
Vitamin E and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses

Abstract
1. Introduction
2. Methods
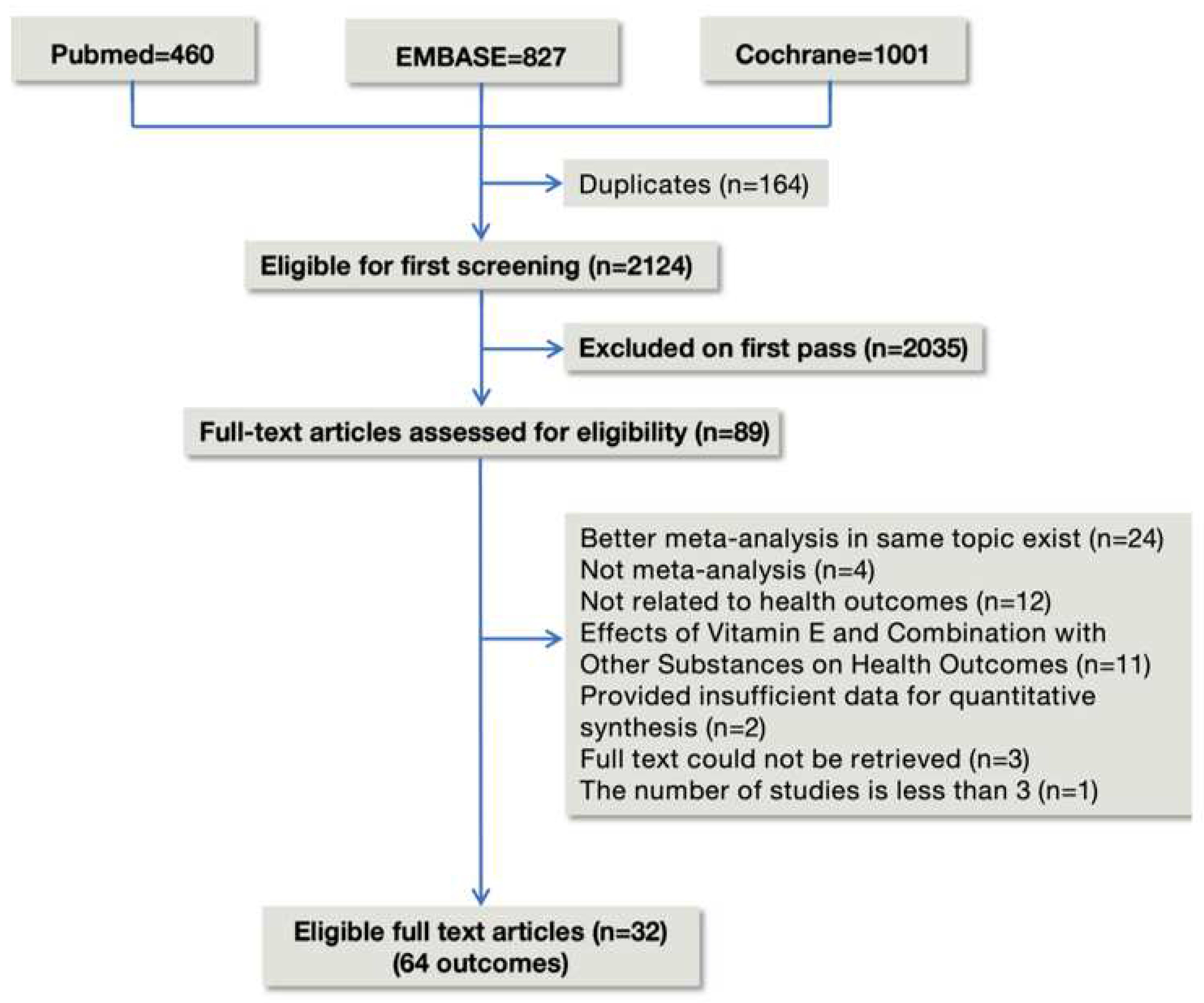
2.1. Literature Search and Selection Criteria
2.2. Selection of Meta-Analyses
2.3. Data Extraction
2.4. Methodological Quality Assessment
2.5. Data Analysis
2.6. Patient Involvement
3. Results
3.1. Characteristics of Meta-Analyses
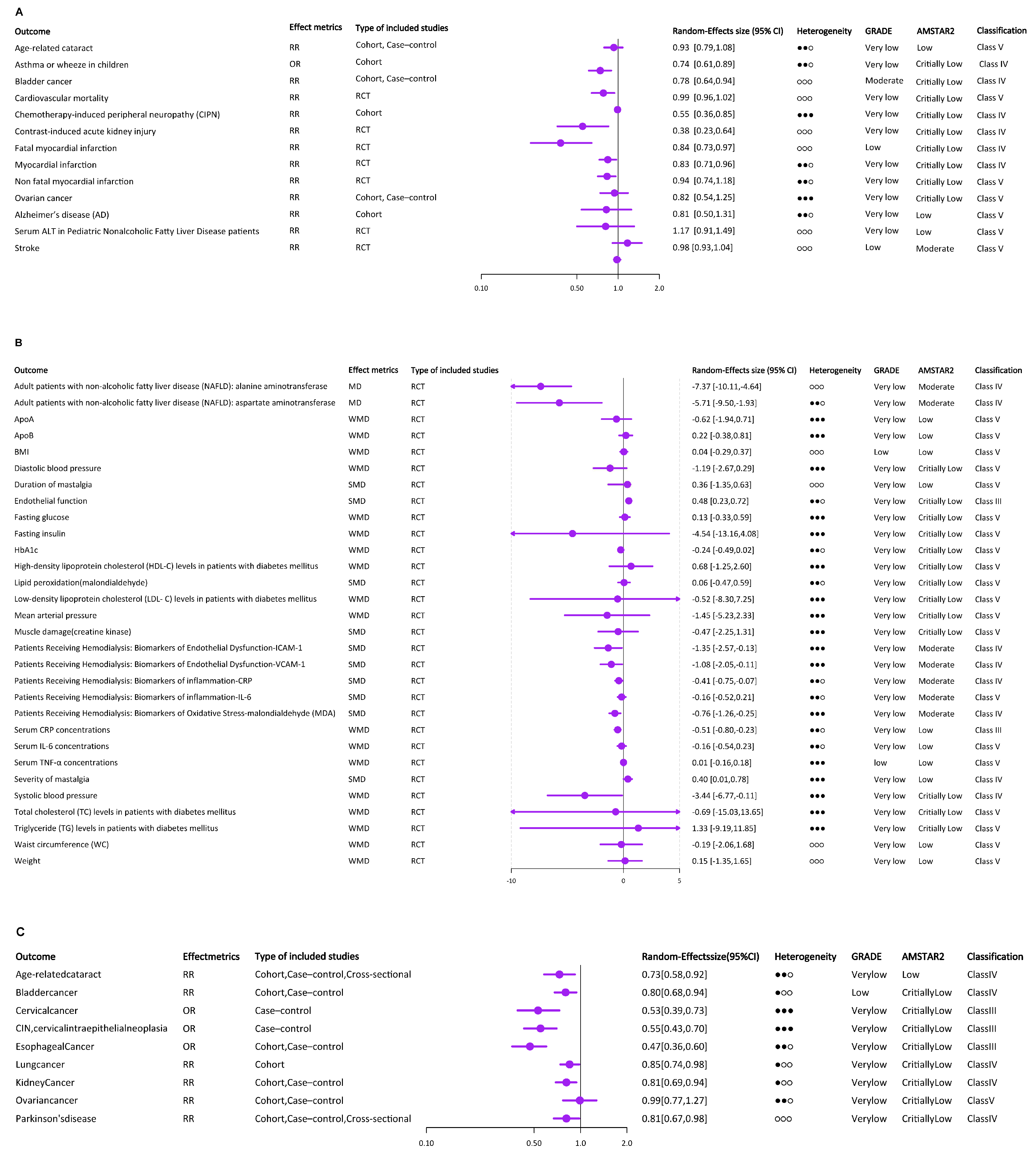
3.2. Supplemental Vitamin E Intake
3.2.1. Cardiovascular System
3.2.2. Cancer
3.2.3. Special Population
3.2.4. Nervous System
3.2.5. Others
3.3. Dietary Vitamin E Intake
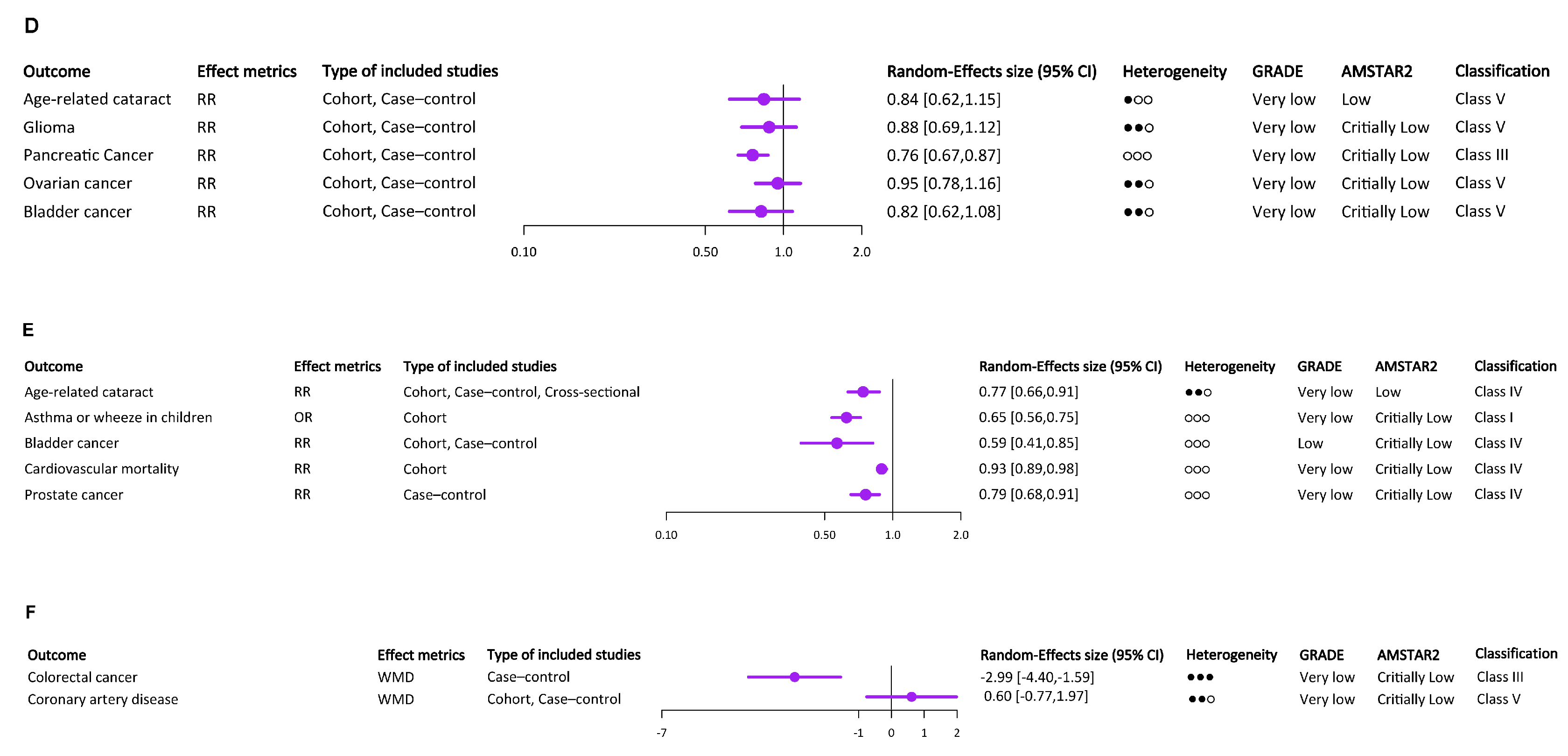
3.4. Total Vitamin E Intake
3.5. Circulating α-Tocopherol Levels
3.6. Heterogeneity between Primary Studies
3.7. Publication Bias of Included Studies
3.8. AMSTAR and GRADE Classification of Included Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, G.Y.; Han, S.N. The Role of Vitamin E in Immunity. Nutrients 2018, 10, 1614. [Google Scholar] [CrossRef] [PubMed]
- Traber, M.G.; Head, B. Vitamin E: How much is enough, too much and why! Free Radic. Biol. Med. 2021, 177, 212–225. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, Agricultural Research Service. FoodData Centralexternal Link Disclaimer; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2019.
- Rychter, A.M.; Hryhorowicz, S.; Słomski, R.; Dobrowolska, A.; Krela-Kaźmierczak, I. Antioxidant effects of vitamin E and risk of cardiovascular disease in women with obesity—A narrative review. Clin. Nutr. 2022, 41, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Cook, N.R.; Gaziano, J.M.; Gordon, D.; Ridker, P.M.; Manson, J.E.; Hennekens, C.H.; Buring, J.E. Vitamin E in the primary prevention of cardiovascular disease and cancer: The Women’s Health Study: A randomized controlled trial. JAMA 2005, 294, 56–65. [Google Scholar] [CrossRef]
- Peh, H.Y.; Tan, W.D.; Liao, W.; Wong, W.F. Vitamin E therapy beyond cancer: Tocopherol versus tocotrienol. Pharmacol. Ther. 2016, 162, 152–169. [Google Scholar] [CrossRef]
- Icer, M.A.; Arslan, N.; Gezmen-Karadag, M. Effects of vitamin E on neurodegenerative diseases: An update. Acta Neurobiol. Exp. 2021, 81, 21–33. [Google Scholar] [CrossRef]
- Christen, W.G.; Glynn, R.J.; Chew, E.Y.; Buring, J.E. Vitamin E and age-related macular degeneration in a randomized trial of women. Ophthalmology 2010, 117, 1163–1168. [Google Scholar] [CrossRef]
- Podszun, M.C.; Frank, J. Impact of vitamin E on redox biomarkers in non-alcoholic fatty liver disease. Redox Biol. 2021, 42, 101937. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Foroutan, F.; Guyatt, G.; Zuk, V.; Vandvik, P.O.; Alba, A.C.; Mustafa, R.; Vernooij, R.; Arevalo-Rodriguez, I.; Munn, Z.; Roshanov, P.; et al. GRADE Guidelines 28: Use of GRADE for the assessment of evidence about prognostic factors: Rating certainty in identification of groups of patients with different absolute risks. J. Clin. Epidemiol. 2020, 121, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef]
- Jayedi, A.; Rashidy-Pour, A.; Parohan, M.; Zargar, M.S.; Shab-Bidar, S. Dietary and circulating vitamin C, vitamin E, β-carotene and risk of total cardi-ovascular mortality: A systematic review and dose–response meta-analysis of prospective observational studies. Public Health Nutr. 2019, 22, 1872–1887. [Google Scholar] [CrossRef] [PubMed]
- Asbaghi, O.; Sadeghian, M.; Nazarian, B.; Sarreshtedari, M.; Mozaffari-Khosravi, H.; Maleki, V.; Alizadeh, M.; Shokri, A.; Sadeghi, O. The effect of vitamin E supplementation on selected inflammatory biomarkers in adults: A systematic review and meta-analysis of randomized clinical trials. Sci. Rep. 2020, 10, 17234. [Google Scholar] [CrossRef] [PubMed]
- Hamedi-Kalajahi, F.; Zarezadeh, M.; Dehghani, A.; Musazadeh, V.; Kolahi, A.; Shabbidar, S.; Djafarian, K. A systematic review and meta-analysis on the impact of oral vitamin E supplementation on apolipoproteins A1 and B100. Clin. Nutr. ESPEN 2021, 46, 106–114. [Google Scholar] [CrossRef]
- Loffredo, L.; Perri, L.; Di Castelnuovo, A.; Iacoviello, L.; De Gaetano, G.; Violi, F. Supplementation with vitamin E alone is associated with reduced myocardial infarction: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 354–363. [Google Scholar] [CrossRef]
- Ashor, A.W.; Siervo, M.; Lara, J.; Oggioni, C.; Afshar, S.; Mathers, J.C. Effect of vitamin C and vitamin E supplementation on endothelial function: A systematic review and meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 113, 1182–1194. [Google Scholar] [CrossRef]
- Emami, M.R.; Safabakhsh, M.; Alizadeh, S.; Asbaghi, O.; Khosroshahi, M.Z. Effect of vitamin E supplementation on blood pressure: A systematic review and meta-analysis. J. Hum. Hypertens. 2019, 33, 499–507. [Google Scholar] [CrossRef]
- Chen, F.; Li, Q.; Yu, Y.; Yang, W.; Shi, F.; Qu, Y. Association of vitamin C, vitamin D, vitamin E and risk of bladder cancer: A meta-analysis. Sci. Rep. 2015, 5, 9599. [Google Scholar] [CrossRef]
- Leng, Y.; Zhou, H.; Meng, F.; Tian, T.; Xu, J.; Yan, F. Association of vitamin E on the risk of ovarian cancer: A meta-analysis. Biosci. Rep. 2019, 39, BSR20193311. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.U.; Yeom, J.; Kim, W. Beneficial Effects of Vitamin E Supplementation on Endothelial Dysfunction, Inflammation, and Oxidative Stress Biomarkers in Patients Receiving Hemodialysis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Mol. Sci. 2021, 22, 11923. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.H.; Kim, S.N.; Park, H.W.; Chung, S.; Kim, K.S. Could vitamin E prevent contrast-induced acute kidney injury? A systematic review and meta-analysis. J. Korean Med. Sci. 2017, 32, 1468. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Zhang, S.; Tao, A.; Chen, G.; Zhang, M. Influence of vitamin E supplementation on glycaemic control: A meta-analysis of randomised controlled trials. PLoS ONE 2014, 9, e95008. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Falahi, E.; Barakatun-Nisak, M.Y.; Hanipah, Z.N.; Redzwan, S.M.; Yusof, L.M.; Gheitasvand, M.; Rezaie, F. Systematic review and meta-analyses of vitamin E (alpha-tocopherol) supplementation and blood lipid parameters in patients with diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102158. [Google Scholar] [CrossRef]
- Wu, H.; Zhang, C.; Wang, Y.; Li, Y. Does vitamin E prevent asthma or wheeze in children: A systematic review and meta-analysis. Paediatr. Respir. Rev. 2018, 27, 60–68. [Google Scholar] [CrossRef]
- Sarkhy, A.A.; Al-Hussaini, A.A.; Nobili, V. Does vitamin E improve the outcomes of pediatric nonalcoholic fatty liver disease? A systematic review and meta-analysis. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2014, 20, 143. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, W.; Xie, Z.; Wu, W.; Zhang, D. Vitamin E and risk of age-related cataract: A meta-analysis. Public Health Nutr. 2015, 18, 2804–2814. [Google Scholar] [CrossRef]
- Wang, W.; Li, J.; Zhang, H.; Wang, X.; Zhang, X. Effects of vitamin E supplementation on the risk and progression of AD: A systematic review and meta-analysis. Nutr. Neurosci. 2021, 24, 13–22. [Google Scholar] [CrossRef]
- Loh, H.C.; Lim, R.; Lee, K.W.; Ooi, C.Y.; Chuan, D.R.; Looi, I.; Hay, Y.K.; Khan, N.A.K. Effects of vitamin E on stroke: A systematic review with meta-analysis and trial sequential analysis. Stroke Vasc. Neurol. 2021, 6, 109–120. [Google Scholar] [CrossRef]
- Chen, J.; Shan, H.; Yang, W.; Zhang, J.; Dai, H.; Ye, Z. Vitamin E for the prevention of chemotherapy-induced peripheral neuropathy: A meta-analysis. Front. Pharmacol. 2021, 12, 684550. [Google Scholar] [CrossRef] [PubMed]
- Vadarlis, A.; Antza, C.; Bakaloudi, D.R.; Doundoulakis, I.; Kalopitas, G.; Samara, M.; Dardavessis, T.; Maris, T.; Chourdakis, M. Systematic review with meta-analysis: The effect of vitamin E supplementation in adult patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2021, 36, 311–319. [Google Scholar] [CrossRef]
- Hajizadeh, K.; Charandabi, S.M.A.; Hasanzade, R.; Mirghafourvand, M. Effect of vitamin E on severity and duration of cyclic mastalgia: A systematic review and meta-analysis. Complement. Ther. Med. 2019, 44, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Emami, M.R.; Jamshidi, S.; Zarezadeh, M.; Khorshidi, M.; Olang, B.; Hezaveh, Z.S.; Sohouli, M.; Aryaeian, N. Can vitamin E supplementation affect obesity indices? A systematic review and meta-analysis of twenty-four randomized controlled trials. Clin. Nutr. 2021, 40, 3201–3209. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.J.; Bo, Y.C.; Liu, X.X.; Qiu, C.G. Association of dietary vitamin E intake with risk of lung cancer: A dose-response meta-analysis. Asia Pac. J. Clin. Nutr. 2017, 26, 271–277. [Google Scholar]
- Shen, C.; Huang, Y.; Yi, S.; Fang, Z.; Li, L. Association of vitamin E intake with reduced risk of kidney cancer: A meta-analysis of obser-vational studies. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 3420. [Google Scholar] [CrossRef]
- Hu, X.; Li, S.; Zhou, L.; Zhao, M.; Zhu, X. Effect of vitamin E supplementation on uterine cervical neoplasm: A meta-analysis of case-control studies. PLoS ONE 2017, 12, e0183395. [Google Scholar] [CrossRef]
- Cui, L.; Li, L.; Tian, Y.; Xu, F.; Qiao, T. Association between dietary vitamin E intake and esophageal cancer risk: An updated meta-analysis. Nutrients 2018, 10, 801. [Google Scholar] [CrossRef]
- Etminan, M.; Gill, S.S.; Samii, A. Intake of vitamin E, vitamin C, and carotenoids and the risk of Parkinson’s disease: A meta-analysis. Lancet Neurol. 2005, 4, 362–365. [Google Scholar] [CrossRef]
- Qin, S.; Wang, M.; Zhang, T.; Zhang, S. Vitamin E intake is not associated with glioma risk: Evidence from a meta-analysis. Neuroepidemiology 2015, 43, 253–258. [Google Scholar] [CrossRef]
- Peng, L.; Liu, X.; Lu, Q.; Tang, T.; Yang, Z. Vitamin E intake and pancreatic cancer risk: A meta-analysis of observational studies. Med. Sci. Monit. 2015, 21, 1249–1255. [Google Scholar]
- Dong, Y.; Liu, Y.; Shu, Y.; Chen, X.; Hu, J.; Zheng, R.; Ma, D.; Yang, C.; Guan, X. Link between risk of colorectal cancer and serum vitamin E levels: A meta-analysis of case-control studies. Medicine 2017, 96, e7470. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Li, Y.; Chen, X.; Sun, H.; Hou, X.; Shi, J. Circulating tocopherols and risk of coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2016, 23, 748–757. [Google Scholar] [CrossRef]
- Cui, R.; Liu, Z.Q.; Xu, Q. Blood α-tocopherol, γ-tocopherol levels and risk of prostate cancer: A meta-analysis of prospective studies. PLoS ONE 2014, 9, e93044. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 64, 328–357. [Google Scholar] [CrossRef]
- Jiang, Q. Natural forms of vitamin E as effective agents for cancer prevention and therapy. Adv. Nutr. 2017, 8, 850–864. [Google Scholar] [CrossRef]
- Moyer, V.A.; US Preventive Services Task Force. Vitamin, mineral, and multivitamin supplements for the primary prevention of cardiovascular disease and cancer: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2014, 160, 558–564. [Google Scholar] [CrossRef]
- Tanner, M. USPSTF recommends against beta carotene or vitamin E supplements for preventing CVD or cancer in adults. Ann. Intern. Med. 2022, 175, Jc110. [Google Scholar] [CrossRef]
- Jiang, Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and their role in disease pre-vention and therapy. Free. Radic. Biol. Med. 2014, 72, 76–90. [Google Scholar] [CrossRef]
- Jiang, Q.; Yin, X.; Lill, M.A.; Danielson, M.L.; Freiser, H.; Huang, J. Long-chain carboxychromanols, metabolites of vitamin E, are potent inhibitors of cyclooxy-genases. Proc. Natl. Acad. Sci. USA 2008, 105, 20464–20469. [Google Scholar] [CrossRef]
- Jang, Y.; Park, N.Y.; Rostgaard-Hansen, A.L.; Huang, J.; Jiang, Q. Vitamin E metabolite 13′-carboxychromanols inhibit pro-inflammatory enzymes, induce apoptosis and autophagy in human cancer cells by modulating sphingolipids and suppress colon tumor development in mice. Free. Radic. Biol. Med. 2016, 95, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Kayden, H.J.; Traber, M.G. Absorption, lipoprotein transport, and regulation of plasma concentrations of vitamin E in humans. J. Lipid Res. 1993, 34, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Stonehouse, W.; Brinkworth, G.D.; Thompson, C.H.; Abeywardena, M.Y. Short term effects of palm-tocotrienol and palm-carotenes on vascular function and cardiovascular disease risk: A randomised controlled trial. Atherosclerosis 2016, 254, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Sozen, E.; Demirel, T.; Ozer, N.K. Vitamin E: Regulatory role in the cardiovascular system. Iubmb Life 2019, 71, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.L.; Jeong, G.H.; Yang, J.W.; Lee, K.H.; Kronbichler, A.; Van Der Vliet, H.J.; Grosso, G.; Galvano, F.; Aune, D.; Kim, J.Y.; et al. Tea consumption and risk of cancer: An umbrella review and meta-analysis of observa-tional studies. Adv. Nutr. 2020, 11, 1437–1452. [Google Scholar] [CrossRef]
- Perumpail, B.J.; Li, A.A.; John, N.; Sallam, S.; Shah, N.D.; Kwong, W.; Cholankeril, G.; Kim, D.; Ahmed, A. The Role of Vitamin E in the Treatment of NAFLD. Diseases 2018, 6, 86. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. JAMA 2007, 297, 842–857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Outcome | Author | Year | Effect Metrics | Number of Included Studies | Type of Included Studies | Egger p Value | Random-Effects Size (95% CI) | p Value | I2(%) | Q Test p Value | Tau2 | 95% Prediction Interval | GRADE | AMSTAR2 | Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Supplemental vitamin E | |||||||||||||||
| Adult patients with non-alcoholic fatty liver disease (NAFLD): alanine aminotransferase | Vadarlis | 2021 | MD | 7 | RCT | NA | −7.37 [−10.11,−4.64] | 1.29495 × 10−7 | 0.00 | 0.4493543 | 0 | −10.96 to −3.78 | Very low | Moderate | Class IV |
| Adult patients with non-alcoholic fatty liver disease (NAFLD): aspartate aminotransferase | Vadarlis | 2021 | MD | 7 | RCT | NA | −5.71 [−9.50,−1.93] | 0.0031 | 67.99 | 0.004613523 | 14.29 | −16.62 to 5.20 | Very low | Moderate | Class IV |
| Age-related cataract | Zhang | 2015 | RR | 10 | Cohort, Case–control | NA | 0.93 [0.79,1.08] | 0.34 | 73.27 | 0.000101994 | 0.033 | 0.59 to 1.47 | Very low | Low | Class V |
| Alzheimer’s disease (AD) | Wang | 2021 | RR | 5 | Cohort | 0.66 | 0.81 [0.50,1.31] | 0.39 | 68.06 | 0.01386352 | 0.18 | 0.17 to 3.84 | Very low | Low | Class V |
| ApoA | Hamedi | 2021 | WMD | 4 | RCT | 0.73 | −0.62 [−1.94,0.71] | 0.36 | 93.53 | 4.75651 × 10−10 | 1.68 | −6.90 to 5.66 | Very low | Low | Class V |
| ApoB | Hamedi | 2021 | WMD | 7 | RCT | 0.55 | 0.22 [−0.38,0.81] | 0.48 | 84.83 | 5.58564 × 10−7 | 0.51 | −1.78 to 2.21 | Very low | Low | Class V |
| Asthmatic diseases in children | Wu | 2018 | OR | 10 | Cohort | 0.13 | 0.74 [0.61,0.89] | 0.0013 | 73.28 | 0.000101632 | 0.042 | 0.44 to 1.24 | Very low | Critially Low | Class IV |
| Bladder cancer | Chen | 2015 | RR | 7 | Cohort, Case–control | 0.39 | 0.78 [0.64,0.94] | 0.01 | 0.00 | 0.4242131 | 0 | 0.60 to 1.00 | Moderate | Critially Low | Class IV |
| BMI | Emami | 2021 | WMD | 27 | RCT | 0.38 | 0.04 [−0.29,0.37] | 0.82 | 0.00 | 0.9994954 | 0 | −0.30 to 0.38 | Low | Low | Class V |
| Cardiovascular mortality | Jayedi | 2019 | RR | 7 | Cohort | NA | 0.99 [0.96,1.02] | 0.54 | 0.00 | 0.6680903 | 0 | 0.95 to 1.03 | Very low | Critially Low | Class V |
| Chemotherapy-induced peripheral neuropathy (CIPN) | Chen | 2021 | RR | 8 | RCT | NA | 0.55 [0.36,0.85] | 0.0069 | 77.14 | 7.29272 × 10−5 | 0.23 | 0.15 to 2.01 | Very low | Critially Low | Class IV |
| Contrast-induced acute kidney injury | Cho | 2017 | RR | 3 | RCT | NA | 0.38 [0.23,0.64] | 0.0003 | 0.00 | 0.6189431 | 0 | 0.01 to 11.37 | Very low | Critially Low | Class IV |
| Diastolic blood pressure | Emami | 2019 | WMD | 17 | RCT | NA | −1.19 [−2.67,0.29] | 0.11 | 89.79 | 3.59574 × 10−25 | 5.95 | −6.64 to 4.25 | Very low | Critially Low | Class V |
| Duration of mastalgia | Hajizadeh | 2019 | SMD | 3 | RCT | NA | 0.36 [−1.35,0.63] | 0.47 | 0.00 | 0.8534552 | 0 | −6.78 to 6.06 | Very low | Low | Class V |
| Endothelial function | Siervo | 2015 | SMD | 27 | RCT | 0.61 | 0.48 [0.23,0.72] | 0.00012 | 64.48 | 2.23892 × 10−6 | 0.26 | −0.60 to 1.55 | Very low | Critially Low | Class III |
| Fasting glucose | Xu | 2014 | WMD | 12 | RCT | 0.87 | 0.13 [−0.33,0.59] | 0.57 | 88.05 | 6.56948 × 10−15 | 0.36 | −1.31 to 1.57 | Very low | Critially Low | Class V |
| Fasting insulin | Xu | 2014 | WMD | 6 | RCT | 0.27 | −4.54 [−13.16,4.08] | 0.3 | 88.55 | 2.71116 × 10−8 | 59.27 | −29.15 to 20.08 | Very low | Critially Low | Class V |
| Fatal myocardial infarction | Loffredo | 2015 | RR | 6 | RCT | 0.09 | 0.84 [0.73,0.97] | 0.015 | 0.00 | 0.5299839 | 0 | 0.69 to 1.02 | Low | Critially Low | Class IV |
| HbA1c | Xu | 2014 | WMD | 12 | RCT | 0.46 | −0.24 [−0.49,0.02] | 0.066 | 66.89 | 0.000484398 | 0.11 | −1.02 to 0.55 | Very low | Critially Low | Class V |
| High-density lipoprotein cholesterol (HDL-C) levels in patients with diabetes mellitus | Mohammad | 2021 | WMD | 11 | RCT | NA | 0.68 [−1.25,2.60] | 0.49 | 85.37 | 9.19549 × 10−11 | 7.14 | −5.76 to 7.12 | Very low | Critially Low | Class V |
| Lipid peroxidation(malondialdehyde) | Stepanyan | 2014 | SMD | 10 | RCT | NA | 0.06 [−0.47,0.59] | 0.83 | 56.75 | 0.01351643 | 0.41 | −1.55 to 1.66 | Very low | Critially Low | Class V |
| Low-density lipoprotein cholesterol (LDL- C) levels in patients with diabetes mellitus | Mohammad | 2021 | WMD | 11 | RCT | NA | −0.52 [−8.30,7.25] | 0.89 | 89.00 | 3.60121 × 10−15 | 139.75 | −28.73 to 27.68 | Very low | Critially Low | Class V |
| Mean arterial pressure | Emami | 2019 | WMD | 7 | RCT | NA | −1.45 [−5.23,2.33] | 0.45 | 79.02 | 7.2278 × 10−5 | 13.32 | −12.07 to 9.16 | Very low | Critially Low | Class V |
| Muscle damage(creatine kinase) | Stepanyan | 2014 | SMD | 8 | RCT | NA | −0.47 [−2.25,1.31] | 0.61 | 91.31 | 1.08004 × 10−14 | 5.87 | −6.80 to 5.87 | Very low | Critially Low | Class V |
| Myocardial infarction | Loffredo | 2015 | RR | 8 | RCT | 0.09 | 0.83 [0.71,0.96] | 0.014 | 58.67 | 0.01782035 | 0.022 | 0.55 to 1.25 | Very low | Critially Low | Class IV |
| Non fatal myocardial infarction | Loffredo | 2015 | RR | 7 | RCT | 0.15 | 0.94 [0.74,1.18] | 0.57 | 63.97 | 0.01064533 | 0.047 | 0.50 to 1.77 | Very low | Critially Low | Class V |
| Ovarian cancer | Leng | 2019 | RR | 5 | Cohort, Case–control | NA | 0.82 [0.54,1.25] | 0.35 | 82.33 | 0.000149404 | 0.19 | 0.18 to 3.78 | Very low | Critially Low | Class V |
| Patients Receiving Hemodialysis: Biomarkers of Endothelial Dysfunction-ICAM-1 | Nguyen | 2021 | SMD | 4 | RCT | 0.37 | −1.35 [−2.57,−0.13] | 0.03 | 89.01 | 5.12701 × 10−6 | 1.28 | −6.91 to 4.21 | Very low | Moderate | Class IV |
| Patients Receiving Hemodialysis: Biomarkers of Endothelial Dysfunction-VCAM-1 | Nguyen | 2021 | SMD | 3 | RCT | 0.83 | −1.08 [−2.05,−0.11] | 0.029 | 80.38 | 0.006122837 | 0.58 | −12.60 to 10.44 | Very low | Moderate | Class IV |
| Patients Receiving Hemodialysis: Biomarkers of inflammation-CRP | Nguyen | 2021 | SMD | 9 | RCT | 0.58 | −0.41 [−0.75,−0.07] | 0.017 | 63.71 | 0.0048335 | 0.16 | −1.45 to 0.63 | Very low | Moderate | Class IV |
| Patients Receiving Hemodialysis: Biomarkers of inflammation-IL-6 | Nguyen | 2021 | SMD | 5 | RCT | 0.23 | −0.16 [−0.52,0.21] | 0.4 | 52.96 | 0.07476872 | 0.089 | −1.27 to 0.96 | Very low | Moderate | Class V |
| Patients Receiving Hemodialysis: Biomarkers of Oxidative Stress-malondialdehyde (MDA) | Nguyen | 2021 | SMD | 6 | RCT | 0.059 | −0.76 [−1.26,−0.25] | 0.0032 | 76.58 | 0.000694967 | 0.3 | −2.43 to 0.92 | Very low | Moderate | Class IV |
| Serum ALT in Pediatric Nonalcoholic Fatty Liver Disease patients | Sarkhy | 2014 | RR | 4 | RCT | NA | 1.17 [0.91,1.49] | 0.22 | 0.00 | 0.7688677 | 0 | 0.68 to 1.99 | Very low | Low | Class V |
| Serum CRP concentrations | Asbaghi | 2020 | WMD | 36 | RCT | NA | −0.51 [−0.80,−0.23] | 0.00042 | 59.82 | 2.48248 × 10−6 | 0.23 | −1.53 to 0.50 | Very low | Low | Class III |
| Serum IL-6 concentrations | Asbaghi | 2020 | WMD | 21 | RCT | NA | −0.16 [−0.54,0.23] | 0.42 | 74.35 | 8.60757 × 10−9 | 0.4 | −1.54 to 1.23 | Very low | Low | Class V |
| Serum TNF-α concentrations | Asbaghi | 2020 | WMD | 19 | RCT | NA | 0.01 [−0.16,0.18] | 0.93 | 78.90 | 9.87231 × 10−11 | 0.062 | −0.55 to 0.56 | low | Low | Class V |
| Severity of mastalgia | Hajizadeh | 2019 | SMD | 7 | RCT | NA | 0.40 [0.01,0.78] | 0.042 | 79.06 | 7.06353 × 10−5 | 0.2 | −0.86 to 1.66 | Very low | Low | Class IV |
| Stroke | Loh | 2020 | RR | 12 | RCT | 0.25 | 0.98 [0.93,1.04] | 0.59 | 0.00 | 0.4715554 | 0 | 0.92 to 1.05 | Low | Moderate | Class V |
| Systolic blood pressure | Emami | 2019 | WMD | 23 | RCT | NA | −3.44 [−6.77,−0.11] | 0.043 | 94.00 | 2.93369 × 10−64 | 55.23 | −19.29 to 12.42 | Very low | Critially Low | Class IV |
| Total cholesterol (TC) levels in patients with diabetes mellitus | Mohammad | 2021 | WMD | 12 | RCT | NA | −0.69 [−15.03,13.65] | 0.92 | 96.32 | 1.31883 × 10−57 | 597.03 | −57.52 to 56.14 | Very low | Critially Low | Class V |
| Triglyceride (TG) levels in patients with diabetes mellitus | Mohammad | 2021 | WMD | 12 | RCT | NA | 1.33 [−9.19,11.85] | 0.8 | 76.73 | 1.92346 × 10−6 | 186.61 | −31.37 to 34.03 | Very low | Critially Low | Class V |
| Waist circumference (WC) | Emami | 2021 | WMD | 7 | RCT | 0.072 | −0.19 [−2.06,1.68] | 0.84 | 0.00 | 0.9777026 | 0 | −2.64 to 2.26 | Very low | Low | Class V |
| Weight | Emami | 2021 | WMD | 16 | RCT | 0.63 | 0.15 [−1.35,1.65] | 0.845 | 0.00 | 0.9998251 | 0 | −1.49 to 1.79 | Very low | Low | Class V |
| Dietary vitamin E | |||||||||||||||
| Age-related cataract | Zhang | 2015 | RR | 8 | Cohort, Case–control, Cross-sectional | NA | 0.73 [0.58,0.92] | 0.0073 | 69.13 | 0.001942455 | 0.066 | 0.37 to 1.46 | Very low | Low | Class IV |
| Bladder cancer | Chen | 2015 | RR | 9 | Cohort, Case–control | 0.01 | 0.80 [0.68,0.94] | 0.0077 | 32.97 | 0.1541656 | 0.02 | 0.54 to 1.18 | Low | Critially Low | Class IV |
| Cervical cancer | Hu | 2017 | OR | 9 | Case–control | NA | 0.53 [0.39,0.73] | 7.32494 × 10−5 | 77.64 | 1.92167 × 10−5 | 0.17 | 0.19 to 1.50 | Very low | Critially Low | Class III |
| CIN, cervical intraepithelial neoplasia | Hu | 2017 | OR | 17 | Case–control | NA | 0.55 [0.43,0.70] | 1.2434 × 10−6 | 78.10 | 2.88363 × 10−9 | 0.2 | 0.21 to 1.46 | Very low | Critially Low | Class III |
| Esophageal Cancer | Cui | 2018 | OR | 14 | Cohort, Case–control | 0.008 | 0.47 [0.36, 0.60] | 3.77685 × 10−9 | 66.95 | 0.000177109 | 0.13 | 0.20 to 1.09 | Very low | Critially Low | Class III |
| Lung cancer | Zhu | 2017 | RR | 11 | Cohort | 0.25 | 0.85 [0.74, 0.98] | 0.03 | 41.83 | 0.07023408 | 0.023 | 0.58 to 1.25 | Very low | Critially Low | Class IV |
| Kidney Cancer | Shen | 2015 | RR | 13 | Cohort, Case–control | 0.93 | 0.81 [0.69,0.94] | 0.0065 | 49.22 | 0.02282328 | 0.035 | 0.52 to 1.26 | Very low | Critially Low | Class IV |
| Ovarian cancer | Leng | 2019 | RR | 8 | Cohort, Case–control | NA | 0.99 [0.77,1.27] | 0.95 | 52.76 | 0.0383885 | 0.066 | 0.49 to 2.00 | Very low | Critially Low | Class V |
| Parkinson’s disease | Etminan | 2005 | RR | 7 | Cohort, Case–control, Cross-sectional | NA | 0.81 [0.67,0.98] | 0.028 | 0.00 | 0.6156204 | 0 | 0.63 to 1.04 | Very low | Critially Low | Class IV |
| Total vitamin E | |||||||||||||||
| Age-related cataract | Zhang | 2015 | RR | 4 | Cohort, Case–control | NA | 0.84 [0.62,1.15] | 0.29 | 47.08 | 0.1288757 | 0.047 | 0.26 to 2.69 | Very low | Low | Class V |
| Glioma | Qin | 2014 | RR | 12 | Cohort, Case–control | 0.51 | 0.88 [0.69,1.12] | 0.31 | 64.87 | 0.000983177 | 0.11 | 0.40 to 1.94 | Very low | Critially Low | Class V |
| Pancreatic Cancer | Peng | 2015 | RR | 12 | Cohort, Case–control | 0.049 | 0.76 [0.67,0.87] | 0.000053 | 19.80 | 0.2548871 | 0.0091 | 0.59 to 0.99 | Very low | Critially Low | Class III |
| Ovarian cancer | Leng | 2019 | RR | 11 | Cohort, Case–control | NA | 0.95 [0.78,1.16] | 0.64 | 53.19 | 0.01869907 | 0.057 | 0.53 to 1.72 | Very low | Critially Low | Class V |
| Bladder cancer | Chen | 2015 | RR | 6 | Cohort, Case–control | 0.35 | 0.82 [0.62,1.08] | 0.15 | 55.17 | 0.04842951 | 0.063 | 0.37 to 1.82 | Very low | Critially Low | Class V |
| Circulating α-tocopherol levels | |||||||||||||||
| Age-related cataract | Zhang | 2015 | RR | 17 | Cohort, Case–control, Cross-sectional | NA | 0.77 [0.66,0.91] | 0.0019 | 52.09 | 0.006544955 | 0.043 | 0.48 to 1.24 | Very low | Low | Class IV |
| Asthma or wheeze in children | Wu | 2018 | OR | 7 | Cohort | 0.035 | 0.65 [0.56,0.75] | 1.37859 × 10−8 | 0.00 | 0.4474548 | 0 | 0.53 to 0.79 | Very low | Critially Low | Class I |
| Bladder cancer | Chen | 2015 | RR | 4 | Cohort, Case–control | 0.39 | 0.59 [0.41,0.85] | 0.0046 | 0.00 | 0.607105 | 0 | 0.26 to 1.32 | Low | Critially Low | Class IV |
| Cardiovascular mortality | Jayedi | 2019 | RR | 4 | Cohort | NA | 0.93 [0.89,0.98] | 0.0043 | 9.15 | 0.3473236 | 0.00055 | 0.81 to 1.08 | Very low | Critially Low | Class IV |
| Colorectal cancer | Dong | 2017 | WMD | 11 | Case–control | NA | −2.99 [−4.40,−1.59] | 2.94537 × 10−5 | 94.98 | 2.50467 × 10−37 | 3.01 | −7.24 to 1.25 | Very low | Critially Low | Class III |
| CVD | Li | 2016 | WMD | 12 | Cohort, Case–control | 0.54 | 0.60 [−0.77,1.97] | 0.39 | 64.44 | 0.001129312 | 3.36 | −3.77 to 4.97 | Very low | Critially Low | Class V |
| Prostate cancer | Cui | 2014 | RR | 9 | Case–control | 0.08 | 0.79 [0.68,0.91] | 0.0015 | 12.45 | 0.3308022 | 0.0062 | 0.61 to 1.02 | Very low | Critially Low | Class IV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, Z.; Liu, L.; Jian, Z.; Ma, Y.; Li, H.; Jin, X.; Liao, B.; Wang, K. Vitamin E and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses. Nutrients 2023, 15, 3301. https://doi.org/10.3390/nu15153301
Xiong Z, Liu L, Jian Z, Ma Y, Li H, Jin X, Liao B, Wang K. Vitamin E and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses. Nutrients. 2023; 15(15):3301. https://doi.org/10.3390/nu15153301
Chicago/Turabian StyleXiong, Zheyu, Linhu Liu, Zhongyu Jian, Yucheng Ma, Hong Li, Xi Jin, Banghua Liao, and Kunjie Wang. 2023. "Vitamin E and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses" Nutrients 15, no. 15: 3301. https://doi.org/10.3390/nu15153301
APA StyleXiong, Z., Liu, L., Jian, Z., Ma, Y., Li, H., Jin, X., Liao, B., & Wang, K. (2023). Vitamin E and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses. Nutrients, 15(15), 3301. https://doi.org/10.3390/nu15153301