


Impact of Chronotype and Mediterranean Diet on the Risk of Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease
 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
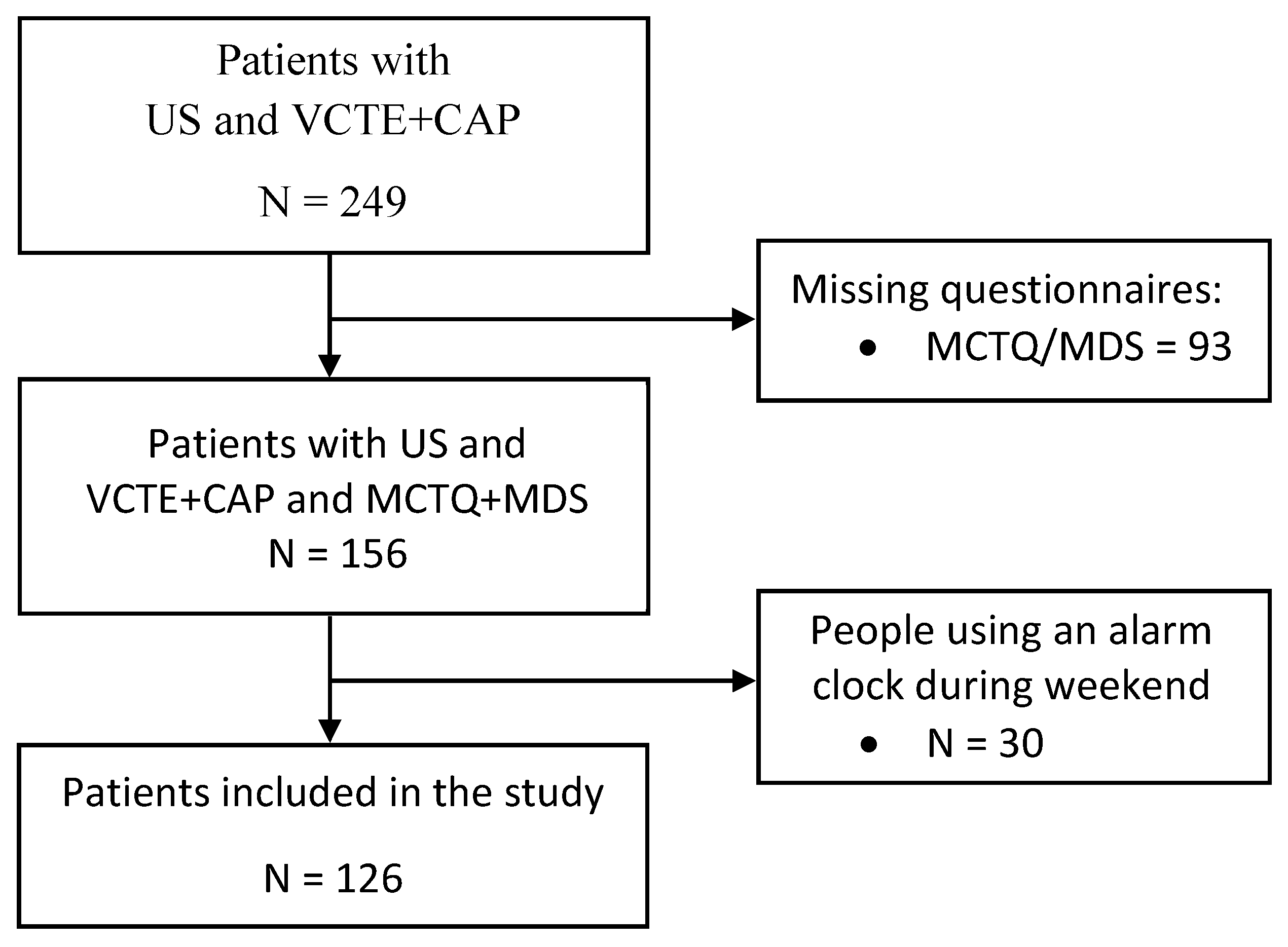
2.1. Study Design and Participants
2.2. Anthropometric, Biochemical and Comorbidity Assessment
2.3. Evaluation of Liver Status
2.4. Chronotype Assessment
2.5. Mediterranean Diet Assessment
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology 2023, 77, 1335. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Brown, G.T.; Kleiner, D.E. Histopathology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Metabolism. 2016, 65, 1080–1086. [Google Scholar] [CrossRef]
- Anstee, Q.M.; Reeves, H.L.; Kotsiliti, E.; Govaere, O.; Heikenwalder, M. From NASH to HCC: Current concepts and future challenges. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 411–428. [Google Scholar] [CrossRef]
- Miller, E.F. Nutrition Management Strategies for Nonalcoholic Fatty Liver Disease: Treatment and Prevention. Clin. Liver Dis. 2020, 15, 144–148. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL) EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016, 59, 1121–1140. [CrossRef]
- Juanola, O.; Martínez-López, S.; Francés, R.; Gómez-Hurtado, I. Non-Alcoholic Fatty Liver Disease: Metabolic, Genetic, Epigenetic and Environmental Risk Factors. Int. J. Environ. Res. Public Health 2021, 18, 5227. [Google Scholar] [CrossRef]
- Schattenberg, J.M.; Allen, A.M.; Jarvis, H.; Zelber-Sagi, S.; Cusi, K.; Dillon, J.F.; Caussy, C.; Francque, S.M.; Younossi, Z.; Alkhouri, N.; et al. A multistakeholder approach to innovations in NAFLD care. Commun. Med. 2023, 3, 1. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Georgoulis, M.; Papatheodoridis, G.V.; Panagiotakos, D.B.; Kontogianni, M.D. Effects of lifestyle interventions on clinical characteristics of patients with non-alcoholic fatty liver disease: A meta-analysis. Metabolism. 2017, 68, 119–132. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Grinshpan, L.S.; Ivancovsky-Wajcman, D.; Goldenshluger, A.; Gepner, Y. One size does not fit all; practical, personal tailoring of the diet to NAFLD patients. Liver Int. 2022, 42, 1731–1750. [Google Scholar] [CrossRef]
- Akram, S.T.; Ewy, M.W.; Said, A. Sleep disruption in nonalcoholic fatty liver disease: What is the role of lifestyle and diet? Eur. J. Gastroenterol. Hepatol. 2021, 33, e308–e312. [Google Scholar] [CrossRef]
- Han, H.; Dou, J.; Hou, Q.; Wang, H. Role of Circadian Rhythm and Impact of Circadian Rhythm Disturbance on the Metabolism and Disease. J. Cardiovasc. Pharmacol. 2022, 79, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef]
- Adamovich, Y.; Rousso-Noori, L.; Zwighaft, Z.; Neufeld-Cohen, A.; Golik, M.; Kraut-Cohen, J.; Wang, M.; Han, X.; Asher, G. Circadian clocks and feeding time regulate the oscillations and levels of hepatic triglycerides. Cell Metab. 2014, 19, 319. [Google Scholar] [CrossRef]
- Shimba, S.; Ogawa, T.; Hitosugi, S.; Ichihashi, Y.; Nakadaira, Y.; Kobayashi, M.; Tezuka, M.; Kosuge, Y.; Ishige, K.; Ito, Y.; et al. Deficient of a Clock Gene, Brain and Muscle Arnt-Like Protein-1 (BMAL1), Induces Dyslipidemia and Ectopic Fat Formation. PLoS ONE 2011, 6, e25231. [Google Scholar] [CrossRef] [PubMed]
- Vetrani, C.; Barrea, L.; Verde, L.; Sarno, G.; Docimo, A.; de Alteriis, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Evening chronotype is associated with severe NAFLD in obesity. Int. J. Obes. (Lond.) 2022, 46, 1638–1643. [Google Scholar] [CrossRef]
- Weng, Z.; Ou, W.; Huang, J.; Singh, M.; Wang, M.; Zhu, Y.; Kumar, R.; Lin, S. Circadian Misalignment Rather Than Sleep Duration is Associated with MAFLD: A Population-Based Propensity Score-Matched Study. Nat. Sci. Sleep 2021, 13, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Perez-Diaz-del-Campo, N.; Castelnuovo, G.; Caviglia, G.P.; Armandi, A.; Rosso, C.; Bugianesi, E. Role of Circadian Clock on the Pathogenesis and Lifestyle Management in Non-Alcoholic Fatty Liver Disease. Nutrients 2022, 14, 5053. [Google Scholar] [CrossRef]
- Ruiz-Lozano, T.; Vidal, J.; De Hollanda, A.; Canteras, M.; Garaulet, M.; Izquierdo-Pulido, M. Evening chronotype associates with obesity in severely obese subjects: Interaction with CLOCK 3111T/C. Int. J. Obes. 2016, 40, 1550–1557. [Google Scholar] [CrossRef] [PubMed]
- Lotti, S.; Pagliai, G.; Colombini, B.; Sofi, F.; Dinu, M. Chronotype Differences in Energy Intake, Cardiometabolic Risk Parameters, Cancer, and Depression: A Systematic Review with Meta-Analysis of Observational Studies. Adv. Nutr. 2022, 13, 269–281. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Aprano, S.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Pugliese, G.; Savastano, S.; Colao, A. Chronotype and Adherence to the Mediterranean Diet in Obesity: Results from the Opera Prevention Project. Nutrients 2020, 12, 1354. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Hasan, H.; Khadem, S.H.; Buanq, M.A.; Al-Mulla, H.K.; Aljassmi, A.K.; Faris, M.A.I.E. Adherence to the Mediterranean Diet and Its Association With Sleep Quality and Chronotype Among Youth: A Cross-Sectional Study. Front. Nutr. 2022, 8, 805955. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, R.S.; Dasarathy, S.; McCullough, A.J.; Shuhart, M.C.; Davis, G.L.; Franco, J.; Harrison, S.A.; Howell, C.D.; Ling, S.C.; Liu, L.U.; et al. Alcoholic liver disease. Hepatology 2010, 51, 307–328. [Google Scholar] [CrossRef]
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension global hypertension practice guidelines. J. Hypertens. 2020, 38, 982–1004. [Google Scholar] [CrossRef]
- Pappan, N.; Rehman, A. Dyslipidemia. Chronic Dis. Follow. Adults Prim. Care 2022, 21, 243–256. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskina, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef]
- Wong, V.W.S.; Vergniol, J.; Wong, G.L.H.; Foucher, J.; Chan, H.L.Y.; Le Bail, B.; Choi, P.C.L.; Kowo, M.; Chan, A.W.H.; Merrouche, W.; et al. Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology 2010, 51, 454–462. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef]
- Reiter, A.M.; Sargent, C.; Roach, G.D. Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire. Clocks Sleep 2021, 3, 342. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, C.; Randler, C. Circadian preferences and personality values: Morning types prefer social values, evening types prefer individual values. Pers. Individ. Dif. 2012, 52, 738–743. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Roenneberg, T.; Keller, L.K.; Fischer, D.; Matera, J.L.; Vetter, C.; Winnebeck, E.C. Human activity and rest in situ. In Methods in Enzymology; CRC Press: Boca Raton, FL, USA, 2015; Volume 552. [Google Scholar]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Castera, L.; Yuen Chan, H.L.; Arrese, M.; Afdhal, N.; Bedossa, P.; Friedrich-Rust, M.; Han, K.H.; Pinzani, M. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef]
- Targher, G.; Corey, K.E.; Byrne, C.D.; Roden, M. The complex link between NAFLD and type 2 diabetes mellitus—Mechanisms and treatments. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 599–612. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Bonora, E.; Targher, G. Nonalcoholic Fatty Liver Disease and Risk of Incident Type 2 Diabetes: A Meta-analysis. Diabetes Care 2018, 41, 372–382. [Google Scholar] [CrossRef]
- Armandi, A.; Rosso, C.; Caviglia, G.P.; Bugianesi, E. Insulin Resistance across the Spectrum of Nonalcoholic Fatty Liver Disease. Metabolites 2021, 11, 155. [Google Scholar] [CrossRef]
- Merikanto, I.; Lahti, T.; Puolijoki, H.; Vanhala, M.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Kronholm, E.; Partonen, T. Associations of chronotype and sleep with cardiovascular diseases and type 2 diabetes. Chronobiol. Int. 2013, 30, 470–477. [Google Scholar] [CrossRef]
- Larcher, S.; Benhamou, P.Y.; Pépin, J.L.; Borel, A.L. Sleep habits and diabetes. Diabetes Metab. 2015, 41, 263–271. [Google Scholar] [CrossRef]
- Schipper, S.B.J.; Van Veen, M.M.; Elders, P.J.M.; van Straten, A.; Van Der Werf, Y.D.; Knutson, K.L.; Rutters, F. Sleep disorders in people with type 2 diabetes and associated health outcomes: A review of the literature. Diabetologia 2021, 64. [Google Scholar] [CrossRef]
- Mir, H.M.; Stepanova, M.; Afendy, H.; Cable, R.; Younossi, Z.M. Association of Sleep Disorders with Nonalcoholic Fatty Liver Disease (NAFLD): A Population-based Study. J. Clin. Exp. Hepatol. 2013, 3, 181–185. [Google Scholar] [CrossRef]
- Becker, N.B.; Jesus, S.N.; João, K.A.D.R.; Viseu, J.N.; Martins, R.I.S. Depression and sleep quality in older adults: A meta-analysis. Psychol. Health Med. 2017, 22, 889–895. [Google Scholar] [CrossRef]
- Chang, H.P.; Chen, Y.F.; Du, J.K. Obstructive sleep apnea treatment in adults. Kaohsiung J. Med. Sci. 2020, 36, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Lo, K.; Woo, B.; Wong, M.; Tam, W. Subjective sleep quality, blood pressure, and hypertension: A meta-analysis. J. Clin. Hypertens. (Greenwich) 2018, 20, 592–605. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.H.; Yun, C.H.; Ahn, J.H.; Suh, S.; Cho, H.J.; Lee, S.K.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; Choi, K.M.; et al. Evening chronotype is associated with metabolic disorders and body composition in middle-aged adults. J. Clin. Endocrinol. Metab. 2015, 100, 1494–1502. [Google Scholar] [CrossRef]
- McMahon, D.M.; Burch, J.B.; Youngstedt, S.D.; Wirth, M.D.; Hardin, J.W.; Hurley, T.G.; Blair, S.N.; Hand, G.A.; Shook, R.P.; Drenowatz, C.; et al. Relationships between chronotype, social jetlag, sleep, obesity and blood pressure in healthy young adults. Chronobiol. Int. 2019, 36, 493–509. [Google Scholar] [CrossRef]
- Rosi, A.; Lotti, S.; Vitale, M.; Pagliai, G.; Madarena, M.P.; Bonaccio, M.; Esposito, S.; Ferraris, C.; Guglielmetti, M.; Angelino, D.; et al. Association between chronotype, sleep pattern, and eating behaviours in a group of Italian adults. Int. J. Food Sci. Nutr. 2022, 73, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Corey, K.E.; Lim, J.K. AGA Clinical Practice Update on Lifestyle Modification Using Diet and Exercise to Achieve Weight Loss in the Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology 2021, 160, 912–918. [Google Scholar] [CrossRef]
- Castera, L. Non-invasive tests for liver fibrosis in NAFLD: Creating pathways between primary healthcare and liver clinics. Liver Int. 2020, 40 (Suppl. S1), 77–81. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Darlay, R.; Cockell, S.; Meroni, M.; Govaere, O.; Tiniakos, D.; Burt, A.D.; Bedossa, P.; Palmer, J.; Liu, Y.L.; et al. Genome-wide association study of non-alcoholic fatty liver and steatohepatitis in a histologically characterised cohort☆. J. Hepatol. 2020, 73, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Valenti, L.; Romeo, S. Genetics and epigenetics of NAFLD and NASH: Clinical impact. J. Hepatol. 2018, 68, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Levandovski, R.; Sasso, E.; Hidalgo, M.P. Chronotype: A review of the advances, limits and applicability of the main instruments used in the literature to assess human phenotype. Trends Psychiatry Psychother. 2013, 35, 3–11. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n | 126 |
|---|---|
| Sex (Male/Female) | 73/53 |
| Age (years) | 55 (46; 63) |
| Anthropometric characteristics | |
| Body Mass Index (kg/m2) | 29.4 (26.2; 32.5) |
| Diabetes n (%) | 33 (26.19%) |
| Arterial hypertension n (%) | 67 (53.17%) |
| Dyslipidaemia n (%) | 80 (63.49%) |
| Depression n (%) | 7 (5.56%) |
| Obstructive sleep apnoea n (%) | 7 (5.56%) |
| Liver and biomarkers assessment | |
| Liver stiffness (kPa) | 5.1 (4.4; 6) |
| Liver stiffness n (%) | |
| ≤7 kPa (F0–F1) | 107 (84.92%) |
| 7.1–8.7 kPa (F2) | 6 (4.76%) |
| 8.8–10.3 Kpa (F3) | 5 (3.97%) |
| ≥10.4 (F4) | 8 (6.35%) |
| CAP (dB/m) | 302 (263; 338) |
| FIB-4 | 0.98 (0.74; 1.26) |
| AST (IU/L) | 28 (24; 38) |
| ALT (IU/L) | 39 (27; 56) |
| GGT (IU/L) | 40 (26; 75) |
| Glucose (mg/dL) | 98 (87; 112) |
| Triglycerides (mg/dL) | 128.5 (100; 171) |
| Cholesterol (mg/dL) | 200 (177; 228) |
| MSF (min) | 240 (210; 285) |
| MSW (min) | 201.5 (170; 235) |
| SDf (min) | 450 (410; 490) |
| SDw (min) | 405 (360; 450) |
| SDweek (min) | 420 (372; 456) |
| Chronotype (min) | 221 (195; 267) |
| Mediterranean diet score | 7 (5; 8) |
| Early | Intermediate + Late | p-Value | |
|---|---|---|---|
| n | 44 | 82 | |
| Sex n (%) | |||
| Male | 23 (52.27%) | 50 (60.98%) | 0.345 |
| Female | 21 (47.73%) | 32 (39.02%) | |
| Age (y) | 57 (49; 62) | 51.5 (42; 63) | 0.301 |
| Diabetes n (%) | |||
| No | 35 (79.55%) | 58 (70.73%) | 0.283 |
| Yes | 9 (20.45%) | 24 (29.27%) | |
| Hypertension n (%) | |||
| No | 17 (38.64%) | 42 (51.22%) | 0.177 |
| Yes | 27 (61.36%) | 40 (48.78%) | |
| Dyslipidaemia n (%) | |||
| No | 14 (31.82%) | 32 (39.02%) | 0.423 |
| Yes | 30 (68.18%) | 50 (60.98%) | |
| Depression n (%) | |||
| No | 43 (97.73%) | 76 (92.68%) | 0.239 |
| Yes | 1 (2.27%) | 6 (7.32%) | |
| Obstructive sleep apnoea n (%) | |||
| No | 41 (93.18%) | 78 (95.12%) | 0.650 |
| Yes | 3 (6.82%) | 4 (4.88%) | |
| Body Mass Index (kg/m2) | 29.05 (26.8; 32.4) | 29.4 (25.7; 32.8) | 0.619 |
| Stiffness n (%) | |||
| ≤7 kPa (F0–F1) | 41 (93.18%) | 66 (80.49%) | 0.149 |
| 7.1–8.7 kPa (F2) | 2 (4.55%) | 4 (4.88%) | |
| 8.8–10.3 kPa (F3) | 1 (2.27%) | 4 (4.88%) | |
| ≥10.4 kPa (F4) | 0 (0%) | 8 (9.76%) | |
| CAP (dB/m) | 305.5 (267.5; 337.5) | 300 (260; 340) | 0.640 |
| FIB-4 | 1.01 (0.84; 1.24) | 0.94 (0.67; 1.30) | 0.376 |
| AST (IU/L) | 30.5 (23; 40.5) | 27.5 (24; 37) | 0.498 |
| ALT (IU/L) | 38.5 (29; 59) | 39 (27; 51) | 0.506 |
| GGT (IU/L) | 40.5 (27; 68) | 39 (26; 76) | 0.840 |
| Glucose (mg/dL) | 101.5 (87; 111.5) | 95 (86; 117) | 0.595 |
| Triglycerides (mg/dL) | 130 (91; 173) | 128 (107; 171) | 0.764 |
| Cholesterol (mg/dL) | 205.94 (49.99) | 203.65 (40.92) | 0.804 |
| SDweek (min) | 429 (372.5; 477.5) | 416.5 (372; 450) | 0.456 |
| MSF (min) | 195 (180; 225) | 272.5 (235; 310) | <0.001 |
| MSW (min) | 170 (120; 190) | 225 (200; 255) | <0.001 |
| SDw (min) | 410 (360; 450) | 400 (360; 440) | 0.695 |
| SDf (min) | 458.34 (87.66) | 445.65 (73.99) | 0.392 |
| Mediterranean diet score | 6.84 (2.07) | 7.09 (2.22) | 0.528 |
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | Pseudo R-Squared | p-Value Model | |
|---|---|---|---|---|---|---|
| Model 1 | 40.39 | <0.001 | ||||
| Intermediate + late chronotype | 3.31 (0.90; 12.07) | 0.069 | 9.29 (1.33; 64.50) | 0.024 | ||
| Mediterranean diet score | 0.74 (0.57; 0.94) | 0.018 | 0.69 (0.50; 0.94) | 0.019 | ||
| Female | 0.77 (0.28; 2.11) | 0.617 | 0.33 (0.71; 1.57) | 0.167 | ||
| Age | 1.04 (0.99; 1.09) | 0.059 | 1.00 (0.94; 1.07) | 0.795 | ||
| Body Mass Index | 1.07 (0.99; 1.16) | 0.063 | 1.02 (0.89; 1.16) | 0.751 | ||
| Diabetes | 9.4 (3.19; 27.82) | <0.001 | 7.60 (1.92; 30.05) | 0.004 | ||
| Obstructive sleep apnoea | 9.24 (1.88; 45.41) | 0.006 | 5.55 (0.43; 70.91) | 0.187 | ||
| Hypertension | 5.85 (1.61; 21.27) | 0.007 | 5.16 (0.73; 36.51) | 0.100 | ||
| Dyslipidaemia | 3.58 (0.98; 13.04) | 0.053 | 4.00 (0.65; 24.35) | 0.132 | ||
| Depress | 2.4 (0.43; 13.38) | 0.318 | - | - |
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | Pseudo R-Squared | p-Value Model | |
|---|---|---|---|---|---|---|
| Model 1 | 45.77 | <0.001 | ||||
| Intermediate + late chronotype | 7.37 (0.92; 58.71) | 0.059 | 23.38 (1.63; 335.10) | 0.020 | ||
| Mediterranean diet score | 0.79 (0.59; 1.05) | 0.107 | 0.63 (0.43; 0.93) | 0.021 | ||
| Female | 0.58 (0.16; 1.99) | 0.388 | 0.23 (0.03; 1.51) | 0.126 | ||
| Age | 1.05 (0.99; 1.11) | 0.089 | 1.00 (0.94; 1.07) | 0.809 | ||
| Body Mass Index | 1.04 (0.95; 1.14) | 0.381 | - | - | ||
| Diabetes | 22.75 (4.70; 110.11) | <0.001 | 27.23 (4.33; 171.11) | <0.001 | ||
| Obstructive sleep apnoea | 3.92 (0.68; 22.67) | 0.126 | - | - | ||
| Hypertension | 5.59 (1.18; 26.40) | 0.030 | 5.68 (0.54; 59.52) | 0.147 | ||
| Dyslipidaemia | 2.04 (0.53; 7.85) | 0.296 | - | - | ||
| Depress | 1.48 (0.16; 13.40) | 0.724 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castelnuovo, G.; Perez-Diaz-del-Campo, N.; Rosso, C.; Guariglia, M.; Armandi, A.; Nicolosi, A.; Caviglia, G.P.; Bugianesi, E. Impact of Chronotype and Mediterranean Diet on the Risk of Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Nutrients 2023, 15, 3257. https://doi.org/10.3390/nu15143257
Castelnuovo G, Perez-Diaz-del-Campo N, Rosso C, Guariglia M, Armandi A, Nicolosi A, Caviglia GP, Bugianesi E. Impact of Chronotype and Mediterranean Diet on the Risk of Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Nutrients. 2023; 15(14):3257. https://doi.org/10.3390/nu15143257
Chicago/Turabian StyleCastelnuovo, Gabriele, Nuria Perez-Diaz-del-Campo, Chiara Rosso, Marta Guariglia, Angelo Armandi, Aurora Nicolosi, Gian Paolo Caviglia, and Elisabetta Bugianesi. 2023. "Impact of Chronotype and Mediterranean Diet on the Risk of Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease" Nutrients 15, no. 14: 3257. https://doi.org/10.3390/nu15143257
APA StyleCastelnuovo, G., Perez-Diaz-del-Campo, N., Rosso, C., Guariglia, M., Armandi, A., Nicolosi, A., Caviglia, G. P., & Bugianesi, E. (2023). Impact of Chronotype and Mediterranean Diet on the Risk of Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Nutrients, 15(14), 3257. https://doi.org/10.3390/nu15143257