

Sexual Function and Depressive Symptoms in Young Women with Euthyroid Hashimoto’s Thyroiditis Receiving Vitamin D, Selenomethionine and Myo-Inositol: A Pilot Study


Abstract
1. Introduction
2. Materials and Methods
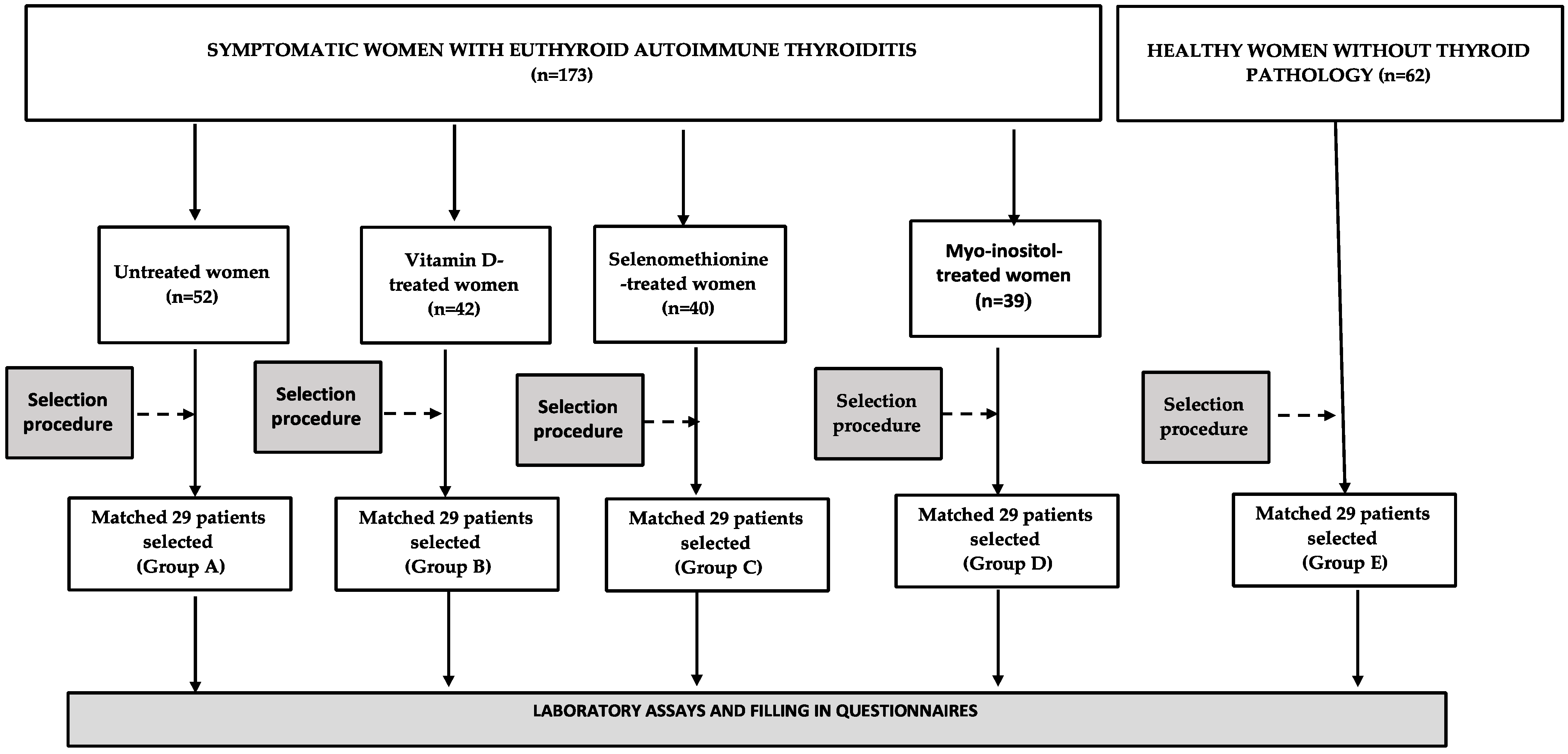
2.1. Study Population
2.2. Laboratory Assays
2.3. Questionnaires
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Groups
3.2. Biochemical Variables
3.3. Sexual Functioning
3.4. Depressive Symptoms
3.5. Correlations
4. Discussion
4.1. Sexual Functioning in Untreated Euthyroid Women with Autoimmune Thyroiditis
4.2. Sexual Functioning in Euthyroid Women with Autoimmune Thyroiditis Receiving Micronutrients
4.3. The Practical Significance of the Obtained Results
4.4. The Putative Role of the Impact on Thyroid Function and Inflammation in Sexual Functioning of Micronutrient-Treated Euthyroid Women with Autoimmune Thyroiditis
4.5. The Putative Role of Vitamin D Status in Sexual Functioning of Micronutrient-Treated Euthyroid Women with Autoimmune Thyroiditis
4.6. The Putative Role of the Impact on Extra-Thyroid Hormones in Sexual Functioning of Micronutrient-Treated Euthyroid Women with Autoimmune Thyroiditis
4.7. Depressive Symptoms in Euthyroid Women with Autoimmune Thyroiditis Receiving Micronutrients
4.8. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BDI-II | Beck Depression Inventory-Second Edition |
| DHEA-S | dehydroepiandrosterone-sulfate |
| FAI | free androgen index |
| FSFI | Female Sexual Function Index |
| SHBG | sex hormone-binding globulin |
| SPINA | structure parameter inference approach |
| TgAb | thyroglobulin antibodies |
| TPOAb | thyroid peroxidase antibodies |
| TSH | thyroid-stimulating hormone |
References
- Caturegli, P.; Kimura, H.; Rocchi, R.; Rose, N.R. Autoimmune thyroid diseases. Curr. Opin. Rheumatol. 2007, 19, 44–48. [Google Scholar] [CrossRef]
- Gessl, A.; Lemmens-Gruber, R.; Kautzky-Willer, A. Thyroid disorders. Handb. Exp. Pharmacol. 2012, 214, 361–386. [Google Scholar]
- Merrill, S.J.; Minucci, S.B. Thyroid autoimmunity: An interplay of factors. Vitam. Horm. 2018, 106, 129–145. [Google Scholar] [PubMed]
- Oppo, A.; Franceschi, E.; Atzeni, F.; Taberlet, A.; Mariotti, S. Effects of hyperthyroidism, hypothyroidism, and thyroid autoimmunity on female sexual function. J. Endocrinol. Investig. 2011, 34, 449–453. [Google Scholar] [CrossRef]
- Krysiak, R.; Drosdzol-Cop, A.; Skrzypulec-Plinta, V.; Okopień, B. Sexual function and depressive symptoms in young women with thyroid autoimmunity and subclinical hypothyroidism. Clin. Endocrinol. 2016, 84, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Bortun, A.C.; Ivan, V.; Navolan, D.B.; Dehelean, L.; Borlea, A.; Stoian, D. Thyroid autoimmune disease-impact on sexual function in young women. J. Clin. Med. 2021, 10, 369. [Google Scholar] [CrossRef]
- Atis, G.; Dalkilinc, A.; Altuntas, Y.; Caskurlu, T.; Ergenekon, E. Sexual dysfunction in women with clinical hypothyroidism and subclinical hypothyroidism. J. Sex. Med. 2010, 7, 2583–2590. [Google Scholar] [CrossRef]
- Veronelli, A.; Mauri, C.; Zecchini, B.; Peca, M.G.; Turri, O.; Valitutti, M.T.; Dall’Asta, C.; Pontiroli, A.E. Sexual dysfunction is frequent in premenopausal women with diabetes, obesity, and hypothyroidism, and correlates with markers of increased cardiovascular risk. A preliminary report. J. Sex. Med. 2009, 6, 1561–1568. [Google Scholar] [CrossRef]
- Pasquali, D.; Maiorino, M.I.; Renzullo, A.; Bellastella, G.; Accardo, G.; Esposito, D.; Barbato, F.; Esposito, K. Female sexual dysfunction in women with thyroid disorders. J. Endocrinol. Investig. 2013, 36, 729–733. [Google Scholar]
- Luo, H.; Zhao, W.; Yang, H.; Han, Q.; Zeng, L.; Tang, H.; Zhu, J. Subclinical hypothyroidism would not lead to female sexual dysfunction in Chinese women. BMC Women’s Health 2018, 18, 26. [Google Scholar] [CrossRef]
- Krysiak, R.; Szkróbka, W.; Okopień, B. Sexual function and depressive symptoms in young women with hypothyroidism receiving levothyroxine/liothyronine combination therapy: A pilot study. Curr. Med. Res. Opin. 2018, 34, 1579–1586. [Google Scholar] [CrossRef]
- Bozkurt, N.C.; Karbek, B.; Ucan, B.; Sahin, M.; Cakal, E.; Ozbek, M.; Delibasi, T. The association between severity of vitamin D deficiency and Hashimoto thyroiditis. Endocr. Pract. 2013, 19, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Chen, X.; Qian, X.; Shao, S. Effects of vitamin D treatment on thyroid function and autoimmunity markers in patients with Hashimoto thyroiditis—A meta-analysis of randomized controlled trials. J. Clin. Pharm. Ther. 2022, 47, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wu, Y.; Zuo, Z.; Zhao, Y.; Wang, K. The effect of vitamin D supplementation on thyroid autoantibody levels in the treatment of autoimmune thyroiditis: A systematic review and a meta-analysis. Endocrine 2018, 59, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Toulis, K.A.; Anastasilakis, A.D.; Tzellos, T.G.; Goulis, D.G.; Kouvelas, D. Selenium supplementation in the treatment of Hashimoto thyroiditis: A systematic review and a meta-analysis. Thyroid 2010, 20, 1163–1173. [Google Scholar] [CrossRef]
- Wichman, J.; Winther, K.H.; Bonnema, S.J.; Hegedüs, L. Selenium supplementation signicantly reduces thyroid autoantibody levels in patients with chronic autoimmune thyroiditis: A systematic review and meta-analysis. Thyroid 2016, 26, 1681–1699. [Google Scholar] [CrossRef]
- Duntas, L.H. The role of iodine and selenium in autoimmune thyroiditis. Horm. Metab. Res. 2015, 47, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Chatree, S.; Thongmaen, N.; Tantivejkul, K.; Sitticharoon, C.; Vucenik, I. Role of inositols and inositol phosphates in energy metabolism. Molecules 2020, 25, 5079. [Google Scholar] [CrossRef]
- Krysiak, R.; Kowalcze, K.; Okopień, B. The impact of vitamin D on thyroid autoimmunity and hypothalamic-pituitary-thyroid axis activity in myo-inositol-treated and myo-inositol-naïve women with autoimmune thyroiditis: A pilot study. J. Clin. Pharm. Ther. 2022, 47, 1759–1767. [Google Scholar] [CrossRef]
- Nordio, M.; Pajalich, R. Combined treatment with myo-inositol and selenium ensures euthyroidism in subclinical hypothyroidism patients with autoimmune thyroiditis. J. Thyroid Res. 2013, 2013, 424163. [Google Scholar] [CrossRef]
- Krysiak, R.; Gilowska, M.; Okopień, B. Sexual function and depressive symptoms in young women with low vitamin D status: A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 204, 108–112. [Google Scholar] [CrossRef]
- Inal, Z.O.; Inal, H.A.; Gorkem, U. Sexual function and depressive symptoms in primary infertile women with vitamin D deficiency undergoing IVF treatment. Taiwan J. Obstet. Gynecol. 2020, 59, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Bahramy, P.; Mohammad-Alizadeh-Charandabi, S.; Ramezani-Nardin, F.; Mirghafourvand, M. Serum levels of vitamin D, calcium, magnesium, and copper, and their relations with mental health and sexual function in pregnant Iranian adolescents. Biol. Trace Elem. Res. 2020, 198, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Jalali-Chimeh, F.; Gholamrezaei, A.; Vafa, M.; Nasiri, M.; Abiri, B.; Darooneh, T.; Ozgoli, G. Effect of vitamin D therapy on sexual function in women with sexual dysfunction and vitamin D deficiency: A randomized, double-blind, placebo controlled clinical trial. J. Urol. 2019, 201, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Caruso, S.; Rapisarda, A.M.; Cianci, S.; Cianci, A. Isoflavones, calcium, vitamin D and inulin improve quality of life, sexual function, body composition and metabolic parameters in menopausal women: Result from a prospective, randomized, placebo-controlled, parallel-group study. Prz. Menopauzalny 2018, 17, 32–38. [Google Scholar] [CrossRef]
- Sarebani, Z.; Chegini, V.; Chen, H.; Aali, E.; Mirzadeh, M.; Abbaspour, M.; Griffiths, M.D.; Alimoradi, Z. Effect of vitamin D vaginal suppository on sexual functioning among postmenopausal women: A three-arm randomized controlled clinical trial. Obstet. Gynecol. Sci. 2023, 66, 208–220. [Google Scholar] [CrossRef]
- Jostel, A.; Ryder, W.D.; Shalet, S.M. The use of thyroid function tests in the diagnosis of hypopituitarism: Definition and evaluation of the TSH Index. Clin. Endocrinol. 2009, 71, 529–534. [Google Scholar] [CrossRef]
- Dietrich, J.W.; Müller, P.; Schiedat, F.; Schlömicher, M.; Strauch, J.; Chatzitomaris, A.; Klein, H.H.; Mügge, A.; Köhrle, J.; Rijntjes, E.; et al. Nonthyroidal illness syndrome in cardiac illness involves elevated concentrations of 3,5-diiodothyronine and correlates with atrial remodeling. Eur. Thyroid J. 2015, 4, 129–137. [Google Scholar] [CrossRef]
- Dietrich, J.W.; Landgrafe-Mende, G.; Wiora, E.; Chatzitomaris, A.; Klein, H.H.; Midgley, J.E.; Hoermann, R. Calculated parameters of thyroid homeostasis: Emerging tools for differential diagnosis and clinical research. Front. Endocrinol. 2016, 7, 57. [Google Scholar] [CrossRef]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Wiegel, M.; Meston, C.; Rosen, R. The Female Sexual Function Index (FSFI): Cross-validation and development of clinical cut-off scores. J. Sex Marital. Ther. 2005, 31, 1–20. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. BDI-II: Beck Depression Inventory Manual, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders—DSM-IV-TR, 4th ed.; American Psychiatric Publishing: Washington, DC, USA, 1994. [Google Scholar]
- Duntas, L.H.; Benvenga, S. Selenium: An element for life. Endocrine 2015, 48, 756–775. [Google Scholar] [CrossRef] [PubMed]
- Benvenga, S.; Nordio, M.; Laganà, A.S.; Unfer, V. The role of inositol in thyroid physiology and in subclinical hypothyroidism management. Front. Endocrinol. 2021, 12, 662582. [Google Scholar] [CrossRef] [PubMed]
- El-Kazaz, S.E.; Abo-Samaha, M.I.; Hafez, M.H.; El-Shobokshy, S.A.; Wirtu, G. Dietary supplementation of nano-selenium improves reproductive performance, sexual behavior and deposition of selenium in the testis and ovary of Japanese quail. J. Adv. Vet. Anim. Res. 2020, 7, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Kłapcińska, B.; Poprzecki, S.; Danch, A.; Sobczak, A.; Kempa, K. Selenium levels in blood of Upper Silesian population: Evidence of suboptimal selenium status in a significant percentage of the population. Biol. Trace Elem. Res. 2005, 108, 1–15. [Google Scholar] [CrossRef]
- Larsen, P.R.; Zavacki, A.M. The role of the iodothyronine deiodinases in the physiology and pathology of thyroid hormone action. Eur. Thyroid J. 2012, 1, 232–242. [Google Scholar]
- Krysiak, R.; Kowalcze, K.; Okopień, B. Selenomethionine potentiates the impact of vitamin D on thyroid autoimmunity in euthyroid women with Hashimoto thyroiditis and low vitamin D status. Pharmacol. Rep. 2019, 71, 367–373. [Google Scholar] [CrossRef]
- Muller, A.F.; Drexhage, H.A.; Berghout, A. Postpartum thyroiditis and autoimmune thyroiditis in women of childbearing age: Recent insights and consequences for antenatal and postnatal care. Endocr. Rev. 2001, 22, 605–630. [Google Scholar] [CrossRef]
- Moutachakkir, M.; Lamrani Hanchi, A.; Baraou, A.; Boukhira, A.; Chellak, S. Immunoanalytical characteristics of C-reactive protein and high sensitivity C-reactive protein. Ann. Biol. Clin. 2017, 75, 225–229. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhou, C.; Chen, H.; Zhao, Q.; Li, L.; Cui, Y.; Shen, B. Rheumatoid arthritis is associated with negatively variable impacts on domains of female sexual function: Evidence from a systematic review and meta-analysis. Psychol. Health Med. 2018, 23, 114–125. [Google Scholar] [CrossRef]
- García Morales, M.; Callejas Rubio, J.I.; Peralta-Ramírez, M.I.; Henares Romero, L.J.; Ríos Fernández, R.; Camps García, M.T.; Navarrete Navarrete, N.; Ortego Centeno, N. Impaired sexual function in women with systemic lupus erythematosus: A cross-sectional study. Lupus 2013, 22, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Diver, M. Laboratory measurement of testosterone. Front. Horm. Res. 2009, 37, 21–31. [Google Scholar] [PubMed]
- Davis, S.R.; Worsley, R.; Miller, K.K.; Parish, S.J.; Santoro, N. Androgens and female sexual function and dysfunction—Findings from the Fourth International Consultation of Sexual Medicine. J. Sex. Med. 2016, 13, 168–178. [Google Scholar] [CrossRef]
- Davison, S.L.; Davis, S.R. Androgens in women. J. Steroid Biochem. Mol. Biol. 2003, 85, 363–366. [Google Scholar] [CrossRef]
- Chang, E.M.; Kim, Y.S.; Won, H.J.; Yoon, T.K.; Lee, W.S. Association between sex steroids, ovarian reserve, and vitamin D levels in healthy nonobese women. J. Clin. Endocrinol. Metab. 2014, 99, 2526–2532. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Frisch, S.; Koertke, H.; Kuhn, J.; Dreier, J.; Obermayer-Pietsch, B.; Wehr, E.; Zittermann, A. Effect of vitamin D supplementation on testosterone levels in men. Horm. Metab. Res. 2011, 43, 223–225. [Google Scholar] [CrossRef]
- Ahonen, M.H.; Zhuang, Y.H.; Aine, R.; Ylikomi, T.; Tuohimaa, P. Androgen receptor and vitamin D receptor in human ovarian cancer: Growth stimulation and inhibition by ligands. Int. J. Cancer 2000, 86, 40–46. [Google Scholar] [CrossRef]
- Borba, V.V.; Zandman-Goddard, G.; Shoenfeld, Y. Prolactin and autoimmunity. Front. Immunol. 2018, 9, 73. [Google Scholar] [CrossRef]
- Krysiak, R.; Drosdzol-Cop, A.; Skrzypulec-Plinta, V.; Okopień, B. Sexual function and depressive symptoms in young women with elevated macroprolactin content: A pilot study. Endocrine 2016, 53, 291–298. [Google Scholar] [CrossRef]
- Drbalová, K.; Matucha, P.; Matejková-Behanová, M.; Bílek, R.; Kríz, L.; Kazihnitková, H.; Hampl, R. Immunoprotective steroids and SHBG in non-treated hypothyroidism and their relationship to autoimmune thyroid disorders. Physiol. Res. 2008, 57 (Suppl. 1), S119–S125. [Google Scholar] [CrossRef]
- Ott, J.; Pecnik, P.; Promberger, R.; Pils, S.; Seemann, R.; Hermann, M.; Frigo, P. Dehydroepiandrosterone in women with premature ovarian failure and Hashimoto thyroiditis. Climacteric 2014, 17, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Vilar, L.; Vilar, C.F.; Lyra, R.; Freitas, M.D. Pitfalls in the diagnostic evaluation of hyperprolactinemia. Neuroendocrinology 2019, 109, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Siegmann, E.M.; Müller, H.H.; Luecke, C.; Philipsen, A.; Kornhuber, J.; Grömer, T.W. Thyroiditis: A systematic review and meta-analysis. JAMA Psychiatry 2018, 75, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Kirim, S.; Keskek, S.O.; Köksal, F.; Haydardedeoglu, F.E.; Bozkirli, E.; Toledano, Y. Depression in patients with euthyroid chronic autoimmune thyroiditis. Endocr. J. 2012, 59, 705–708. [Google Scholar] [CrossRef]
- Musazadeh, V.; Keramati, M.; Ghalichi, F.; Kavyani, Z.; Ghoreishi, Z.; Alras, K.A.; Albadawi, N.; Salem, A.; Albadawi, M.I.; Salem, R.; et al. Vitamin D protects against depression: Evidence from an umbrella meta-analysis on interventional and observational meta-analyses. Pharmacol. Res. 2023, 187, 106605. [Google Scholar] [CrossRef]
- Sajjadi, S.S.; Foshati, S.; Haddadian-Khouzani, S.; Rouhani, M.H. The role of selenium in depression: A systematic review and meta-analysis of human observational and interventional studies. Sci. Rep. 2022, 12, 1045. [Google Scholar] [CrossRef]
- Mukai, T.; Kishi, T.; Matsuda, Y.; Iwata, N. A meta-analysis of inositol for depression and anxiety disorders. Hum. Psychopharmacol. 2014, 29, 55–63. [Google Scholar] [CrossRef]
- Blakely, T.; Pearce, N.; Lynch, J. Case-control studies. JAMA 2019, 321, 806–807. [Google Scholar] [CrossRef]
- Szybiński, Z.; Polish Council for Control of Iodine Deficiency Disorders. Work of the Polish council for control of iodine deficiency disorders, and the model of iodine prophylaxis in Poland. Endokrynol. Pol. 2012, 63, 156–160. [Google Scholar]


{kind=link}
| Variable | Group A | Group B | Group C | Group D | Group E |
|---|---|---|---|---|---|
| Number of patients | 29 | 29 | 29 | 29 | 29 |
| Age (years) | 31 ± 7 | 32 ± 7 | 32 ± 6 | 31 ± 6 | 32 ± 7 |
| Body mass index (kg/m2) | 23.8 ± 4.2 | 23.4 ± 4.8 | 23.2 ± 4.0 | 24.0 ± 4.8 | 23.5 ± 4.3 |
| Smokers (%)/Number of cigarettes a day (n)/Duration of smoking (months) | 34/11 ± 7/82 ± 31 | 38/10 ± 8/84 ± 36 | 41/12 ± 8/88 ± 39 | 34/11 ± 6/80 ± 34 | 38/10 ± 7/86 ± 35 |
| Physical activity: total/several times a week/once a week/once a month (%) | 97/48/34/14 | 93/45/34/14 | 97/52/31/14 | 93/48/34/10 | 97/45/34/17 |
| Primary or vocational/secondary/university education (%) | 17/34/48 | 21/34/45 | 21/38/41 | 17/38/45 | 21/31/48 |
| Occupational activity/Blue-collar/white-collar/pink-collar workers (%) | 89/21/34/34 | 86/17/31/38 | 89/21/38/31 | 93/17/34/41 | 86/17/38/31 |
| Number of sexual partners (n) | 2.4 ± 1.2 | 2.4 ± 0.9 | 2.3 ± 0.8 | 2.2 ± 1.1 | 2.3 ± 1.0 |
| Number of marriages (n)/duration of marriages (months) | 1.2 ± 0.6/44 ± 18 | 1.3 ± 0.6/48 ± 17 | 1.2 ± 0.7/47 ± 19 | 1.1 ± 0.6/43 ± 20 | 1.3 ± 0.7/50 ± 20 |
| Number of deliveries (n)/Number of miscarriages (n) | 1.4 ± 0.7/0.6 ± 0.5 | 1.3 ± 0.6/0.7 ± 0.5 | 1.5 ± 0.8/0.5 ± 0.5 | 1.4 ± 0.6/0.6 ± 0.4 | 1.3 ± 0.7/0.4 ± 0.4 |
| Stress exposure (%) | 76 | 69 | 76 | 72 | 69 |
| Systolic blood pressure (mm Hg) | 124 ± 18 | 120 ± 16 | 121 ± 19 | 124 ± 17 | 120 ± 20 |
| Diastolic blood pressure (mm Hg) | 79 ± 6 | 77 ± 6 | 78 ± 6 | 78 ± 7 | 77 ± 6 |
| Mean daily vitamin D intake 1 (µg) | 8.9 ± 4.0 | 8.3 ± 3.0 | 9.1 ± 3.5 | 8.7 ± 3.8 | 9.5 ± 4.0 |
| Mean daily selenium intake 2 (µg) | 40 ± 10 | 38 ± 13 | 37 ± 12 | 38 ± 10 | 41 ± 11 |
| Mean daily inositol intake 3 (mg) | 750 ± 322 | 783 ± 352 | 812 ± 382 | 795 ± 320 | 822 ± 342 |
| Variable | Group A | Group B | Group C | Group D |
|---|---|---|---|---|
| TPOAb (IU/mL) | 882 ± 324 | 912 ± 365 | 895 ± 279 | 928 ± 370 |
| TgAb (IU/mL) | 845 ± 382 | 832 ± 354 | 861 ± 324 | 870 ± 380 |
| TSH (mIU/L) | 3.0 ± 0.7 | 2.9 ± 0.8 | 3.1 ± 0.7 | 3.0 ± 0.6 |
| Free thyroxine (pmol/L) | 14.2 ± 2.1 | 14.5 ± 2.2 | 13.9 ± 2.0 | 14.3 ± 2.3 |
| Free triiodothyronine (pmol/L) | 3.0 ± 0.5 | 3.2 ± 0.6 | 3.1 ± 0.5 | 3.1 ± 0.6 |
| Jostel’s TSH index | 3.0 ± 0.2 | 3.1 ± 0.2 | 3.0 ± 0.2 | 3.0 ± 0.2 |
| SPINA-GT (pmol/s) | 2.07 ± 0.28 | 2.13 ± 0.35 | 1.99 ± 0.34 | 2.08 ± 0.29 |
| SPINA-GD (nmol/s) | 19.53 ± 2.59 | 20.41 ± 2.75 | 20.62 ± 3.11 | 20.04 ± 2.47 |
| Variable | Group A | Group B | Group C | Group D | Group E |
|---|---|---|---|---|---|
| TPOAb (IU/mL) | 905 ± 348 & | 551 ± 290 *#$& | 680 ± 221 *& | 712 ± 286 *& | 18 ± 8 |
| TgAb (IU/mL) | 882 ± 364 & | 535 ± 267 *& | 623 ± 265 *& | 640 ± 284 *& | 17 ± 10 |
| TSH (mIU/L) | 3.1 ± 1.0 & | 2.6 ± 0.9 | 2.7 ± 0.8 | 2.7 ± 1.0 | 2.3 ± 0.8 * |
| Free thyroxine (pmol/L) | 14.6 ± 2.8 | 15.8 ± 3.5 | 14.5 ± 2.9 | 14.8 ± 2.0 | 16.2 ± 3.7 |
| Free triiodothyronine (pmol/L) | 3.1 ± 0.7 | 3.5 ± 0.9 | 3.4 ± 0.8 | 3.2 ± 0.8 | 3.5 ± 0.9 |
| Jostel’s TSH index | 3.1 ± 0.2 | 3.1 ± 0.2 | 3.0 ± 0.2 | 3.0 ± 0.2 | 3.0 ± 0.2 |
| SPINA-GT (pmol/s) | 2.09 ± 0.41 | 2.47 ± 0.44 * | 2.24 ± 0.47 | 2.27 ± 0.46 | 2.70 ± 0.49 *#$ |
| SPINA-GD (nmol/s) | 19.63 ± 2.83 | 20.38 ± 2.28 | 21.68 ± 2.56 *#^& | 19.99 ± 2.44 | 19.98 ± 2.62 |
| Prolactin (ng/mL) | 17.2 ± 6.4 | 15.8 ± 8.2 | 16.3 ± 6.8 | 17.0 ± 7.0 | 16.5 ± 6.2 |
| Estradiol (pmol/L) | 432 ± 182 | 465 ± 150 | 415 ± 186 | 480 ± 180 | 446 ± 167 |
| Testosterone (pmol/L) | 1.02 ± 0.32 | 1.61 ± 0.38 *#$ | 1.25 ± 0.40 * | 1.30 ± 0.34 * | 1.65 ± 0.41 *#$ |
| SHBG (nmol/L) | 57 ± 16 | 64 ± 14 | 58 ± 17 | 61 ± 15 | 65 ± 21 |
| FAI (%) | 1.79 ± 0.42 | 2.51 ± 0.48 *#$ | 2.15 ± 0.50 * | 2.13 ± 0.46 * | 2.53 ± 0.43 *#$ |
| DHEA-S (μmol/L) | 6.4 ± 2.5 | 7.0 ± 2.5 | 6.8 ± 2.1 | 6.5 ± 2.5 | 7.2 ± 2.2 |
| 25-hydroxyvitamin D (nmol/L) | 64 ± 28 | 106 ± 28 *#$ | 70 ± 26 | 66 ± 20 | 92 ± 32 *#$ |
| hs-CRP (mg/L) | 3.5 ± 1.2 & | 2.0 ± 0.6 *#$& | 2.6 ± 0.9 *& | 2.7 ± 0.8 *& | 1.2 ± 0.3 |
| Variable | Group A | Group B | Group C | Group D |
|---|---|---|---|---|
| Δ TPOAb | 3 ± 8 | −40 ± 18 *#$ | −24 ± 14 * | −23 ± 12 * |
| Δ TgAb | 4 ± 8 | −36 ± 24 * | −28 ± 14 * | −26 ± 14 * |
| Δ TSH | 3 ± 6 | −10 ± 8 * | −13 ± 10 * | −9 ± 8 * |
| Δ Free thyroxine | 3 ± 8 | 9 ± 15 | 4 ± 10 | 3 ± 8 |
| Δ Free triiodothyronine | 3 ± 10 | 9 ± 14 | 10 ± 16 | 3 ± 11 |
| Δ Jostel’s TSH index | 3 ± 11 | 0 ± 8 | 0 ± 7 | 0 ± 12 |
| Δ SPINA-GT | 1 ± 6 | 16 ± 16 * | 12 ± 11 * | 9 ± 10 * |
| Δ SPINA-GD | 1 ± 4 | 0 ± 3 | 5 ± 5 *^$ | 0 ± 4 |
| Variable | Group A | Group B | Group C | Group D | Group E |
|---|---|---|---|---|---|
| FSFI score | 26.95 ± 3.10 & | 31.40 ± 2.25 *#$ | 30.02 ± 2.18 *& | 29.59 ± 3.02 *& | 32.14 ± 2.53 |
| FSFI score ≤ 26.55 (n%) | 14 (48) & | 3 (10) *#$ | 7 (24) *& | 8 (28) *& | 2 (7) |
| Sexual desire | 3.80 ± 0.90 & | 5.15 ± 0.58 *#$ | 4.61 ± 0.76 *& | 4.48 ± 0.82 *& | 5.39 ± 0.60 |
| Sexual arousal | 4.05 ± 0.85 & | 5.10 ± 0.82 *#$ | 4.67 ± 0.53 *& | 4.51 ± 0.62 *& | 5.28 ± 0.65 |
| Lubrication | 4.45 ± 0.84 & | 5.22 ± 0.65 * | 5.12 ± 0.48 * | 4.95 ± 0.78 * | 5.24 ± 0.50 * |
| Orgasm | 5.15 ± 0.75 | 5.40 ± 0.37 | 5.24 ± 0.51 | 5.20 ± 0.65 | 5.42 ± 0.46 |
| Sexual satisfaction | 4.40 ± 0.72 & | 5.18 ± 0.68 *& | 5.20 ± 0.51 *& | 5.23 ± 0.56 *& | 5.50 ± 0.38 |
| Pain | 5.10 ± 0.68 | 5.35 ± 0.42 | 5.18 ± 0.58 | 5.22 ± 0.55 | 5.31 ± 0.45 |
| Variable | Vitamin D Deficiency | Vitamin D Insufficiency | Normal Vitamin D Status |
|---|---|---|---|
| Number of patients: total/Group A/Group B/Group C/Group D/Group E (n) | 21/8/0/6/7/0 | 53/14/1/13/13/12 | 71/7/28/10/9/17 |
| FSFI score | 28.32 ± 3.20 *# | 29.58 ± 2.35 # | 30.84 ± 2.84 |
| FSFI score ≤ 26.55 (n %) | 9 (43) *# | 15 (28) # | 10 (14) |
| Sexual desire | 4.02 ± 0.98 *# | 4.50 ± 0.84 # | 5.03 ± 0.78 |
| Sexual arousal | 4.41 ± 0.92 # | 4.60 ± 0.85 | 4.90 ± 0.88 |
| Lubrication | 4.89 ± 0.84 | 4.93 ± 0.78 | 5.09 ± 0.58 |
| Orgasm | 5.01 ± 0.65 # | 5.28 ± 0.58 | 5.35 ± 0.46 |
| Sexual satisfaction | 4.84 ± 0.75 # | 5.08 ± 0.65 | 5.19 ± 0.60 |
| Pain | 5.15 ± 0.53 | 5.19 ± 0.55 | 5.28 ± 0.48 |
| Variable | Group A | Group B | Group C | Group D | Group E |
|---|---|---|---|---|---|
| BDI-II score | 12.9 ± 3.5 & | 9.2 ± 3.0 *#$& | 11.2 ± 2.9 *& | 11.0 ± 3.4 *& | 7.3 ± 2.8 |
| Depression symptoms (n%) | 14 (48) & | 6 (21) *#$& | 10 (34) *& | 10 (34) *& | 4 (10) |
| Mild symptoms (n%) | 13 (45) & | 6 (21) *#$& | 10 (34) *& | 10 (34) *& | 4 (10) |
| Moderate symptoms (n%) | 1 (3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Severe symptoms (n%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krysiak, R.; Kowalcze, K.; Szkróbka, W.; Okopień, B. Sexual Function and Depressive Symptoms in Young Women with Euthyroid Hashimoto’s Thyroiditis Receiving Vitamin D, Selenomethionine and Myo-Inositol: A Pilot Study. Nutrients 2023, 15, 2815. https://doi.org/10.3390/nu15122815
Krysiak R, Kowalcze K, Szkróbka W, Okopień B. Sexual Function and Depressive Symptoms in Young Women with Euthyroid Hashimoto’s Thyroiditis Receiving Vitamin D, Selenomethionine and Myo-Inositol: A Pilot Study. Nutrients. 2023; 15(12):2815. https://doi.org/10.3390/nu15122815
Chicago/Turabian StyleKrysiak, Robert, Karolina Kowalcze, Witold Szkróbka, and Bogusław Okopień. 2023. "Sexual Function and Depressive Symptoms in Young Women with Euthyroid Hashimoto’s Thyroiditis Receiving Vitamin D, Selenomethionine and Myo-Inositol: A Pilot Study" Nutrients 15, no. 12: 2815. https://doi.org/10.3390/nu15122815
APA StyleKrysiak, R., Kowalcze, K., Szkróbka, W., & Okopień, B. (2023). Sexual Function and Depressive Symptoms in Young Women with Euthyroid Hashimoto’s Thyroiditis Receiving Vitamin D, Selenomethionine and Myo-Inositol: A Pilot Study. Nutrients, 15(12), 2815. https://doi.org/10.3390/nu15122815