
Acute Effect of a Saffron Extract (Safr’InsideTM) and Its Main Volatile Compound on the Stress Response in Healthy Young Men: A Randomized, Double Blind, Placebo-Controlled, Crossover Study
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Tested Products
2.3. Study Design and Protocol
2.4. Maastricht Acute Stress Test
2.5. Salivary Cortisol and Cortisone
2.6. Statistical Analyses
3. Results
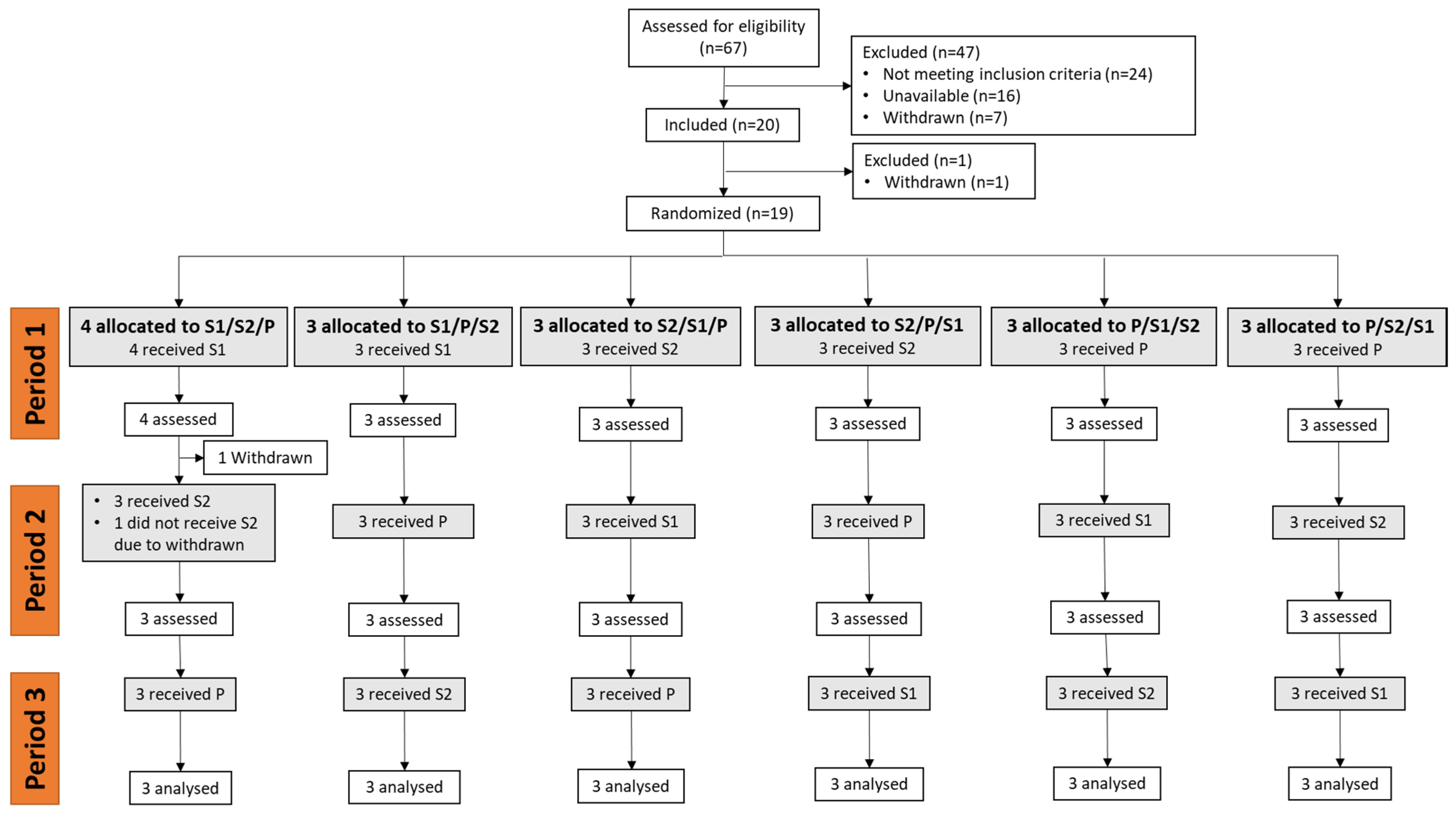
3.1. Inclusion and Population Characteristics
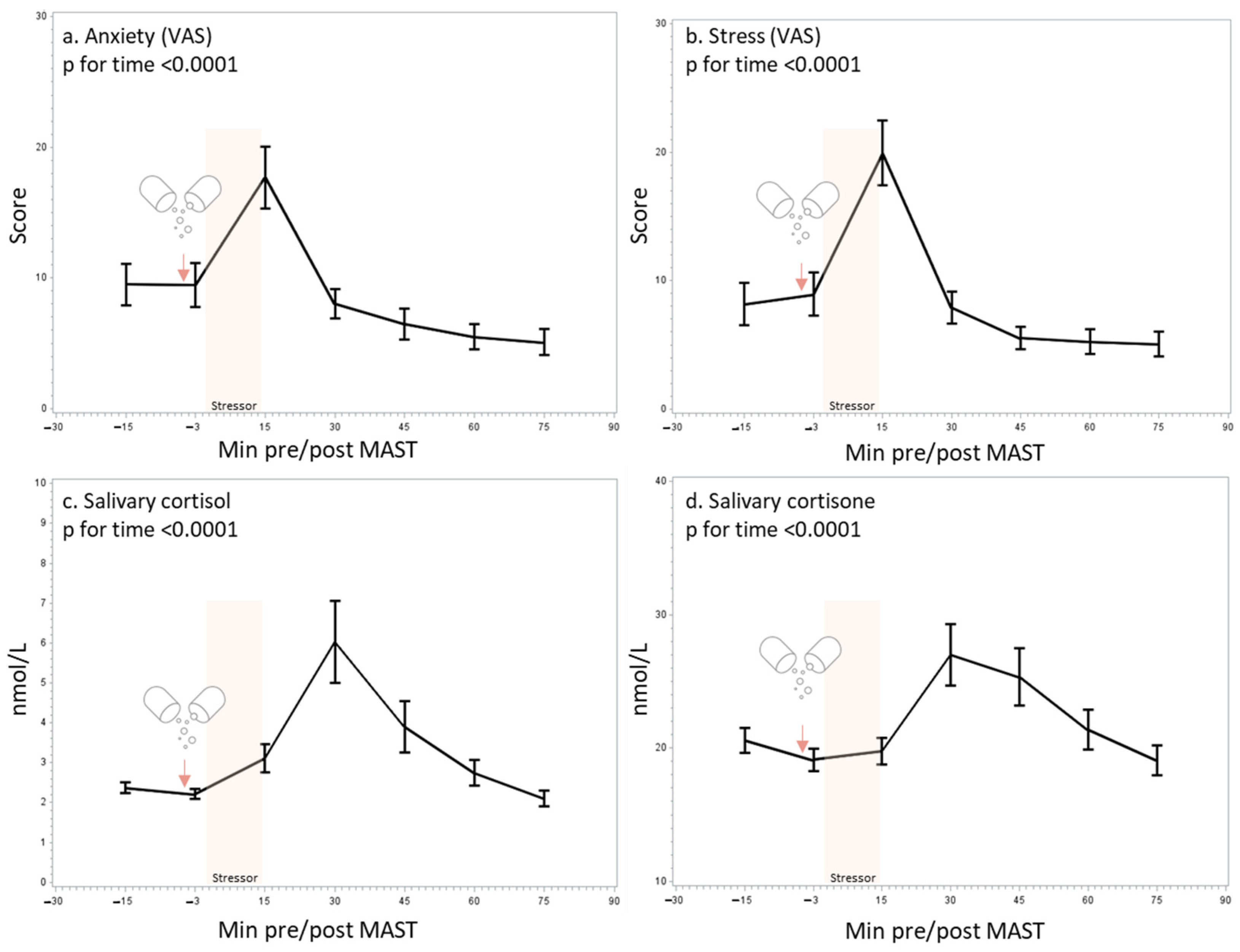
3.2. Validation of the MAST
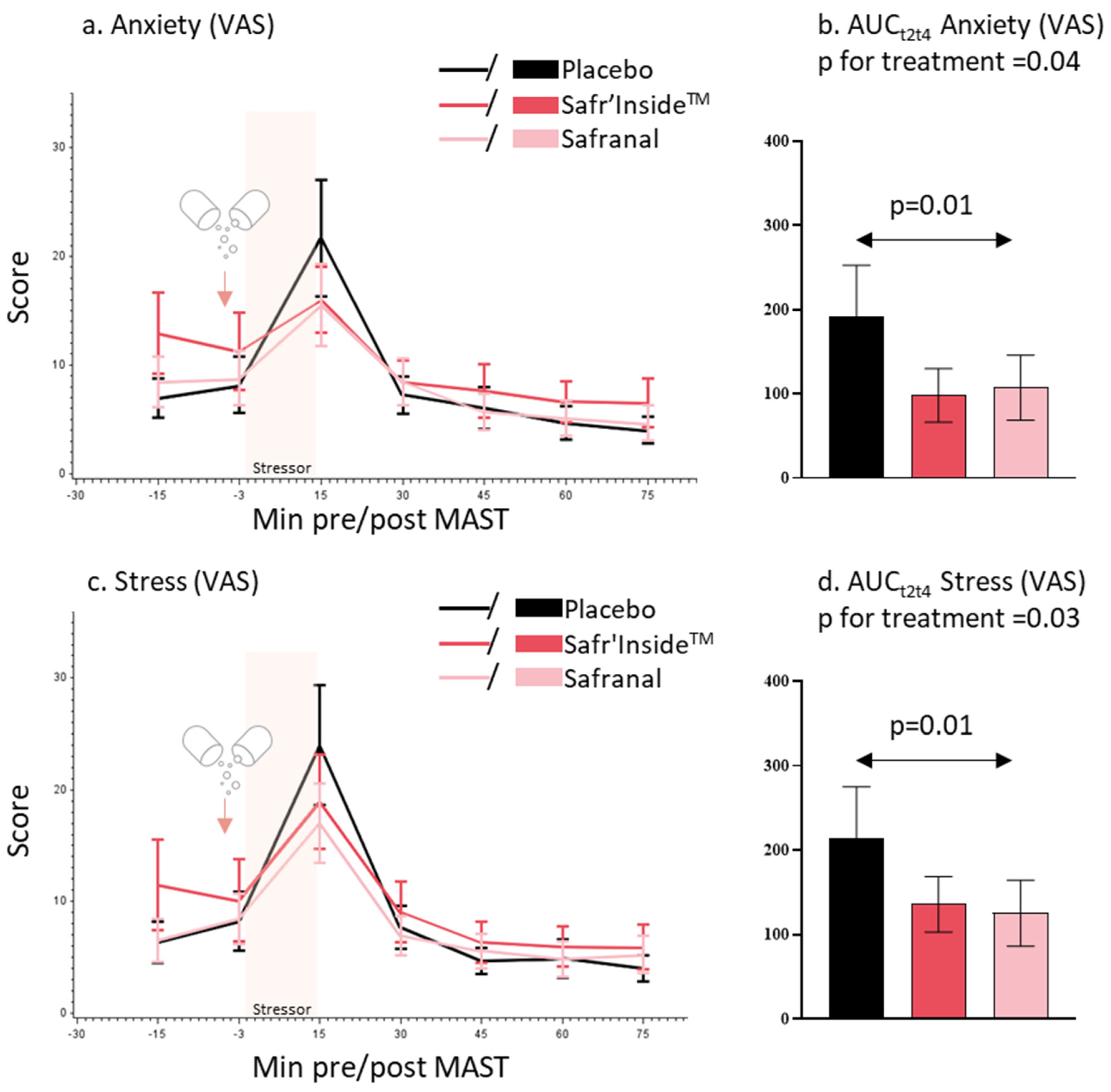
3.3. Self-Perceived Anxiety and Stress
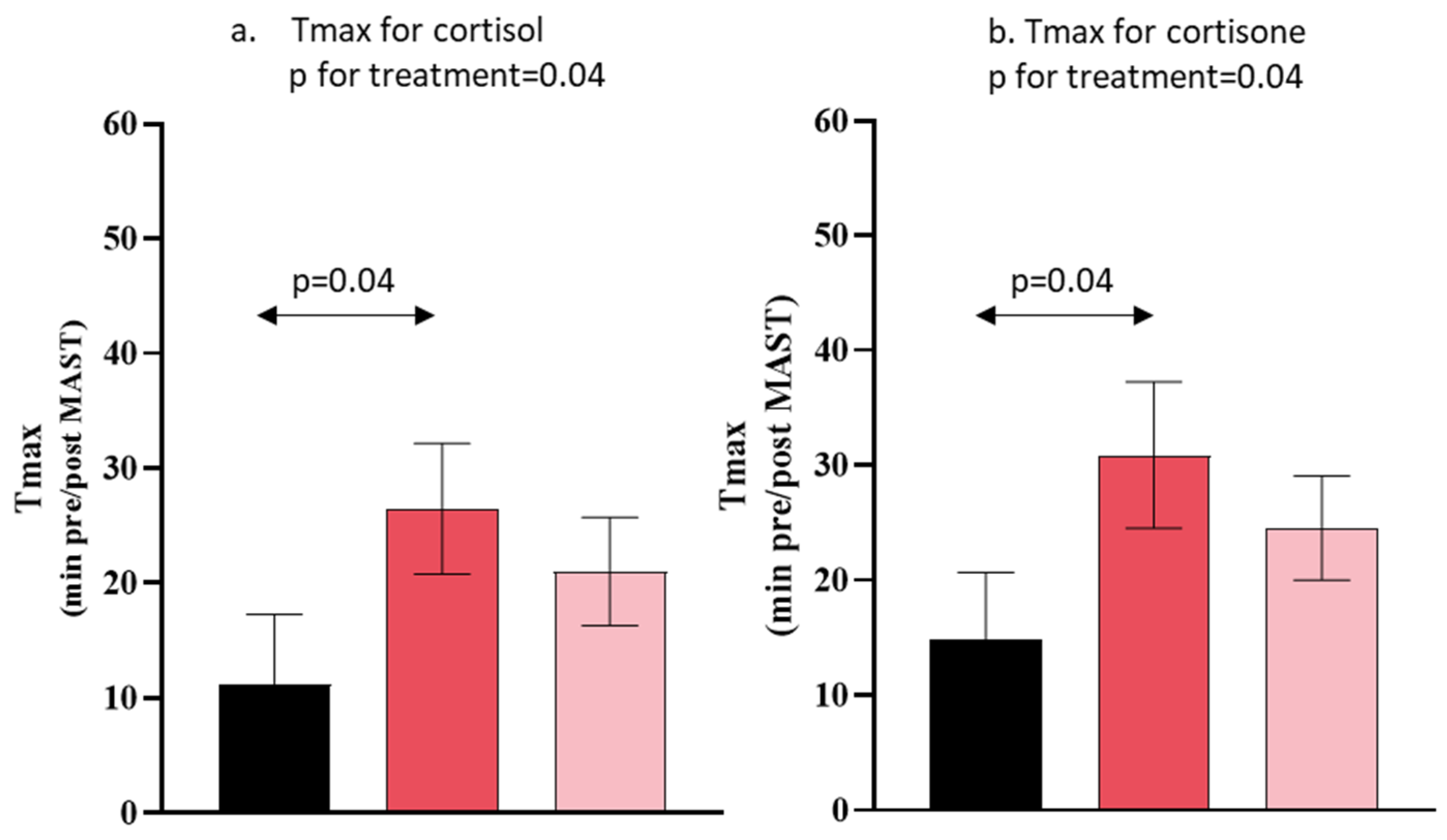
3.4. Salivary Cortisol and Cortisone Concentration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lazarus, R.; Folkman, S. The Stress Concept in the Life Sciences. In Stress, Appraisal and Coping; Springer Publishing Company: New York, NY, USA, 1984; p. 19. [Google Scholar]
- Chu, B.; Marwaha, K.; Sanvictores, T.; Ayers, D. Physiology, Stress Reaction; StatPearls: Tampa, FL, USA, 2022. [Google Scholar]
- Pulopulos, M.M.; Baeken, C.; De Raedt, R. Cortisol Response to Stress: The Role of Expectancy and Anticipatory Stress Regulation. Horm. Behav. 2020, 117, 104587. [Google Scholar] [CrossRef] [PubMed]
- Agorastos, A.; Chrousos, G.P. The Neuroendocrinology of Stress: The Stress-Related Continuum of Chronic Disease Development. Mol. Psychiatry 2022, 27, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Khan, R. Chronic Stress Leads to Anxiety and Depression. Ann. Psychiatry Ment. Health 2017, 5, 1091. [Google Scholar]
- Wechsler, T.F.; Schmidmeier, M.; Biehl, S.; Gerczuk, J.; Guerrero-Cerda, F.M.; Mühlberger, A. Individual Changes in Stress, Depression, Anxiety, Pathological Worry, Posttraumatic Stress, and Health Anxiety from before to during the COVID-19 Pandemic in Adults from Southeastern Germany. BMC Psychiatry 2022, 22, 528. [Google Scholar] [CrossRef] [PubMed]
- Coelho, J.; Micoulaud-Franchi, J.A.; Wiet, A.S.; Nguyen, D.; Taillard, J.; Philip, P. Circadian Misalignment Is Associated with COVID-19 Infection. Sleep Med. 2022, 93, 71–74. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and Cardiovascular Disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef]
- Gallo, L.C.; Roesch, S.C.; Fortmann, A.L.; Carnethon, M.R.; Penedo, F.J.; Perreira, K.; Birnbaum-Weitzman, O.; Wassertheil-Smoller, S.; Castañeda, S.F.; Talavera, G.A.; et al. Associations of Chronic Stress Burden, Perceived Stress, and Traumatic Stress with Cardiovascular Disease Prevalence and Risk Factors in the Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. Psychosom. Med. 2014, 76, 468–475. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief, 2 March 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 26 October 2022).
- McCabe, D.; Lockwood, C. Women’s Experience of Stress and Related Use of Diet and/or Dietary Supplements. Nurs. Health Sci. 2020, 22, 1121–1130. [Google Scholar] [CrossRef]
- Fischer, J.M.; Kandil, F.-I.; Kessler, C.S.; Nayeri, L.; Zager, L.S.; Rocabado Hennhöfer, T.; Steckhan, N.; Koppold-Liebscher, D.A.; Bringmann, H.C.; Schäfer, T.; et al. Clinical Medicine Stress Reduction by Yoga versus Mindfulness Training in Adults Suffering from Distress: A Three-Armed Randomized Controlled Trial Including Qualitative Interviews (RELAX Study). J. Clin. Med. 2022, 11, 5680. [Google Scholar] [CrossRef]
- Goldstein Reasearch Global Stress Management Supplements Market Outlook 2017–2025. Market Report on Dietary Supplement Purchasing Trends. 2018. Available online: https://www.goldsteinresearch.com/report/stress-relief-supplements-market-anxiety-management (accessed on 2 May 2023).
- Doering, B.K.; Wegner, A.; Hadamitzky, M.; Engler, H.; Rief, W.; Schedlowski, M. Effects of Neurexan® in an Experimental Acute Stress Setting—An Explorative Double-Blind Study in Healthy Volunteers. Life Sci. 2016, 146, 139–147. [Google Scholar] [CrossRef]
- Coventry, P.A.; Meader, N.; Melton, H.; Temple, M.; Dale, H.; Wright, K.; Cloitre, M.; Karatzias, T.; Bisson, J.; Roberts, N.P.; et al. Psychological and Pharmacological Interventions for Posttraumatic Stress Disorder and Comorbid Mental Health Problems Following Complex Traumatic Events: Systematic Review and Component Network Meta-Analysis. PLoS Med. 2020, 17, e1003262. [Google Scholar] [CrossRef]
- Sarris, J.; Ravindran, A.; Yatham, L.N.; Marx, W.; Rucklidge, J.J.; McIntyre, R.S.; Akhondzadeh, S.; Benedetti, F.; Caneo, C.; Cramer, H.; et al. Clinician Guidelines for the Treatment of Psychiatric Disorders with Nutraceuticals and Phytoceuticals: The World Federation of Societies of Biological Psychiatry (WFSBP) and Canadian Network for Mood and Anxiety Treatments (CANMAT) Taskforce. World J. Biol. Psychiatry 2022, 23, 424–455. [Google Scholar] [CrossRef]
- Rios, J.L.; Recio, M.C.; Giner, R.M.; Mànez, S. An Update Review of Saffron Ans Its Active Constituents. Phyther. Res. 1996, 10, 189–193. [Google Scholar] [CrossRef]
- Hosseinzadeh, H.; Noraei, N.B. Anxiolytic and Hypnotic Effect of Crocus sativus Aqueous Extract and Its Constituents, Crocin and Safranal, in Mice. Phyther. Res. 2009, 23, 768–774. [Google Scholar] [CrossRef]
- Hooshmandi, Z.; Rohani, A.H.; Eidi, A.; Fatahi, Z.; Golmanesh, L.; Sahraei, H. Reduction of Metabolic and Behavioral Signs of Acute Stress in Male Wistar Rats by Saffron Water Extract and Its Constituent Safranal. Pharm. Biol. 2011, 49, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Halataei, B.A.S.; Khosravi, M.; Arbabian, S.; Sahraei, H.; Golmanesh, L.; Zardooz, H.; Jalili, C.; Ghoshooni, H. Saffron (Crocus sativus) Aqueous Extract and Its Constituent Crocin Reduces Stress-Induced Anorexia in Mice. Phyther. Res. 2011, 25, 1833–1838. [Google Scholar] [CrossRef]
- Fukui, H.; Toyoshima, K.; Komaki, R. Psychological and Neuroendocrinological Effects of Odor of Saffron (Crocus sativus). Phytomedicine 2011, 18, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Jackson, P.A.; Forster, J.; Khan, J.; Pouchieu, C.; Dubreuil, S.; Gaudout, D.; Moras, B.; Pourtau, L.; Joffre, F.; Vaysse, C.; et al. Effects of Saffron Extract Supplementation on Mood, Well-Being, and Response to a Psychosocial Stressor in Healthy Adults: A Randomized, Double-Blind, Parallel Group, Clinical Trial. Front. Nutr. 2021, 7, 365. [Google Scholar] [CrossRef] [PubMed]
- Herbison, C.E.; Henley, D.; Marsh, J.; Atkinson, H.; Newnham, J.P.; Matthews, S.G.; Lye, S.J.; Pennell, C.E. Characterization and Novel Analyses of Acute Stress Response Patterns in a Population-Based Cohort of Young Adults: Influence of Gender, Smoking, and BMI. Stress 2016, 19, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Smeets, T.; Cornelisse, S.; Quaedflieg, C.W.E.M.; Meyer, T.; Jelicic, M.; Merckelbach, H. Introducing the Maastricht Acute Stress Test (MAST): A Quick and Non-Invasive Approach to Elicit Robust Autonomic and Glucocorticoid Stress Responses. Psychoneuroendocrinology 2012, 37, 1998–2008. [Google Scholar] [CrossRef]
- Shilton, A.L.; Laycock, R.; Crewther, S.G. The Maastricht Acute Stress Test (MAST): Physiological and Subjective Responses in Anticipation, and Post-Stress. Front. Psychol. 2017, 8, 567. [Google Scholar] [CrossRef] [PubMed]
- Scholey, A.; Gibbs, A.; Neale, C.; Perry, N.; Ossoukhova, A.; Bilog, V.; Kras, M.; Scholz, C.; Sass, M.; Buchwald-Werner, S. Anti-Stress Effects of Lemon Balm-Containing Foods. Nutrients 2014, 6, 4805–4821. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two Formulas for Computation of the Area under the Curve Represent Measures of Total Hormone Concentration versus Time-Dependent Change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef] [PubMed]
- Quaedflieg, C.W.E.M.; Meyer, T.; van Ruitenbeek, P.; Smeets, T. Examining Habituation and Sensitization across Repetitive Laboratory Stress Inductions Using the MAST. Psychoneuroendocrinology 2017, 77, 175–181. [Google Scholar] [CrossRef]
- Maeda, S. Trait and State Self-Compassion Interactively Predict Cortisol Recovery Following an Acute Stressor in Healthy Males. Psychoneuroendocrinology 2022, 144, 105864. [Google Scholar] [CrossRef] [PubMed]
- Sturmer, L.R.; Dodd, D.; Chao, C.S.; Shi, R.Z. Clinical Utility of an Ultrasensitive Late Night Salivary Cortisol Assay by Tandem Mass Spectrometry. Steroids 2018, 129, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Perogamvros, I.; Keevil, B.G.; Ray, D.W.; Trainer, P.J. Salivary Cortisone Is a Potential Biomarker for Serum Free Cortisol. J. Clin. Endocrinol. Metab. 2010, 95, 4951–4958. [Google Scholar] [CrossRef]
- Mazidi, M.; Shemshian, M.; Mousavi, S.H.; Norouzy, A.; Kermani, T.; Moghiman, T.; Sadeghi, A.; Mokhber, N.; Ghayour-Mobarhan, M.; Ferns, G.A.A. A Double-Blind, Randomized and Placebo-Controlled Trial of Saffron (Crocus sativus L.) in the Treatment of Anxiety and Depression. J. Complement. Integr. Med. 2016, 13, 195–199. [Google Scholar] [CrossRef]
- Jafarnia, N.; Ghorbani, Z.; Nokhostin, M.; Manayi, A.; Nourimajd, S.; Jahromi, S.R. Effect of Saffron (Crocus sativus L.) as an Add-On Therapy to Sertraline in Mild to Moderate Generalized Anxiety Disorder: A Double Blind Randomized Controlled Trial. Arch. Neurosci. 2017, 4, 14332. [Google Scholar] [CrossRef]
- Moazen-Zadeh, E.; Abbasi, S.H.; Safi-Aghdam, H.; Shahmansouri, N.; Arjmandi-Beglar, A.; Hajhosseinn Talasaz, A.; Salehiomran, A.; Forghani, S.; Akhondzadeh, S. Effects of Saffron on Cognition, Anxiety, and Depression in Patients Undergoing Coronary Artery Bypass Grafting: A Randomized Double-Blind Placebo-Controlled Trial. J. Altern. Complement. Med. 2018, 24, 361–368. [Google Scholar] [CrossRef]
- Kell, G.; Rao, A.; Beccaria, G.; Clayton, P.; Inarejos-García, A.M.; Prodanov, M. Affron® a Novel Saffron Extract (Crocus sativus L.) Improves Mood in Healthy Adults over 4 Weeks in a Double-Blind, Parallel, Randomized, Placebo-Controlled Clinical Trial. Complement. Ther. Med. 2017, 33, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Pitsikas, N. Constituents of Saffron (Crocus sativus L.) as Potential Candidates for the Treatment of Anxiety Disorders and Schizophrenia. Molecules 2016, 21, 303. [Google Scholar] [CrossRef]
- Asalgoo, S.; Pirzad Jahromi, G.; Hatef, B.; Sahraei, H.; Raouf Sarshoori, J.; Sadr, S.S.; Meftahi, G.H. Saffron (Crocus sativus) Aqueous Extract Reverses the Hypothalamus-Pituitary-Adrenal Axis Activity in Rat Model of Post-Traumatic Stress Disorder. Rev. Bras. Farmacogn. 2019, 29, 470–476. [Google Scholar] [CrossRef]
- Lechtenberg, M.; Schepmann, D.; Niehues, M.; Hellenbrand, N.; Wünsch, B.; Hensel, A. Quality and Functionality of Saffron: Quality Control, Species Assortment and Affinity of Extract and Isolated Saffron Compounds to NMDA and Σ1 (Sigma-1) Receptors. Planta Med. 2008, 74, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Narang, N.; Sharma, J. Sublingual Mucosa as a Route for Systemic Drug Delivery. Int. J. Pharm. Pharm. Sci. 2011, 3 (Suppl. S2), 18–22. [Google Scholar]
- Verma, R.; Balhara, Y.P.S.; Gupta, C.S. Gender Differences in Stress Response: Role of Developmental and Biological Determinants. Ind. Psychiatry J. 2011, 20, 4. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | SD | |
|---|---|---|
| Age (years) | 22.4 | 2.0 |
| Body mass index (kg/m2) | 22.1 | 1.6 |
| Systolic blood pressure (mmHG) | 113.5 | 8.0 |
| Diastolic blood pressure (mmHG) | 72.8 | 6.4 |
| Heart rate (bpm) | 73.0 | 14.7 |
| Coffee consumption (units/day) | 0.6 | 0.9 |
| Alcohol consumption (units/day) | 0.2 | 0.5 |
| Normal sleep duration (hours) | 8.0 | 1.0 |
| Salivary cortisol change from 15 to 30 min after the MAST (%) | 94 | 59 |
| Placebo (n = 17) | Safr’InsideTM (n = 19) | Safranal (n = 18) | p-Value | |
|---|---|---|---|---|
| Salivary cortisol | ||||
| AUCt1t7 (nmol/L*min) | 58 (26) | 67 (33) | 58 (26) | 0.17 |
| Cmax (nmol/L) | 6.9 (1.9) | 7.4 (2.4) | 6.4 (1.6) | 0.90 |
| Tmax (minutes pre/post MAST) | 11 (6.0) | 26 (5.7) | 21 (4.7) | 0.04 |
| Salivary cortisone | ||||
| AUC t1t7 (nmol/L*min) | 148 (56) | 193 (78) | 161 (70) | 0.10 |
| Cmax (nmol/L) | 32 (4.0) | 32 (5.2) | 31 (4.5) | 0.52 |
| Tmax (minutes pre/post MAST) | 15 (5.8) | 31 (6.4) | 24 (4.5) | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouchieu, C.; Pourtau, L.; Brossaud, J.; Gaudout, D.; Corcuff, J.-B.; Capuron, L.; Castanon, N.; Philip, P. Acute Effect of a Saffron Extract (Safr’InsideTM) and Its Main Volatile Compound on the Stress Response in Healthy Young Men: A Randomized, Double Blind, Placebo-Controlled, Crossover Study. Nutrients 2023, 15, 2921. https://doi.org/10.3390/nu15132921
Pouchieu C, Pourtau L, Brossaud J, Gaudout D, Corcuff J-B, Capuron L, Castanon N, Philip P. Acute Effect of a Saffron Extract (Safr’InsideTM) and Its Main Volatile Compound on the Stress Response in Healthy Young Men: A Randomized, Double Blind, Placebo-Controlled, Crossover Study. Nutrients. 2023; 15(13):2921. https://doi.org/10.3390/nu15132921
Chicago/Turabian StylePouchieu, Camille, Line Pourtau, Julie Brossaud, David Gaudout, Jean-Benoit Corcuff, Lucile Capuron, Nathalie Castanon, and Pierre Philip. 2023. "Acute Effect of a Saffron Extract (Safr’InsideTM) and Its Main Volatile Compound on the Stress Response in Healthy Young Men: A Randomized, Double Blind, Placebo-Controlled, Crossover Study" Nutrients 15, no. 13: 2921. https://doi.org/10.3390/nu15132921
APA StylePouchieu, C., Pourtau, L., Brossaud, J., Gaudout, D., Corcuff, J.-B., Capuron, L., Castanon, N., & Philip, P. (2023). Acute Effect of a Saffron Extract (Safr’InsideTM) and Its Main Volatile Compound on the Stress Response in Healthy Young Men: A Randomized, Double Blind, Placebo-Controlled, Crossover Study. Nutrients, 15(13), 2921. https://doi.org/10.3390/nu15132921