

Does Vitamin Supplementation Play a Role in Chronic Kidney Disease?
Abstract
1. Introduction
2. Chronic Kidney Disease
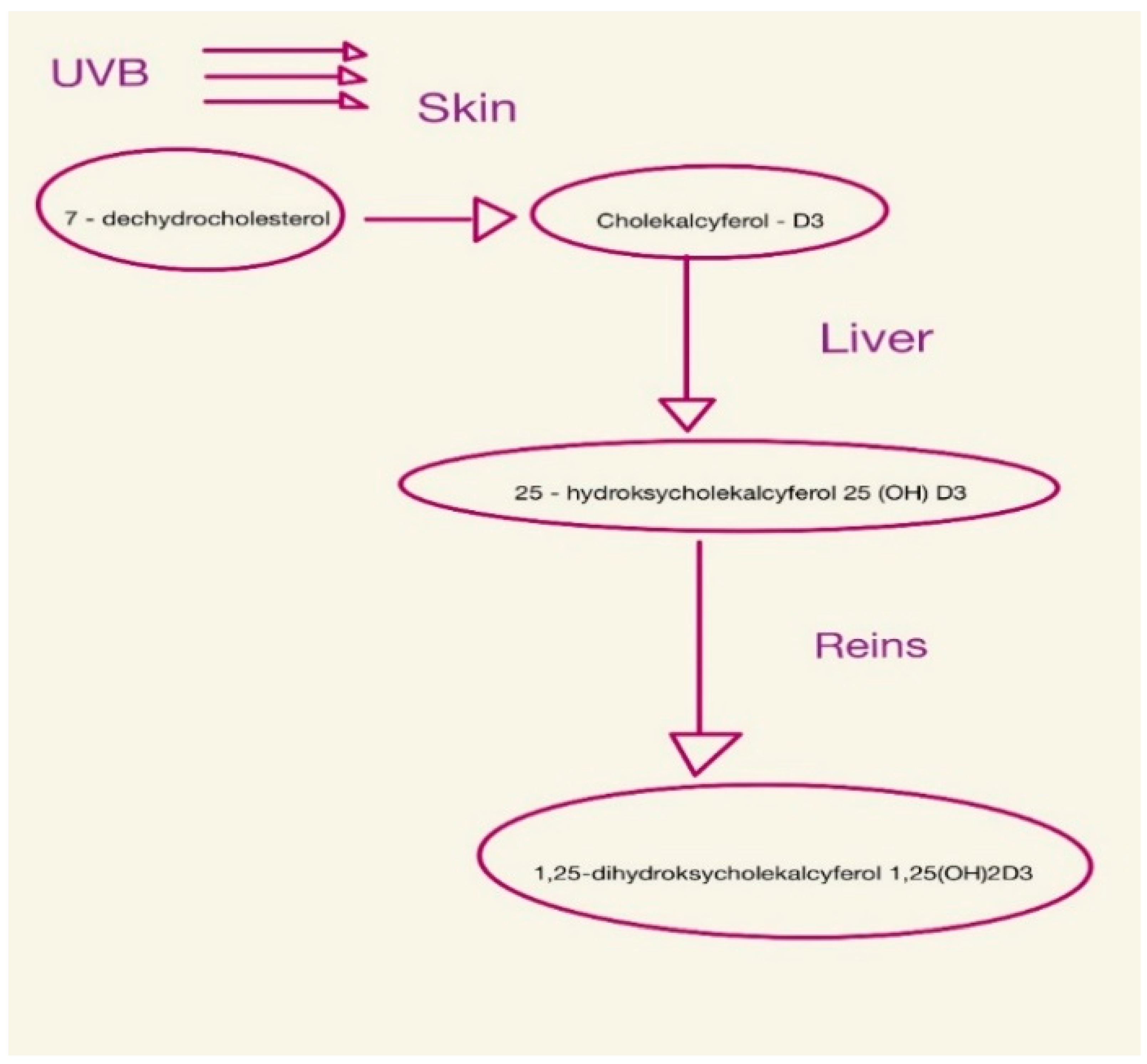
3. The Effects of Vitamin D on Chronic Kidney Disease
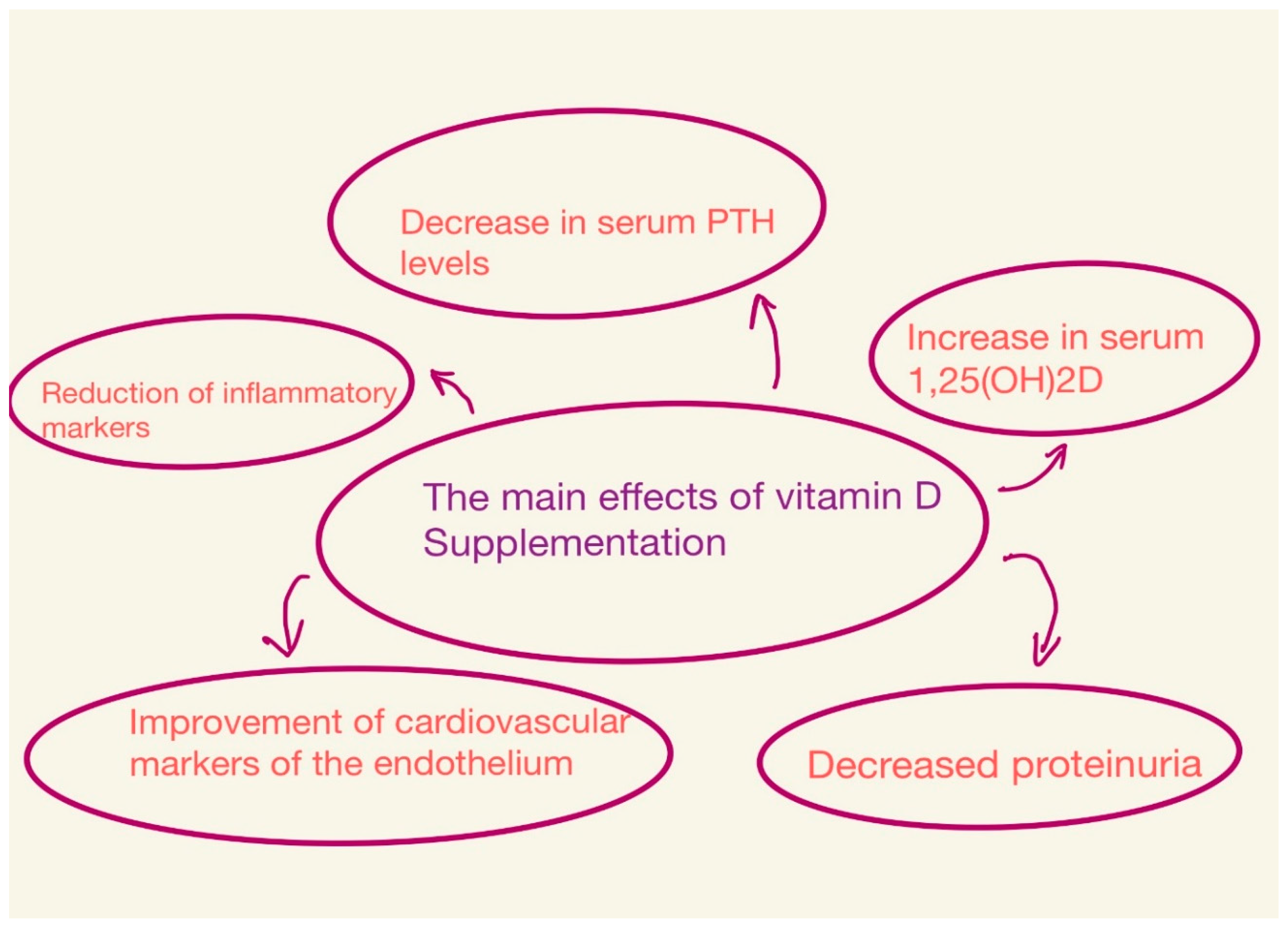
Vitamin D Supplementation
4. Effect and Supplementation of B Vitamins
4.1. Thiamine—B1
4.2. Riboflavin—B2
4.3. Niacin—B3
4.4. Pyridoxine—B6
4.5. Cobalamin—B12
4.6. Folic Acid—B9
5. Vitamin C
6. Vitamin A
7. Vitamin E
8. Vitamin K
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kestenbaum, B.; Belozeroff, V. Mineral Metabolism Disturbances in Patients with Chronic Kidney Disease. Eur. J. Clin. Investig. 2007, 37, 607–622. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Anderson, J.E.; Kalantar-Zadeh, K. Paradoxical Association between Body Mass Index and Mortality in Men with CKD Not Yet on Dialysis. Am. J. Kidney Dis. 2007, 49, 581–591. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Kilpatrick, R.D.; McAllister, C.J.; Shinaberger, C.S.; Gjertson, D.W.; Greenland, S. Association of Morbid Obesity and Weight Change over Time with Cardiovascular Survival in Hemodialysis Population. Am. J. Kidney Dis. 2005, 46, 489–500. [Google Scholar] [CrossRef]
- Karamouzis, I.; Sarafidis, P.A.; Karamouzis, M.; Iliadis, S.; Haidich, A.B.; Sioulis, A.; Triantos, A.; Vavatsi-Christaki, N.; Grekas, D.M. Increase in Oxidative Stress but Not in Antioxidant Capacity with Advancing Stages of Chronic Kidney Disease. Am. J. Nephrol. 2008, 28, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Kędzierska-Kapuza, K.; Szczuko, U.; Stolińska, H.; Bakaloudi, D.R.; Wierzba, W.; Szczuko, M. Demand for Water-Soluble Vitamins in a Group of Patients with CKD versus Interventions and Supplementation—A Systematic Review. Nutrients 2023, 15, 860. [Google Scholar] [CrossRef] [PubMed]
- Schlieper, G.; Schurgers, L.; Brandenburg, V.; Reutelingsperger, C.; Floege, J. Vascular Calcification in Chronic Kidney Disease: An Update. Nephrol. Dial. Transplant. 2016, 31, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Coveney, N.; Polkinghorne, K.R.; Linehan, L.; Corradini, A.M.; Kerr, P.G. Water-Soluble Vitamin Levels in Extended Hours Hemodialysis. Hemodial. Int. 2011, 15, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Chazot, C.; Jean, G.; Kopple, J.D. Can Outcomes Be Improved in Dialysis Patients by Optimizing Trace Mineral, Micronutrient, and Antioxidant Status?: The Impact of Vitamins and Their Supplementation. Semin. Dial. 2016, 29, 39–48. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Qazi, R.A.; González, E.A.; Zeringue, A.; Martin, K.J. Changes in Serum 25-Hydroxyvitamin D and Plasma Intact PTH Levels Following Treatment with Ergocalciferol in Patients with CKD. Am. J. Kidney Dis. 2007, 50, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Steiber, A.L.; Kopple, J.D. Vitamin Status and Needs for People with Stages 3-5 Chronic Kidney Disease. J. Ren. Nutr. 2011, 21, 355–368. [Google Scholar] [CrossRef]
- de Vriese, A.S.; Caluwé, R.; Pyfferoen, L.; de Bacquer, D.; de Boeck, K.; Delanote, J.; de Surgeloose, D.; van Hoenacker, P.; van Vlem, B.; Verbeke, F. Multicenter Randomized Controlled Trial of Vitamin K Antagonist Replacement by Rivaroxaban with or without Vitamin K2 in Hemodialysis Patients with Atrial Fibrillation: The Valkyrie Study. J. Am. Soc. Nephrol. 2020, 31, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Fissell, R.B.; Bragg-Gresham, J.L.; Gillespie, B.W.; Goodkin, D.A.; Bommer, J.; Saito, A.; Akiba, T.; Port, F.K.; Young, E.W. International Variation in Vitamin Prescription and Association with Mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2004, 44, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Descombes, E.; Hanck, A.B.; Fellay, G. Water Soluble Vitamins in Chronic Hemodialysis Patients and Need for Supplementation. Kidney Int. 1993, 43, 1319–1328. [Google Scholar] [CrossRef]
- Corken, M.; Porter, J. Is Vitamin B 6 Deficiency an Under-Recognized Risk in Patients Receiving Haemodialysis? A Systematic Review: 2000–2010. Nephrology 2011, 16, 619–625. [Google Scholar] [CrossRef] [PubMed]
- La Russa, D.; Pellegrino, D.; Montesanto, A.; Gigliotti, P.; Perri, A.; Russa, A.L.; Bonofiglio, R. Oxidative Balance and Inflammation in Hemodialysis Patients: Biomarkers of Cardiovascular Risk? Oxidative Med. Cell. Longev. 2019, 2019, 8567275. [Google Scholar] [CrossRef] [PubMed]
- Cianciolo, G.; De Pascalis, A.; Di Lullo, L.; Ronco, C.; Zannini, C.; La Manna, G. Folic Acid and Homocysteine in Chronic Kidney Disease and Cardiovascular Disease Progression: Which Comes First? Cardiorenal Med. 2017, 7, 255–266. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Fried, L.F.; Shlipak, M.G.; Crump, C.; Bleyer, A.J.; Gottdiener, J.S.; Kronmal, R.A.; Kuller, L.H.; Newman, A.B. Renal Insufficiency as a Predictor of Cardiovascular Outcomes and Mortality in Elderly Individuals. J. Am. Coll. Cardiol. 2003, 41, 1364–1372. [Google Scholar] [CrossRef]
- Angelini, A.; Cappuccilli, M.L.; Magnoni, G.; Chiocchini, A.L.C.; Aiello, V.; Napoletano, A.; Iacovella, F.; Troiano, A.; Mancini, R.; Capelli, I.; et al. The link between homocysteine, folic acid and vitamin B12 in chronic kidney disease. G. Ital. Nefrol. 2021, 38, 1–17. [Google Scholar]
- Cianciolo, G.; La Manna, G.; Colì, L.; Donati, G.; D’Addio, F.; Persici, E.; Comai, G.; Wratten, M.; Dormi, A.; Mantovani, V.; et al. 5-Methyltetrahydrofolate Administration Is Associated with Prolonged Survival and Reduced Inflammation in ESRD Patients. Am. J. Nephrol. 2008, 28, 941–948. [Google Scholar] [CrossRef]
- Bhan, I.; Thadhani, R. Vitamin D Therapy for Chronic Kidney Disease. Semin. Nephrol. 2009, 29, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Zisman, A.L.; Hristova, M.; Ho, L.T.; Sprague, S.M. Impact of Ergocalciferol Treatment of Vitamin D Deficiency on Serum Parathyroid Hormone Concentrations in Chronic Kidney Disease. Am. J. Nephrol. 2007, 27, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.M.; Rothwell, P.M. Prevention and Treatment of Stroke in Patients with Chronic Kidney Disease: An Overview of Evidence and Current Guidelines. Kidney Int. 2020, 97, 266–278. [Google Scholar] [CrossRef]
- Eckardt, K.U.; Bansal, N.; Coresh, J.; Evans, M.; Grams, M.E.; Herzog, C.A.; James, M.T.; Heerspink, H.J.L.; Pollock, C.A.; Stevens, P.E.; et al. Improving the Prognosis of Patients with Severely Decreased Glomerular Filtration Rate (CKD G4+): Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2018, 93, 1281–1292. [Google Scholar] [CrossRef] [PubMed]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Dounousi, E.; Mertens, P.R. Oxidative Stress in Hemodialysis Patients: A Review of the Literature. Oxidative Med. Cell. Longev. 2017, 2017, 3081856. [Google Scholar] [CrossRef]
- Kandula, P.; Dobre, M.; Schold, J.D.; Schreiber, M.J.; Mehrotra, R.; Navaneethan, S.D. Vitamin D Supplementation in Chronic Kidney Disease: A Systematic Review and Meta-Analysis of Observational Studies and Randomized Controlled Trials. Clin. J. Am. Soc. Nephrol. 2011, 6, 50–62. [Google Scholar] [CrossRef]
- Jankowska, M.; Rutkowski, B.; Dębska-Ślizień, A. Vitamins and Microelement Bioavailability in Different Stages of Chronic Kidney Disease. Nutrients 2017, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Weekers, L.; Warling, X.; Moonen, M.; Smelten, N.; Médart, L.; Krzesinski, J.M.; Cavalier, E. Cholecalciferol in Haemodialysis Patients: A Randomized, Double-Blind, Proof-of-Concept and Safety Study. Nephrol. Dial. Transplant. 2013, 28, 1779–1786. [Google Scholar] [CrossRef]
- DeVille, J.; Thorp, M.L.; Tobin, L.; Gray, E.; Johnson, E.S.; Smith, D.H. Effect of Ergocalciferol Supplementation on Serum Parathyroid Hormone and Serum 25-Hydroxyvitamin D in Chronic Kidney Disease. Nephrology 2006, 11, 555–559. [Google Scholar] [CrossRef]
- Jean, G.; Terrat, J.C.; Vanel, T.; Hurot, J.M.; Lorriaux, C.; Mayor, B.; Chazot, C. Evidence for Persistent Vitamin D 1-Alpha-Hydroxylation in Hemodialysis Patients: Evolution of Serum 1,25-Dihydroxycholecalciferol after 6 Months of 25-Hydroxycholecalciferol Treatment. Nephron Clin. Pr. 2008, 110, c58–c65. [Google Scholar] [CrossRef]
- Armas, L.A.G.; Hollis, B.W.; Heaney, R.P. Vitamin D2 Is Much Less Effective than Vitamin D3 in Humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed]
- Wissing, K.M.; Broeders, N.; Moreno-Reyes, R.; Gervy, C.; Stallenberg, B.; Abramowicz, D. A Controlled Study of Vitamin D3 to Prevent Bone Loss in Renal-Transplant Patients Receiving Low Doses of Steroids. Transplantation 2005, 79, 108–115. [Google Scholar] [CrossRef]
- Okša, A.; Spustová, V.; Krivošíková, Z.; Gazdíková, K.; Fedelešová, V.; Lajdová, I.; Štefíková, K.; Bernasovská, G.; Žilinská, Z.; Dzúrik, R. Effects of Long-Term Cholecalciferol Supplementation on Mineral Metabolism and Calciotropic Hormones in Chronic Kidney Disease. Kidney Blood Press. Res. 2008, 31, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Ravani, P.; Malberti, F.; Tripepi, G.; Pecchini, P.; Cutrupi, S.; Pizzini, P.; Mallamaci, F.; Zoccali, C. Vitamin D Levels and Patient Outcome in Chronic Kidney Disease. Kidney Int. 2009, 75, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Filipov, J.J.; Zlatkov, B.K.; Dimitrov, E.P.; Svinarov, D. Relationship between Vitamin D Status and Immunosuppressive Therapy in Kidney Transplant Recipients. Biotechnol. Biotechnol. Equip. 2015, 29, 331–335. [Google Scholar] [CrossRef]
- Blair, D.; Byham-Gray, L.; Lewis, E.; McCaffrey, S. Prevalence of Vitamin D [25(OH)D] Deficiency and Effects of Supplementation with Ergocalciferol (Vitamin D2) in Stage 5 Chronic Kidney Disease Patients. J. Ren. Nutr. 2008, 18, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Iodice, S.; Zittermann, A.; Grant, W.B.; Gandini, S. Vitamin D Status and Mortality Risk in CKD: A Meta-Analysis of Prospective Studies. Am. J. Kidney Dis. 2011, 58, 374–382. [Google Scholar] [CrossRef]
- Alp Ikizler, T.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Jordi Goldstein-Fuchs, D.; et al. Kdoqi clinical practice guideline for nutrition in ckd: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Thadhani, R. Is Calcitriol Life-Protective for Patients with Chronic Kidney Disease? J. Am. Soc. Nephrol. 2009, 20, 2285–2290. [Google Scholar] [CrossRef]
- Holick, M.F.; Biancuzzo, R.M.; Chen, T.C.; Klein, E.K.; Young, A.; Bibuld, D.; Reitz, R.; Salameh, W.; Ameri, A.; Tannenbaum, A.D. Vitamin D2 Is as Effective as Vitamin D3 in Maintaining Circulating Concentrations of 25-Hydroxyvitamin D. J. Clin. Endocrinol. Metab. 2008, 93, 677–681. [Google Scholar] [CrossRef]
- Chandra, P.; Nilo, J.; Binongo, G.; Ziegler, T.R.; Schlanger, L.E.; Wang, W.; Someren, J.T.; Tangpricha, V. Cholecalciferol (vita min d 3) therapy and vitamin d insufficiency in patients with chronic kidney disease: A randomized controlled pilot study. Endocr. Pract. 2008, 14, 10–17. [Google Scholar] [CrossRef]
- Tokmak, F.; Quack, I.; Schieren, G.; Sellin, L.; Rattensperger, D.; Holland-Letz, T.; Weiner, S.M.; Rump, L.C. High-Dose Cholecalciferol to Correct Vitamin D Deficiency in Haemodialysis Patients. Nephrol. Dial. Transplant. 2008, 23, 4016–4020. [Google Scholar] [CrossRef] [PubMed]
- Courbebaisse, M.; Thervet, E.; Souberbielle, J.C.; Zuber, J.; Eladari, D.; Martinez, F.; Mamzer-Bruneel, M.F.; Urena, P.; Legendre, C.; Friedlander, G.; et al. Effects of Vitamin D Supplementation on the Calcium-Phosphate Balance in Renal Transplant Patients. Kidney Int. 2009, 75, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Matias, P.J.; Jorge, C.; Ferreira, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. Cholecalciferol Supplementation in Hemodialysis Patients: Effects on Mineral Metabolism, Inflammation, and Cardiac Dimension Parameters. Clin. J. Am. Soc. Nephrol. 2010, 5, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Bernardini, J.; Piraino, B. Prevalence and correction of 25(oh) vitamin d deficiency in peritoneal dialysis patients. Perit. Dial. Int. 2005, 25, 362–366. [Google Scholar] [CrossRef]
- Saab, G.; Young, D.O.; Gincherman, Y.; Giles, K.; Norwood, K.; Coyne, D.W. Prevalence of Vitamin D Deficiency and the Safety and Effectiveness of Monthly Ergocalciferol in Hemodialysis Patients. Nephron Clin. Pr. 2007, 105, c132–c138. [Google Scholar] [CrossRef]
- Moe, S.M.; Saifullah, A.; LaClair, R.E.; Usman, S.A.; Yu, Z. A Randomized Trial of Cholecalciferol versus Doxercalciferol for Lowering Parathyroid Hormone in Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 299–306. [Google Scholar] [CrossRef]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Monthly Cholecalciferol Administration in Haemodialysis Patients: A Simple and Efficient Strategy for Vitamin D Supplementation. Nephrol. Dial. Transplant. 2009, 24, 3799–3805. [Google Scholar] [CrossRef]
- Dogan, E.; Erkoc, R.; Sayarlioglu, H.; Soyoral, Y.; Dulger, H. Effect of Depot Oral Cholecalciferol Treatment on Secondary Hyperparathyroidism in Stage 3 and Stage 4 Chronic Kidney Diseases Patients. Ren. Fail. 2008, 30, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Vitamin D in Chronic Kidney Disease and Dialysis Patients. Nutrients 2017, 9, 328. [Google Scholar] [CrossRef]
- Don, T.; Friedlander, S.; Wong, W. Dietary Intakes and Biochemical Status of B Vitamins in a Group of Children Receiving Dialysis. J. Ren. Nutr. 2010, 20, 23–28. [Google Scholar] [CrossRef] [PubMed]
- House, A.A.; Eliasziw, M.; Cattran, D.C.; Churchill, D.N.; Oliver, M.J.; Fine, A.; Dresser, G.K.; David Spence, J. Effect of B-Vitamin Therapy on Progression of Diabetic Nephropathy A Randomized Controlled Trial. JAMA 2010, 303, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, F.J.; Moradi, H.; Gollapudi, P.; Ju Kim, H.; Vaziri, N.D.; Said, H.M. Effect of Chronic Kidney Disease on the Expression of Thiamin and Folic Acid Transporters. Nephrol. Dial. Transplant. 2011, 26, 2137–2144. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.; Czeche, K.; Bitsch, R.; Stein, G. Assessment of Thiamin Status in Chronic Renal Failure, Transplant Recipients and Hemodialysis Patients a Multivitamin. Int. J. Vitam. Nutr. Res. 2000, 70, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.C.; Hung, S.H.; Tarng, D.C.; Yang, W.C.; Chen, T.W.; Huang, T.P. Thiamine Deficiency and Unexplained Encephalopathy in Hemodialysis and Peritoneal Dialysis Patients. Am. J. Kidney Dis. 2001, 38, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Saka, Y.; Naruse, T.; Kato, A.; Tawada, N.; Noda, Y.; Mimura, T.; Watanabe, Y. Thiamine Status in End-Stage Chronic Kidney Disease Patients: A Single-Center Study. Int. Urol. Nephrol. 2018, 50, 1913–1918. [Google Scholar] [CrossRef] [PubMed]
- Suwannasom, N.; Kao, I.; Pruß, A.; Georgieva, R.; Bäumler, H. Riboflavin: The Health Benefits of a Forgotten Natural Vitamin. Int. J. Mol. Sci. 2020, 21, 950. [Google Scholar] [CrossRef]
- Fischer, M.; Bacher, A. Biosynthesis of Vitamin B2: Structure and Mechanism of Riboflavin Synthase. Arch. Biochem. Biophys. 2008, 474, 252–265. [Google Scholar] [CrossRef]
- Porrini, M.; Simonetti, P.; Ciappellano, S.; Testolin, G.; Gentile, M.; Manna, G.; Fellin, G.; D’Amico, G. Thiamin, Riboflavin and Pyridoxine Status in Chronic Renal Insufficiency. Int. J. Vitam. Nutr. Res. 1989, 59, 4–8. [Google Scholar] [CrossRef]
- Berns, J.S. Niacin and Related Compounds for Treating Hyperphosphatemia in Dialysis Patients. Semin. Dial. 2008, 21, 203–205. [Google Scholar] [CrossRef]
- Rennick, A.; Kalakeche, R.; Seel, L.; Shepler, B. Nicotinic Acid and Nicotinamide: A Review of Their Use for Hyperphosphatemia in Dialysis Patients. Pharmacotherapy 2013, 33, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.C.; Young, D.O.; Huang, Y.; Delmez, J.A.; Coyne, D.W. A Randomized, Double-Blind, Placebo-Controlled Trial of Niacinamide for Reduction of Phosphorus in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.J.; Kim, D.K.; Lee, S.M.; Kim, K.H.; Han, S.H.; Kim, K.H.; Kim, S.E.; Son, Y.K.; An, W.S. Effects of Low-Dose Niacin on Dyslipidemia and Serum Phosphorus in Patients with Chronic Kidney Disease. Kidney Res. Clin. Pract. 2013, 32, 21–26. [Google Scholar] [CrossRef]
- Kopple, J.D.; Mercurio, K.; Blumenkrantz, M.J.; Jones, M.R.; Tallos, J.; Roberts, C.; Card, B.; Saltzman, R.; Casciato, D.A.; Swendseid, M.E. Daily Requirement for Pyridoxine Supplements in Chronic Renal Failure. Kidney Int. 1981, 19, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Podda, G.M.; Lussana, F.; Moroni, G.; Faioni, E.M.; Lombardi, R.; Fontana, G.; Ponticelli, C.; Maioli, C.; Cattaneo, M. Abnormalities of Homocysteine and B Vitamins in the Nephrotic Syndrome. Thromb. Res. 2007, 120, 647–652. [Google Scholar] [CrossRef]
- Capelli, I.; Cianciolo, G.; Gasperoni, L.; Zappulo, F.; Tondolo, F.; Cappuccilli, M.; La Manna, G. Folic Acid and Vitamin B12 Administration in CKD, Why Not? Nutrients 2019, 11, 383. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.H.L.; Wang, A.Y.M. Vitamin B12 and Chronic Kidney Disease. Vitam. Horm. 2022, 119, 325–353. [Google Scholar] [CrossRef]
- Jamison, R.L.; Hartigan, P.; Kaufman, J.S.; Goldfarb, D.S.; Warren, S.R.; Guarino, P.D.; Gaziano, J.M. Effect of Homocysteine Lowering on Mortality and Vascular Disease in Advanced Chronic Kidney Disease and End-Stage Renal Disease A Randomized Controlled Trial. JAMA 2007, 298, 1163–1170. [Google Scholar] [CrossRef]
- Dastidar, R.; Sikder, K. Diagnostic Reliability of Serum Active B12 (Holo-Transcobalamin) in True Evaluation of Vitamin B12 Deficiency: Relevance in Current Perspective. BMC Res. Notes 2022, 15, 329. [Google Scholar] [CrossRef]
- Heinz, J.; Kropf, S.; Domröse, U.; Westphal, S.; Borucki, K.; Luley, C.; Neumann, K.H.; Dierkes, J. B Vitamins and the Risk of Total Mortality and Cardiovascular Disease in End-Stage Renal Disease: Results of a Randomized Controlled Trial. Circulation 2010, 121, 1432–1438. [Google Scholar] [CrossRef]
- Huo, Y.; Li, J.; Qin, X.; Huang, Y.; Wang, X.; Gottesman, R.F.; Tang, G.; Wang, B.; Chen, D.; He, M.; et al. Efficacy of Folic Acid Therapy in Primary Prevention of Stroke among Adults with Hypertension in China: The CSPPT Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2015, 313, 1325–1335. [Google Scholar] [CrossRef]
- Deicher, R.; Hörl, W.H. Vitamin C in Chronic Kidney Disease and Hemodialysis Patients. Kidney Blood Press. Res. 2003, 26, 100–106. [Google Scholar] [CrossRef]
- Chaghouri, P.; Maalouf, N.; Peters, S.L.; Nowak, P.J.; Peczek, K.; Zasowska-Nowak, A.; Nowicki, M. Two Faces of Vitamin C in Hemodialysis Patients: Relation to Oxidative Stress and Inflammation. Nutrients 2021, 13, 791. [Google Scholar] [CrossRef]
- Martins, M.L.; da Silva, A.T.; Machado, R.P.; Ramos, H.P.; Martinelli, C.; Silveira, T.T.; da Silva, E.L.; Wazlawik, E. Vitamin C Decreases Reduced Glutathione in Chronic Haemodialysis Patients: A Pilot, Randomised, Double-Blind Trial. Int. Urol. Nephrol. 2021, 53, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Morena, M.; Cristol, J.-P.; Bosc, J.-Y.; Tetta, C.; Forret, G.; Leger, C.-L.; Delcourt, C.; Papoz, L.; Descomps, B.; Canaud, B.; et al. Convective and Diffusive Losses of Vitamin C during Haemodiafiltration Session: A Contributive Factor to Oxidative Stress in Haemodialysis Patients. Nephrol. Dial. Transplant. 2002, 17, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Canavese, C.; Petrarulo, M.; Massarenti, P.; Berutti, S.; Fenoglio, R.; Pauletto, D.; Lanfranco, G.; Bergamo, D.; Sandri, L.; Marangella, M. Long-Term, Low-Dose, Intravenous Vitamin C Leads to Plasma Calcium Oxalate Supersaturation in Hemodialysis Patients. Am. J. Kidney Dis. 2005, 45, 540–549. [Google Scholar] [CrossRef]
- Böhm, F.; Tiroke, K.; Schneider, S.; Sperschneider, H.; Stein, G.; Bitsch, R. Vitamin C Status of Patients with Chronic Renal Failure, Dialysis Patients and Patients after Renal Transplantation. Int. J. Vitam. Nutr. Res. 1997, 67, 2–6. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, L.; Cheng, X.; Dong, J.; Geng, Q.; Zuo, L. Low Levels of Vitamin C in Dialysis Patients Is Associated with Decreased Prealbumin and Increased C-Reactive Protein. BMC Nephrol. 2011, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Raimann, J.G.; Levin, N.W.; Craig, R.G.; Sirover, W.; Kotanko, P.; Handelman, G. Is Vitamin C Intake Too Low in Dialysis Patients? Semin. Dial. 2013, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sarandol, E.; Erdinc, S.; Senol, E.; Ersoy, A.; Surmen-Gur, E. Effects of Vitamin C Supplementation on Oxidative Stress and Serum Paraoxonase/Arylesterase Activities in Patients on Long-Term Hemodialysis. Nefrologia 2022. [Google Scholar] [CrossRef]
- Omar, S.; El Borolossy, R.M.; Elsaid, T.; Sabri, N.A. Evaluation of the Combination Effect of Rutin and Vitamin C Supplementation on the Oxidative Stress and Inflammation in Hemodialysis Patients. Front. Pharm. 2022, 13, 961590. [Google Scholar] [CrossRef] [PubMed]
- Fumeron, C.; Nguyen-Khoa, T.; Saltiel, C.; Kebede, M.; Buisson, C.; Drüeke, T.B.; Lacour, B.; Massy, Z.A. Effects of Oral Vitamin C Supplementation on Oxidative Stress and Inflammation Status in Haemodialysis Patients. Nephrol. Dial. Transplant. 2005, 20, 1874–1879. [Google Scholar] [CrossRef]
- Rojo-Trejo, M.H.; Robles-Osorio, M.L.; Sabath, E. Liposoluble Vitamins A and E in Kidney Disease. World J. Nephrol. 2022, 11, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Manickavasagar, B.; McArdle, A.J.; Yadav, P.; Shaw, V.; Dixon, M.; Blomhoff, R.; O’Connor, G.; Rees, L.; Ledermann, S.; van’t Hoff, W.; et al. Hypervitaminosis A Is Prevalent in Children with CKD and Contributes to Hypercalcemia. Pediatr. Nephrol. 2014, 30, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Frey, S.K.; Nagl, B.; Henze, A.; Raila, J.; Schlosser, B.; Berg, T.; Tepel, M.; Zidek, W.; Weickert, M.O.; Pfeiffer, A.F.H.; et al. Isoforms of Retinol Binding Protein 4 (RBP4) Are Increased in Chronic Diseases of the Kidney but Not of the Liver. Lipids Health Dis. 2008, 7, 29. [Google Scholar] [CrossRef]
- Espe, K.M.; Raila, J.; Henze, A.; Krane, V.; Schweigert, F.J.; Hocher, B.; Wanner, C.; Drechsler, C. Impact of Vitamin A on Clinical Outcomes in Haemodialysis Patients. Nephrol. Dial. Transplant. 2011, 26, 4054–4061. [Google Scholar] [CrossRef]
- Miller Iii, E.R.; Pastor-Barriuso, R.; Dalal, D.; Riemersma, R.A.; Appel, L.J.; Guallar, E. Meta-Analysis: High-Dosage Vitamin E Supplementation May Increase All-Cause Mortality Background: Experimental Models and Observational Studies. Ann. Intern. Med. 2005, 142, 37–46. [Google Scholar] [CrossRef]
- Lonn, E.; Bosch, J.; Yusuf, S.; Sheridan, P.; Pogue, J.; Arnold, J.M.; Ross, C.; Arnold, A.; Sleight, P.; Probstfield, J.; et al. Effects of Long-Term Vitamin E Supplementation on Cardiovascular Events and Cancer A Randomized Controlled Trial. JAMA 2005, 293, 1338–1347. [Google Scholar] [PubMed]
- Galli, F.; Buoncristiani, U.; Conte, C.; Aisa, C.; Floridi, A. Vitamin E in Uremia and Dialysis Patients. Ann. N. Y. Acad. Sci. 2004, 1031, 348–351. [Google Scholar] [CrossRef]
- Nanayakkara, P.W.B.; Kiefte-de Jong, J.C.; ter Wee, P.M.; Stehouwer, C.D.A.; van Ittersum, F.J.; Olthof, M.R.; Teerlink, T.; Twisk, J.W.R.; van Guldener, C.; Smulders, Y.M. Randomized Placebo-Controlled Trial Assessing a Treatment Strategy Consisting of Pravastatin, Vitamin E, and Homocysteine Lowering on Plasma Asymmetric Dimethylarginine Concentration in Mild to Moderate CKD. Am. J. Kidney Dis. 2009, 53, 41–50. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Lonn, E.M.; Yi, Q.; Gerstein, H.C.; Hoogwerf, B.J.; Pogue, J.; Bosch, J.; Dagenais, G.R.; Yusuf, S. Effects of Vitamin E on Cardiovascular Outcomes in People with Mild-to-Moderate Renal Insufficiency: Results of the HOPE Study. Kidney Int. 2004, 65, 1375–1380. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Sheridan, P.; McQueen, M.J.; Held, C.; Arnold, J.M.O.; Fodor, G.; Yusuf, S.; Lonn, E.M. Homocysteine Lowering with Folic Acid and B Vitamins in People with Chronic Kidney Disease—Results of the Renal Hope-2 Study. Nephrol. Dial. Transplant. 2008, 23, 645–653. [Google Scholar] [CrossRef]
- Brandenburg, V.M.; Reinartz, S.; Kaesler, N.; Krüger, T.; Dirrichs, T.; Kramann, R.; Peeters, F.; Floege, J.; Keszei, A.; Marx, N.; et al. Slower Progress of Aortic Valve Calcification with Vitamin K Supplementation: Results from a Prospective Interventional Proof-of-Concept Study. Circulation 2017, 135, 2081–2083. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.J.; Booth, S.L.; Hopman, W.M.; Holden, R.M. Assessment of Potential Biomarkers of Subclinical Vitamin K Deficiency in Patients with End-Stage Kidney Disease. Can. J. Kidney Health Dis. 2014, 1, 13. [Google Scholar] [CrossRef]
- Grzejszczak, P.; Kurnatowska, I. Role of Vitamin K in CKD: Is Its Supplementation Advisable in CKD Patients? Kidney Blood Press. Res. 2021, 46, 523–530. [Google Scholar] [CrossRef]
- Fulton, R.L.; McMurdo, M.E.; Hill, A.; Abboud, R.J.; Arnold, G.; Struthers, A.; Khan, F.; Vermeer, C.; Knapen, M.H.; Drummen, N.E.; et al. Effect of Vitamin K on Vascular Health and Physical Function in Older People with Vascular Disease—A Randomised Controlled Trial. J. Nutr. Health Aging. 2016, 20, 25–33. [Google Scholar] [CrossRef]
- Holden, R.M.; Morton, A.R.; Garland, J.S.; Pavlov, A.; Day, A.G.; Booth, S.L. Vitamins K and D Status in Stages 3-5 Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Westenfeld, R.; Krueger, T.; Schlieper, G.; Cranenburg, E.C.M.; Magdeleyns, E.J.; Heidenreich, S.; Holzmann, S.; Vermeer, C.; Jahnen-Dechent, W.; Ketteler, M.; et al. Effect of Vitamin K 2 Supplementation on Functional Vitamin K Deficiency in Hemodialysis Patients: A Randomized Trial. Am. J. Kidney Dis. 2012, 59, 186–195. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Vitamins | HD Losses | European Guidelines for HD Patients | Risk of Toxicity |
|---|---|---|---|
| D | No | No | Yes |
| B1 | 13–40 mL/min | 1.1–1.2 mg | No |
| B2 | 27–52 mL/min | 1.1–1.3 mg | No |
| B3 | Very low | 14–16 mg | No data |
| B6 | 54–173 mL/min | 10 mg | Yes |
| B9 | 135 mL/min | 1 mg | Yes |
| B12 | Controversial | 2.4 lg | No data |
| C | 80–280 mg/session | 75–90 mg | Yes |
| A | No | No | Yes |
| E | No | 400–800 IU | Possible |
| K | No data | No | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juszczak, A.B.; Kupczak, M.; Konecki, T. Does Vitamin Supplementation Play a Role in Chronic Kidney Disease? Nutrients 2023, 15, 2847. https://doi.org/10.3390/nu15132847
Juszczak AB, Kupczak M, Konecki T. Does Vitamin Supplementation Play a Role in Chronic Kidney Disease? Nutrients. 2023; 15(13):2847. https://doi.org/10.3390/nu15132847
Chicago/Turabian StyleJuszczak, Aleksandra Beata, Maciej Kupczak, and Tomasz Konecki. 2023. "Does Vitamin Supplementation Play a Role in Chronic Kidney Disease?" Nutrients 15, no. 13: 2847. https://doi.org/10.3390/nu15132847
APA StyleJuszczak, A. B., Kupczak, M., & Konecki, T. (2023). Does Vitamin Supplementation Play a Role in Chronic Kidney Disease? Nutrients, 15(13), 2847. https://doi.org/10.3390/nu15132847