

Family Mealtimes: A Systematic Umbrella Review of Characteristics, Correlates, Outcomes and Interventions


Abstract
1. Introduction
- What are the characteristics of family mealtimes?
- What are the correlates of family mealtimes?
- What outcomes, if any, are family mealtimes associated with?
- Are interventions aimed at promoting family mealtimes effective?
2. Materials and Methods
2.1. Eligibility Criteria and Information Source
- Systematic reviews with or without meta-analysis and/or meta-synthesis;
- Systematic reviews of studies whose participants included families comprising children and/or adolescents aged from birth to 18 years (PICO Population);
- Systematic reviews that reported at least one aspect of family mealtimes (characteristics, correlates, outcomes or interventions) (PICO Intervention, Comparison and Outcome);
- Peer-reviewed;
- English Language.
- Systematic reviews of studies whose participants were restricted to adults aged >18 years;
- Systematic reviews of studies in which only non-family meals were investigated e.g., eating at school;
- Systematic reviews of studies investigating breakfast consumption if the focus was exclusively on the nutrition associated with consuming breakfast rather than breakfast as a family mealtime;
- Systematic reviews of studies whose participants were families with children/adolescents with a medical condition that may affect their eating, for example, Type 1 or Type 2 diabetes; eating disorders (e.g., anorexia); feeding or food intake disorders or difficulties; Autism Spectrum Disorder (ASD); Attention Deficit Hyperactivity Disorder (ADHD);
- Systematic reviews of studies where participants were restricted to adolescents/children who were overweight;
- Systematic reviews of studies in which participants were restricted to parents with eating disorders;
- Primary studies reporting original data;
- Non-systematic reviews e.g., scoping reviews;
- Commentaries, editorials, position papers.
2.2. Search Selection
- Exclusion of systematic reviews that focused on families with children/adolescents with a medical condition that may affect their eating (see exclusion criteria for detail);
- The inclusion of “review” as a search term in the title but not in the abstract; doing so resulted in the inclusion of articles that described reviewing the literature but were not reviews. Meta-analysis and meta-synthesis were searched for in both the title and the abstract.
2.3. Data Extraction
- Authors and year of publication;
- Key search criteria: dates of review; age of participants; designs included/excluded;
- Systematic review question(s);
- Conceptualisation, definition and/or operationalisation of family mealtimes and other constructs relevant to the article;
- Key systematic review characteristics: design; number of articles/studies; quality;
- Key findings and limitations relevant to family mealtime research.
2.4. Assessment of Quality and Risk of Bias
2.5. Data Synthesis
- Characteristics of family mealtimes;
- Correlates of family mealtimes;
- Outcomes predicted by family mealtimes;
- Interventions aimed at promoting family mealtimes.
3. Results
3.1. Search Results
3.2. Characteristics of the Included Systematic Reviews
3.2.1. Constructs Assessed
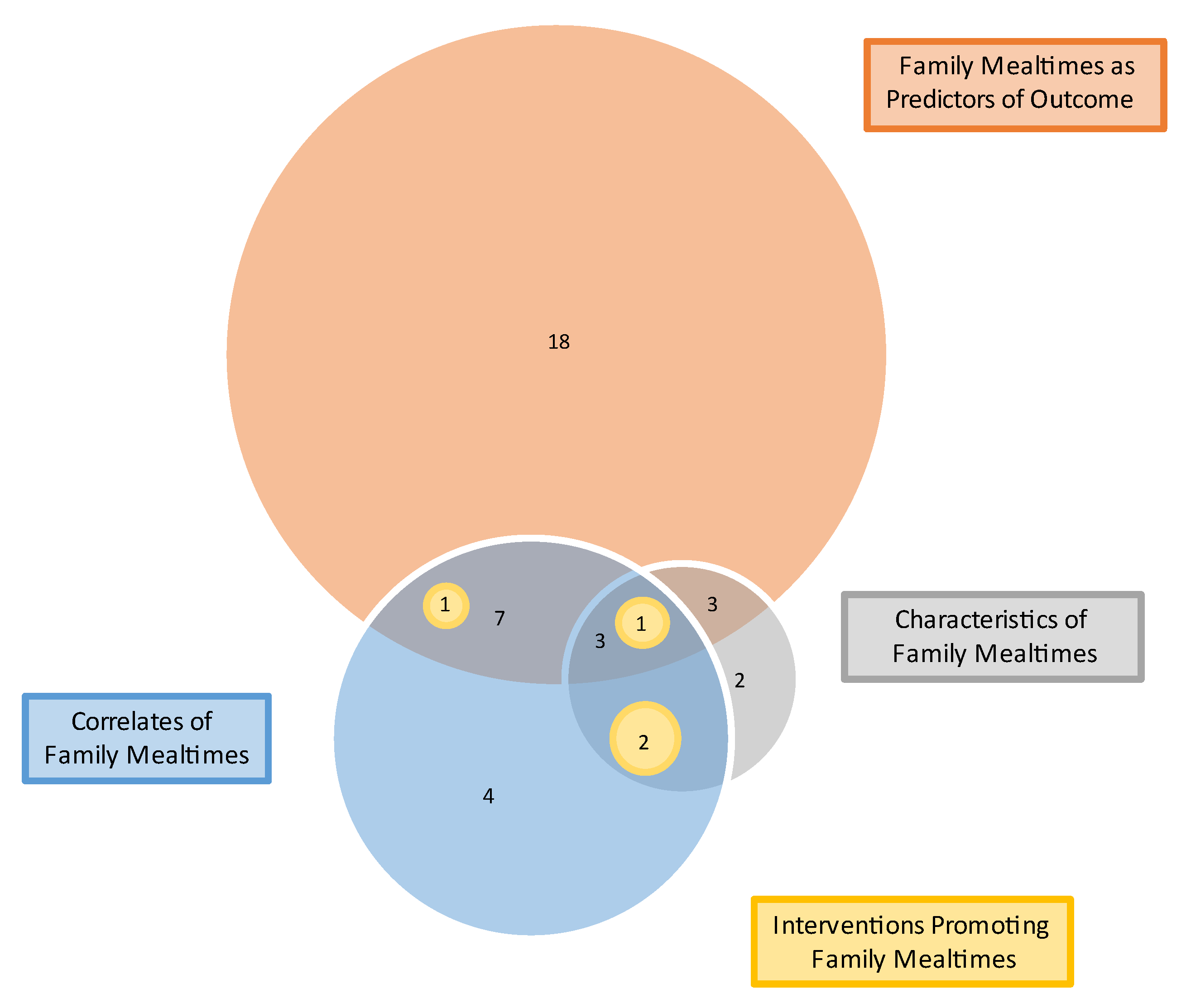
3.2.2. Overlap
3.2.3. Quality and Risk of Bias
- All reviews described their research question and inclusion criteria;
- While some reviews were pre-registered (6) or explicitly stated the review methods were established in advance (11), most had not pre-registered or made an explicit statement (24);
- Few reviews (3) explained their rationale for their selection of study designs;
- In almost all reviews, at least two databases (40) were searched and most reported keywords (37); however, few reviews provided a full rationale for their search limitations (34). In total, only 5 reviews described their literature search strategy comprehensively;
- Approximately half (19) of reviews described at least two reviewers independently agreeing on eligible articles, and approximately one third (15) described at least two reviewers agreeing on the extracted data;
- None of the reviews provided a list of excluded studies or justified exclusions;
- A majority of reviews described the studies included in partial (11) or full (19);
- Reviews that assessed the risk of bias of the original studies also accounted for risk of bias when interpreting their results; however, most reviews (22) did not describe a satisfactory technique for assessing the risk of bias in original studies;
- Most reviews discussed any heterogeneity in the results;
- None of the reviews reported the sources of funding for the original studies that were included;
- A majority of reviews (29) reported potential sources of conflict (including funding); however, reporting may be an artifact of the journal in which the review was published as some require this to be reported while others do not. Of the fourteen that received funding, ten received institutional grants or scholarships, three received industry grants and one did not specify.
3.3. Characteristics of Family Mealtimes
3.4. Correlates of Family Mealtimes
3.4.1. Correlates of Family Meal Frequency
3.4.2. Correlates of Other (Non-Frequency) Aspects of Family Meals
3.5. Outcomes Associated with Family Mealtimes
3.5.1. Family Mealtimes as a Predictor of Eating Behaviours/Nutrition
3.5.2. Family Meals as a Predictor of Weight-Status
3.6. Family Mealtimes as a Predictor of Psychosocial Outcomes
3.7. Moderators of the Relationship between Family Mealtimes and Outcomes
3.8. Interventions Aimed at Promoting Family Mealtimes
3.9. Heterogeneity of Results
4. Discussion
4.1. What Are the Characteristics of Family Mealtimes?
4.2. What Are the Correlates of Family Mealtimes?
4.3. What Outcomes Are Associated with Family Mealtimes?
4.4. Are Interventions Aimed at Promoting Family Mealtimes Effective?
4.5. Strengths and Limitations of Systematic Reviews
4.6. Strengths and Limitations of Umbrella Review
4.7. Implications for Practice, Policy and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCullough, M.B.; Robson, S.H.; Stark, L.J. A review of the structural characteristics of family meals with children in the United States. Adv. Nutr. 2016, 7, 627–640. [Google Scholar] [CrossRef]
- Martin-Biggers, J.; Spaccarotella, K.; Berhaupt-Glickstein, A.; Hongu, N.; Worobey, J.; Byrd-Bredbenner, C. Come and Get It! A Discussion of Family Mealtime Literature and Factors Affecting Obesity Risk1–3. Adv. Nutr. 2014, 5, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Metcalfe, J.J.; Folta, S.C.; Brown, A.; Fiese, B. Diet and Health Benefits Associated with In-Home Eating and Sharing Meals at Home: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1577. [Google Scholar] [CrossRef] [PubMed]
- Duriancik, D.M.; Goff, C.R. Children of single-parent households are at a higher risk of obesity: A systematic review. J. Child Health Care 2019, 23, 358–369. [Google Scholar] [CrossRef]
- Burrows, T.; Goldman, S.; Pursey, K.; Lim, R. Is there an association between dietary intake and academic achievement: A systematic review. J. Hum. Nutr. Diet. 2017, 30, 117–140. [Google Scholar] [CrossRef] [PubMed]
- Skeer, M.R.; Ballard, E.L. Are family meals as good for youth as we think they are? A review of the literature on family meals as they pertain to adolescent risk prevention. J. Youth Adolesc. 2013, 42, 943–963. [Google Scholar] [CrossRef]
- Dwyer, L.; Oh, A.; Patrick, H.; Hennessy, E. Promoting family meals: A review of existing interventions and opportunities for future research. Adolesc. Health Med. Ther. 2015, 6, 115–131. [Google Scholar] [PubMed]
- Fulkerson, J.A.; Larson, N.; Horning, M.; Neumark-Sztainer, D. A review of associations between family or shared meal frequency and dietary and weight status outcomes across the lifespan. J. Nutr. Educ. Behav. 2014, 46, 2–19. [Google Scholar] [CrossRef]
- Tosatti, A.M.; Ribeiro, L.W.; Machado, R.H.V.; Maximino, P.; Bozzini, A.B.; Ramos, C.C.; Fisberg, M. Does family mealtime have a protective effect on obesity and good eating habits in young people? A 2000–2016 review. Rev. Bras. Saude Matern. Infant. 2017, 17, 425–434. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Hanning, R.M. A Review of family meal influence on adolescents’ dietary intake. Can. J. Diet. Pract. Res. 2008, 69, 14–22. [Google Scholar] [CrossRef]
- Robson, S.M.; McCullough, M.B.; Rex, S.; Munafo, M.R.; Taylor, G. Family meal frequency, diet, and family functioning: A systematic review with meta-analyses. J. Nutr. Educ. Behav. 2020, 52, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Verhage, C.L.; Gillebaart, M.; van der Veek, S.M.; Vereijken, C.M. The relation between family meals and health of infants and toddlers: A review. Appetite 2018, 127, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Middleton, G.; Golley, R.; Patterson, K.; Le Moal, F.; Coveney, J. What can families gain from the family meal? A mixed-papers systematic review. Appetite 2020, 153, 104725. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.J.; Kang, H. Introduction to Umbrella Reviews as a Useful Evidence-Based Practice. J. Lipid Atheroscler. 2023, 12, 3–11. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Tugwell, P.; Kristjansson, E. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.F.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overview of Reviews. In Cochrane Handbook for Systematic Reviews of Interventions. Version 6, 3rd ed.; Higgins, J.T.J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: Hoboken, NJ, USA, 2022. [Google Scholar]
- Pollock, M.; Fernandes, R.M.; Pieper, D.; Tricco, A.C.; Gates, M.; Gates, A.; Hartling, L. Preferred Reporting Items for Overviews of Reviews (PRIOR): A protocol for development of a reporting guideline for overviews of reviews of healthcare interventions. Syst. Rev. 2019, 8, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Higgins, J.P.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. Version 6, 3rd ed.; Wiley: Hoboken, NJ, USA, 2022. [Google Scholar]
- Sadoyu, S.; Tanni, K.A.; Punrum, N.; Paengtrai, S.; Kategaew, W.; Promchit, N.; Lai, N.M.; Thakkinstian, A.; Ngorsuraches, S.; Bangpan, M.; et al. Methodological approaches for assessing certainty of the evidence in umbrella reviews: A scoping review. PLoS ONE 2022, 17, e0269009. [Google Scholar] [CrossRef]
- Hammons, A.J.; Fiese, B.H. Is frequency of shared family meals related to the nutritional health of children and adolescents? Pediatrics 2011, 127, e1565–e1574. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.J.; Gorely, T. Family correlates of breakfast consumption among children and adolescents. A systematic review. Appetite 2009, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Van der Horst, K.; Sleddens, E.F. Parenting styles, feeding styles and food-related parenting practices in relation to toddlers’ eating styles: A cluster-analytic approach. PLoS ONE 2017, 12, e0178149. [Google Scholar] [CrossRef] [PubMed]
- Cislak, A.; Safron, M.; Pratt, M.; Gaspar, T.; Luszczynska, A. Family-related predictors of body weight and weight-related behaviours among children and adolescents: A systematic umbrella review. Child Care Health Dev. 2012, 38, 321–331. [Google Scholar] [CrossRef]
- Dallacker, M.; Hertwig, R.; Mata, J. The frequency of family meals and nutritional health in children: A meta-analysis. Obes. Rev. 2018, 19, 638–653. [Google Scholar] [CrossRef] [PubMed]
- Dallacker, M.; Hertwig, R.; Mata, J. Quality Matters: A Meta-Analysis on Components of Healthy Family Meals. Health Psychol. 2019, 38, 1137–1149. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.E.; Norris, M.L.; Obeid, N.; Fu, M.; Weinstangel, H.; Sampson, M. Systematic review of the effects of family meal frequency on psychosocial outcomes in youth. Can. Fam. Physician 2015, 61, e96–e106. [Google Scholar]
- Rahill, S.; Kennedy, A.; Kearney, J. A review of the influence of fathers on children’s eating behaviours and dietary intake. Appetite 2020, 147, 104540. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.; Skouteris, H.; McCabe, M.; Ricciardelli, L.A.; Milgrom, J.; Baur, L.A. Paternal Influences on Children’s Weight Gain: A Systematic Review. Fathering 2011, 9, 252–267. [Google Scholar] [CrossRef]
- Liu, K.S.N.; Chen, J.Y.; Ng, M.Y.C.; Yeung, M.H.Y.; Bedford, L.E.; Lam, C.L.K. How does the family influence adolescent eating habits in terms of knowledge, attitudes and practices? A global systematic review of qualitative studies. Nutrients 2021, 13, 3717. [Google Scholar] [CrossRef]
- Valdés, J.; Rodríguez-Artalejo, F.; Aguilar, L.; Jaén-Casquero, M.B.; Royo-Bordonada, M.A. Frequency of family meals and childhood overweight: A systematic review. Pediatr. Obes. 2013, 8, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- Khandpur, N.; Blaine, R.E.; Fisher, J.O.; Davison, K.K. Fathers’ child feeding practices: A review of the evidence. Appetite 2014, 78, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M. A review of familial correlates of child and adolescent obesity: What has the 21st century taught us so far? Int. J. Adolesc. Med. Health 2009, 21, 457–483. [Google Scholar] [CrossRef]
- Vollmer, R.L.; Mobley, A.R. Parenting styles, feeding styles, and their influence on child obesogenic behaviors and body weight. A review. Appetite 2013, 71, 232–241. [Google Scholar] [CrossRef]
- Jenkins, S.; Horner, S.D. Barriers that Influence Eating Behaviors in Adolescents. J. Pediatr. Nurs. 2005, 20, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Titis, E. Parental Perspectives of the Impact of COVID-19 Lockdown on Food-Related Behaviors: Systematic Review. Foods 2022, 11, 2851. [Google Scholar] [CrossRef]
- Do Amaral e Melo, G.; Priscila Olin, S.; Nakabayashi, J.; Bandeira, M.V.; Toral, N.; Monteiro, R. Family meal frequency and its association with food consumption and nutritional status in adolescents: A systematic review. PLoS ONE 2020, 15, e0239274. [Google Scholar] [CrossRef]
- Krølner, R.; Rasmussen, M.; Brug, J.; Klepp, K.-I.; Wind, M.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part II: Qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.J.H.; Gorely, T. Family correlates of fruit and vegetable consumption in children and adolescents: A systematic review. Public Health Nutr. 2008, 12, 267–283. [Google Scholar] [CrossRef]
- Rasmussen, M.; Krølner, R.; Klepp, K.-I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 1–19. [Google Scholar] [CrossRef]
- Smith, J.A.; Saltzman, J.A.; Dev, D.A. Mealtime emotional climate and child health: A systematic review. Eat. Behav. Int. J. 2022, 44, 101582. [Google Scholar] [CrossRef]
- Avery, A.; Anderson, C.; McCullough, F. Associations between children’s diet quality and watching television during meal or snack consumption: A systematic review. Matern. Child Nutr. 2017, 13, e12428. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.R.; Buscemi, J.; Nicholson, L.M.; Cory, M.; Jagpal, A.; Bohnert, A.M. Links between the organization of the family home environment and child obesity: A systematic review. Obes. Rev. 2018, 19, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Tzanninis, S.; Ntanasis-Stathopoulos, I.; Panotopoulos, G.; Kostopoulou, M.; Tzanninis, I.G.; Tsagianni, A.; Sergentanis, T.N. Prevention and treatment of childhood and adolescent obesity: A systematic review of meta-analyses. World J. Pediatr. 2019, 15, 350–381. [Google Scholar] [CrossRef]
- Beckers, D.; Karssen, L.T.; Vink, J.M.; Burk, W.J.; Larsen, J.K. Food parenting practices and children’s weight outcomes: A systematic review of prospective studies. Appetite 2021, 158, 105010. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, S.S.; Tarver, W.L.; Locher, J.L.; Preskitt, J.; Sen, B. A systematic review of the association between family meals and adolescent risk outcomes. J. Adolesc. 2015, 44, 134–149. [Google Scholar] [CrossRef]
- Dorol-Beauroy-Eustache, O.; Mishara, B.L. Systematic review of risk and protective factors for suicidal and self-harm behaviors among children and adolescents involved with cyberbullying. Prev. Med. Int. J. Devoted Pract. Theory 2021, 152, 106684. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Obesity: No European country is on track to halt rising levels by 2025, WHO warns. BMJ 2022, 377, o1107. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. Obesity in US children increased at an unprecedented rate during the pandemic. BMJ 2021, 374, n2332. [Google Scholar] [CrossRef] [PubMed]
- House of Commons Library. Obesity Statistics. 2023. Available online: https://commonslibrary.parliament.uk/research-briefings/sn03336/#:~:text=Childhood%20obesity%20in%20England,and%20published%20by%20NHS%20Digital (accessed on 16 May 2023).
- Australian Institute of Health and Welfare. Overweight and Obesity among Australian Children and Adolescents; Australian Institute of Health and Welfare: Sydney, Australia, 2020.
- Canada Go. Tackling Obesity in Canada: Childhood Obesity and Excess Weight Rates in Canada. 2017. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/obesity-excess-weight-rates-canadian-children.html (accessed on 16 May 2023).
- CDC. Mealtime Routines and Tips 2021. Available online: https://www.cdc.gov/nutrition/infantandtoddlernutrition/mealtime/mealtime-routines-and-tips.html (accessed on 16 May 2023).
- European Union. EU Action Plan on Childhood Obesity 2014–2020. 2014. Available online: https://health.ec.europa.eu/system/files/2016-11/childhoodobesity_actionplan_2014_2020_en_0.pdf (accessed on 16 May 2023).
- Department of Health & Social Care. Childhood Obesity: A Plan for Action. 2017. Available online: https://www.gov.uk/government/publications/childhood-obesity-a-plan-for-action/childhood-obesity-a-plan-for-action (accessed on 16 May 2023).
- CDC. Overweight & Obesity. 2023. Available online: https://www.cdc.gov/obesity/strategies/healthcare/index.html (accessed on 16 May 2023).



{kind=link}
{kind=link}
| Reference | Authors (Year of Publication) | Review Question(s) Pertinent to Family Mealtimes | Review Design | Key Findings Pertinent to Family Mealtime Research |
|---|---|---|---|---|
| [1] | McCullough et al., (2016) | How has the family meal environment been characterised in the existing literature? |
| All studies reported ≥ 1 of the structural characteristics; most reported one, none reported all four.
|
| [2] | Martin-Biggers et al., (2014) |
|
| A range of definitions of family meals was used across studies, with some specifying the number of people who must be present and meal type (dinner). Parents experiences of family meals:
|
| [3] | Glanz et al., (2021) |
|
| Factors associated with more frequent in-home eating:
|
| [4] | Duriancik & Goff (2015) | Are children living in a single-parent household at risk of obesity? |
| Two studies investigated family meals. One investigated family meal frequency and found that children from single-mother homes had higher odds of infrequent family meals. The other investigated shared meals as a possible mechanism to explain the association between family structure and children’s higher risk of obesity but found it non-significant. Key limitation(s) pertinent to family mealtimes: Most studies were cross-sectional and causality could not be determined. |
| [5] | Burrows et al., (2017) | What are the effects of dietary intakes and behaviours on the academic achievement of school aged children? |
| One study reviewed assessed the frequency of family meals and found eating family meals ≥5 days per week was not associated with academic achievement. Key limitation(s) pertinent to family mealtimes: studies focused on household routines with few examining broader components of the home environment. |
| [6] | Skeer & Ballard (2013) | What mechanisms contribute to the protective effect against adolescent risk behaviour afforded by family meal frequency? |
|
|
| [7] | Dwyer et al., (2015) |
|
| Six intervention studies evaluating multiple session programmes delivered to families (3) or children/adolescents (3). Of the 6, 4 demonstrated a positive effect on family meal frequency while 2 were not significantly related to family meals. Non-intervention articles showed:
|
| [8] | Fulkerson et al. (2014) | What are the associations between family meal frequency and children and adolescents’ dietary/weight outcomes? |
|
|
| [9] | Tosatti et al., (2017) | Do family mealtimes have a protective effect on obesity and good eating habits in young people? |
|
|
| [10] | Woodruff et al., (2008) |
|
|
|
| [11] | Robson et al., (2020) | What is the direction and magnitude of the exposure to family meals and:
|
| Dietary Outcomes:
Evidence of a positive association between family meal/family dinner frequency and family functioning. Key limitation(s) pertinent to family mealtimes: lack of definitions and standardised measure for family meals. |
| [12] | Verhage et al., (2018) | Are characteristics of the family meal associated with outcomes in terms of health benefits in infants and toddlers? |
| Nine studies investigated the family meal frequency and parents’ perceptions of sharing meals: Most children had regular meals at the age of three.Mothers perceived mealtimes as a valuable moment to socialise.Family meals were more frequent among families that were Hispanic and non-Hispanic white compared to non-Hispanic black.
Interventions to promote family meals (2 studies):
|
| [13] | Middleton et al., (2020) | What impact does the family meal have on the health and wellbeing of the family? |
| Intervention Studies:
|
| [22] | Hammons & Fiese (2011) | What is the strength of the relationship between the frequency of shared family mealtimes and children’s nutritional health? |
|
|
| [23] | Pearson et al., (2009) | What are the correlates of the family environment associated with children’s and adolescent’s breakfast behaviour? |
|
|
| [24] | Scaglioni et al., (2018) | How does the family environment influence children’s eating behaviours? |
|
|
| [25] | van der Horst et al., (2017) |
|
| Three studies reported findings relating to family meals:
|
| [26] | Cislak et al., (2012) | What is the evidence for relationships between family variables, weight-related behaviours and body weight in children and adolescents? |
| Of two reviews examining frequency of family meals (breakfast/dinner), both found that a higher frequency was positively associated with healthy diet in children/adolescents. Key limitation(s) pertinent to family mealtimes: none reported. |
| [27] | Dallacker et al., (2019) |
|
|
|
| [28] | Dallacker et al., (2018) |
|
|
|
| [29] | Harrison et al., (2015) | What is the relationship between family meals and psychosocial outcomes in children and adolescents and are their differences between males and females? |
|
|
| [30] | Rahill et al., (2020) |
|
|
|
| [31] | Fraser et al., (2011) | In relation to children’s weight gain, overweight and obesity:
|
| One qualitative study identified two themes relating to family mealtimes: mealtime rituals and routines; tension during mealtimes and found a variety of strategies are required to establish healthy eating patterns and consistent routines. Key limitation(s) pertinent to family mealtimes: small, unrepresentative samples. |
| [32] | Liu et al., (2009) | How does the family influence adolescent eating habits in terms of knowledge, attitudes and practices? |
|
|
| [33] | Valdés et al., (2013) | What is the relationship between the frequency of family meals and the risk of overweight in children and adolescents? |
| While several studies found an inverse relationship between frequency of family meals and BMI/overweight, the association became non-significant once adjustments were made for potentially confounding variables (age, gender, socio-economic status, diet, physical activity). Key limitation(s) pertinent to family mealtimes: lack of definition of family meal and scarce information about the characteristics of family meals. |
| [34] | Khandpur et al., (2014) |
|
|
|
| [35] | Berge et al., (2009) | What are the familial correlates of child and adolescent obesity? |
| Correlates of family meal frequency:
|
| [36] | Vollmer & Mobley (2013) | What is the relationship between parenting and/or feeding styles on child body weight and/or child obesogenic behaviours? |
| One of five studies examining the role of family meal characteristics found an authoritative parenting style was positively associated with family meal frequency. Key limitation(s) pertinent to family mealtimes: None reported. |
| [37] | Jenkins & Horner (2005) | What are the barriers that influence eating behaviours in adolescence? |
|
|
| [38] | Titis (2022) | What are parents’ perspectives of the impact of the COVID-19 lockdown on the family food environment and food-related activities? |
| Changes arising from the COVID-19 lockdown were associated with parents having more time, greater interest in health and nutrition, increased motivation to eat more healthily. Specifically:
|
| [39] | Do Amaral e Melo et al., (2020) | What is the association between family meals frequency and food consumed and/or children’s, adolescents’ and young adults’ nutritional status? |
| Studies varied in the operationalisation of meal frequency, assessing the frequency of meals in general, dinner/supper/evening meal, dinner only, all three main meals (breakfast, lunch, and dinner), breakfast only, breakfast and dinner, lunch and dinner with most assessing meal frequency over a 1-week period. Association between family meal frequency and nutritional status:
|
| [40] | Krølner et al., (2011) | What are children/adolescents’ views and experiences regarding determinants of their intake of fruit and vegetables? |
| Children/adolescents perceived that family dinner at home is the only appropriate time to eat vegetables. Key limitation(s) pertinent to family mealtimes: none reported. |
| [41] | Pearson et al., (2008) | What are the correlates of the family environment associated with children’s and adolescent’s fruit and vegetable intake? |
|
|
| [42] | Rasmussen et al., (2006) | What are the determinants of fruit and vegetable consumption in children and adolescents? |
| Five of six papers investigating the influence of shared family meals found a positive association with children’s consumption of fruit and/or vegetables. The sixth paper found no association. Key limitation(s) pertinent to family mealtimes: many studies were based on small, non-representative samples; the validity of instruments used to assess constructs was reported either superficially or not at all. |
| [43] | Smith et al., (2022) | What are the child/adolescent level correlates of mealtime emotional climate? |
|
|
| [44] | Avery et al., (2017) | What are the associations between watching TV during a meal or while consuming a snack, and children’s diet quality? |
| Having the TV on during the family meal was associated with poorer diet quality in terms of adolescents’ consumption of fried foods (girls), soft drinks, grains, calcium-rich foods, and vegetables. Key limitation(s) pertinent to family mealtimes: none reported. |
| [45] | Bates et al., (2018) | What relations exist between the organisation of the family home environment and child obesity? |
| 10/16 studies found a significant relation between meal routines and child weight, 70% of which was in the expected direction. Less likelihood of obesity if:
|
| [46] | Psaltopoulou et al., (2019) | What is the observational and/or interventional evidence for nutritional, physical activity and behavioural factors preventing and/or treating child and adolescent obesity? |
| One meta-analysis investigated the frequency of family meals and childhood obesity and found that children having ≥3 family meals per week were 12% less likely to become obese compared to children who had <3 family meals per week. Key limitation(s) pertinent to family mealtimes: none reported. |
| [47] | Beckers et al., (2021) | What are the prospective links between food parenting practices and children’s weight outcomes? |
| Nine studies (six independent datasets) examined the association between meal routines and weight outcomes.
|
| [48] | Goldfarb et al., (2015) | What role does the family meal play in adolescent risk behaviours? |
|
|
| [49] | Dolor-Beauroy-Eustache & Mishara (2021) | What factors influence the impact of cyberbullying on suicidal and self-harm behaviours among children and adolescents? |
| A single study investigating the role of family meals showed that family dinners moderated the relationship between cyberbullying and internalising problems (including self-harm, suicide attempts and ideation). Key limitation(s) pertinent to family mealtimes: Most studies were cross-sectional so direction/causality could not be determined; studies used different instruments and conceptualisations to measure cyberbullying and suicidal and self-harm behaviours. |
| Reference | Author (Year of Publication) | Constructs (n) | Characteristics of Investigated Family Mealtimes (11 Reviews) | Correlates of Investigated Family Mealtime Characteristics (18 Reviews) | Investigated Outcome(s) that Family Mealtimes Predict (33 Reviews) | Interventions Promoting Family Mealtimes (4 Reviews) |
|---|---|---|---|---|---|---|
| [1] | McCullough et al., (2016) | 1 | location; duration; presence of family members | |||
| [2] | Martin-Biggers et al., (2014) | 3 | parents’ experiences | socio-demographics; meal structure, location, TV on; barriers/facilitators | BMI/weight status; psychosocial | |
| [3] | Glanz et al., (2021) | 3 | previous family meal frequency; ethnicity | BMI/weight status | 4 interventions evaluated | |
| [4] | Duriancik & Goff (2015) | 2 | single-mother homes | BMI/weight status | ||
| [5] | Burrows et al., (2017) | 1 | psychosocial | |||
| [6] | Skeer & Ballard (2013) | 1 | psychosocial | |||
| [7] | Dwyer et al., (2015) | 3 | parents’ experiences | socio-demographics; barriers/facilitators | 6 interventions evaluated | |
| [8] | Fulkerson et al., (2014) | 2 | meal frequency; TV | nutrition; BMI/weight status | ||
| [9] | Tosatti et al., (2017) | 2 | meal frequency | eating behaviour; nutrition; BMI/weight status | ||
| [10] | Woodruff et al., (2008) | 3 | meal frequency; TV | socio-demographics | nutrition | |
| [11] | Robson et al., (2020) | 2 | family functioning | nutrition; psychosocial | ||
| [12] | Verhage et al., (2018) | 3 | meal frequency; location; TV; presence of parent | ethnicity; feeding approach | eating behaviour; nutrition | 2 interventions evaluated |
| [13] | Middleton et al., (2020) | 3 | meal frequency; parents’ motivations, perceptions, strategies | barriers/facilitators | 9 interventions evaluated | |
| [22] | Hammons & Fiese (2011) | 2 | meal frequency | nutrition | ||
| [23] | Pearson et al., (2009) | 1 | nutrition | |||
| [24] | Scaglioni et al., (2018) | 2 | socio-demographics | eating behaviour; nutrition; psychosocial | ||
| [25] | van der Horst et al., (2017) | 2 | single-mother homes | eating behaviours; nutrition | ||
| [26] | Cislak et al., (2012) | 1 | nutrition | |||
| [27] | Dallacker et al., (2019) | 1 | nutrition; BMI/weight status | |||
| [28] | Dallacker et al., (2018) | 1 | nutrition | |||
| [29] | Harrison et al., (2015) | 3 | meal frequency | socio-demographics | psychosocial | |
| [42] | Rasmussen et al., (2006) | 1 | nutrition | |||
| [30] | Rahill et al., (2020) | 2 | parents’ roles | |||
| [31] | Fraser et al., (2011) | 1 | fathers’ experiences | |||
| [32] | Liu et al., (2009) | 2 | atmosphere at home | eating behaviours | ||
| [33] | Valdés et al., (2013) | 1 | nutrition; BMI/weight status | |||
| [34] | Khandpur et al., (2014) | 2 | food parenting practices | BMI/weight status | ||
| [35] | Berge et al., (2009) | 2 | prioritisation of family meals; family connectedness | nutrition; BMI/weight status | ||
| [36] | Vollmer & Mobley (2013) | 1 | parenting style | |||
| [37] | Jenkins & Horner (2005) | 2 | mothers’ employment | nutrition | ||
| [38] | Titis (2022) | 1 | COVID-19 pandemic restrictions | |||
| [39] | Do Amaral e Melo et al., (2020) | 1 | nutrition | |||
| [40] | Krølner et al., (2011) | 1 | eating behaviours | |||
| [41] | Pearson et al., (2008) | 1 | eating behaviours | |||
| [43] | Smith et al., (2022) | 1 | eating behaviour; nutrition; BMI/weight status | |||
| [44] | Avery et al., (2017) | 1 | nutrition | |||
| [45] | Bates et al., (2018) | 1 | BMI/weight status | |||
| [46] | Psaltopoulou et al., (2019) | 1 | BMI/weight status | |||
| [47] | Beckers et al., (2021) | 1 | nutrition | |||
| [48] | Goldfarb et al., (2015) | 1 | psychosocial | |||
| [49] | Dolor-Beauroy-Eustache & Mishara (2021) | 1 | psychosocial |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Snuggs, S.; Harvey, K. Family Mealtimes: A Systematic Umbrella Review of Characteristics, Correlates, Outcomes and Interventions. Nutrients 2023, 15, 2841. https://doi.org/10.3390/nu15132841
Snuggs S, Harvey K. Family Mealtimes: A Systematic Umbrella Review of Characteristics, Correlates, Outcomes and Interventions. Nutrients. 2023; 15(13):2841. https://doi.org/10.3390/nu15132841
Chicago/Turabian StyleSnuggs, Sarah, and Kate Harvey. 2023. "Family Mealtimes: A Systematic Umbrella Review of Characteristics, Correlates, Outcomes and Interventions" Nutrients 15, no. 13: 2841. https://doi.org/10.3390/nu15132841
APA StyleSnuggs, S., & Harvey, K. (2023). Family Mealtimes: A Systematic Umbrella Review of Characteristics, Correlates, Outcomes and Interventions. Nutrients, 15(13), 2841. https://doi.org/10.3390/nu15132841