
Vitamin D Status, Cdx2 Genotype, and Colorectal Cancer Survival: Population-Based Patient Cohort
 , , ,
, , , Highlights
- Colorectal cancer (CRC) patients with Vitamin D deficiency had notably poorer long-term survival outcomes compared to those with adequate vitamin D status.
- We observed a clear survival benefit from adequate Vitamin D status in GG carriers of the Cdx2 vitamin D receptor gene, compared to those with AA/AG genotypes.
- Vitamin D supplementation might offer a tailored therapeutic advantage in improving survival outcomes, particularly for CRC patients with Vitamin D deficiency and the GG Cdx2 genotype.
- Further research, including randomized trials, are needed to explore whether Vitamin D supplementation can be recommended as a supportive therapy for improving CRC prognosis in these patients.
Abstract
1. Introduction
2. Materials and Methods
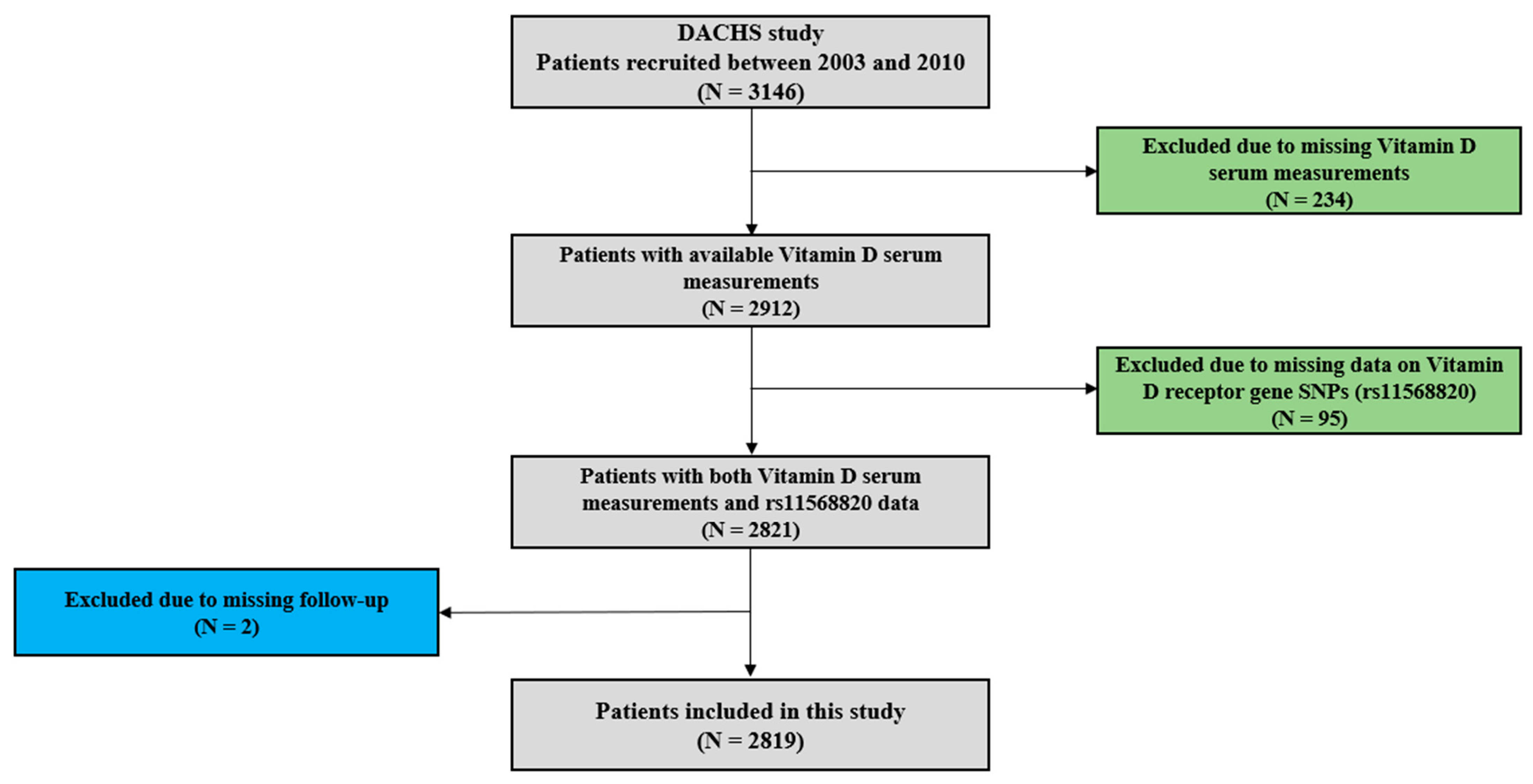
2.1. Study Details
2.2. Serum Vitamin D Measurements
2.3. Genotyping for Cdx2
2.4. Outcomes
2.5. Statistical Analyses
3. Results
3.1. Description of Patient Characteristics
3.2. Vitamin D Status and Survival
3.3. VDR Cdx2 Locus Genotypes and Survival
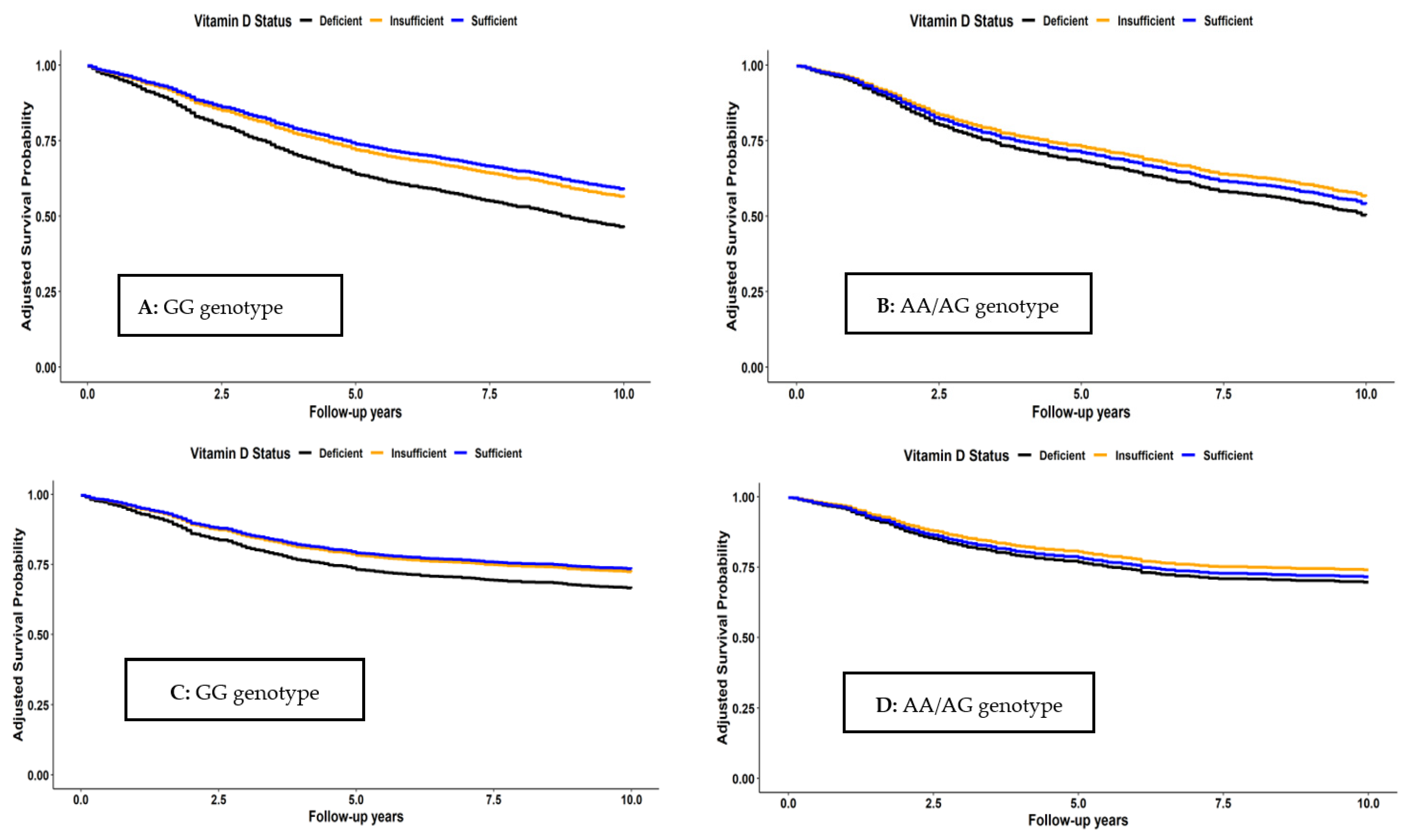
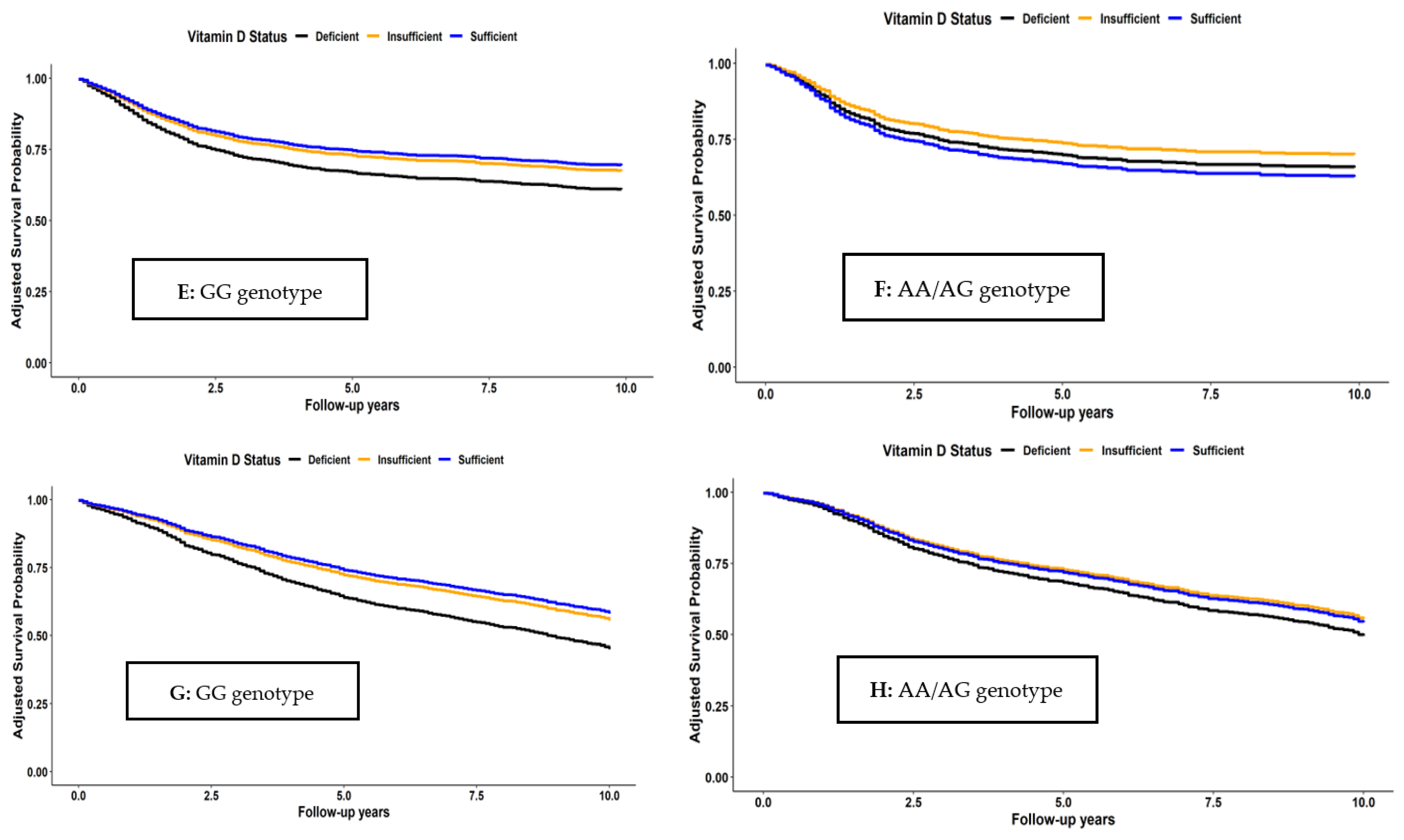
3.4. Joint Associations of Vitamin D Status and VDR Cdx2 Locus Genotypes with Survival
4. Discussion
4.1. Vitamin D Status and Survival
4.2. VDR Cdx2 Locus Genotypes and Survival
4.3. Joint Associations of Vitamin D Status and Cdx2 Genotypes with Survival
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Zgaga, L.; Theodoratou, E.; Farrington, S.M.; Din, F.V.; Ooi, L.Y.; Glodzik, D.; Johnston, S.; Tenesa, A.; Campbell, H.; Dunlop, M.G. Plasma vitamin D concentration influences survival outcome after a diagnosis of colorectal cancer. J. Clin. Oncol. 2014, 32, 2430–2439. [Google Scholar] [CrossRef] [PubMed]
- Maalmi, H.; Walter, V.; Jansen, L.; Chang-Claude, J.; Owen, R.W.; Ulrich, A.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Relationship of very low serum 25-hydroxyvitamin D(3) levels with long-term survival in a large cohort of colorectal cancer patients from Germany. Eur. J. Epidemiol. 2017, 32, 961–971. [Google Scholar] [CrossRef]
- Maalmi, H.; Walter, V.; Jansen, L.; Boakye, D.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients 2018, 10, 896. [Google Scholar] [CrossRef]
- Wu, G.; Xue, M.; Zhao, Y.; Han, Y.; Zhang, S.; Zhang, J.; Li, C.; Xu, J. Low circulating 25-hydroxyvitamin D level is associated with increased colorectal cancer mortality: A systematic review and dose-response meta-analysis. Biosci. Rep. 2020, 40, BSR20201008. [Google Scholar] [CrossRef] [PubMed]
- Vaughan-Shaw, P.G.; Buijs, L.F.; Blackmur, J.P.; Theodoratou, E.; Zgaga, L.; Din, F.V.N.; Farrington, S.M.; Dunlop, M.G. The effect of vitamin D supplementation on survival in patients with colorectal cancer: Systematic review and meta-analysis of randomised controlled trials. Br. J. Cancer 2020, 123, 1705–1712. [Google Scholar] [CrossRef] [PubMed]
- Vaughan-Shaw, P.G.; Zgaga, L.; Ooi, L.Y.; Theodoratou, E.; Timofeeva, M.; Svinti, V.; Walker, M.; O’Sullivan, F.; Ewing, A.; Johnston, S.; et al. Low plasma vitamin D is associated with adverse colorectal cancer survival after surgical resection, independent of systemic inflammatory response. Gut 2020, 69, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Chang-Claude, J.; Seiler, C.M.; Rickert, A.; Hoffmeister, M. Protection from colorectal cancer after colonoscopy: A population-based, case-control study. Ann. Intern. Med. 2011, 154, 22–30. [Google Scholar] [CrossRef]
- Brenner, H.; Chang-Claude, J.; Jansen, L.; Knebel, P.; Stock, C.; Hoffmeister, M. Reduced risk of colorectal cancer up to 10 years after screening, surveillance, or diagnostic colonoscopy. Gastroenterology 2014, 146, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Carr, P.R.; Jansen, L.; Walter, V.; Kloor, M.; Roth, W.; Bläker, H.; Chang-Claude, J.; Brenner, H.; Hoffmeister, M. Associations of red and processed meat with survival after colorectal cancer and differences according to timing of dietary assessment. Am. J. Clin. Nutr. 2016, 103, 192–200. [Google Scholar] [CrossRef]
- Walter, V.; Jansen, L.; Ulrich, A.; Roth, W.; Bläker, H.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Alcohol consumption and survival of colorectal cancer patients: A population-based study from Germany. Am. J. Clin. Nutr. 2016, 103, 1497–1506. [Google Scholar] [CrossRef]
- Phinney, K.W. Development of a standard reference material for vitamin D in serum. Am. J. Clin. Nutr. 2008, 88, 511s–512s. [Google Scholar] [CrossRef]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Institute of Medicine Committee to Review Dietary Reference Intakes for Calcium and Vitamin D; National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar]
- Perna, L.; Hoffmeister, M.; Schöttker, B.; Arndt, V.; Haug, U.; Holleczek, B.; Burwinkel, B.; Ordóñez-Mena, J.M.; Brenner, H. Vitamin D receptor polymorphism and colorectal cancer-specific and all-cause mortality. Cancer Epidemiol. 2013, 37, 905–907. [Google Scholar] [CrossRef]
- Chen, X.; Li, H.; Guo, F.; Hoffmeister, M.; Brenner, H. Alcohol consumption, polygenic risk score, and early- and late-onset colorectal cancer risk. EClinicalMedicine 2022, 49, 101460. [Google Scholar] [CrossRef]
- Guo, F.; Edelmann, D.; Cardoso, R.; Chen, X.; Carr, P.R.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Polygenic Risk Score for Defining Personalized Surveillance Intervals After Adenoma Detection and Removal at Colonoscopy. Clin. Gastroenterol. Hepatol. 2023, 21, 210–219.e211. [Google Scholar] [CrossRef]
- Gupta, S.; Lieberman, D.; Anderson, J.C.; Burke, C.A.; Dominitz, J.A.; Kaltenbach, T.; Robertson, D.J.; Shaukat, A.; Syngal, S.; Rex, D.K. Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Am. J. Gastroenterol. 2020, 115, 415–434. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Li, Y.; Gong, Y.; Huang, Q.; Cai, S.; Peng, J. Vitamin D Status and Survival in Stage II-III Colorectal Cancer. Front. Oncol. 2020, 10, 581597. [Google Scholar] [CrossRef]
- Zhou, J.; Ge, X.; Fan, X.; Wang, J.; Miao, L.; Hang, D. Associations of vitamin D status with colorectal cancer risk and survival. Int. J. Cancer 2021, 149, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Weng, Y.T.; Hsieh, N.T.; Li, P.C.; Lee, T.Y.; Li, C.I.; Liu, H.S.; Lee, M.F. Bioactive Vitamin D Attenuates MED28-Mediated Cell Growth and Epithelial-Mesenchymal Transition in Human Colorectal Cancer Cells. Biomed. Res. Int. 2022, 2022, 2268818. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Weng, Y.T.; Li, P.C.; Hsieh, N.T.; Li, C.I.; Liu, H.S.; Lee, M.F. Calcitriol Suppresses Warburg Effect and Cell Growth in Human Colorectal Cancer Cells. Life 2021, 11, 963. [Google Scholar] [CrossRef]
- Latacz, M.; Snarska, J.; Kostyra, E.; Fiedorowicz, E.; Savelkoul, H.F.; Grzybowski, R.; Cieślińska, A. Single Nucleotide Polymorphisms in 25-Hydroxyvitamin D3 1-Alpha-Hydroxylase (CYP27B1) Gene: The Risk of Malignant Tumors and Other Chronic Diseases. Nutrients 2020, 12, 801. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, L.; Xu, H.J.; Li, Y.; Hu, C.M.; Yang, J.Y.; Sun, M.Y. The Anti-Inflammatory Effects of Vitamin D in Tumorigenesis. Int. J. Mol. Sci. 2018, 19, 2736. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hou, J.; Xiao, Z.; Zhao, Y.; Du, F.; Wu, X.; Li, M.; Chen, Y.; Zhang, L.; Cho, C.H.; et al. The Role of Vitamin D in Gastrointestinal Diseases: Inflammation, Gastric Cancer, and Colorectal Cancer. Curr. Med. Chem. 2022, 29, 3836–3856. [Google Scholar] [CrossRef] [PubMed]
- Flügge, J.; Krusekopf, S.; Goldammer, M.; Osswald, E.; Terhalle, W.; Malzahn, U.; Roots, I. Vitamin D receptor haplotypes protect against development of colorectal cancer. Eur. J. Clin. Pharmacol. 2007, 63, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Ochs-Balcom, H.M.; Cicek, M.S.; Thompson, C.L.; Tucker, T.C.; Elston, R.C.; S, J.P.; Casey, G.; Li, L. Association of vitamin D receptor gene variants, adiposity and colon cancer. Carcinogenesis 2008, 29, 1788–1793. [Google Scholar] [CrossRef]
- Theodoratou, E.; Farrington, S.M.; Tenesa, A.; McNeill, G.; Cetnarskyj, R.; Barnetson, R.A.; Porteous, M.E.; Dunlop, M.G.; Campbell, H. Modification of the inverse association between dietary vitamin D intake and colorectal cancer risk by a FokI variant supports a chemoprotective action of Vitamin D intake mediated through VDR binding. Int. J. Cancer 2008, 123, 2170–2179. [Google Scholar] [CrossRef]
- Slattery, M.L.; Wolff, R.K.; Curtin, K.; Fitzpatrick, F.; Herrick, J.; Potter, J.D.; Caan, B.J.; Samowitz, W.S. Colon tumor mutations and epigenetic changes associated with genetic polymorphism: Insight into disease pathways. Mutat. Res. 2009, 660, 12–21. [Google Scholar] [CrossRef]
- Bentley, R.W.; Keown, D.A.; Gearry, R.B.; Cameron, V.A.; Keenan, J.; Roberts, R.L.; Day, A.S. Vitamin D receptor polymorphisms in colorectal cancer in New Zealand: An association study. N. Z. Med. J. 2012, 125, 47–51. [Google Scholar]
- Serrano, D.; Gnagnarella, P.; Raimondi, S.; Gandini, S. Meta-analysis on vitamin D receptor and cancer risk: Focus on the role of TaqI, ApaI, and Cdx2 polymorphisms. Eur. J. Cancer Prev. 2016, 25, 85–96. [Google Scholar] [CrossRef]
- Fang, Y.; van Meurs, J.B.; Bergink, A.P.; Hofman, A.; van Duijn, C.M.; van Leeuwen, J.P.; Pols, H.A.; Uitterlinden, A.G. Cdx-2 polymorphism in the promoter region of the human vitamin D receptor gene determines susceptibility to fracture in the elderly. J. Bone Miner. Res. 2003, 18, 1632–1641. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.; Bellerba, F.; Corso, F.; De Angelis, S.P.; Belloni, P.; Caini, S.; Gandini, S. Ethnicity as modifier of risk for Vitamin D receptors polymorphisms: Comprehensive meta-analysis of all cancer sites. Crit. Rev. Oncol. Hematol. 2021, 158, 103202. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Mayorga, G.; Gómez-López, G.; Barbáchano, A.; Fernández-Barral, A.; Peña, C.; Pisano, D.G.; Cantero, R.; Rojo, F.; Muñoz, A.; Larriba, M.J. Vitamin D receptor expression and associated gene signature in tumour stromal fibroblasts predict clinical outcome in colorectal cancer. Gut 2017, 66, 1449–1462. [Google Scholar] [CrossRef]
- Shi, Q.; Han, X.P.; Yu, J.; Peng, H.; Chen, Y.Z.; Li, F.; Cui, X.B. Decreased vitamin D receptor protein expression is associated with progression and poor prognosis of colorectal cancer patients. Int. J. Clin. Exp. Pathol. 2020, 13, 746–755. [Google Scholar] [PubMed]
- Al-Ghafari, A.B.; Balamash, K.S.; Al Doghaither, H.A. Serum vitamin D receptor (VDR) levels as a potential diagnostic marker for colorectal cancer. Saudi. J. Biol. Sci. 2020, 27, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Miyamoto, K.I.; Yoshida, M.; Yamamoto, H.; Taketani, Y.; Morita, K.; Kubota, M.; Yoshida, S.; Ikeda, M.; Watabe, F.; et al. The polymorphism in the caudal-related homeodomain protein Cdx-2 binding element in the human vitamin D receptor gene. J. Bone Miner. Res. 2001, 16, 1256–1264. [Google Scholar] [CrossRef]
- Brenner, H.; Jansen, L.; Saum, K.U.; Holleczek, B.; Schöttker, B. Vitamin D Supplementation Trials Aimed at Reducing Mortality Have Much Higher Power When Focusing on People with Low Serum 25-Hydroxyvitamin D Concentrations. J. Nutr. 2017, 147, 1325–1333. [Google Scholar] [CrossRef]
- Grant, W.B.; Boucher, B.J.; Al Anouti, F.; Pilz, S. Comparing the Evidence from Observational Studies and Randomized Controlled Trials for Nonskeletal Health Effects of Vitamin D. Nutrients 2022, 14, 3811. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | % | |
|---|---|---|---|
| Sex | Female | 1136 | 40.3 |
| Male | 1683 | 59.7 | |
| Age at diagnosis (years) | Median (IQR) | 69 (62–76) | |
| 30–59 | 553 | 19.6 | |
| 60–69 | 914 | 32.4 | |
| 70–79 | 923 | 32.7 | |
| 80+ | 429 | 15.2 | |
| UICC Cancer Stage (TNM) | I | 650 | 23.1 |
| II | 879 | 31.3 | |
| III | 889 | 31.7 | |
| IV | 391 | 13.9 | |
| Cancer Site | Colon | 1687 | 59.8 |
| Rectum | 1132 | 40.2 | |
| Serum 25(OH)D | <30 nmol/L | 1675 | 59.4 |
| 30–49 nmol/L | 695 | 24.7 | |
| ≥50 nmol/L | 449 | 15.9 | |
| Cdx2 genotype | AA | 122 | 4.3 |
| AG | 872 | 30.9 | |
| GG | 1825 | 64.7 | |
| Body Mass Index [kg/m2] | Median (IQR) | 26.1 (23.6–29.0) | |
| <25 | 1077 | 38.2 | |
| 25- < 30 | 1208 | 42.9 | |
| ≥30 | 534 | 18.9 | |
| Tumour detected by screening | Yes | 658 | 23.4 |
| No | 2161 | 76.6 | |
| Surgical treatment for CRC | Yes | 2744 | 97.3 |
| No | 75 | 2.7 | |
| Received chemotherapy | Yes | 1287 | 45.9 |
| No | 1532 | 54.1 | |
| History of cardiovascular disease | Yes | 709 | 25.8 |
| No | 2110 | 74.2 | |
| History of diabetes | Yes | 521 | 18.5 |
| No | 2298 | 81.5 | |
| History of hypertension | Yes | 1445 | 51.3 |
| No | 1374 | 48.7 | |
| Smoking exposure (lifetime pack-years) | Never | 1280 | 45.7 |
| <10 | 501 | 17.9 | |
| 10–19 | 365 | 13.0 | |
| 20–29 | 278 | 9.9 | |
| ≥30 | 379 | 13.5 | |
| Alcohol consumption 1 | None | 818 | 29.4 |
| Low | 1253 | 45.1 | |
| High | 710 | 25.5 | |
| Physical activity 2 | Low | 923 | 33.4 |
| Moderate | 920 | 33.3 | |
| High | 917 | 33.2 | |
| School education [yrs.] | <9 | 1914 | 68.1 |
| 9–10 | 470 | 16.7 | |
| ≥10 | 428 | 15.2 | |
| Late entry 3 | ≤1 month | 1400 | 51.9 |
| >1 month | 1300 | 48.1 | |
| Season of blood draw | Spring | 780 | 27.7 |
| Summer | 756 | 26.8 | |
| Autumn | 671 | 23.8 | |
| Winter | 612 | 21.7 | |
| Vitamin D Status | Cdx2 Genotype | ||
|---|---|---|---|
| GG | AG | AA | |
| Deficient | 1100 (60) | 502 (58) | 73 (60) |
| Insufficient | 443 (24) | 220 (25) | 32 (26) |
| Sufficient | 282 (15) | 150 (17) | 17 (14) |
| Total | 1825 (100) | 872 (100) | 122 (100) |
| Survival Endpoint | Predictor | N/Events | Hazard Ratio (95% CI) | ||
|---|---|---|---|---|---|
| Model 1 * | Model 2 ** | ||||
| Overall | Serum 25(OH)D | <30 nmol/L | 1673/1012 | 1.00 (ref) | 1.00 (ref) |
| 30–49 nmol/L | 695/317 | 0.67 (0.59–0.75) | 0.73 (0.63–0.85) | ||
| ≥50 nmol/L | 449/190 | 0.62 (0.53–0.72) | 0.71 (0.59–0.84) | ||
| Cdx2 genotype | GG | 1824/999 | 1.00 (ref) | 1.00 (ref) | |
| AA or AG | 993/520 | 0.95 (0.86–1.06) | 0.99 (0.88–1.11) | ||
| CRC-specific | Serum 25(OH)D | <30 nmol/L | 1657/542 | 1.00 (ref) | 1.00 (ref) |
| 30–49 nmol/L | 686/154 | 0.61 (0.51–0.73) | 0.72 (0.59–0.89) | ||
| ≥50 nmol/L | 442/102 | 0.61 (0.49–0.75) | 0.76 (0.60–0.95) | ||
| Cdx2 genotype | GG | 1806/534 | 1.00 (ref) | 1.00 (ref) | |
| AA or AG | 979/264 | 0.90 (0.78–1.05) | 0.93 (0.80–1.09) | ||
| Recurrence-free | Serum 25(OH)D | <30 nmol/L | 1662/612 | 1.00 (ref) | 1.00 (ref) |
| 30–49 nmol/L | 690/187 | 0.65 (0.55–0.76) | 0.76 (0.64–0.90) | ||
| ≥50 nmol/L | 444/119 | 0.62 (0.51–0.76) | 0.79 (0.64–0.98) | ||
| Cdx2 genotype | GG | 1811/603 | 1.00 (ref) | 1.00 (ref) | |
| AA or AG | 985/314 | 0.95 (0.83–1.09) | 0.97 (0.84–1.11) | ||
| Disease-free | Serum 25(OH)D | <30 nmol/L | 1661/1034 | 1.00 (ref) | 1.00 (ref) |
| 30–49 nmol/L | 690/331 | 0.67 (0.59–0.76) | 0.73 (0.62–0.85) | ||
| ≥50 nmol/L | 444/194 | 0.60 (0.51–0.70) | 0.69 (0.58–0.82) | ||
| Cdx2 genotype | GG | 1810/1026 | 1.00 (ref) | 1.00 (ref) | |
| AA or AG | 985/533 | 0.95 (0.86–1.06) | 0.98 (0.88–1.10) | ||
| Survival Endpoint | Cdx2 Genotype | 25(OH)D | N/Events | Adjusted Hazard Ratio (95% CI) * | Ptrend |
|---|---|---|---|---|---|
| Overall | GG | <30 nmol/L | 1099/683 | 1.00 (ref) | <0.001 |
| 30–49 nmol/L | 443/200 | 0.69 (0.56–0.84) | |||
| ≥50 nmol/L | 282/116 | 0.63 (0.50–0.78) | |||
| AA or AG | <30 nmol/L | 574/329 | 1.00 (ref) | 0.08 | |
| 30–49 nmol/L | 252/117 | 0.77 (0.61–0.98) | |||
| ≥50 nmol/L | 167/74 | 0.85 (0.64–1.13) | |||
| Pinteraction | 0.33 | ||||
| CRC-specific | GG | <30 nmol/L | 1091/370 | 1.00 (ref) | 0.002 |
| 30–49 nmol/L | 439/102 | 0.71 (0.55–0.92) | |||
| ≥50 nmol/L | 276/62 | 0.68 (0.50–0.90) | |||
| AA or AG | <30 nmol/L | 566/172 | 1.00 (ref) | 0.24 | |
| 30–49 nmol/L | 247/53 | 0.74 (0.52–1.05) | |||
| ≥50 nmol/L | 166/40 | 0.87 (0.59–1.29) | |||
| Pinteraction | 0.88 | ||||
| Recurrence-free | GG | <30 nmol/L | 1090/411 | 1.00 (ref) | <0.001 |
| 30–49 nmol/L | 440/120 | 0.73 (0.58–0.91) | |||
| ≥50 nmol/L | 281/71 | 0.66 (0.51–0.86) | |||
| AA or AG | <30 nmol/L | 572/200 | 1.00 (ref) | 0.99 | |
| 30–49 nmol/L | 250/67 | 0.79 (0.58–1.07) | |||
| ≥50 nmol/L | 163/47 | 1.13 (0.79–1.61) | |||
| Pinteraction | 0.50 | ||||
| Disease-free | GG | <30 nmol/L | 1089/696 | 1.00 (ref) | <0.001 |
| 30–49 nmol/L | 440/209 | 0.68 (0.56–0.83) | |||
| ≥50 nmol/L | 281/121 | 0.62 (0.50–0.77) | |||
| AA or AG | <30 nmol/L | 572/338 | 1.00 (ref) | 0.04 | |
| 30–49 nmol/L | 250/122 | 0.78 (0.62–0.99) | |||
| ≥50 nmol/L | 163/73 | 0.81 (0.61–1.08) | |||
| Pinteraction | 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gwenzi, T.; Schrotz-King, P.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Vitamin D Status, Cdx2 Genotype, and Colorectal Cancer Survival: Population-Based Patient Cohort. Nutrients 2023, 15, 2717. https://doi.org/10.3390/nu15122717
Gwenzi T, Schrotz-King P, Schöttker B, Hoffmeister M, Brenner H. Vitamin D Status, Cdx2 Genotype, and Colorectal Cancer Survival: Population-Based Patient Cohort. Nutrients. 2023; 15(12):2717. https://doi.org/10.3390/nu15122717
Chicago/Turabian StyleGwenzi, Tafirenyika, Petra Schrotz-King, Ben Schöttker, Michael Hoffmeister, and Hermann Brenner. 2023. "Vitamin D Status, Cdx2 Genotype, and Colorectal Cancer Survival: Population-Based Patient Cohort" Nutrients 15, no. 12: 2717. https://doi.org/10.3390/nu15122717
APA StyleGwenzi, T., Schrotz-King, P., Schöttker, B., Hoffmeister, M., & Brenner, H. (2023). Vitamin D Status, Cdx2 Genotype, and Colorectal Cancer Survival: Population-Based Patient Cohort. Nutrients, 15(12), 2717. https://doi.org/10.3390/nu15122717