
New Food Frequency Questionnaire to Estimate Vitamin K Intake in a Mediterranean Population

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Food Frequency Questionnaire (FFQ)
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Food Frequency Questionnaire Items
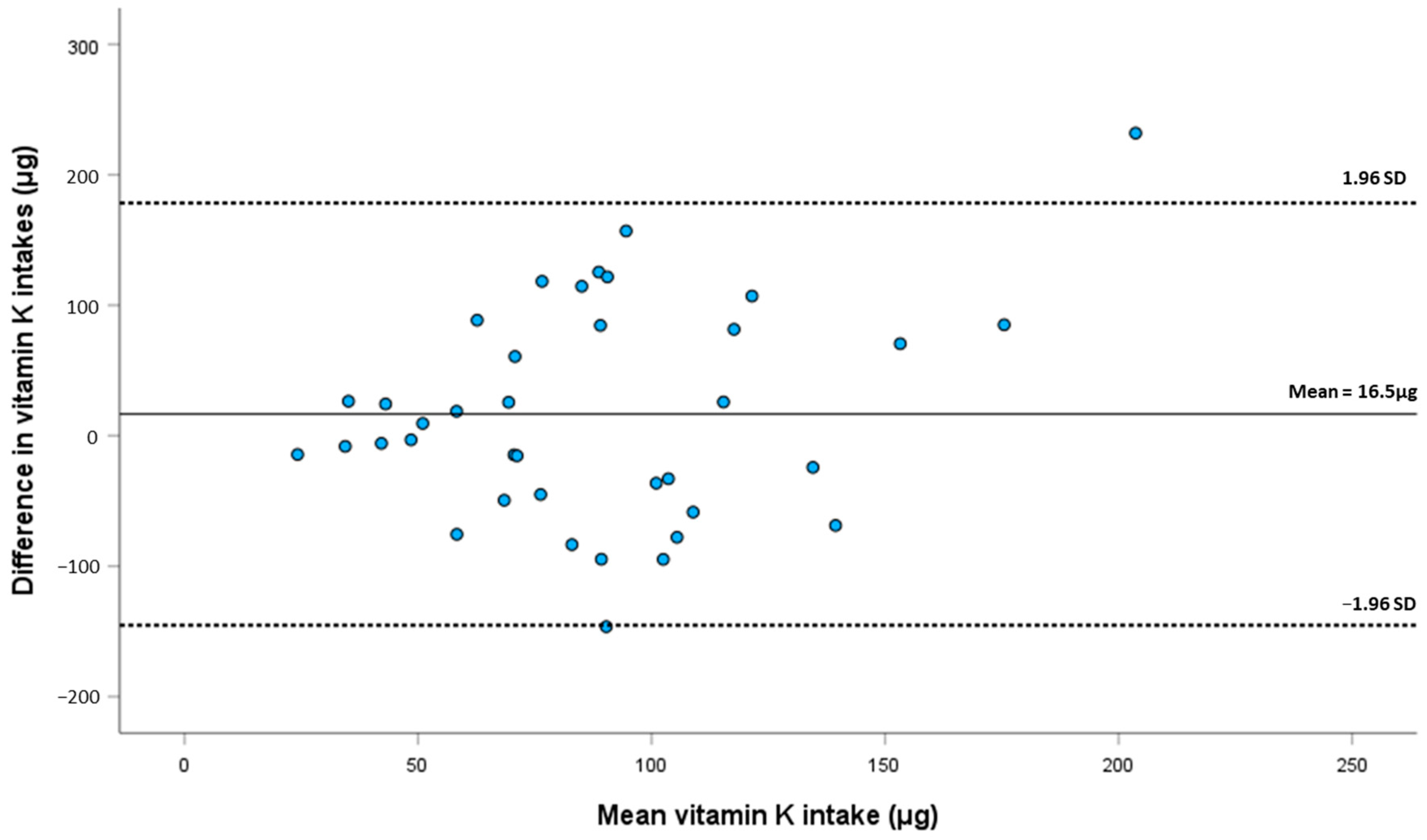
3.3. Comparison between Food Records and Food Frequency Questionnaire
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simes, D.C.; Viegas, C.S.B.; Araújo, N.; Marreiros, C. Vitamin K as a Diet Supplement with Impact in Human Health: Current Evidence in Age-Related Diseases. Nutrients 2020, 12, 138. [Google Scholar] [CrossRef]
- Simes, D.C.; Viegas, C.S.B.; Araújo, N.; Marreiros, C. Vitamin K as a Powerful Micronutrient in Aging and Age-Related Diseases: Pros and Cons from Clinical Studies. Int. J. Mol. Sci. 2019, 20, 4150. [Google Scholar] [CrossRef] [PubMed]
- Mishima, E.; Ito, J.; Wu, Z.; Nakamura, T.; Wahida, A.; Doll, S.; Tonnus, W.; Nepachalovich, P.; Eggenhofer, E.; Aldrovandi, M.; et al. A non-canonical vitamin K cycle is a potent ferroptosis suppressor. Nature 2022, 608, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.L. Vitamin K: Food composition and dietary intakes. Food Nutr. Res. 2012, 56, 5505. [Google Scholar] [CrossRef] [PubMed]
- Shearer, M.J.; Newman, P. Recent trends in the metabolism and cell biology of vitamin K with special reference to vitamin K cycling and MK-4 biosynthesis. J. Lipid Res. 2014, 55, 345–362. [Google Scholar] [CrossRef]
- Thijssen, H.H.; Drittij-Reijnders, M.J. Vitamin K distribution in rat tissues: Dietary phylloquinone is a source of tissue menaquinone-4. Br. J. Nutr. 1994, 72, 415–425. [Google Scholar] [CrossRef]
- Schurgers, L.J.; Vermeer, C. Determination of phylloquinone and menaquinones in food. Effect of food matrix on circulating vitamin K concentrations. Haemostasis 2000, 30, 298–307. [Google Scholar]
- Akbulut, A.C.; Pavlic, A.; Petsophonsakul, P.; Halder, M.; Maresz, K.; Kramann, R.; Schurgers, L. Vitamin K2 Needs an RDI Separate from Vitamin K1. Nutrients 2020, 12, 1852. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, DC, USA, 2001. [Google Scholar]
- Passarelli, S.; Free, C.M.; Allen, L.H.; Batis, C.; Beal, T.; Biltoft-Jensen, A.P.; Bromage, S.; Cao, L.; Castellanos-Gutiérrez, A.; Christensen, T.; et al. Estimating national and subnational nutrient intake distributions of global diets. Am. J. Clin. Nutr. 2022, 116, 551–560. [Google Scholar] [CrossRef]
- Browner, W.; Newman, T.; Hulley, S. Estimating Sample Size and Power: Applications and Examples. In Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Hulley, S., Cummings, S., Browner, W., Grady, D., Newman, T., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 55–83. [Google Scholar]
- Bingham, S.A.; Welch, A.A.; McTaggart, A.; Mulligan, A.A.; Runswick, S.A.; Luben, R.; Oakes, S.; Khaw, K.T.; Wareham, N.; Day, N.E. Nutritional methods in the European Prospective Investigation of Cancer in Norfolk. Public Health Nutr. 2001, 4, 847. [Google Scholar] [CrossRef]
- University of Porto; National Health Institute Doutor Ricardo Jorge; University of Lisbon; SilicoLife Lda; Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Guiomar, S.; Alarcão, V.; et al. National Food, Nutrition and Physical Activity Survey of the Portuguese general population. EFSA Support. Publ. 2017, 14, EN-1341. [Google Scholar] [CrossRef]
- Bingham, S.A.; Gill, C.; Welch, A.; Cassidy, A.; Runswick, S.A.; Oakes, S.; Lubin, R.; Thurnham, D.I.; Key, T.J.; Roe, L.; et al. Validation of dietary assessment methods in the UK arm of EPIC using weighed records, and 24-hour urinary nitrogen and potassium and serum vitamin C and carotenoids as biomarkers. Int. J. Epidemiol. 1997, 26, S137–S151. [Google Scholar] [CrossRef]
- Presse, N.; Shatenstein, B.; Kergoat, M.J.; Ferland, G. Validation of a Semi-Quantitative Food Frequency Questionnaire Measuring Dietary Vitamin K Intake in Elderly People. J. Am. Diet Assoc. 2009, 109, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Dias Mendonça, D.; Zuchinali, P.; Souza, G.C. Development of a food frequency questionnaire to determine vitamin k intake in anticoagulated patients: A pilot study. Rev. Chil. Nut. 2018, 45, 363–371. [Google Scholar] [CrossRef]
- Roe, M.; Pinchen, H.; Church, S.; Finglas, P. McCance and Widdowson’s The Composition of Foods Seventh Summary Edition and updated Composition of Foods Integrated Dataset. Nutr. Bull. 2015, 40, 36–39. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef]
- Willett, W. Mediterranean Dietary Pyramid. Int. J. Environ. Res. Public Health 2021, 18, 4568. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; pp. 70–95. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2003, 5, 567–587. [Google Scholar] [CrossRef]
- Nelson, M. The validation of dietary assessment. In Design Concepts in Nutritional Epidemiology, 2nd ed.; Barrie, M., Margetts, B.M., Nelson, M., Eds.; Oxford University Press: New York, NY, USA, 1997; pp. 241–272. [Google Scholar]
- US Department of Agriculture. FoodData Central. Available online: https://fdc.nal.usda.gov/index.html (accessed on 30 November 2022).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Doğan, N.Ö. Bland-Altman analysis: A paradigm to understand correlation and agreement. Turk. J. Emerg. Med. 2018, 18, 139–141. [Google Scholar] [CrossRef]
- Ludbrook, J. Confidence in Altman–Bland plots: A critical review of the method of differences. Clin. Exp. Pharmacol. Physiol. 2010, 37, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.E. Measuring diet in the 21st century: Use of new technologies. Proc. Nutr. Soc. 2017, 76, 276–282. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Schulz, C.A.; Oluwagbemigun, K.; Nöthlings, U. Advances in dietary pattern analysis in nutritional epidemiology. Eur. J. Nutr. 2021, 60, 4115–4130. [Google Scholar] [CrossRef] [PubMed]
- Buitenhuis, H.; Soute, B.; Vermeer, C. Comparison of the vitamins K1, K2 and K3 as cofactors for the hepatic vitamin K-dependent carboxylase. Biochim. Biophys. Acta 1990, 1034, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Akiyama, Y.; Nakamura, T.; Murota, S.; Morita, I. The inhibitory effect of vitamin K2 (menatetrenone) on bone resorption may be related to its side chain. Bone 1995, 16, 179–184. [Google Scholar] [CrossRef]
- Ambrożewicz, E.; Muszyńska, M.; Tokajuk, G.; Grynkiewicz, G.; Žarković, N.; Skrzydlewska, E. Beneficial Effects of Vitamins K and D3 on Redox Balance of Human Osteoblasts Cultured with Hydroxypatite-Based Biomaterials. Cells 2019, 8, 325. [Google Scholar] [CrossRef]
- Lev, M.; Milford, A. The 3-Ketodihydrosphingosine melaninogenicus: Synthetase of Bacteroides melaninogenicus: Induction by Vitamin K. Arch. Biochem. Biophys. 1973, 157, 500–508. [Google Scholar] [CrossRef]
- Sundaram, K.S.; Lev, M. Regulation of sulfotransferase activity by vitamin k in mouse brain. Arch. Biochem. Biophys. 1990, 277, 109–113. [Google Scholar] [CrossRef]
- Xv, F.; Chen, J.; Duan, L.; Li, S. Research progress on the anticancer effects of vitamin K2. Oncol. Lett. 2018, 15, 8926–8934. [Google Scholar] [CrossRef]
- Thijssen, H.; Drittij-Reijnders, M. Vitamin K status in human tissues: Tissue-specific accumulation of phylloquinone and menaquinone-4. Br. J. Nutr. 1996, 75, 121–127. [Google Scholar] [CrossRef]
- Thijssen, H.H.; Drittij, M.J.; Vermeer, C.; Schoffelen, E. Menaquinone-4 in breast milk is derived from dietary phylloquinone. Br. J. Nutr. 2002, 87, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.L.; Sokoll, L.J.; O’Brien, M.E.; Tucker, K.; Dawson-Hughes, B.; Sadowski, J.A. Assessment of dietary phylloquinone intake and vitamin K status in postmenopausal women. Eur. J. Clin. Nutr. 1995, 49, 832–841. [Google Scholar]
- Booth, S.L.; Tucker, K.L.; McKeown, N.M.; Davidson, K.W.; Dallal, G.E.; Sadowski, J.A. Relationships between Dietary Intakes and Fasting Plasma Concentrations of Fat-Soluble Vitamins in Humans. J. Nutr. 1997, 127, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, J.M.; Seechurn, T.; Atkinson, S.A. A food frequency questionnaire for the assessment of calcium, vitamin D and vitamin K: A pilot validation study. Nutrients 2010, 2, 805–819. [Google Scholar] [CrossRef] [PubMed]
- Couris, R.R.; Tataronis, G.R.; Booth, S.L.; Dallal, G.E.; Blumberg, J.B.; Dwyer, J.T. Development of a self-assessment instrument to determine daily intake and variability of dietary vitamin K. J. Am. Coll. Nutr. 2000, 19, 801–807. [Google Scholar] [CrossRef]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef]
- Cantin, J.; Latour, E.; Ferland-Verry, R.; Morales Salgado, S.; Lambert, J.; Faraj, M.; Nigam, A. Validity and reproducibility of a food frequency questionnaire focused on the Mediterranean diet for the Quebec population. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 154–161. [Google Scholar] [CrossRef]
- Zwakenberg, S.R.; Engelen, A.I.P.; Dalmeijer, G.W.; Booth, S.L.; Vermeer, C.; Drijvers, J.J.M.M.; Ocke, M.C.; Feskens, E.J.M.; van der Schouw, Y.T.; Beulens, J.W.J. Reproducibility and relative validity of a food frequency questionnaire to estimate intake of dietary phylloquinone and menaquinones. Eur. J. Clin. Nutr. 2017, 71, 1423–1428. [Google Scholar] [CrossRef]
- Bu, S.Y.; Choi, M.K.; Jin So, E. Validity and Reliability of a Self-administered Food Frequency Questionnaire to Assess Vitamin K Intake in Korean Adults. Clin. Nutr. Res. 2016, 5, 153–160. [Google Scholar]
- Thane, C.W.; Paul, A.A.; Bates, C.J.; Bolton-Smith, C.; Prentice, A.; Shearer, M.J. Intake and sources of phylloquinone (vitamin K1): Variation with socio-demographic and lifestyle factors in a national sample of British elderly people. Br. J. Nutr. 2002, 87, 605–613. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intake Frequency | Conversion Factor |
|---|---|
| Never or less than once per month | 0.02 |
| 1–3 per month | 0.07 |
| 1 per week | 0.14 |
| 2–4 per week | 0.43 |
| 5–6 per week | 0.79 |
| 1 per day | 1 |
| 2–3 per day | 2.5 |
| 4+ per day | 4 |
| Characteristics | All | Males | Females | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| (n = 38) | (n = 15) | (n = 23) | ||||||
| Age (years) | Mean (±SD) | 37 | (±12.2) | 31 | (±4.5) | 41 | (±14) | 0.004 a |
| Median (IQR) | 36.5 | (19) | 31 | (8) | 44 | (27) | ||
| BMI (kg/m2) | Mean (±SD) | 24.6 | (±0.6) | 24.8 | (±0.3) | 24.5 | (±0.7) | |
| Median (IQR) | 24.6 | (0.5) | 24.7 | (0.6) | 24.6 | (0.6) | 0.051 b | |
| Education (level): | ||||||||
| Primary school (4 years); n (%) | 2 | (5%) | - | 2 | (9%) | 0.002 c | ||
| Middle school (5–9 years); n (%) | 2 | (5%) | - | 2 | (9%) | |||
| High school (10–12 years); n (%) | 8 | (21%) | - | 8 | (35%) | |||
| College level degree; n (%) | 26 | (69%) | 15 | (100%) | 11 | (48%) | ||
| Category | Food Item |
|---|---|
| Meat, fish, and eggs | Tuna in oil, drained; Beef, minced meat or hamburger; Cold cuts (ham, mortadella, chorizo, etc.); Mackerel, horse mackerel or small fish; Scrambled or fried egg |
| Grains and tubers | Homemade or restaurant French fries; Packaged potato chips or corn snacks; Homemade bread |
| Desserts and sweets | Cookies, biscuits; Cake, tart or other pastry product (croissant, etc.); Milk chocolate |
| Fruits | Plum, cherry; Almond, walnut, hazelnut; Peanut, cashew; Dried figs; Apple, pear; Strawberry; Nectarines; Peach; Grapes; Avocado |
| Vegetables and pulses | Pumpkin; Watercress, arugula; Lettuce or mixed green salad; Leek; Eggplant; Broccoli; Carrot; Coriander or parsley; Kale; Cabbage, collard greens, brussels sprouts; Cauliflower; Zucchini; Peas; Asparagus, green beans; Spinach; Cooked beans; Cooked chickpeas; Greens, creamed spinach, green vegetable puree; Cucumber; Green pepper; Red pepper; Tomato |
| Fats and oils | Olive oil; Butter, margarine or vegetable spread, mayonnaise; Cooking oil |
| Other | Espresso coffee |
| Meals | Lasagna or pasta; Stir-fry or stew with vegetables and/or pasta |
| Dairy products | Creamy cheese (Brie, Camembert) or Serra da Estrela cheese; Cream cheese, spreadable; Cured cow or sheep cheese, Edam cheese; Goat cheese; Cottage or fresh cheese |
| Food Records | FFQ | p-Value | ||||
|---|---|---|---|---|---|---|
| Vitamin K intake (μg) | Mean (±SD) | 80 | (±47.7) | 96.5 | (±64.3) | 0.293 a,b |
| Median (IQR) | 77.4 | (84.5) | 80.9 | (89.4) | ||
| Minimum | 16.1 | 17 | ||||
| Maximum | 173.8 | 319 | ||||
| Difference between FFQ and food records: Mean (±SD); (95% CI) | 16.5 (±82.57); (−10.7, 43.6) | 0.226 b | ||||
| Correlation between FFQ and food: | 0.697 | 0.003 a | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, E.; Viegas, C.; Martins, P.V.; Nascimento, T.; Schurgers, L.; Simes, D. New Food Frequency Questionnaire to Estimate Vitamin K Intake in a Mediterranean Population. Nutrients 2023, 15, 3012. https://doi.org/10.3390/nu15133012
Pinto E, Viegas C, Martins PV, Nascimento T, Schurgers L, Simes D. New Food Frequency Questionnaire to Estimate Vitamin K Intake in a Mediterranean Population. Nutrients. 2023; 15(13):3012. https://doi.org/10.3390/nu15133012
Chicago/Turabian StylePinto, Ezequiel, Carla Viegas, Paula Ventura Martins, Tânia Nascimento, Leon Schurgers, and Dina Simes. 2023. "New Food Frequency Questionnaire to Estimate Vitamin K Intake in a Mediterranean Population" Nutrients 15, no. 13: 3012. https://doi.org/10.3390/nu15133012
APA StylePinto, E., Viegas, C., Martins, P. V., Nascimento, T., Schurgers, L., & Simes, D. (2023). New Food Frequency Questionnaire to Estimate Vitamin K Intake in a Mediterranean Population. Nutrients, 15(13), 3012. https://doi.org/10.3390/nu15133012