

The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis
 ,
,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Reporting Guidelines and Protocol Registration
2.2. Criteria for Eligibility
2.3. Literature Search
2.4. Study Selection
2.5. Data Extraction
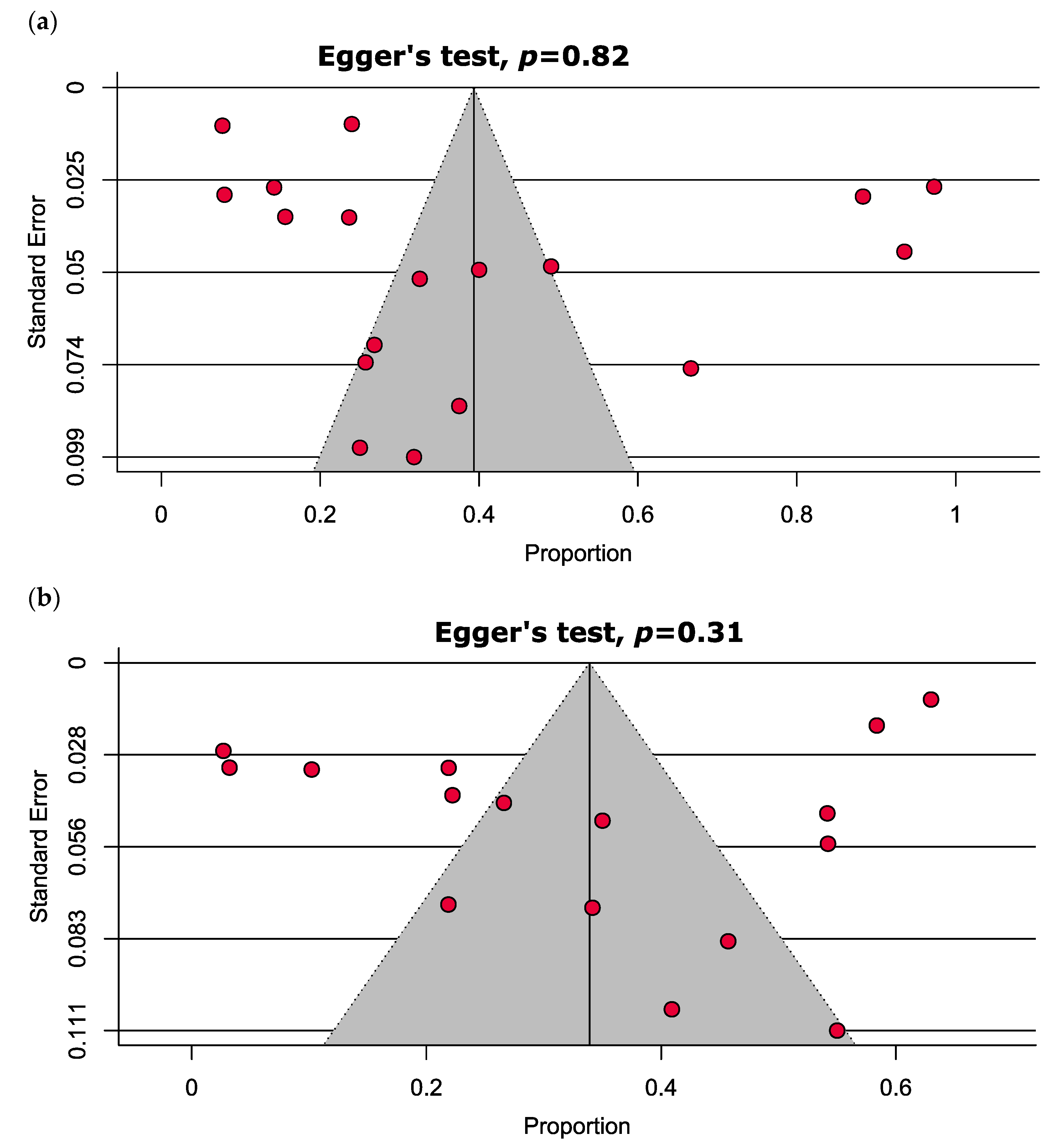
2.6. Quality Assessment and Publication Bias
2.7. Data Analyses
3. Results
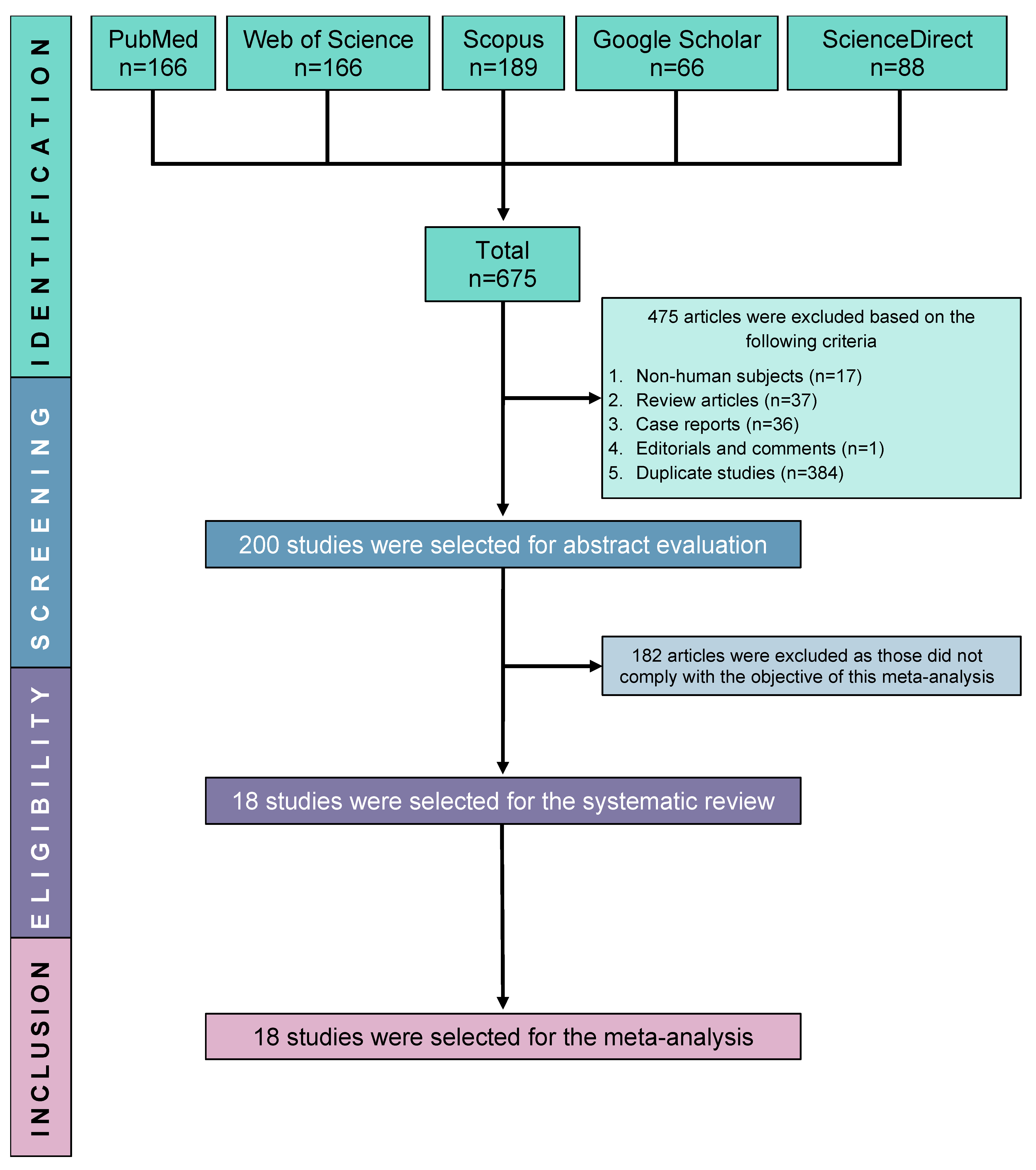
3.1. Selection and Inclusion of Studies
3.2. Study Characteristics
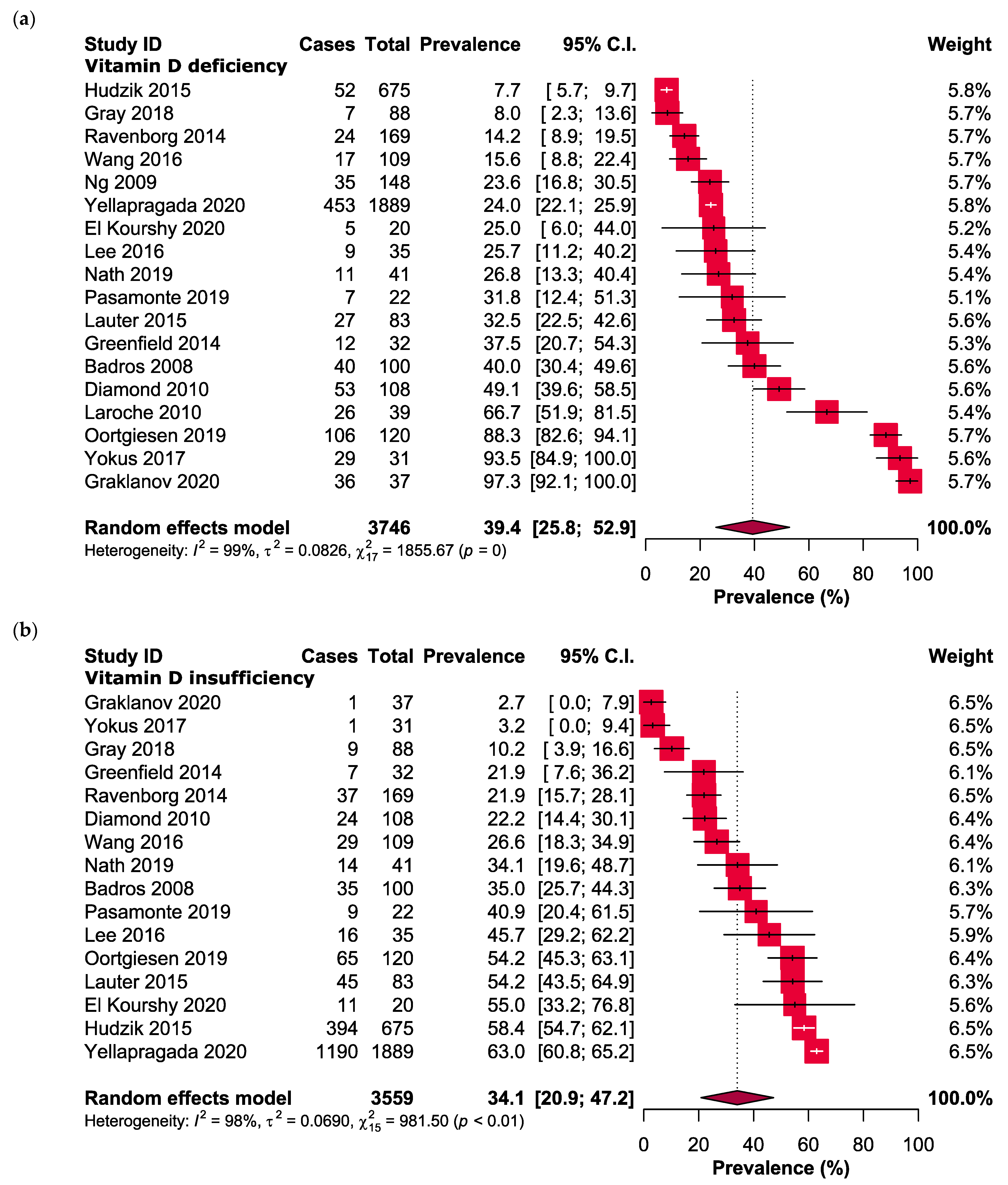
3.3. Main Results: Vitamin D Levels in MM
3.4. Subgroup Analyses
3.5. Quality Assessment
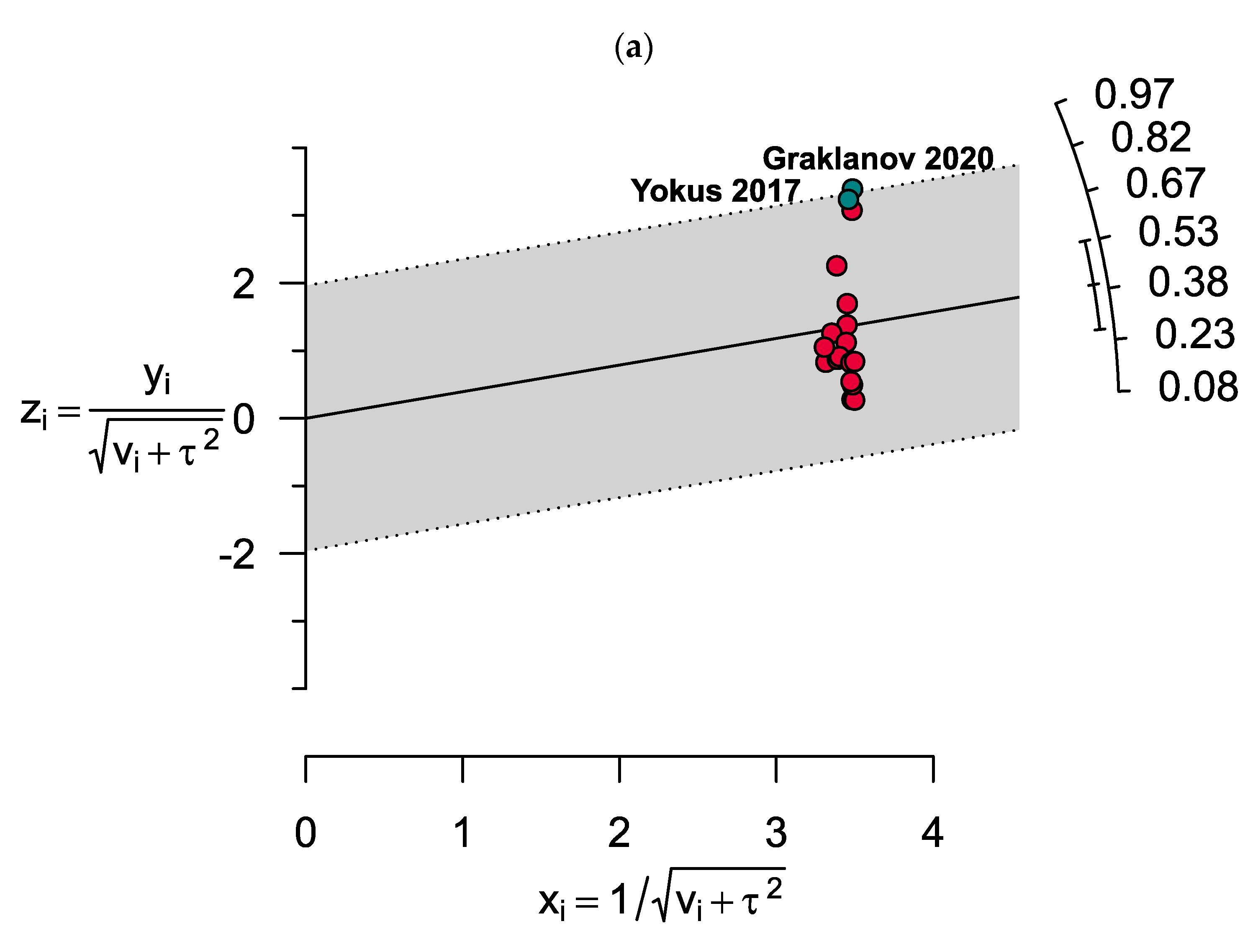
3.6. Heterogeneity and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fairfield, H.; Falank, C.; Avery, L.; Reagan, M.R. Multiple myeloma in the marrow: Pathogenesis and treatments. Ann. N. Y. Acad. Sci. 2016, 1364, 32–51. [Google Scholar] [CrossRef]
- Kumar, S.K.; Rajkumar, V.; Kyle, R.A.; van Duin, M.; Sonneveld, P.; Mateos, M.-V.; Gay, F.; Anderson, K.C. Multiple myeloma. Nat. Rev. Dis. Primers 2017, 3, 17046. [Google Scholar] [CrossRef] [PubMed]
- Capalbo, A.; Lauritano, C. Multiple Myeloma: Possible Cure from the Sea. Cancers 2022, 14, 2965. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Yu, Q.; Wei, G.; Wang, L.; Huang, Y.; Hu, K.; Hu, Y.; Huang, H. Measuring the global, regional, and national burden of multiple myeloma from 1990 to 2019. BMC Cancer 2021, 21, 606. [Google Scholar] [CrossRef] [PubMed]
- Poh, C.; Keegan, T.; Rosenberg, A.S. Second primary malignancies in multiple myeloma: A review. Blood Rev. 2021, 46, 100757. [Google Scholar] [CrossRef]
- Georgakopoulou, R.; Fiste, O.; Sergentanis, T.N.; Andrikopoulou, A.; Zagouri, F.; Gavriatopoulou, M.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Occupational Exposure and Multiple Myeloma Risk: An Updated Review of Meta-Analyses. J. Clin. Med. 2021, 10, 4179. [Google Scholar] [CrossRef]
- Ito, S. Proteasome Inhibitors for the Treatment of Multiple Myeloma. Cancers 2020, 12, 265. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Landgren, O.; Mateos, M.V. Treatment of relapsed and refractory multiple myeloma. Blood Res. 2020, 55, S43–S53. [Google Scholar]
- Rajkumar, S.V.; Landgren, O.; Mateos, M.V. Smoldering multiple myeloma. Blood 2015, 125, 3069–3075. [Google Scholar] [CrossRef]
- Barwick, B.G.; Gupta, V.A.; Vertino, P.M.; Boise, L.H. Cell of Origin and Genetic Alterations in the Pathogenesis of Multiple Myeloma. Front. Immunol. 2019, 10, 1121. [Google Scholar] [CrossRef] [PubMed]
- Abeykoon, J.P.; Tawfiq, R.K.; Kumar, S.; Ansell, S.M. Monoclonal gammopathy of undetermined significance: Evaluation, risk assessment, management, and beyond. Fac. Rev. 2022, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Blum, A.; Bazou, D.; O’Gorman, P. Smoldering multiple myeloma: Prevalence and current evidence guiding treatment decisions. Blood Lymphat. Cancer 2018, 8, 21–31. [Google Scholar] [CrossRef]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The Roles of Vitamin D in Skeletal Muscle: Form, Function, and Metabolism. Endocr. Rev. 2013, 34, 33–83. [Google Scholar] [CrossRef] [PubMed]
- Jones, G. Interpreting vitamin D assay results: Proceed with caution. Clin. J. Am. Soc. Nephrol. 2015, 10, 331–334. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef]
- Thambiah, S.C.; Yeap, S.S. Osteoporosis in South-East Asian Countries. Clin. Biochem. Rev. 2020, 41, 29–40. [Google Scholar]
- Kulling, P.M.; Olson, K.C.; Olson, T.L.; Feith, D.J.; Loughran, T.P., Jr. Vitamin D in hematological disorders and malignancies. Eur. J. Haematol. 2017, 98, 187–197. [Google Scholar] [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef]
- Tabasi, N.; Rastin, M.; Mahmoudi, M.; Ghoryani, M.; Mirfeizi, Z.; Rabe, S.Z.; Reihani, H. Influence of vitamin D on cell cycle, apoptosis, and some apoptosis related molecules in systemic lupus erythematosus. Iran. J. Basic Med. Sci. 2015, 18, 1107–1111. [Google Scholar]
- Ng, A.C.; Khosla, S.; Charatcharoenwitthaya, N.; Kumar, S.K.; Achenbach, S.J.; Holets, M.F.; McCready, L.K.; Melton, L.J., 3rd; Kyle, R.A.; Rajkumar, S.V.; et al. Bone microstructural changes revealed by high-resolution peripheral quantitative computed tomography imaging and elevated DKK1 and MIP-1α levels in patients with MGUS. Blood 2011, 118, 6529–6534. [Google Scholar] [CrossRef]
- Kristinsson, S.Y.; Tang, M.; Pfeiffer, R.M.; Björkholm, M.; Blimark, C.; Mellqvist, U.H.; Wahlin, A.; Turesson, I.; Landgren, O. Monoclonal gammopathy of undetermined significance and risk of skeletal fractures: A population-based study. Blood 2010, 116, 2651–2655. [Google Scholar] [CrossRef]
- Piot, J.M.; Royer, M.; Schmidt-Tanguy, A.; Hoppé, E.; Gardembas, M.; Bourrée, T.; Hunault, M.; François, S.; Boyer, F.; Ifrah, N.; et al. Factors associated with an increased risk of vertebral fracture in monoclonal gammopathies of undetermined significance. Blood Cancer J. 2015, 5, e345. [Google Scholar] [CrossRef] [PubMed]
- Innao, V.; Allegra, A.; Ginaldi, L.; Pioggia, G.; De Martinis, M.; Musolino, C.; Gangemi, S. Reviewing the Significance of Vitamin D Substitution in Monoclonal Gammopathies. Int. J. Mol. Sci. 2021, 22, 4922. [Google Scholar] [CrossRef] [PubMed]
- Hope, C.; Ollar, S.J.; Heninger, E.; Hebron, E.; Jensen, J.L.; Kim, J.; Maroulakou, I.; Miyamoto, S.; Leith, C.; Yang, D.T.; et al. TPL2 kinase regulates the inflammatory milieu of the myeloma niche. Blood 2014, 123, 3305–3315. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.; Kumar, S.K.; Rajkumar, S.V.; Drake, M.T. Impact of vitamin D deficiency on the clinical presentation and prognosis of patients with newly diagnosed multiple myeloma. Am. J. Hematol. 2009, 84, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Aribi, M.; Mennechet, F.J.D.; Touil-Boukoffa, C. Editorial: The role of vitamin D as an immunomodulator. Front. Immunol. 2023, 14, 1186635. [Google Scholar] [CrossRef]
- McCachren, S.S.; Dhodapkar, K.M.; Dhodapkar, M.V. Co-evolution of Immune Response in Multiple Myeloma: Implications for Immune Prevention. Front. Immunol. 2021, 12, 632564. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Carrillo-Cruz, E.; Montero, I.; Perez-Simon, J.A. Vitamin D: Effect on Haematopoiesis and Immune System and Clinical Applications. Int. J. Mol. Sci. 2018, 19, 2663. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, L.; Xu, H.J.; Li, Y.; Hu, C.M.; Yang, J.Y.; Sun, M.Y. The Anti-Inflammatory Effects of Vitamin D in Tumorigenesis. Int. J. Mol. Sci. 2018, 19, 2736. [Google Scholar] [CrossRef]
- D’Amore, C.; Marsico, F.; Parente, A.; Paolillo, S.; De Martino, F.; Gargiulo, P.; Ferrazzano, F.; De Roberto, A.M.; La Mura, L.; Marciano, C.; et al. Vitamin D deficiency and clinical outcome in patients with chronic heart failure: A review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 837–849. [Google Scholar] [CrossRef] [PubMed]
- Gotsman, I.; Shauer, A.; Zwas, D.R.; Hellman, Y.; Keren, A.; Lotan, C.; Admon, D. Vitamin D deficiency is a predictor of reduced survival in patients with heart failure; Vitamin D supplementation improves outcome. Eur. J. Heart Fail. 2012, 14, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Ravenborg, N.; Udd, K.; Berenson, A.; Costa, F.; Berenson, J.R. Vitamin D Levels Are Frequently below Normal in Multiple Myeloma Patients and Are Infrequently Assessed By Their Treating Physicians. Blood 2014, 124, 5769. [Google Scholar] [CrossRef]
- Clement, Z.; Ashford, M.; Sivakumaran, S. Vitamin D deficiency in a man with multiple myeloma. N. Am. J. Med. Sci. 2011, 3, 469–471. [Google Scholar] [PubMed]
- Schjesvold, F. Evolution of diagnostic workup and treatment for multiple myeloma 2013–2019. Eur. J. Haematol. 2020, 105, 434–448. [Google Scholar] [CrossRef]
- Ito, Y.; Honda, A.; Kurokawa, M. Impact of vitamin D level at diagnosis and transplantation on the prognosis of hematological malignancy: A meta-analysis. Blood Adv. 2022, 6, 1499–1511. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- Seak, Y.S.; Nor, J.; Tuan Kamauzaman, T.H.; Arithra, A.; Islam, M.A. Efficacy and Safety of Intranasal Ketamine for Acute Pain Management in the Emergency Setting: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3978. [Google Scholar] [CrossRef]
- Hasim, N.; Bakar, M.A.A.; Islam, M.A. Efficacy and Safety of Isotonic and Hypotonic Intravenous Maintenance Fluids in Hospitalised Children: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Children 2021, 8, 785. [Google Scholar] [CrossRef]
- Badros, A.; Goloubeva, O.; Terpos, E.; Milliron, T.; Baer, M.R.; Streeten, E. Prevalence and significance of vitamin D deficiency in multiple myeloma patients. Br. J. Haematol. 2008, 142, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Diamond, T.; Golombick, T.; Manoharan, A. Vitamin D status may effect the skeletal complications of multiple myeloma. Am. J. Hematol. 2010, 85, 302–303. [Google Scholar] [CrossRef] [PubMed]
- Graklanov, V.; Popov, V.; Raycheva, R. Serum Levels of Vitamin D in Patients with Multiple Myeloma. Folia Medica 2020, 62, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Gray, N.; Herbert, F.; Shields, M.; Frewin, R. Vitamin D Deficiency and Bisphosphonate usage in myeloma. In British Journal of Haematology; Wiley: Hoboken, NJ, USA, 2018. [Google Scholar]
- Greenfield, D.M.; Boland, E.; Ezaydi, Y.; Ross, R.J.; Ahmedzai, S.H.; Snowden, J.A. Endocrine, metabolic, nutritional and body composition abnormalities are common in advanced intensively-treated (transplanted) multiple myeloma. Bone Marrow Transpl. 2014, 49, 907–912. [Google Scholar] [CrossRef]
- Hudzik, S.; Snoad, B.; Mousa, L.; Sborov, D.W.; Williams, N.; Jones, D.; Hofmeister, C.C. The Majority of Myeloma Patients Are Vitamin D Deficient, Unrelated to Survival or Cytogenetics. Blood 2015, 126, 5336. [Google Scholar] [CrossRef]
- Laroche, M.; Lemaire, O.; Attal, M. Vitamin D deficiency does not alter biochemical markers of bone metabolism before or after autograft in patients with multiple myeloma. Eur. J. Haematol. 2010, 85, 65–67. [Google Scholar] [CrossRef]
- Lauter, B.; Schmidt-Wolf, I.G. Prevalence, Supplementation, and Impact of Vitamin D Deficiency in Multiple Myeloma Patients. Cancer Investig. 2015, 33, 505–509. [Google Scholar] [CrossRef]
- Lee, M.S.; Kim, S.H.; Yun, J.; Kim, C.K.; Park, S.K.; Hong, D.S. Associations Between Serum Vitamin D Level and Skeletal Complications in Multiple Myeloma Patients. Soonchunhyang Med. Sci. 2016, 22, 102–107. [Google Scholar] [CrossRef]
- Nath, K.; Ganeshalingam, V.; Ewart, B.; Heyer, E.; Watt, K.; Birchley, A.; Casey, J.; Lai, H.C.; Morris, E.; Hodges, G. A retrospective analysis of the prevalence and clinical outcomes of vitamin D deficiency in myeloma patients in tropical Australia. Support. Care Cancer 2020, 28, 1249–1254. [Google Scholar] [CrossRef]
- Wang, J.; Udd, K.A.; Vidisheva, A.; Swift, R.A.; Spektor, T.M.; Bravin, E.; Ibrahim, E.; Treisman, J.; Masri, M.; Berenson, J.R. Low serum vitamin D occurs commonly among multiple myeloma patients treated with bortezomib and/or thalidomide and is associated with severe neuropathy. Support. Care Cancer 2016, 24, 3105–3110. [Google Scholar] [CrossRef]
- Yellapragada, S.V.; Fillmore, N.R.; Frolov, A.; Zhou, Y.; Dev, P.; Yameen, H.; Ifeorah, C.; Do, N.V.; Brophy, M.T.; Munshi, N.C. Vitamin D deficiency predicts for poor OS in white but not African American patients with multiple myeloma. Blood Adv. 2020, 4, 1643–1646. [Google Scholar] [CrossRef] [PubMed]
- Yokuş, O.; Hilmi, D.; Aydinli, F.; Eren, R.; Altindal, S. Vitamin D deficiency and its effects on patients with multiple myeloma. Hematol. Transfus. Int. J. 2017, 5, 00112. [Google Scholar]
- Oortgiesen, B.E.; Kroes, J.A.; Scholtens, P.; Hoogland, J.; Dannenberg-de Keijzer, P.; Siemes, C.; Jansman, F.G.A.; Kibbelaar, R.E.; Veeger, N.; Hoogendoorn, M.; et al. High prevalence of peripheral neuropathy in multiple myeloma patients and the impact of vitamin D levels, a cross-sectional study. Support. Care Cancer 2022, 30, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Pasamonte, D.; Mesina, F. Status of Vitamin D-25 Hydroxy Vitamin D {25 (OH)} in Patients with Multiple Myeloma. J. Med. Univ. St. Tomas 2019, 3, 277–281. [Google Scholar] [CrossRef]
- El Kourshy, S.A.E.W.E.; Same, H.F.A.E.; Fouad, M.M.; Ibrahim, N.M. MM-125: Assessment of Vitamin D Levels in Multiple Myeloma Patients Newly Diagnosed and After Treatment. Clin. Lymphoma Myeloma Leuk. 2020, 20, S294. [Google Scholar] [CrossRef]
- Burwick, N. Vitamin D and plasma cell dyscrasias: Reviewing the significance. Ann. Hematol. 2017, 96, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Looker, A.C.; Pfeiffer, C.M.; Lacher, D.A.; Schleicher, R.L.; Picciano, M.F.; Yetley, E.A. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am. J. Clin. Nutr. 2008, 88, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Maier, G.S.; Horas, K.; Kurth, A.A.; Lazovic, D.; Seeger, J.B.; Maus, U. Prevalence of vitamin D deficiency in patients with bone metastases and multiple myeloma. Anticancer Res. 2015, 35, 6281–6285. [Google Scholar]
- Moan, J.; Porojnicu, A.C.; Dahlback, A.; Setlow, R.B. Addressing the health benefits and risks, involving vitamin D or skin cancer, of increased sun exposure. Proc. Natl. Acad. Sci. USA 2008, 105, 668–673. [Google Scholar] [CrossRef]
- Drake, M.; Ng, A. Vitamin D Deficiency in Multiple Myeloma. Eur. J. Clin. Med. Oncol. 2010, 2, 1. [Google Scholar]
- Yeum, K.J.; Song, B.C.; Joo, N.S. Impact of Geographic Location on Vitamin D Status and Bone Mineral Density. Int. J. Environ. Res. Public Health 2016, 13, 184. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J.; et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, N.G.; Chaplin, G. The evolution of human skin coloration. J. Hum. Evol. 2000, 39, 57–106. [Google Scholar] [CrossRef] [PubMed]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- MacLaughlin, J.; Holick, M.F. Aging decreases the capacity of human skin to produce vitamin D3. J. Clin. Investig. 1985, 76, 1536–1538. [Google Scholar] [CrossRef]
- Holick, M.F.; Matsuoka, L.Y.; Wortsman, J. Age, vitamin D, and solar ultraviolet. Lancet 1989, 2, 1104–1105. [Google Scholar] [CrossRef]
- Chailurkit, L.O.; Aekplakorn, W.; Ongphiphadhanakul, B. Regional variation and determinants of vitamin D status in sunshine-abundant Thailand. BMC Public Health 2011, 11, 853. [Google Scholar] [CrossRef]
- Andersen, T.L.; Boissy, P.; Sondergaard, T.; Kupisiewicz, K.; Plesner, T.; Rasmussen, T.; Haaber, J.; Kølvraa, S.; Delaissé, J.M. Osteoclast nuclei of myeloma patients show chromosome translocations specific for the myeloma cell clone: A new type of cancer–host partnership? J. Pathol. 2007, 211, 10–17. [Google Scholar] [CrossRef]
- Calvani, N.; Cafforio, P.; Silvestris, F.; Dammacco, F. Functional osteoclast-like transformation of cultured human myeloma cell lines. Br. J. Haematol. 2005, 130, 926–938. [Google Scholar] [CrossRef]
- Walsh, M.C.; Choi, Y. Biology of the RANKL–RANK–OPG system in immunity, bone, and beyond. Front. Immunol. 2014, 5, 511. [Google Scholar] [CrossRef]
- elton III, L.J.; Rajkumar, S.V.; Khosla, S.; Achenbach, S.J.; Oberg, A.L.; Kyle, R.A. Fracture risk in monoclonal gammopathy of undetermined significance. J. Bone Miner Res. 2004, 19, 25–30. [Google Scholar]
- De Martinis, M.; Allegra, A.; Sirufo, M.M.; Tonacci, A.; Pioggia, G.; Raggiunti, M.; Ginaldi, L.; Gangemi, S. Vitamin D Deficiency, Osteoporosis and Effect on Autoimmune Diseases and Hematopoiesis: A Review. Curr. Opin. Rheumatol. 2021, 22, 8855. [Google Scholar] [CrossRef] [PubMed]
- Miceli, T.J.N.A. Maintaining bone health in patients with multiple myeloma. Clin. J. Oncol. Nurs. 1969, 15, 9–23. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L.J.A.O.B. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Roodman, G.D.J.L. Pathogenesis of myeloma bone disease. Leukemia 2009, 23, 435–441. [Google Scholar] [CrossRef]
- Tobeiha, M.; Moghadasian, M.H.; Amin, N.; Jafarnejad, S. RANKL/RANK/OPG pathway: A mechanism involved in exercise-induced bone remodeling. BioMed Res. Int. 2020, 2020, 6910312. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Wang, Y.; Lu, M.; Chu, B.; Shi, L.; Gao, S.; Fang, L.; Xiang, Q.; Ding, Y.; Liu, X.; et al. Vitamin D deficiency linked to abnormal bone and lipid metabolism predicts high-risk multiple myeloma with poorer prognosis. Front. Endocrinol. 2023, 14, 1157969. [Google Scholar] [CrossRef]
- Iranijam, E.; Matin, S.; Negaresh, M. A case of a Young Multiple Myeloma Patient With Poor Prognostic Cytogenetics. Clin. Med. Insights Case Rep. 2023, 16, 11795476231157245. [Google Scholar] [CrossRef]
- Pike, J.W.; Meyer, M.B.J.R.D.C. The vitamin D receptor: New paradigms for the regulation of gene expression by 1, 25-dihydroxyvitamin D3. Endocrinol. Metab. Clin. N. Am. 2012, 38, 13–27. [Google Scholar] [CrossRef]
- Rui, H.; Liu, Y.; Lin, M.; Zheng, X. Vitamin D receptor gene polymorphism is associated with multiple myeloma. J. Cell. Biochem. 2020, 121, 224–230. [Google Scholar] [CrossRef]
- Shafia, S.; Qasim, I.; Aziz, S.A.; Bhat, I.A.; Nisar, S.; Shah, Z. Role of vitamin D receptor (VDR) polymorphisms in susceptibility to multiple myeloma in ethnic Kashmiri population. Blood Cells Mol. Dis. 2013, 51, 56–60. [Google Scholar] [CrossRef]
- Gascoyne, D.M.; Lyne, L.; Spearman, H.; Buffa, F.M.; Soilleux, E.J.; Banham, A. Vitamin D receptor expression in plasmablastic lymphoma and myeloma cells confers susceptibility to vitamin D. Endocrinology 2017, 158, 503–515. [Google Scholar] [CrossRef]
- Kumar, R.; Gupta, N.; Sharma, A. Delineating association between polymorphic variants of vitamin D receptor (VDR) gene and multiple myeloma disease in Indian population. J. Steroid Biochem. Mol. Biol. 2019, 19, e69. [Google Scholar] [CrossRef]
- Kumar, R.; Gupta, N.; Singh, V.; Kumar, V.; Haq, A.; Mirza, A.A.; Sharma, A.J. Unveiling molecular associations of polymorphic variants of VDR gene (FokI, BsmI and ApaI) in multiple myeloma patients of Indian population. J. Steroid Biochem. Mol. Biol. 2020, 199, 105588. [Google Scholar] [CrossRef]
- Chen, P.; Du, Z.-L.; Zhang, Y.; Liu, B.; Guo, Z.; Lou, J.-X.; He, X.-P.; Chen, H.-R. Association of VEGF and VDR gene-gene and gene-smoking interaction on risk of multiple myeloma in Chinese Han population. Oncotarget 2017, 8, 36509. [Google Scholar] [CrossRef]
- Wiers, K.M.; Lathers, D.M.R.; Wright, M.A.; Young, M.R.I. Vitamin D3 treatment to diminish the levels of immune suppressive CD34+ cells increases the effectiveness of adoptive immunotherapy. J. Immunother. 2000, 23, 115–124. [Google Scholar] [CrossRef]
- De Veirman, K.; Menu, E.; Maes, K.; De Beule, N.; De Smedt, E.; Maes, A.; Vlummens, P.; Fostier, K.; Kassambara, A.; Moreaux, J.J.C.L. Myeloid-derived suppressor cells induce multiple myeloma cell survival by activating the AMPK pathway. Cancer Lett. 2019, 442, 233–241. [Google Scholar] [CrossRef]
- Dauletbaev, N.; Herscovitch, K.; Das, M.; Chen, H.; Bernier, J.; Matouk, E.; Bérubé, J.; Rousseau, S.; Lands, L.J. Down-regulation of IL-8 by high-dose vitamin D is specific to hyperinflammatory macrophages and involves mechanisms beyond up-regulation of DUSP1. Br. J. Pharmacol. 2015, 172, 4757–4771. [Google Scholar] [CrossRef]
- Görgün, G.T.; Whitehill, G.; Anderson, J.L.; Hideshima, T.; Maguire, C.; Laubach, J.; Raje, N.; Munshi, N.C.; Richardson, P.G.; Anderson, K.C.J.B. Tumor-promoting immune-suppressive myeloid-derived suppressor cells in the multiple myeloma microenvironment in humans. Blood 2013, 121, 2975–2987. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Arima, K.; Mizukami, S.; Nishimura, T.; Tomita, Y.; Nakashima, H.; Abe, Y.; Aoyagi, K. Epidemiology of the association between serum 25-hydroxyvitamin D levels and musculoskeletal conditions among elderly individuals: A literature review. J. Physiol. Anthropol. 2020, 39, 1–6. [Google Scholar] [CrossRef]
- Kulig, P.; Łuczkowska, K.; Bielikowicz, A.; Zdrojewska, D.; Baumert, B.; Machaliński, B.J.N. Vitamin D as a Potential Player in Immunologic Control over Multiple Myeloma Cells: Implications for Adjuvant Therapies. Nutrients 2022, 14, 1802. [Google Scholar] [CrossRef]
- Van Schoor, N.; Visser, M.; Pluijm, S.; Kuchuk, N.; Smit, J.; Lips, P.J.B. Vitamin D deficiency as a risk factor for osteoporotic fractures. Bone 2008, 42, 260–266. [Google Scholar] [CrossRef]
- de Haan, K.; Groeneveld, A.; de Geus, H.R.; Egal, M.; Struijs, A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: Systematic review and meta-analysis. Crit Care 2014, 18, 660. [Google Scholar] [CrossRef]
- Kostoglou-Athanassiou, I.; Pantazi, E.; Kontogiannis, S.; Kousouris, D.; Mavropoulos, I.; Athanassiou, P. Vitamin D in acutely ill patients. J. Int. Med. Res. 2018, 46, 4246–4257. [Google Scholar] [CrossRef]
- Terpos, E.; Sezer, O.; Croucher, P.; García-Sanz, R.; Boccadoro, M.; San Miguel, J.; Ashcroft, J.; Bladé, J.; Cavo, M.; Delforge, M.J.A.o.O. The use of bisphosphonates in multiple myeloma: Recommendations of an expert panel on behalf of the European Myeloma Network. Ann. Oncol. 2009, 20, 1303–1317. [Google Scholar] [CrossRef]
- Polascik, T.J.; Mouraviev, V.J.T. Zoledronic acid in the management of metastatic bone disease. Ther. Clin. Risk Manag. 2008, 4, 261. [Google Scholar] [CrossRef]
- Drake, M.T.; Clarke, B.L.; Khosla, S. Bisphosphonates: Mechanism of action and role in clinical practice. In Mayo Clinic Proceedings; Elsevie: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Nancollas, G.; Tang, R.; Phipps, R.; Henneman, Z.; Gulde, S.; Wu, W.; Mangood, A.; Russell, R.; Ebetino, F.J.B. Novel insights into actions of bisphosphonates on bone: Differences in interactions with hydroxyapatite. Bone 2006, 38, 617–627. [Google Scholar] [CrossRef]
- Park, J.; Pandya, V.R.; Ezekiel, S.J.; Berghuis, A.M. Phosphonate and bisphosphonate inhibitors of farnesyl pyrophosphate synthases: A structure-guided perspective. Front. Chem. 2021, 8, 1233. [Google Scholar] [CrossRef]
- Terpos, E.; Zamagni, E.; Lentzsch, S.; Drake, M.T.; García-Sanz, R.; Abildgaard, N.; Ntanasis-Stathopoulos, I.; Schjesvold, F.; de la Rubia, J.; Kyriakou, C. Treatment of multiple myeloma-related bone disease: Recommendations from the Bone Working Group of the International Myeloma Working Group. Lancet Oncol. 2021, 22, e119–e130. [Google Scholar] [CrossRef]
- Schieferdecker, A.; Voigt, M.; Riecken, K.; Braig, F.; Schinke, T.; Loges, S.; Bokemeyer, C.; Fehse, B.; Binder, M.J.O. Denosumab mimics the natural decoy receptor osteoprotegerin by interacting with its major binding site on RANKL. Oncotarget 2014, 5, 6647. [Google Scholar] [CrossRef]
- Goldstein, D.A.J.H. Denosumab for bone lesions in multiple myeloma–what is its value? Haematologica 2018, 103, 753. [Google Scholar] [CrossRef] [PubMed]
- Lipton, A.; Fizazi, K.; Stopeck, A.T.; Henry, D.H.; Brown, J.E.; Yardley, D.A.; Richardson, G.E.; Siena, S.; Maroto, P.; Clemens, M. Superiority of denosumab to zoledronic acid for prevention of skeletal-related events: A combined analysis of 3 pivotal, randomised, phase 3 trials. Eur. J. Cancer 2012, 48, 3082–3092. [Google Scholar] [CrossRef]
- Henry, D.H.; Costa, L.; Goldwasser, F.; Hirsh, V.; Hungria, V.; Prausova, J.; Scagliotti, G.V.; Sleeboom, H.; Spencer, A.; Vadhan-Raj, S. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J. Clin. Oncol. 2011, 29, 1125–1132. [Google Scholar] [CrossRef]
- Raje, N.; Terpos, E.; Willenbacher, W.; Shimizu, K.; García-Sanz, R.; Durie, B.; Legieć, W.; Krejčí, M.; Laribi, K.; Zhu, L. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: An international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018, 19, 370–381. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Study ID [References] | Type of Study | Country, Location (Latitude) | Number of MM Patients (Female%), MM Stage (%) | Types of MM Patients | Age of the Participants (Mean ± SD/Median (IQR)/Range) (Years) | Vitamin D Measurement Method | Cut-Off for Vitamin D Insufficiency; Deficiency (ng/mL) | Current Treatment Status | Were the Patients on Vitamin D Supplements? |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Badros 2008 [41] | Cohort | USA, Baltimore, 39.2904° N | 100 (42.0), NR | NDMM | 59.0 (29.0–80.0) | NR | 14–30; ≤14 | None | Yes, 20% |
| 2 | Diamond 2010 [42] | Cohort | Australia, New South Wales, 31.2532° S | 108 (46.0), NR | UT | 69.1 ± 10.5 | Chemiluminescent immunoassay | 20–30; <20 | NR | NR |
| 3 | El Kourshy 2020 [56] | Case-control | Egypt, Cairo, 30.0444° N | 60 (NR), NR | NDMM and UT | NR | ELISA | 10–30; <10 | NR | NR |
| 4 | Graklanov 2020 [43] | Cross-sectional | Bulgaria, Plovdiv, 42.1354° N | 37 (51.4), Stage I: 13.5 Stage II: 13.5 Stage III: 70.0 | NDMM | 68.0 ± NR | ELISA | 20–30; <20 | None | NR |
| 5 | Gray 2018 [44] | Cohort | Gloucester, United Kingdom 51.8642° N | 88 (NR), NR | NDMM | NR | NR | NR | None | NR |
| 6 | Greenfield 2014 [45] | Cross-sectional | Sheffield, United Kingdom, 53.3811° N | 32 (47.0), NR | UT | 61.0 (41.0–71.0) | NR | 12–20; <12 | Cyclophosphamide, melphalan, high-dose steroids, doxorubicin, vincristine, thalidomide, bortezomib, lenalidomide, fludarabine, etoposide, cytarabine, cisplatin, and/or interferon alpha | NR |
| 7 | Hudzik 2015 [46] | Cross-sectional | Ohio State, USA, 40.4173° N | 675 (NR), Stage I: 28.6 Stage II: 48.7 Stage III: 21.9 | NDMM | 64.0 (28.0–95.0) | NR | 10–30; <10 | NR | NR |
| 8 | Laroche 2010 [47] | Cohort | Toulouse, France, 43.6047° N | 39 (59.0), NR | NDMM and UT | 56.0 ± 6.6 | Chemiluminescent immunoassay | <20; NR | High-dose chemotherapy | NR |
| 9 | Lauter 2015 [48] | Cohort | Bonn, Germany, 50.7374° N | 83 (38.5), NR | NDMM and UT | 66.3 (43.0–86.0) | Chemiluminescence immunoassay | 10–30; <10 | NR | Yes |
| 10 | Lee 2016 [49] | Cross-sectional | Bucheon, South Korea, 37.5034° N | 35 (42.9), NR | NDMM | 64.0 (60.0–74.0) | Tandem mass spectrometry | 10–20; <10 | Analgesic, acetaminophen, and opioid | NR |
| 11 | Nath 2019 [50] | Cross-sectional | Townsville, Australia, 19.2590° S | 41 (76.0), Stage I: 47.0 Stage II: 42.0 Stage III: 11.0 | UT | 69.0 (45.0–90.0) | Liquid chromatography–tandem mass spectrometry | 8–12; <20 | Bisphosphonate, alkylators, steroids, proteasome inhibitors, immunomodulatory agents, monoclonal antibodies, and/or bisphosphonates | Yes |
| 12 | Ng 2009 [26] | Cohort | Rochester, USA, 43.1566° N | 148 (38.0), NR | NDMM | 60.3 (56.6–63.9) | Liquid chromatography–tandem mass spectrometry or high-performance liquid chromatography | NR; <20 | None | NR |
| 13 | Oortgiesen 2019 [54] | Cross-sectional | Leeuwarden, Netherlands, 53.2012° N | 120 (42.5), NR | UT | 68.0 (48.0–84.0) | NR | NR; <30 | NR | NR |
| 14 | Pasamonte 2019 [55] | Cross-sectional | Manila, Philippines, 14.5995° N | 22 (55.0), NR | NDMM and UT | 61.3 ± 10.0 | NR | 21–29; <20 | NR | NR |
| 15 | Ravenborg 2014 [33] | Cohort | West Hollywood, USA, 34.0900° N | 169 (38.0), NR | NR | 65.4 (38.0–85.0) | NR | 20–30; <20 | NR | NR |
| 16 | Wang 2016 [51] | Cohort | California, USA, 36.7783° N | 111 (46.0), NR | UT | 66.0 (42.0–89.0) | Liquid chromatography–tandem mass spectrometry or immunoassay | 20.0–29.9; <20 | Bortezomib and/or thalidomide | NR |
| 17 | Yellapragada 2020 [52] | Cohort | Boston, USA, 42.3601° N | 1889 (3.2), Stage I: 18.3 Stage II: 30.2 Stage III: 51.5 | UT | 68.9 ± 10.2 | NR | NR; <20 | NR | Yes |
| 18 | Yokus 2017 [53] | Cohort | Istanbul, Turkey, 41.0082° N | 30 (36.7), Stage I: 16.1 Stage II: 35.5 Stage III: 48.4 | UT | 63.0 (49.0–90.0) | NR | 21–29; ≤20 | NR | NR |
| Strategies of Subgroup Analyses | Prevalence [95% CIs] (%) | Number of Studies Analyzed | Total Number of Subjects | Heterogeneity | |
|---|---|---|---|---|---|
| I2 | p-Value | ||||
| Vitamin D deficiency | |||||
| NDMM | 43.0 [6.8–79.1] | 6 | 385 | 99% | <0.0001 |
| UT | 41.6 [19.3–64.0] | 7 | 2488 | 99% | <0.0001 |
| Europe | 60.7 [29.4–91.9] | 7 | 430 | 99% | <0.0001 |
| North America | 20.4 [11.8–28.9] | 6 | 3090 | 97% | <0.0001 |
| Australia | 30.1 [22.8–37.5] | 2 | 149 | 0% | 0.57 |
| Asia | 27.9 [16.3–39.5] | 2 | 57 | 0% | 0.62 |
| Africa | 25.0 [6.0–44.0] | 1 | 20 | NA | NA |
| Vitamin D insufficiency | |||||
| NDMM | 30.2 [3.2–57.2] | 5 | 935 | 99% | <0.0001 |
| UT | 32.3 [10.0–54.5] | 7 | 2330 | 99% | <0.0001 |
| Europe | 24.1 [6.4–41.8] | 6 | 391 | 97% | <0.0001 |
| North America | 41.3 [25.5–57.0] | 5 | 2942 | 98% | <0.0001 |
| Australia | 26.6 [15.3–37.8] | 2 | 149 | 50% | 0.15 |
| Asia | 43.8 [31.0–56.7] | 2 | 57 | 0% | 0.72 |
| Africa | 55.0 [33.2–76.8] | 1 | 20 | NA | NA |
| Strategies of Sensitivity Analyses | Prevalence [95% CIs] (%) | The Difference in Pooled Prevalence Compared to the Main Result | Number of Studies Analyzed | Total Number of Subjects | Heterogeneity | |
|---|---|---|---|---|---|---|
| I2 | p-Value | |||||
| Vitamin D deficiency | ||||||
| Excluding small studies | 32.7 [17.8–47.6] | 6.7% lower | 8 | 3318 | 99% | <0.0001 |
| Excluding low- and moderate-quality studies | 41.0 [25.0–57.0] | 1.6% higher | 14 | 3418 | 99% | <0.0001 |
| Considering only cross-sectional studies | 45.2 [5.8–84.5] | 5.8% higher | 7 | 962 | 100% | <0.0001 |
| Vitamin D insufficiency | ||||||
| Excluding small studies | 40.4 [26.6–54.2] | 6.3% higher | 7 | 3170 | 98% | <0.0001 |
| Excluding low- and moderate-quality studies | 38.1 [22.7–53.4] | 4.0% higher | 12 | 3231 | 99% | <0.0001 |
| Considering only cross-sectional studies | 33.8 [7.2–60.5] | 0.3% lower | 6 | 842 | 98% | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismail, N.H.; Mussa, A.; Al-Khreisat, M.J.; Mohamed Yusoff, S.; Husin, A.; Johan, M.F.; Islam, M.A. The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3227. https://doi.org/10.3390/nu15143227
Ismail NH, Mussa A, Al-Khreisat MJ, Mohamed Yusoff S, Husin A, Johan MF, Islam MA. The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(14):3227. https://doi.org/10.3390/nu15143227
Chicago/Turabian StyleIsmail, Nor Hayati, Ali Mussa, Mutaz Jamal Al-Khreisat, Shafini Mohamed Yusoff, Azlan Husin, Muhammad Farid Johan, and Md Asiful Islam. 2023. "The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis" Nutrients 15, no. 14: 3227. https://doi.org/10.3390/nu15143227
APA StyleIsmail, N. H., Mussa, A., Al-Khreisat, M. J., Mohamed Yusoff, S., Husin, A., Johan, M. F., & Islam, M. A. (2023). The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis. Nutrients, 15(14), 3227. https://doi.org/10.3390/nu15143227