Matos, M. Effectiveness on hospital-acquired pressure ulcers prevention: A systematic review. Int. Wound J. 2019, 16, 1087–1102. [Google Scholar] [CrossRef]
- Aadal, L.; Mortensen, J.; Nielsen, J.F. Weight reduction after severe brain injury: A challenge during the rehabilitation course. J. Neurosci. Nurs. 2015, 47, 85–90. [Google Scholar] [CrossRef]
- Dhandapani, M.; Dhandapani, S.; Agarwal, M.; Mahapatra, A.K. Pressure ulcer in patients with severe traumatic brain injury: Significant factors and association with neurological outcome. J. Clin. Nurs. 2014, 23, 1114–1119. [Google Scholar] [CrossRef]
- Aadal, L.; Holst, M.; Rasmussen, H.H.; Nielsen, J.F.; Odgaard, L. Malnutrition in Patients with Moderate to Severe Acquired Brain Injury: Prevalence During 4 Weeks of Subacute Rehabilitation. J. Neurosci. Nurs. 2023, 55, 38–44. [Google Scholar] [CrossRef]
- Vázquez-Lorente, H.; Herrera-Quintana, L.; Molina-López, J.; Zapata-Soria, M.; Planells, E. Need of nutritional assessment and monitoring in a population with acquired brain injury: An analytical cross-sectional study. Nutr. Neurosci. 2022, 26, 525–534. [Google Scholar] [CrossRef]
- Aquilani, R.; Zuccarelli, G.C.; Maestri, R.; Rutili, C.; Colombo, M.; Condino, A.M.; Barbieri, A.; Cecchetti, A.; Vanzati, S.; Bonazza, E.; et al. Inflammation, pressure ulcers and poor functional status predict negative re-habilitation outcomes in postacute geriatric patients. Aging Clin. Exp. Res. 2021, 33, 463–467. [Google Scholar] [CrossRef]
- Montalcini, T.; Moraca, M.; Ferro, Y.; Romeo, S.; Serra, S.; Raso, M.G.; Rossi, F.; Sannita, W.G.; Dolce, G.; Pujia, A. Nutritional parameters predicting pressure ulcers and short-term mortality in patients with minimal conscious state as a result of traumatic and non-traumatic acquired brain injury. J. Transl. Med. 2015, 13, 305. [Google Scholar] [CrossRef]
- Sachs, M.B.; Wolffbrandt, M.M.; Poulsen, I. Prevention of pressure ulcers in patients undergoing subacute rehabilitation after severe brain injury: An observational study. J. Clin. Nurs. 2018, 27, 2776–2784. [Google Scholar] [CrossRef]
- Saghaleini, S.H.; Dehghan, K.; Shadvar, K.; Sanaie, S.; Mahmoodpoor, A.; Ostadi, Z. Pressure Ulcer and Nutrition. Indian J. Crit. Care Med. 2018, 22, 283–289. [Google Scholar] [CrossRef]
- Munoz, N.; Posthauer, M.E.; Cereda, E.; Schols, J.M.; Haesler, E. The Role of Nutrition for Pressure Injury Prevention and Healing: The 2019 International Clinical Practice Guideline Recommendations. Adv. Skin Wound Care 2020, 33, 123–136. [Google Scholar] [CrossRef]
- Munoz, N.; Posthauer, M.E. Nutrition strategies for pressure injury management: Implementing the 2019 International Clinical Practice Guideline. Nutr. Clin. Pract. 2022, 37, 567–582. [Google Scholar] [CrossRef]
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of Pressure Ulcers: Quick Reference Guide; National Pressure Ulcer Advisory Panel: Washington, DC, USA, 2019. [Google Scholar]
- Serón-Arbeloa, C.; Labarta-Monzón, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-López, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition Screening and Assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef]
- BAPEN. The ‘MUST’ Report Nutritional Screening of Adults: A Multidisciplinary Responsibility. Development and Use of the ‘Malnutrition Universal Screening Tool’ (‘MUST’) for Adults. Chairman of Malnutrition Advisory Group (MAG) and Editor: Professor Marinos Elia. 2003. Available online: www.bapen.org (accessed on 15 July 2023).
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Furuyama, T.; Yamashita, S.; Yoshiya, K.; Kurose, S.; Yoshino, S.; Nakayama, K.; Inoue, K.; Morisaki, K.; Matsumoto, T.; Mori, M. The Controlling Nutritional (CONUT) score is significantly associated with complete ulcer healing in patients with critical limb ischemia. Ann. Vasc. Surg. 2020, 66, 510–517. [Google Scholar] [CrossRef]
- Cecchi, F.; Diverio, M.; Arienti, C.; Corbella, E.; Marrazzo, F.; Speranza, G.; DEL Zotto, E.; Poggianti, G.; Gigliotti, F.; Polcaro, P.; et al. Development and implementation of a stroke rehabilitation integrated care pathway in an Italian no profit institution: An observational study. Eur. J. Phys. Rehabil. Med. 2020, 56, 713–724. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek Listy. 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Chung, M.L.; Widdel, M.; Kirchhoff, J.; Sellin, J.; Jelali, M.; Geiser, F.; Mücke, M.; Conrad, R. Risk factors for pressure ulcers in adult patients: A meta-analysis on sociodemographic factors and the Braden scale. J. Clin. Nurs. 2022, 32, 1979–1992. [Google Scholar] [CrossRef]
- Lima Serrano, M.; González Méndez, M.I.; Carrasco Cebollero, F.M.; Lima Rodríguez, J.S. Risk factors for pressure ulcer development in Intensive Care Units: A systematic review. Factores de riesgo asociados al desarrollo de úlceras por presión en unidades de cuidados intensivos de adultos: Revisión sistemática. Med. Intensiva. 2017, 41, 339–346. [Google Scholar] [CrossRef]
- Charalambous, C.; Koulori, A.; Vasilopoulos, A.; Roupa, Z. Evaluation of the Validity and Reliability of the Waterlow Pressure Ulcer Risk Assessment Scale. Med. Arch. 2018, 72, 141–144. [Google Scholar] [CrossRef]
- Chung, M.-L.; Widdel, M.; Kirchhoff, J.; Sellin, J.; Jelali, M.; Geiser, F.; Mücke, M.; Conrad, R. Risk Factors for Pressure Injuries in Adult Patients: A Narrative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 761. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Chen, T.-L.; Cheng, C.-C.; Yang, Y.-C.; Wang, J.-H.; Yip, H.-T.; Hsu, C.-Y.; Cheng, H.-Y. High-Intensity Post-Stroke Rehabilitation Is Associated with Lower Risk of Pressure Ulcer Development in Patients with Stroke: Real-World Evidence from a Nationwide, Population-Based Cohort Study. Medicina 2022, 58, 402. [Google Scholar] [CrossRef]
- Anghel, S.; Kerr, K.W.; Valladares, A.F.; Kilgore, K.M.; Sulo, S. Identifying patients with malnutrition and improving use of nutrition interventions: A quality study in four US hospitals. Nutrition 2021, 91–92, 111360. [Google Scholar] [CrossRef]
- Rossato, E.; Verzini, E.; Scandola, M.; Ferrari, F.; Bonadiman, S. Role of LCF scale as an outcome prognostic index in patients with traumatic brain injury. Neurol. Sci. 2021, 42, 2747–2752. [Google Scholar] [CrossRef]
- Hakiki, B.; Draghi, F.; Scarpino, M.; Portaccio, E.; Romoli, A.; Mannini, A.; Atzori, T.; Lolli, F.; Macchi, C.; Grippo, A. Critical illness polyneuromyopathy: Functional impact after severe acquired brain injuries. Acta Neurol. Scand. 2020, 142, 574–584. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Luisi, M.L.E.; Alicante, P.; Ballarin, G.; Biffi, B.; Gheri, C.F.; Scalfi, L. The Assessment of the Risk of Malnutrition (Undernutrition) in Stroke Patients. Nutrients 2023, 15, 683. [Google Scholar] [CrossRef]
- Huang, X.-W.; Luo, J.-J.; Baldinger, B. The controlling nutritional status score and clinical outcomes in patients with heart failure: Pool analysis of observational studies. Front. Cardiovasc. Med. 2022, 9, 961141. [Google Scholar] [CrossRef]
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef]


{kind=link}
| No PU at Admission (n = 18) N (%) Median [IQR] | PU at Admission (n = 70) N (%) Median [IQR] | p-Value | |
|---|---|---|---|
| Age | 61 [15] | 64 [20] | 0.354 |
| Sex (women) | 4 (22.2%) | 24 (34.3%) | 0.327 |
| BMI (kg/m2) | 25.8 [3.6] | 25.1 [6.6] | 0.280 |
| CRS at admission | 12 [10.5] | 14 [16.75] | 0.233 |
| LCF at admission | 4 [2] | 3 [2] | 0.456 |
| FOIS at admission | 1 [0] | 1 [0] | 0.402 |
| DRS at admission | 19.5 [11] | 21 [8] | 0.176 |
| FIM at admission | 19 [9] | 18 [3] | 0.193 |
| Etiology | 0.637 | ||
| Traumatic | 5 (27.8%) | 21 (30.0%) | |
| Hemorrhagic | 4 (22.2%) | 10 (14.3%) | |
| Ischemic | 4 (22.2%) | 13 (18.6%) | |
| Anoxic | 3 (16.7%) | 17 (24.3%) | |
| Other | 2 (11.1%) | 9 (12.9%) | |
| Time post event (days) | 30 [28] | 44 [39] | 0.034 |
| KCal tot | 1800 [27.8] | 1800 [426.8] | 0.270 |
| MUST at admission | 2 [0] | 2 [2] | 0.008 |
| CONUT at admission | 5.5 [4.25] | 5 [4] | 0.145 |
| Neutrophil/lymphocytes at admission | 3.3 [3.6] | 4 [4.1] | 0.213 |
| No PU at Discharge (n = 47) N (%) Median [IQR] | PU at Discharge (n = 23) N (%) Median [IQR] | p-Value | |
|---|---|---|---|
| Age | 65 [19] | 63 [28] | 0.920 |
| Sex (women) | 21 (44.7%) | 3 (13.0%) | 0.009 |
| BMI (kg/m2) at admission | 25 [6] | 24 [8] | 0.658 |
| CRS at admission | 16 [16] | 10 [19] | 0.106 |
| LCF at admission | 3 [1] | 2 [2] | 0.042 |
| DRS at admission | 21 [8] | 23.5 [9] | 0.128 |
| FIM at admission | 18 [3] | 18 [2] | 0.460 |
| Etiology | 0.732 | ||
| Traumatic | 15 (31.9%) | 6 (26.1%) | |
| Hemorrhagic | 5 (10.6%) | 5 (21.7%) | |
| Ischemic | 10 (21.3%) | 3 (13.0%) | |
| Anoxic | 12 (25.5%) | 5 (21.7%) | |
| Other | 5 (10.6%) | 4 (17.4%) | |
| Time post event (days) | 43 [58] | 45 [32] | 0.661 |
| Length of stay (days) | 157 [101] | 170 [86] | 0.761 |
| Ulcers severity (higher grade) at admission | 2 [2] | 3 [1] | 0.005 |
| Kcal tot at admission | 1800 [379] | 1800 [505] | 0.900 |
| Arm circumference at admission | 28 [5] | 29 [5] | 0.677 |
| MUST at admission | 2 [2] | 2 [2] | 0.624 |
| CONUT at admission | 4 [3.5] | 6 [6] | 0.039 |
| Neutrophil/lymphocytes at admission | 3.8 [2.9] | 3.8 [4.8] | 0.600 |
| R2 = 0.351 | B | SE | p-Value | OR | 95% CI (OR) | |
|---|---|---|---|---|---|---|
| Inferior | Superior | |||||
| Sex | −1.308 | 0.773 | 0.090 | 0.270 | 0.059 | 1.229 |
| LCF at admission | −0.505 | 0.273 | 0.064 | 0.603 | 0.353 | 1.030 |
| Ulcers severity (higher grade) | 0.723 | 0.367 | 0.049 | 2.060 | 1.004 | 4.226 |
| CONUT | 0.312 | 0.146 | 0.032 | 1.366 | 1.027 | 1.818 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheri, C.F.; Scalfi, L.; Biffi, B.; Pancani, S.; Madiai, S.; Di Vincenzo, O.; Ghaderi, M.; Celoni, R.; Dalladonna, M.; Draghi, F.; et al. Relationship between Nutritional Risk, Clinical and Demographic Characteristics, and Pressure Ulcers in Patients with Severe Acquired Brain Injuries Attending a Rehabilitative Program. Nutrients 2023, 15, 3336. https://doi.org/10.3390/nu15153336
Gheri CF, Scalfi L, Biffi B, Pancani S, Madiai S, Di Vincenzo O, Ghaderi M, Celoni R, Dalladonna M, Draghi F, et al. Relationship between Nutritional Risk, Clinical and Demographic Characteristics, and Pressure Ulcers in Patients with Severe Acquired Brain Injuries Attending a Rehabilitative Program. Nutrients. 2023; 15(15):3336. https://doi.org/10.3390/nu15153336
Chicago/Turabian StyleGheri, Chiara Francesca, Luca Scalfi, Barbara Biffi, Silvia Pancani, Sara Madiai, Olivia Di Vincenzo, Michele Ghaderi, Rebecca Celoni, Mara Dalladonna, Francesca Draghi, and et al. 2023. "Relationship between Nutritional Risk, Clinical and Demographic Characteristics, and Pressure Ulcers in Patients with Severe Acquired Brain Injuries Attending a Rehabilitative Program" Nutrients 15, no. 15: 3336. https://doi.org/10.3390/nu15153336
APA StyleGheri, C. F., Scalfi, L., Biffi, B., Pancani, S., Madiai, S., Di Vincenzo, O., Ghaderi, M., Celoni, R., Dalladonna, M., Draghi, F., Maccanti, D., Macchi, C., Romoli, A. M., Cecchi, F., Hakiki, B., & Luisi, M. L. E. (2023). Relationship between Nutritional Risk, Clinical and Demographic Characteristics, and Pressure Ulcers in Patients with Severe Acquired Brain Injuries Attending a Rehabilitative Program. Nutrients, 15(15), 3336. https://doi.org/10.3390/nu15153336