
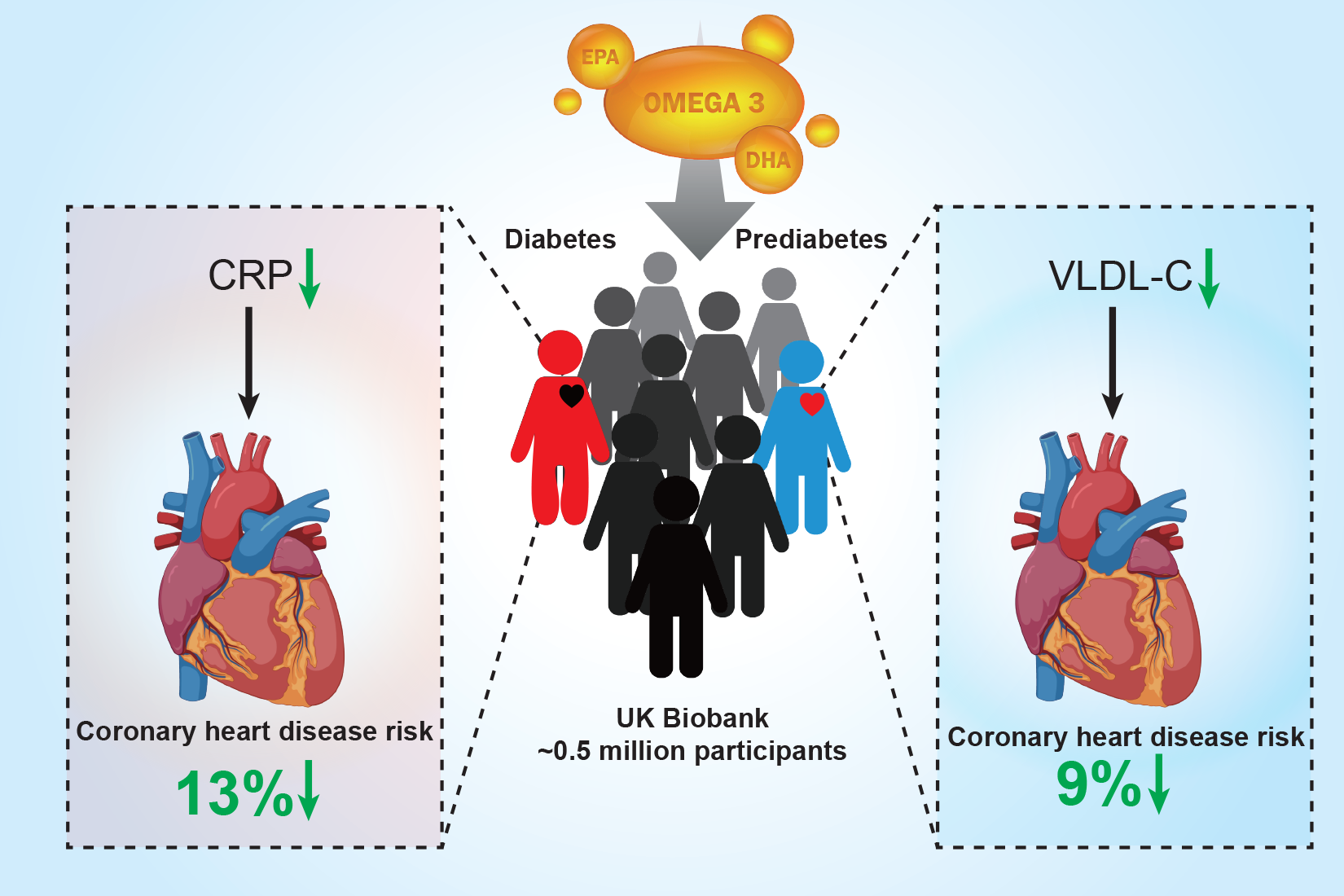
Association of Fish Oil Supplementation with Risk of Coronary Heart Disease in Individuals with Diabetes and Prediabetes: A Prospective Study in the UK Biobank

 , and
, and
Abstract

1. Introduction
2. Methods
2.1. Study Population
2.2. Assessment of Fish Oil Supplementation and Covariates
2.3. Ascertainment of Coronary Heart Disease (CHD)
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Fish Oil Supplementation and Risk of CHD
3.3. Fish Oil Supplementation and Serum Biomarkers
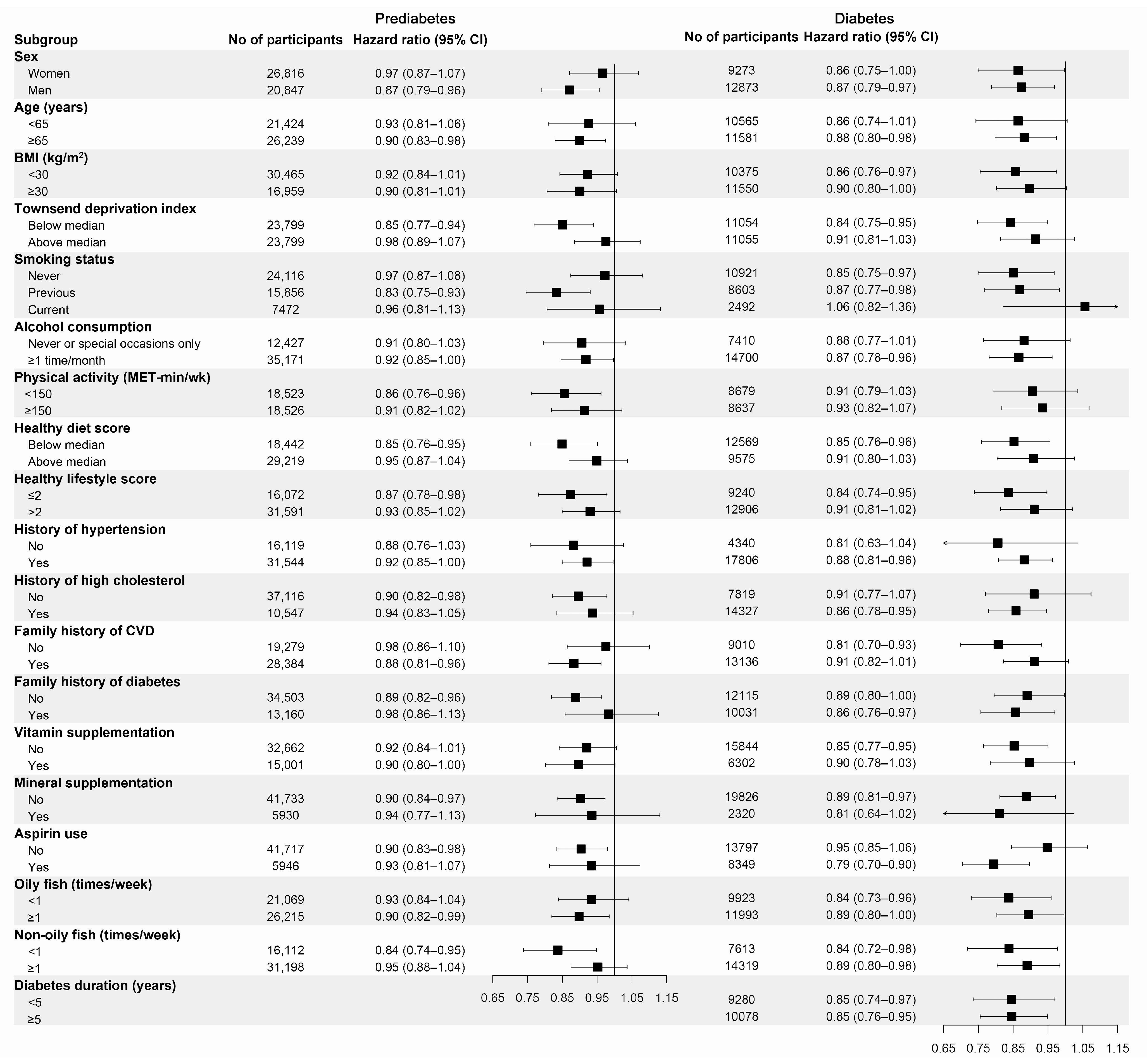
3.4. Subgroup and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Welsh, C.; Welsh, P.; Celis-Morales, C.A.; Mark, P.B.; Mackay, D.; Ghouri, N.; Ho, F.K.; Ferguson, L.D.; Brown, R.; Lewsey, J.; et al. Glycated hemoglobin, prediabetes, and the links to cardiovascular disease: Data from UK Biobank. Diabetes Care 2020, 43, 440–445. [Google Scholar] [CrossRef]
- Hu, H.; Mizoue, T.; Sasaki, N.; Ogasawara, T.; Tomita, K.; Nagahama, S.; Hori, A.; Nishihara, A.; Imai, T.; Yamamoto, M.; et al. Prediabetes and cardiovascular disease risk: A nested case-control study. Atherosclerosis 2018, 278, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Imamura, F.; Aslibekyan, S.; Marklund, M.; Virtanen, J.K.; Wennberg, M.; Yakoob, M.Y.; Chiuve, S.E.; Dela Cruz, L.; Frazier-Wood, A.C.; et al. ω-3 polyunsaturated fatty acid biomarkers and coronary heart disease: Pooling project of 19 cohort studies. JAMA Intern. Med. 2016, 176, 1155–1166. [Google Scholar] [CrossRef]
- Rimm, E.B.; Appel, L.J.; Chiuve, S.E.; Djoussé, L.; Engler, M.B.; Kris-Etherton, P.M.; Mozaffarian, D.; Siscovick, D.S.; Lichtenstein, A.H. Seafood long-chain n-3 polyunsaturated fatty acids and cardiovascular disease: A science advisory from the American Heart Association. Circulation 2018, 138, e35–e47. [Google Scholar] [CrossRef] [PubMed]
- Siscovick, D.S.; Barringer, T.A.; Fretts, A.M.; Wu, J.H.; Lichtenstein, A.H.; Costello, R.B.; Kris-Etherton, P.M.; Jacobson, T.A.; Engler, M.B.; Alger, H.M.; et al. Omega-3 polyunsaturated fatty acid (fish oil) supplementation and the prevention of clinical cardiovascular disease: A science advisory from the American Heart Association. Circulation 2017, 135, e867–e884. [Google Scholar] [CrossRef]
- Bosch, J.; Gerstein, H.C.; Dagenais, G.R.; Díaz, R.; Dyal, L.; Jung, H.; Maggiono, A.P.; Probstfield, J.; Ramachandran, A.; Riddle, M.C.; et al. N-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N. Engl. J. Med. 2012, 367, 309–318. [Google Scholar] [CrossRef]
- Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; Cox, J.; et al. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Sherman, R.E.; Anderson, S.A.; Dal Pan, G.J.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.W.; Robb, M.A.; et al. Real-world evidence—What is it and what can it tell us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef]
- Hu, F.B.; Cho, E.; Rexrode, K.M.; Albert, C.M.; Manson, J.E. Fish and long-chain omega-3 fatty acid intake and risk of coronary heart disease and total mortality in diabetic women. Circulation 2003, 107, 1852–1857. [Google Scholar] [CrossRef] [PubMed]
- Strand, E.; Pedersen, E.R.; Svingen, G.F.; Schartum-Hansen, H.; Rebnord, E.W.; Bjørndal, B.; Seifert, R.; Bohov, P.; Meyer, K.; Hiltunen, J.K.; et al. Dietary intake of n-3 long-chain polyunsaturated fatty acids and risk of myocardial infarction in coronary artery disease patients with or without diabetes mellitus: A prospective cohort study. BMC Med. 2013, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; He, L.; Luo, Y.; Zhang, G.; Cheng, X.; Bai, Y. Use of fish oil and mortality of patients with cardiometabolic multimorbidity: A prospective study of UK biobank. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2751–2759. [Google Scholar] [CrossRef]
- Ma, T.; He, L.; Luo, Y.; Li, J.; Zhang, G.; Cheng, X.; Bai, Y. Associations of baseline use of fish oil with progression of cardiometabolic multimorbidity and mortality among patients with hypertension: A prospective study of UK Biobank. Eur. J. Nutr. 2022, 61, 3461–3470. [Google Scholar] [CrossRef]
- Li, Z.H.; Zhong, W.F.; Liu, S.; Kraus, V.B.; Zhang, Y.J.; Gao, X.; Lv, Y.B.; Shen, D.; Zhang, X.R.; Zhang, P.D.; et al. Associations of habitual fish oil supplementation with cardiovascular outcomes and all cause mortality: Evidence from a large population based cohort study. BMJ 2020, 368, m456. [Google Scholar] [CrossRef]
- Eastwood, S.V.; Mathur, R.; Atkinson, M.; Brophy, S.; Sudlow, C.; Flaig, R.; de Lusignan, S.; Allen, N.; Chaturvedi, N. Algorithms for the capture and adjudication of prevalent and incident diabetes in UK Biobank. PLoS ONE 2016, 11, e0162388. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Townsend, P. Deprivation. J. Soc. Policy 2009, 16, 125–146. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Said, M.A.; Verweij, N.; van der Harst, P. Associations of Combined Genetic and Lifestyle Risks with Incident Cardiovascular Disease and Diabetes in the UK Biobank Study. JAMA Cardiol. 2018, 3, 693–702. [Google Scholar] [CrossRef]
- UK Biobank. Biomarker Assay Quality Procedures: Approaches Used to Minimise Systematic and Random Errors (and the Wider Epidemiological Implications). Available online: https://biobank.ctsu.ox.ac.uk/showcase/ukb/docs/biomarker_issues.pdf (accessed on 2 April 2023).
- Bartlett, M.S. The use of transformations. Biometrics 1947, 3, 39–52. [Google Scholar] [CrossRef] [PubMed]
- UK Biobank. Nightingale Health Metabolic Biomarkers: Phase 1 Release. Available online: https://biobank.ctsu.ox.ac.uk/crystal/refer.cgi?id=3000 (accessed on 2 April 2023).
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Li, X.; Zhou, T.; Sun, D.; Liang, Z.; Li, Y.; Heianza, Y.; Qi, L. Glucosamine use, inflammation, and genetic susceptibility, and incidence of type 2 diabetes: A prospective study in UK Biobank. Diabetes Care 2020, 43, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.R.; Zhao, S.D.; Parast, L. Estimation of the proportion of treatment effect explained by a high-dimensional surrogate. Stat. Med. 2022, 41, 2227–2246. [Google Scholar] [CrossRef]
- Alexander, D.D.; Miller, P.E.; Van Elswyk, M.E.; Kuratko, C.N.; Bylsma, L.C. A meta-analysis of randomized controlled trials and prospective cohort studies of eicosapentaenoic and docosahexaenoic long-chain omega-3 fatty acids and coronary heart disease risk. Mayo Clin. Proc. 2017, 92, 15–29. [Google Scholar] [CrossRef]
- Jiao, J.; Liu, G.; Shin, H.J.; Hu, F.B.; Rimm, E.B.; Rexrode, K.M.; Manson, J.E.; Zong, G.; Sun, Q. Dietary fats and mortality among patients with type 2 diabetes: Analysis in two population based cohort studies. BMJ 2019, 366, l4009. [Google Scholar] [CrossRef]
- Jayedi, A.; Soltani, S.; Abdolshahi, A.; Shab-Bidar, S. Fish consumption and the risk of cardiovascular disease and mortality in patients with type 2 diabetes: A dose-response meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2021, 61, 1640–1650. [Google Scholar] [CrossRef]
- Goel, A.; Pothineni, N.V.; Singhal, M.; Paydak, H.; Saldeen, T.; Mehta, J.L. Fish, fish oils and cardioprotection: Promise or fish tale? Int. J. Mol. Sci. 2018, 19, 3703. [Google Scholar] [CrossRef]
- Harris, K.; Oshima, M.; Sattar, N.; Würtz, P.; Jun, M.; Welsh, P.; Hamet, P.; Harrap, S.; Poulter, N.; Chalmers, J.; et al. Plasma fatty acids and the risk of vascular disease and mortality outcomes in individuals with type 2 diabetes: Results from the ADVANCE study. Diabetologia 2020, 63, 1637–1647. [Google Scholar] [CrossRef]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020, 3, Cd003177. [Google Scholar] [CrossRef]
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine omega-3 supplementation and cardiovascular disease: An updated meta-analysis of 13 randomized controlled trials involving 127 477 participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, S.; Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Suppressive effect of EPA on the incidence of coronary events in hypercholesterolemia with impaired glucose metabolism: Sub-analysis of the Japan EPA Lipid Intervention Study (JELIS). Atherosclerosis 2009, 206, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Lincoff, A.M.; Garcia, M.; Bash, D.; Ballantyne, C.M.; Barter, P.J.; Davidson, M.H.; Kastelein, J.J.P.; Koenig, W.; McGuire, D.K.; et al. Effect of high-dose omega-3 fatty acids vs. corn oil on major adverse cardiovascular events in patients at high cardiovascular risk: The STRENGTH randomized clinical trial. JAMA 2020, 324, 2268–2280. [Google Scholar] [CrossRef]
- Bernasconi, A.A.; Wiest, M.M.; Lavie, C.J.; Milani, R.V.; Laukkanen, J.A. Effect of omega-3 dosage on cardiovascular outcomes: An updated meta-analysis and meta-regression of interventional trials. Mayo Clin. Proc. 2021, 96, 304–313. [Google Scholar] [CrossRef]
- George, E.S.; Marshall, S.; Mayr, H.L.; Trakman, G.L.; Tatucu-Babet, O.A.; Lassemillante, A.M.; Bramley, A.; Reddy, A.J.; Forsyth, A.; Tierney, A.C.; et al. The effect of high-polyphenol extra virgin olive oil on cardiovascular risk factors: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2019, 59, 2772–2795. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Liu, G.; Li, Y.; Sampson, L.; Manson, J.E.; Salas-Salvadó, J.; Martínez-González, M.A.; Stampfer, M.J.; Willett, W.C.; Sun, Q.; et al. Olive oil consumption and cardiovascular risk in U.S. adults. J. Am. Coll. Cardiol. 2020, 75, 1729–1739. [Google Scholar] [CrossRef]
- Do Vale, F.M.; Diógenes, M.J.; Barbacena, H.A. Controversies about the cardiovascular effects of OM3FA. Did inappropriate placebos skew clinical trial results? Pharmacol. Res. 2021, 164, 105368. [Google Scholar] [CrossRef]
- Meeting of the Endocrinologic and Metabolic Drugs Advisory Committee Meeting Announcement. Available online: https://www.fda.gov/advisory-committees/november-14-2019-meeting-endocrinologic-and-metabolic-drugs-advisory-committee-meeting-announcement (accessed on 10 October 2020).
- Vistisen, D.; Witte, D.R.; Brunner, E.J.; Kivimäki, M.; Tabák, A.; Jørgensen, M.E.; Færch, K. Risk of cardiovascular disease and death in individuals with prediabetes defined by different criteria: The Whitehall II study. Diabetes Care 2018, 41, 899–906. [Google Scholar] [CrossRef]
- O’Mahoney, L.L.; Matu, J.; Price, O.J.; Birch, K.M.; Ajjan, R.A.; Farrar, D.; Tapp, R.; West, D.J.; Deighton, K.; Campbell, M.D. Omega-3 polyunsaturated fatty acids favourably modulate cardiometabolic biomarkers in type 2 diabetes: A meta-analysis and meta-regression of randomized controlled trials. Cardiovasc. Diabetol. 2018, 17, 98. [Google Scholar] [CrossRef]
- Gao, C.; Liu, Y.; Gan, Y.; Bao, W.; Peng, X.; Xing, Q.; Gao, H.; Lai, J.; Liu, L.; Wang, Z.; et al. Effects of fish oil supplementation on glucose control and lipid levels among patients with type 2 diabetes mellitus: A Meta-analysis of randomized controlled trials. Lipids Health Dis. 2020, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- De Luis, D.A.; Conde, R.; Aller, R.; Izaola, O.; González Sagrado, M.; Perez Castrillón, J.L.; Dueñas, A.; Romero, E. Effect of omega-3 fatty acids on cardiovascular risk factors in patients with type 2 diabetes mellitus and hypertriglyceridemia: An open study. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 51–55. [Google Scholar]
- Khalili, L.; Valdes-Ramos, R.; Harbige, L.S. Effect of n-3 (omega-3) polyunsaturated fatty acid supplementation on metabolic and inflammatory biomarkers and body weight in patients with type 2 diabetes mellitus: A systematic review and meta-analysis of RCTs. Metabolites 2021, 11, 742. [Google Scholar] [CrossRef]
- Li, K.; Huang, T.; Zheng, J.; Wu, K.; Li, D. Effect of marine-derived n-3 polyunsaturated fatty acids on C-reactive protein, interleukin 6 and tumor necrosis factor α: A meta-analysis. PLoS ONE 2014, 9, e88103. [Google Scholar] [CrossRef]
- Adkins, Y.; Kelley, D.S. Mechanisms underlying the cardioprotective effects of omega-3 polyunsaturated fatty acids. J. Nutr. Biochem. 2010, 21, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Jump, D.B. Dietary polyunsaturated fatty acids and regulation of gene transcription. Curr. Opin. Lipidol. 2002, 13, 155–164. [Google Scholar] [CrossRef]
- Hartweg, J.; Farmer, A.J.; Perera, R.; Holman, R.R.; Neil, H.A. Meta-analysis of the effects of n-3 polyunsaturated fatty acids on lipoproteins and other emerging lipid cardiovascular risk markers in patients with type 2 diabetes. Diabetologia 2007, 50, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Balling, M.; Afzal, S.; Varbo, A.; Langsted, A.; Davey Smith, G.; Nordestgaard, B.G. VLDL cholesterol accounts for one-half of the risk of myocardial infarction associated with apoB-containing lipoproteins. J. Am. Coll. Cardiol. 2020, 76, 2725–2735. [Google Scholar] [CrossRef]
- Dogay Us, G.; Mushtaq, S. N-3 fatty acid supplementation mediates lipid profile, including small dense LDL, when combined with statins: A randomized double blind placebo controlled trial. Lipids Health Dis. 2022, 21, 84. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | Prediabetes | Diabetes | ||||||
|---|---|---|---|---|---|---|---|---|
| Overall | Fish Oil Non-Users | Fish Oil Users | p-Value | Overall | Fish Oil Non-Users | Fish Oil Users | p-Value | |
| (n = 47,663) | (n = 31,727) | (n = 15,936) | (n = 22,146) | (n = 15,836) | (n = 6310) | |||
| Male/n (%) | 43.7 | 45.7 | 39.8 | <0.001 | 58.1 | 58.6 | 57.0 | 0.038 |
| Age (year) | 59.0 ± 7.1 | 58.1 ± 7.4 | 60.7 ± 6.3 | <0.001 | 58.4 ± 7.6 | 57.7 ± 7.7 | 60.1 ± 6.9 | <0.001 |
| Race/n (%) | <0.001 | <0.001 | ||||||
| White | 89.2 | 88.6 | 90.6 | 85.6 | 85.0 | 87.3 | ||
| Nonwhite/mixed | 10.3 | 11.0 | 9.0 | 13.8 | 14.5 | 12.3 | ||
| BMI (kg/m2) | 28.9 ± 5.3 | 29.1 ± 5.4 | 28.5 ± 5.0 | <0.001 | 31.2 ± 5.9 | 31.4 ± 6.0 | 30.9 ± 5.7 | <0.001 |
| Household income (GBP) | <0.001 | 0.016 | ||||||
| <18,000 * | 24.2 | 23.9 | 24.6 | 27.5 | 27.6 | 27.1 | ||
| 18,000 to 30,999 | 23.6 | 22.9 | 25.1 | 23.0 | 22.6 | 24.1 | ||
| 31,000 to 51,999 | 20.0 | 20.4 | 19.2 | 18.1 | 17.9 | 18.5 | ||
| 52,000 to 100,000 | 12.1 | 12.8 | 10.6 | 11.5 | 11.8 | 10.8 | ||
| >100,000 | 2.8 | 3.1 | 2.3 | 2.5 | 2.7 | 2.2 | ||
| Townsend deprivation index | −1.0 ± 3.2 | −0.9 ± 3.3 | −1.3 ± 3.1 | <0.001 | −0.5 ± 3.4 | −0.4 ± 3.4 | −0.8 ± 3.3 | <0.001 |
| Smoking status/n (%) | <0.001 | <0.001 | ||||||
| Never | 50.6 | 50.4 | 51.1 | 49.3 | 50.3 | 47.0 | ||
| Previous | 33.3 | 31.7 | 36.4 | 38.9 | 37.2 | 42.9 | ||
| Current | 15.7 | 17.5 | 12.2 | 11.3 | 12.0 | 9.3 | ||
| Alcohol consumption/n (%) | <0.001 | <0.001 | ||||||
| <1 times/week | 38.5 | 39.6 | 36.1 | 45.9 | 47.4 | 42.0 | ||
| 1 or 2 times/week | 25.2 | 24.9 | 25.6 | 23.4 | 23.0 | 24.5 | ||
| 3 or 4 times/week | 19.1 | 18.4 | 20.4 | 15.8 | 15.1 | 17.4 | ||
| ≥5 times/week | 17.2 | 16.9 | 17.8 | 14.8 | 14.3 | 16.0 | ||
| Physical activity (MET-h/wk) | 44.8 ± 47.1 | 43.3 ± 46.9 | 47.6 ± 47.3 | <0.001 | 38.1 ± 43.3 | 36.3 ± 42.6 | 42.6 ± 44.8 | <0.001 |
| History of hypertension/n (%) | 66.2 | 65.5 | 67.6 | <0.001 | 80.4 | 80.0 | 81.5 | 0.008 |
| History of high cholesterol/n (%) | 22.1 | 21.0 | 24.4 | <0.001 | 64.7 | 63.9 | 66.6 | <0.001 |
| Family history of CVD/n (%) | 59.6 | 58.9 | 60.8 | <0.001 | 59.3 | 58.8 | 60.6 | 0.018 |
| Family history of diabetes/n (%) | 27.6 | 27.9 | 27.0 | 0.032 | 45.3 | 45.6 | 44.6 | 0.197 |
| Aspirin use/n (%) | 12.5 | 11.3 | 14.8 | <0.001 | 37.7 | 35.9 | 42.2 | <0.001 |
| Lipid-lowering drug/n (%) | 21.0 | 20.1 | 22.9 | <0.001 | 65.5 | 64.9 | 66.9 | 0.006 |
| Glucose-lowering medication/n (%) | ||||||||
| Oral | - | - | - | - | 50.6 | 51.2 | 49.3 | 0.010 |
| Insulin | - | - | - | - | 17.2 | 17.8 | 15.5 | <0.001 |
| Vitamin supplementation/n (%) | 31.5 | 19.6 | 55.2 | <0.001 | 28.5 | 18.2 | 54.1 | <0.001 |
| Mineral supplementation/n (%) | 12.4 | 8.3 | 20.7 | <0.001 | 10.5 | 7.7 | 17.5 | <0.001 |
| Dietary consumption | ||||||||
| Oily fish (times/week) | <0.001 | <0.001 | ||||||
| <1 | 44.2 | 48.3 | 36.1 | 44.8 | 48.3 | 36.0 | ||
| 1 | 37.1 | 35.2 | 40.9 | 34.9 | 33.3 | 38.9 | ||
| ≥2 | 17.9 | 15.6 | 22.5 | 19.3 | 17.2 | 24.4 | ||
| Non-oily fish (times/week) | <0.001 | <0.001 | ||||||
| <1 | 33.8 | 36.3 | 28.9 | 34.4 | 36.3 | 29.5 | ||
| 1 | 49.4 | 47.9 | 52.4 | 47.8 | 46.5 | 51.3 | ||
| ≥2 | 16.0 | 15.0 | 18.2 | 16.8 | 16.2 | 18.5 | ||
| Poultry (times/week) | <0.001 | 0.026 | ||||||
| <2 | 53.5 | 53.7 | 53.1 | 51.1 | 51.5 | 50.2 | ||
| 2–4 | 44.0 | 43.6 | 44.8 | 45.4 | 44.8 | 46.7 | ||
| >4 | 2.3 | 2.5 | 1.9 | 3.1 | 3.2 | 2.8 | ||
| Processed meat (times/week) | <0.001 | <0.001 | ||||||
| <1 | 37.9 | 36.7 | 40.2 | 33.4 | 32.8 | 35.1 | ||
| 1 | 29.0 | 28.6 | 29.7 | 28.9 | 28.7 | 29.3 | ||
| ≥2 | 32.8 | 34.3 | 29.8 | 37.2 | 38.1 | 35.1 | ||
| Unprocessed red meat (times/week) | <0.001 | 0.563 | ||||||
| <2.0 | 47.8 | 47.5 | 48.4 | 45.2 | 45.4 | 44.8 | ||
| 2.0–4.0 | 42.6 | 42.5 | 42.9 | 43.8 | 43.6 | 44.5 | ||
| >4.0 | 9.4 | 9.8 | 8.6 | 10.7 | 10.8 | 10.4 | ||
| Vegetables (servings/day) | <0.001 | <0.001 | ||||||
| <1.0 | 18.8 | 20.7 | 15.1 | 19.7 | 21.4 | 15.6 | ||
| 1.0–2.9 | 71.6 | 69.8 | 75.3 | 69.1 | 67.9 | 72.1 | ||
| ≥3.0 | 8.7 | 8.6 | 9.0 | 10.1 | 9.6 | 11.3 | ||
| Fruits (servings/day) | <0.001 | <0.001 | ||||||
| <2.0 | 36.7 | 40.3 | 29.5 | 30.7 | 32.8 | 25.4 | ||
| 2.0–3.9 | 46.2 | 44.4 | 49.8 | 48.1 | 47.2 | 50.3 | ||
| ≥4.0 | 16.8 | 14.9 | 20.5 | 20.8 | 19.6 | 24.0 | ||
| Whole grains (servings/day) | <0.001 | <0.001 | ||||||
| <1.0 | 46.3 | 50.0 | 38.9 | 43.9 | 47.0 | 36.1 | ||
| 1.0–2.9 | 40.6 | 37.6 | 46.6 | 39.3 | 37.2 | 44.6 | ||
| ≥3.0 | 12.0 | 11.3 | 13.5 | 15.7 | 14.7 | 18.3 | ||
| Refined grains (servings/day) | <0.001 | <0.001 | ||||||
| <1.0 | 54.5 | 51.7 | 60.0 | 53.3 | 51.1 | 58.9 | ||
| 1.0–2.9 | 33.5 | 35.3 | 30.1 | 33.3 | 34.4 | 30.6 | ||
| ≥3.0 | 10.9 | 11.9 | 8.9 | 12.3 | 13.3 | 9.6 | ||
| Cheese (pieces/day) | 0.013 | 0.101 | ||||||
| <2 | 41.3 | 41.1 | 41.7 | 46.5 | 47.0 | 45.5 | ||
| 2–4 | 43.7 | 43.6 | 44.1 | 39.4 | 38.9 | 40.6 | ||
| >4 | 12.3 | 12.7 | 11.6 | 10.0 | 10.1 | 9.7 | ||
| Coffee (cups/day) | <0.001 | <0.001 | ||||||
| <1 | 30.4 | 31.2 | 28.9 | 31.4 | 32.1 | 29.5 | ||
| 1–2 | 37.8 | 35.8 | 41.8 | 35.6 | 34.1 | 39.3 | ||
| ≥3 | 31.5 | 32.6 | 29.1 | 32.4 | 33.2 | 30.6 | ||
| Sugar-sweetened beverages consumer/n (%) | 83.3 | 84.5 | 81.0 | <0.001 | 57.3 | 58.5 | 54.2 | <0.001 |
| Healthy diet score | 3.0 ± 1.4 | 2.8 ± 1.4 | 3.2 ± 1.4 | <0.001 | 3.3 ± 1.5 | 3.2 ± 1.5 | 3.5 ± 1.5 | <0.001 |
| Diabetes duration (year) | 0.126 | |||||||
| <5 | - | - | - | - | 41.9 | 41.7 | 42.4 | |
| 5–10 | - | - | - | 22.4 | 22.2 | 23.0 | ||
| ≥10 | - | - | - | 23.1 | 23.3 | 22.7 | ||
| Fish Oil Supplementation | p-Value | ||
|---|---|---|---|
| Non-Users | Users | ||
| Prediabetes | |||
| n (%) | 31,727 (66.6) | 15,936 (33.4) | |
| Cases of CHD (%) | 2871 (9.1) | 1433 (9.0) | |
| Person-years | 351,221 | 176,993 | |
| Model 1 | 1 [Ref.] | 0.91 (0.85–0.97) | 0.004 |
| Model 2 | 1 [Ref.] | 0.91 (0.85–0.97) | 0.006 |
| Model 3 | 1 [Ref.] | 0.92 (0.86–0.99) | 0.018 |
| Model 4 | 1 [Ref.] | 0.91 (0.85–0.98) | 0.009 |
| Diabetes | |||
| n (%) | 15,836 (71.5) | 6310 (28.5) | |
| Case of CHD (%) | 2393 (15.1) | 901 (14.3) | |
| Person-years | 167,867 | 67,194 | |
| Model 1 | 1 [Ref.] | 0.85 (0.79–0.92) | <0.001 |
| Model 2 | 1 [Ref.] | 0.87 (0.80–0.95) | 0.001 |
| Model 3 | 1 [Ref.] | 0.88 (0.81–0.96) | 0.003 |
| Model 4 | 1 [Ref.] | 0.87 (0.80–0.95) | 0.001 |
| Mediator | Prediabetes | Diabetes | ||||
|---|---|---|---|---|---|---|
| Cases/N | Proportion (%) of Effect Due to Mediation (95% CI) | p-Value | Cases/N | Proportion (%) of Effect Due to Mediation (95% CI) | p-Value | |
| Glucose | 3770/41,648 | NA | NA | 2851/19,032 | NA | NA |
| HbA1c | 4304/47,663 | NA | NA | 3099/20,726 | 2.5% (0.7–8.6%) | 0.034 |
| CRP * | 4085/45,309 | 5.9% (1.9–16.9%) | 0.003 | 3097/20,714 | 2.1% (0.3–11.6%) | 0.125 |
| TG | 4095/45,391 | NA | NA | 3103/20,740 | NA | NA |
| TC | 4096/45,426 | NA | NA | 3109/20,775 | NA | NA |
| VLDL-C | 992/11,366 | NA | NA | 796/5226 | 6.1% (1.5–22.5%) | 0.033 |
| Large VLDL-C | 992/11,366 | NA | NA | 796/5226 | 3.7% (0.7–18.3%) | 0.084 |
| Medium VLDL-C | 992/11,366 | NA | NA | 796/5226 | 3.9% (0.7–18.9%) | 0.083 |
| Small VLDL-C | 992/11,366 | NA | NA | 796/5226 | 5.3% (1.1–21.9%) | 0.058 |
| Very large VLDL-C | 992/11,366 | NA | NA | 796/5226 | 4.9% (1.1–19.4%) | 0.044 |
| Very small VLDL-C | 992/11,366 | NA | NA | 796/5226 | 3.8% (0.6–20.6%) | 0.111 |
| LDL-C | 4091/45,336 | NA | NA | 3101/20,707 | NA | NA |
| Large LDL-C | 992/11,366 | NA | NA | 796/5226 | 2.6% (0.4–14.7%) | 0.104 |
| Medium LDL-C | 992/11,366 | NA | NA | 796/5226 | 3.9% (0.8–17.2%) | 0.058 |
| Small LDL-C | 992/11,366 | NA | NA | 796/5226 | 4.9% (1.1–19.2%) | 0.039 |
| IDL-C | 992/11,366 | NA | NA | 796/5226 | 2.3% (0.3–15.4%) | 0.135 |
| HDL-C | 3773/41,665 | 3.8% (0.9–15.6%) | 0.033 | 2852/19,039 | 3.1% (1.0–9.6%) | 0.018 |
| Large HDL-C | 992/11,366 | NA | NA | 796/5226 | NA | NA |
| Medium HDL-C | 992/11,366 | NA | NA | 796/5226 | 1.6% (0.2–14.9%) | 0.186 |
| Small HDL-C | 992/11,366 | NA | NA | 796/5226 | NA | NA |
| Very large HDL-C | 992/11,366 | NA | NA | 796/5226 | NA | NA |
| Apo A | 3760/41,516 | 2.8% (0.4–17.0%) | 0.116 | 2844/18,996 | 3.1% (1.0–9.1%) | 0.013 |
| Apo B | 4070/45,148 | NA | NA | 3084/20,544 | NA | NA |
| IGF-1 | 4077/45,173 | 3.2% (1.0–10.3%) | 0.013 | 3092/20,644 | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Li, Y.; Wan, X.; Zhuang, P.; Wu, Y.; Zhang, L.; Ao, Y.; Yao, J.; Zhang, Y.; Jiao, J. Association of Fish Oil Supplementation with Risk of Coronary Heart Disease in Individuals with Diabetes and Prediabetes: A Prospective Study in the UK Biobank. Nutrients 2023, 15, 3176. https://doi.org/10.3390/nu15143176
Liu X, Li Y, Wan X, Zhuang P, Wu Y, Zhang L, Ao Y, Yao J, Zhang Y, Jiao J. Association of Fish Oil Supplementation with Risk of Coronary Heart Disease in Individuals with Diabetes and Prediabetes: A Prospective Study in the UK Biobank. Nutrients. 2023; 15(14):3176. https://doi.org/10.3390/nu15143176
Chicago/Turabian StyleLiu, Xiaohui, Yin Li, Xuzhi Wan, Pan Zhuang, Yuqi Wu, Lange Zhang, Yang Ao, Jianxin Yao, Yu Zhang, and Jingjing Jiao. 2023. "Association of Fish Oil Supplementation with Risk of Coronary Heart Disease in Individuals with Diabetes and Prediabetes: A Prospective Study in the UK Biobank" Nutrients 15, no. 14: 3176. https://doi.org/10.3390/nu15143176
APA StyleLiu, X., Li, Y., Wan, X., Zhuang, P., Wu, Y., Zhang, L., Ao, Y., Yao, J., Zhang, Y., & Jiao, J. (2023). Association of Fish Oil Supplementation with Risk of Coronary Heart Disease in Individuals with Diabetes and Prediabetes: A Prospective Study in the UK Biobank. Nutrients, 15(14), 3176. https://doi.org/10.3390/nu15143176