
The Association of Food Groups and Consumption Time with Hyperuricemia: The U.S. National Health and Nutrition Examination Survey, 2005–2018

 ,
,
Abstract
1. Introduction
2. Materials and Methods
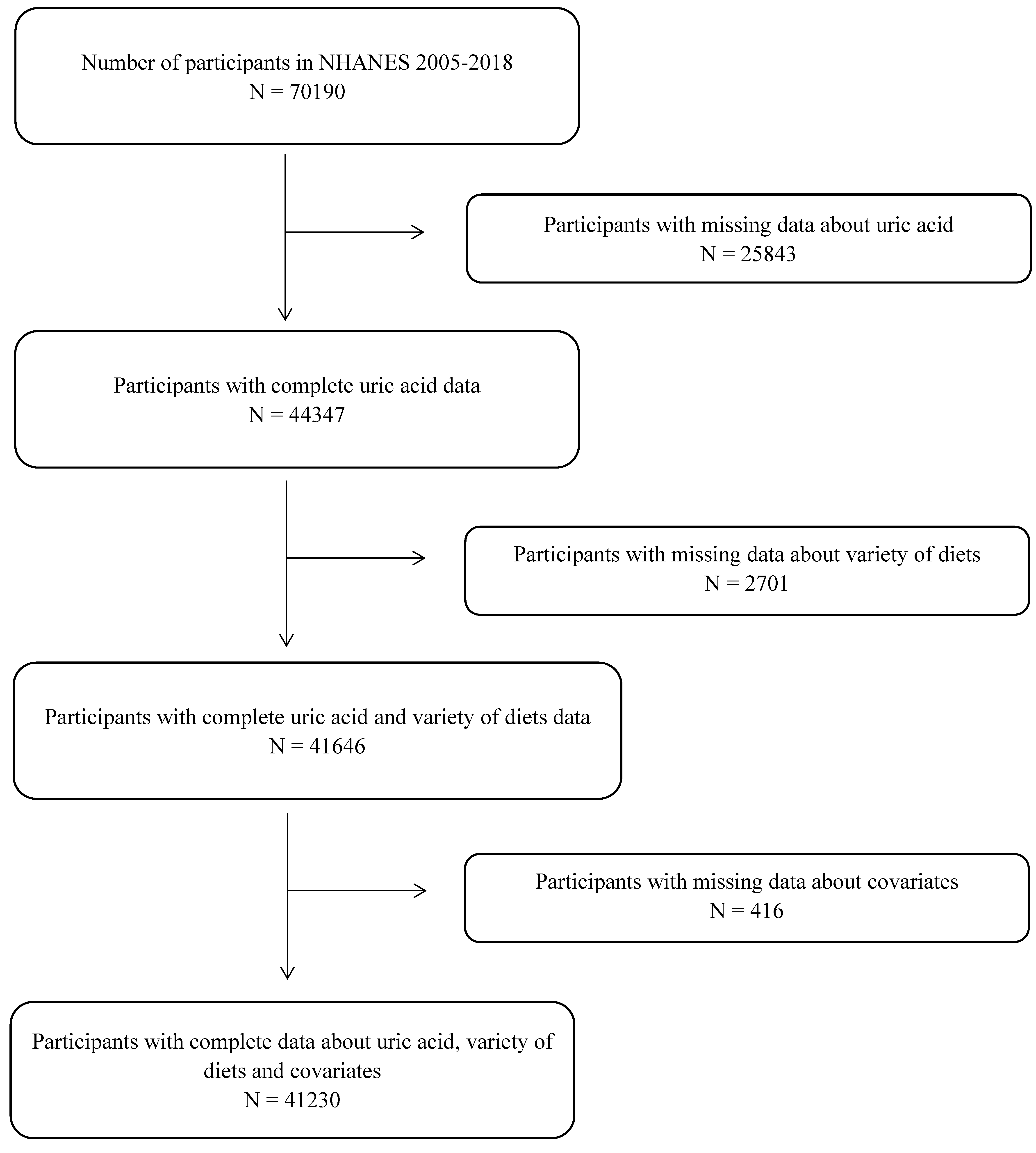
2.1. Data Source and Study Population
2.2. Dietary Assessment
2.3. Main Exposure
2.4. Outcome Variable and Covariates
2.5. Statistical Analysis
2.6. Sensitivity Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Characteristics of the Food Group
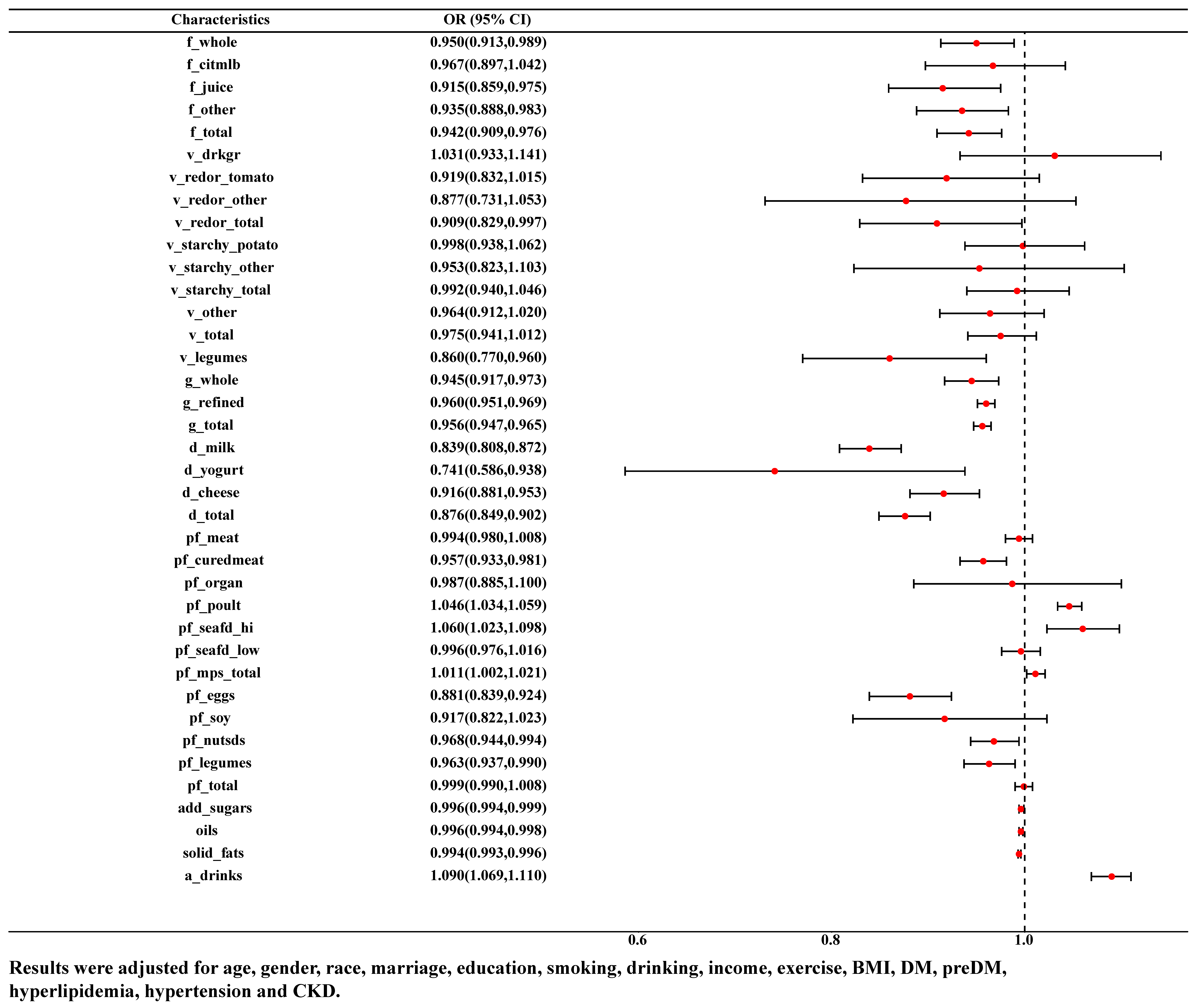
3.3. Association between Food Groups and HUA
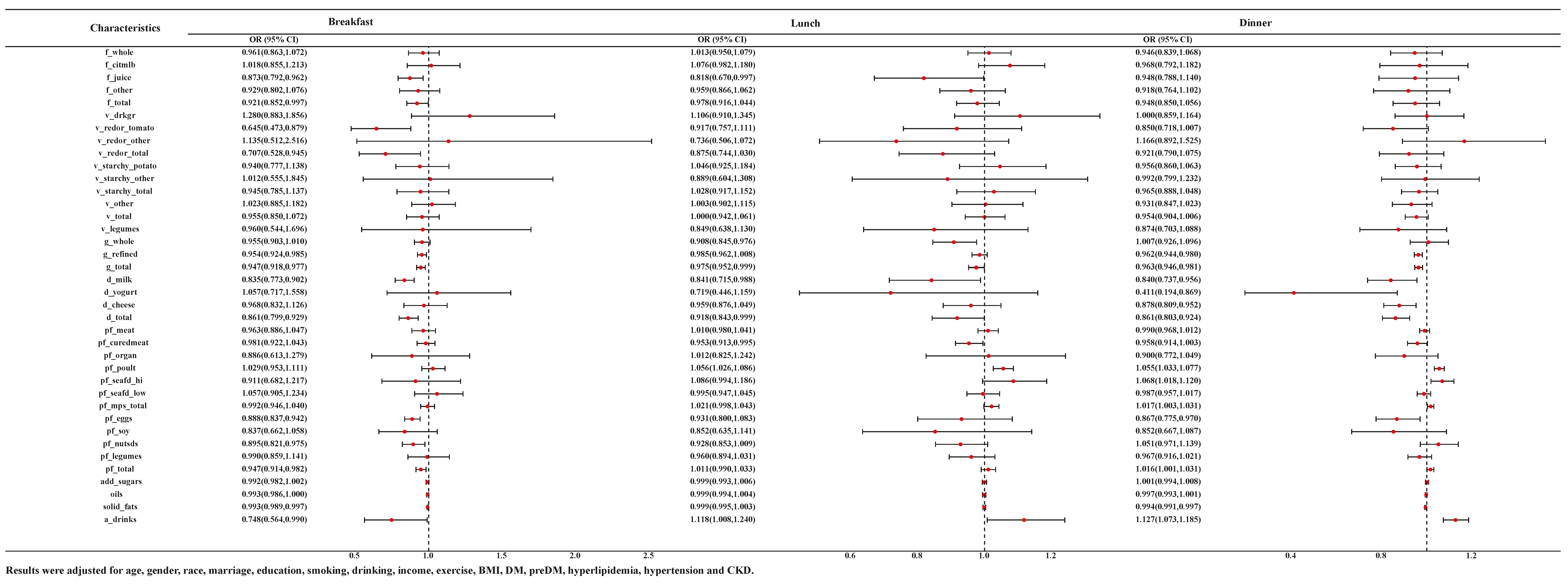
3.4. Association between Food Intake Time and HUA
3.5. Sensitivity Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Z.; Gao, L.; Zhong, X.; Feng, G.; Huang, F.; Xia, S. Association of Visceral Fat Area and Hyperuricemia in Non-Obese US Adults: A Cross-Sectional Study. Nutrients 2022, 14, 3992. [Google Scholar] [CrossRef]
- Chen-Xu, M.; Yokose, C.; Rai, S.K.; Pillinger, M.H.; Choi, H.K. Contemporary Prevalence of Gout and Hyperuricemia in the United States and Decadal Trends: The National Health and Nutrition Examination Survey, 2007–2016. Arthritis Rheumatol. 2019, 71, 991–999. [Google Scholar] [CrossRef]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef]
- Liu, R.; Han, C.; Wu, D.; Xia, X.; Gu, J.; Guan, H.; Shan, Z.; Teng, W. Prevalence of Hyperuricemia and Gout in Mainland China from 2000 to 2014: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2015, 2015, 762820. [Google Scholar] [CrossRef]
- Zhong, L.; Liu, S.; Qiu, X.; Zeng, X.; Su, L.; Huang, D.; Guo, X.; Liang, J.; Yang, Y.; Tang, X.; et al. High Prevalence of Hyperuricemia and Associated Factors among Zhuang Adults: A Cross-Sectional Study Based on the Ethnic Minority Population Cohort in the Southwestern China. Int. J. Environ. Res. Public Health 2022, 19, 16040. [Google Scholar] [CrossRef]
- Zhou, M.; Huang, X.; Li, R.; Zhang, Z.; Zhang, L.; Gao, X.; Yang, H.; Ma, Y. Association of dietary patterns with blood uric acid concentration and hyperuricemia in northern Chinese adults. Nutr. J. 2022, 21, 42. [Google Scholar] [CrossRef]
- Song, P.; Wang, H.; Xia, W.; Chang, X.; Wang, M.; An, L. Prevalence and correlates of hyperuricemia in the middle-aged and older adults in China. Sci. Rep. 2018, 8, 4314. [Google Scholar] [CrossRef]
- Ting, K.; Gill, T.K.; Keen, H.; Tucker, G.R.; Hill, C.L. Prevalence and associations of gout and hyperuricaemia: Results from an Australian population-based study. Intern. Med. J. 2016, 46, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; McCormick, N.; Lu, N.; Rai, S.K.; Yokose, C.; Zhang, Y. Population Impact Attributable to Modifiable Risk Factors for Hyperuricemia. Arthritis Rheumatol. 2020, 72, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Hong, F.; Zheng, A.; Xu, P.; Wang, J.; Xue, T.; Dai, S.; Pan, S.; Guo, Y.; Xie, X.; Li, L.; et al. High-Protein Diet Induces Hyperuricemia in a New Animal Model for Studying Human Gout. Int. J. Mol. Sci. 2020, 21, 2147. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chen, S.; Zhao, J.; Liang, J.; Gao, X.; Gao, Q.; He, S.; Wang, T. Association between nutrient patterns and hyperuricemia: Mediation analysis involving obesity indicators in the NHANES. BMC Public. Health 2022, 22, 1981. [Google Scholar] [CrossRef]
- Jiang, W.; Song, Q.; Zhang, J.; Chen, Y.; Jiang, H.; Long, Y.; Li, Y.; Han, T.; Sun, H.; Wei, W. The Association of Consumption Time for Food With Cardiovascular Disease and All-Cause Mortality Among Diabetic Patients. J. Clin. Endocrinol. Metab. 2022, 107, e3066–e3075. [Google Scholar] [CrossRef]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns during Pregnancy Are Associated with Risk of Gestational Diabetes Mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Byers, T. Dietary assessment resource manual. J. Nutr. 1994, 124, 2245S–2317S. [Google Scholar] [CrossRef]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Ruxton, C.H.S.; Myers, M. Fruit Juices: Are They Helpful or Harmful? An Evidence Review. Nutrients 2021, 13, 1815. [Google Scholar] [CrossRef] [PubMed]
- Byrd-Bredbenner, C.; Ferruzzi, M.G.; Fulgoni, V.L., 3rd; Murray, R.; Pivonka, E.; Wallace, T.C. Satisfying America’s Fruit Gap: Summary of an Expert Roundtable on the Role of 100% Fruit Juice. J. Food Sci. 2017, 82, 1523–1534. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Lanaspa, M.A.; Johnson, R.J. The effects of fruit consumption in patients with hyperuricaemia or gout. Rheumatology 2019, 58, 1133–1141. [Google Scholar] [CrossRef]
- Vargas-Santos, A.B.; Neogi, T. Management of Gout and Hyperuricemia in CKD. Am. J. Kidney Dis. 2017, 70, 422–439. [Google Scholar] [CrossRef]
- Torralba, K.D.; De Jesus, E.; Rachabattula, S. The interplay between diet, urate transporters and the risk for gout and hyperuricemia: Current and future directions. Int. J. Rheum. Dis. 2012, 15, 499–506. [Google Scholar] [CrossRef]
- Seal, C.J.; Brownlee, I.A. Whole-grain foods and chronic disease: Evidence from epidemiological and intervention studies. Proc. Nutr. Soc. 2015, 74, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Riley, M.; Taylor, A.; Noakes, M. Meal-specific food patterns and the incidence of hyperglycemia in a Chinese adult population. Br. J. Nutr. 2017, 118, 53–59. [Google Scholar] [CrossRef]
- Aihemaitijiang, S.; Zhang, Y.; Zhang, L.; Yang, J.; Ye, C.; Halimulati, M.; Zhang, W.; Zhang, Z. The Association between Purine-Rich Food Intake and Hyperuricemia: A Cross-Sectional Study in Chinese Adult Residents. Nutrients 2020, 12, 3835. [Google Scholar] [CrossRef]
- Fukuuchi, T.; Itahashi, I.; Takayanagi, F.; Yamaoka, N.; Kaneko, K. Determination of total purine and free purine content in milk, soymilk, and enteral nutritional supplements to assist nutritional therapy for hyperuricemia and gout. Nucleosides Nucleotides Nucleic Acids 2022, 41, 1287–1295. [Google Scholar] [CrossRef]
- Min, K.B.; Min, J.Y. Increased risk for hyperuricemia in adults sensitized to cow milk allergen. Clin. Rheumatol. 2017, 36, 1407–1412. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, C.; Kishimoto, Y.; Suzuki-Sugihara, N.; Saita, E.; Usuda, M.; Wang, W.; Masuda, Y.; Kondo, K. Regular egg consumption at breakfast by Japanese woman university students improves daily nutrient intakes: Open-labeled observations. Asia Pac. J. Clin. Nutr. 2018, 27, 359–365. [Google Scholar] [CrossRef]
- Xiao, K.; Furutani, A.; Sasaki, H.; Takahashi, M.; Shibata, S. Effect of a High Protein Diet at Breakfast on Postprandial Glucose Level at Dinner Time in Healthy Adults. Nutrients 2022, 15, 85. [Google Scholar] [CrossRef]
- Major, T.J.; Topless, R.K.; Dalbeth, N.; Merriman, T.R. Evaluation of the diet wide contribution to serum urate levels: Meta-analysis of population based cohorts. BMJ 2018, 363, k3951. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, N. Dietary factors and hyperuricaemia. Curr. Pharm. Des. 2005, 11, 4133–4138. [Google Scholar] [CrossRef]
- Nieradko-Iwanicka, B. The role of alcohol consumption in pathogenesis of gout. Crit. Rev. Food Sci. Nutr. 2022, 62, 7129–7137. [Google Scholar] [CrossRef]
- Miao, Z.; Li, C.; Chen, Y.; Zhao, S.; Wang, Y.; Wang, Z.; Chen, X.; Xu, F.; Wang, F.; Sun, R.; et al. Dietary and lifestyle changes associated with high prevalence of hyperuricemia and gout in the Shandong coastal cities of Eastern China. J. Rheumatol. 2008, 35, 1859–1864. [Google Scholar]
- Zhang, T.; Rayamajhi, S.; Meng, G.; Zhang, Q.; Liu, L.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, S.; Wang, X.; et al. Dietary patterns and risk for hyperuricemia in the general population: Results from the TCLSIH cohort study. Nutrition 2022, 93, 111501. [Google Scholar] [CrossRef]
- Hak, A.E.; Curhan, G.C.; Grodstein, F.; Choi, H.K. Menopause, postmenopausal hormone use and risk of incident gout. Ann. Rheum. Dis. 2010, 69, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Fung, T.T.; Lu, N.; Keller, S.F.; Curhan, G.C.; Choi, H.K. The Dietary Approaches to Stop Hypertension (DASH) diet, Western diet, and risk of gout in men: Prospective cohort study. BMJ 2017, 357, j1794. [Google Scholar] [CrossRef] [PubMed]
- Golabek, K.D.; Regulska-Ilow, B. Dietary support in insulin resistance: An overview of current scientific reports. Adv. Clin. Exp. Med. 2019, 28, 1577–1585. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Non-HUA | HUA | p-Value |
|---|---|---|---|---|
| N = 41,230 | n = 34,488 | n = 6742 | ||
| Age (years) | 43.53 ± 20.89 | 42.49 ± 20.61 | 48.67 ± 20.48 | <0.001 |
| Male, % | 20,297 (49.23) | 16,485 (46.83) | 3812 (57.22) | <0.001 |
| Non-Hispanic white, % | 16,618 (40.31) | 13,648 (39.77) | 2970 (44.39) | <0.001 |
| College graduate or above, % | 7571 (18.36) | 6345 (18.10) | 1226 (18.79) | <0.001 |
| Household income over $75,000, % | 10,146 (24.61) | 8672 (25.24) | 1474 (20.72) | <0.001 |
| Exercised regularly, % | 11,920 (28.91) | 10,320 (29.70) | 1600 (23.95) | <0.001 |
| Married, % | 17,198 (41.71) | 14,133 (40.68) | 3065 (45.40) | <0.001 |
| Smoking, % | 6817 (16.53) | 5739 (17.43) | 1078 (16.01) | <0.001 |
| Drinking, % | 21,653 (52.52) | 17,787 (51.66) | 3866 (56.81) | <0.001 |
| BMI, kg/m2 | 28.43 ± 7.09 | 27.62 ± 6.63 | 32.41 ± 7.88 | <0.001 |
| DM, % | 9230 (22.39) | 6799 (20.29) | 2431 (35.93) | <0.001 |
| Pre-DM, % | 11,003 (26.69) | 8638 (24.20) | 2365 (34.11) | <0.001 |
| Hypertension, % | 14,129 (34.27) | 10,267 (29.34) | 3862 (53.63) | <0.001 |
| Hyperlipidemia, % | 26,658 (64.66) | 21,256 (62.21) | 5402 (80.68) | <0.001 |
| CKD, % | 6886 (16.7) | 4792 (11.54) | 2094 (26.02) | <0.001 |
| Characteristics | Total | Non-HUA | HUA | Adjust.p |
|---|---|---|---|---|
| N = 41,230 | n = 34,488 | n = 6742 | ||
| f_whole (cup) | 0.66 ± 1.08 | 0.68 ± 1.09 | 0.60 ± 1.06 | 0.002 |
| f_citmlb (cup) | 0.20 ± 0.64 | 0.20 ± 0.63 | 0.19 ± 0.68 | 0.355 |
| f_juice (cup) | 0.29 ± 0.80 | 0.30 ± 0.82 | 0.24 ± 0.69 | <0.001 |
| f_other (cup) | 0.46 ± 0.82 | 0.47 ± 0.83 | 0.41 ± 0.77 | 0.002 |
| f_total (cup) | 0.95 ± 1.38 | 0.97 ± 1.40 | 0.84 ± 1.28 | <0.001 |
| v_drkgr (cup) | 0.14 ± 0.37 | 0.14 ± 0.37 | 0.15 ± 0.38 | 0.883 |
| v_redor_tomato (cup) | 0.30 ± 0.41 | 0.30 ± 0.41 | 0.29 ± 0.40 | 0.813 |
| v_redor_other (cup) | 0.09 ± 0.23 | 0.09 ± 0.23 | 0.08 ± 0.22 | 0.182 |
| v_redor_total (cup) | 0.39 ± 0.47 | 0.39 ± 0.47 | 0.38 ± 0.46 | 0.429 |
| v_starchy_potato (cup) | 0.37 ± 0.60 | 0.36 ± 0.59 | 0.39 ± 0.61 | 0.049 |
| v_starchy_other (cup) | 0.08 ± 0.26 | 0.08 ± 0.26 | 0.08 ± 0.26 | 0.599 |
| v_starchy_total (cup) | 0.44 ± 0.66 | 0.44 ± 0.66 | 0.47 ± 0.67 | 0.049 |
| v_other (cup) | 0.55 ± 0.70 | 0.55 ± 0.71 | 0.54 ± 0.65 | 0.738 |
| v_total (cup) | 1.52 ± 1.25 | 1.52 ± 1.25 | 1.53 ± 1.21 | 0.599 |
| v_legumes (cup) | 0.11 ± 0.37 | 0.12 ± 0.37 | 0.11 ± 0.34 | 0.275 |
| g_whole (oz) | 0.83 ± 1.29 | 0.85 ± 1.29 | 0.76 ± 1.31 | 0.002 |
| g_refined (oz) | 5.86 ± 4.30 | 5.94 ± 4.40 | 5.46 ± 4.00 | <0.001 |
| g_total (oz) | 6.69 ± 4.40 | 6.79 ± 4.50 | 6.22 ± 4.10 | <0.001 |
| d_milk (cup) | 0.80 ± 1.08 | 0.83 ± 1.11 | 0.63 ± 0.89 | <0.001 |
| d_yogurt (cup) | 0.06 ± 0.19 | 0.06 ± 0.19 | 0.05 ± 0.17 | 0.002 |
| d_cheese (cup) | 0.77 ± 1.03 | 0.78 ± 1.04 | 0.71 ± 0.94 | 0.002 |
| d_total (cup) | 1.66 ± 1.55 | 1.71 ± 1.58 | 1.41 ± 1.34 | <0.001 |
| pf_meat (oz) | 1.65 ± 2.62 | 1.64 ± 2.61 | 1.71 ± 2.65 | 0.205 |
| pf_curedmeat (oz) | 1.02 ± 1.75 | 1.02 ± 1.74 | 1.01 ± 1.81 | 0.940 |
| pf_organ (oz) | 0.02 ± 0.31 | 0.02 ± 0.30 | 0.02 ± 0.40 | 0.738 |
| pf_poult (oz) | 1.53 ± 2.68 | 1.47 ± 2.59 | 1.84 ± 3.10 | <0.001 |
| pf_seafd_hi (oz) | 0.15 ± 0.89 | 0.15 ± 0.84 | 0.20 ± 1.08 | 0.019 |
| pf_seafd_low (oz) | 0.44 ± 1.88 | 0.43 ± 1.82 | 0.49 ± 2.15 | 0.158 |
| pf_mps_total (oz) | 4.82 ± 4.20 | 4.72 ± 4.10 | 5.27 ± 4.60 | <0.001 |
| pf_eggs (oz) | 0.53 ± 0.94 | 0.54 ± 0.96 | 0.49 ± 0.88 | 0.004 |
| pf_soy (oz) | 0.08 ± 0.37 | 0.08 ± 0.38 | 0.06 ± 0.30 | 0.002 |
| pf_nutsds (oz) | 0.71 ± 1.74 | 0.73 ± 1.75 | 0.62 ± 1.67 | 0.004 |
| pf_legumes (oz) | 0.46 ± 1.47 | 0.46 ± 1.49 | 0.42 ± 1.35 | 0.275 |
| pf_total (oz) | 6.14 ± 4.70 | 6.08 ± 4.70 | 6.44 ± 5.10 | 0.002 |
| add_sugars (tsp) | 18.20 ± 17.00 | 18.32 ± 17.00 | 17.59 ± 17.00 | 0.036 |
| oils (grams) | 25.67 ± 21.00 | 25.78 ± 22.00 | 25.17 ± 21.00 | 0.253 |
| solid_fats (grams) | 38.04 ± 28.00 | 38.36 ± 29.00 | 36.47 ± 27.00 | 0.006 |
| a_drinks (nunber of drinks) | 0.69 ± 1.85 | 0.63 ± 1.71 | 0.99 ± 2.41 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Yang, R.; Cao, Z.; Han, S.; Han, T.; Jiang, W.; Wang, X.; Wei, W. The Association of Food Groups and Consumption Time with Hyperuricemia: The U.S. National Health and Nutrition Examination Survey, 2005–2018. Nutrients 2023, 15, 3109. https://doi.org/10.3390/nu15143109
Wang Y, Yang R, Cao Z, Han S, Han T, Jiang W, Wang X, Wei W. The Association of Food Groups and Consumption Time with Hyperuricemia: The U.S. National Health and Nutrition Examination Survey, 2005–2018. Nutrients. 2023; 15(14):3109. https://doi.org/10.3390/nu15143109
Chicago/Turabian StyleWang, Yuanyuan, Ruiming Yang, Ziteng Cao, Sijia Han, Tianshu Han, Wenbo Jiang, Xinyang Wang, and Wei Wei. 2023. "The Association of Food Groups and Consumption Time with Hyperuricemia: The U.S. National Health and Nutrition Examination Survey, 2005–2018" Nutrients 15, no. 14: 3109. https://doi.org/10.3390/nu15143109
APA StyleWang, Y., Yang, R., Cao, Z., Han, S., Han, T., Jiang, W., Wang, X., & Wei, W. (2023). The Association of Food Groups and Consumption Time with Hyperuricemia: The U.S. National Health and Nutrition Examination Survey, 2005–2018. Nutrients, 15(14), 3109. https://doi.org/10.3390/nu15143109