
Youth and Peer Mentor Led Interventions to Improve Biometric-, Nutrition, Physical Activity, and Psychosocial-Related Outcomes in Children and Adolescents: A Systematic Review


Abstract
1. Introduction
- Examine the training of peers and implementation of peer roles when developing peer-led nutrition and physical activity interventions.
- Evaluate the extent to which peer-led nutrition and physical activity interventions had an effect on biometrics, nutrition, physical activity, and psychosocial outcomes on child and adolescent intervention participants.
- Evaluate to what extent peer-led nutrition and physical activity interventions had an effect on biometrics, nutrition, physical activity, and psychosocial outcomes on the peers themselves.
- Evaluate process outcomes of the peer-led nutrition and physical activity interventions.
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
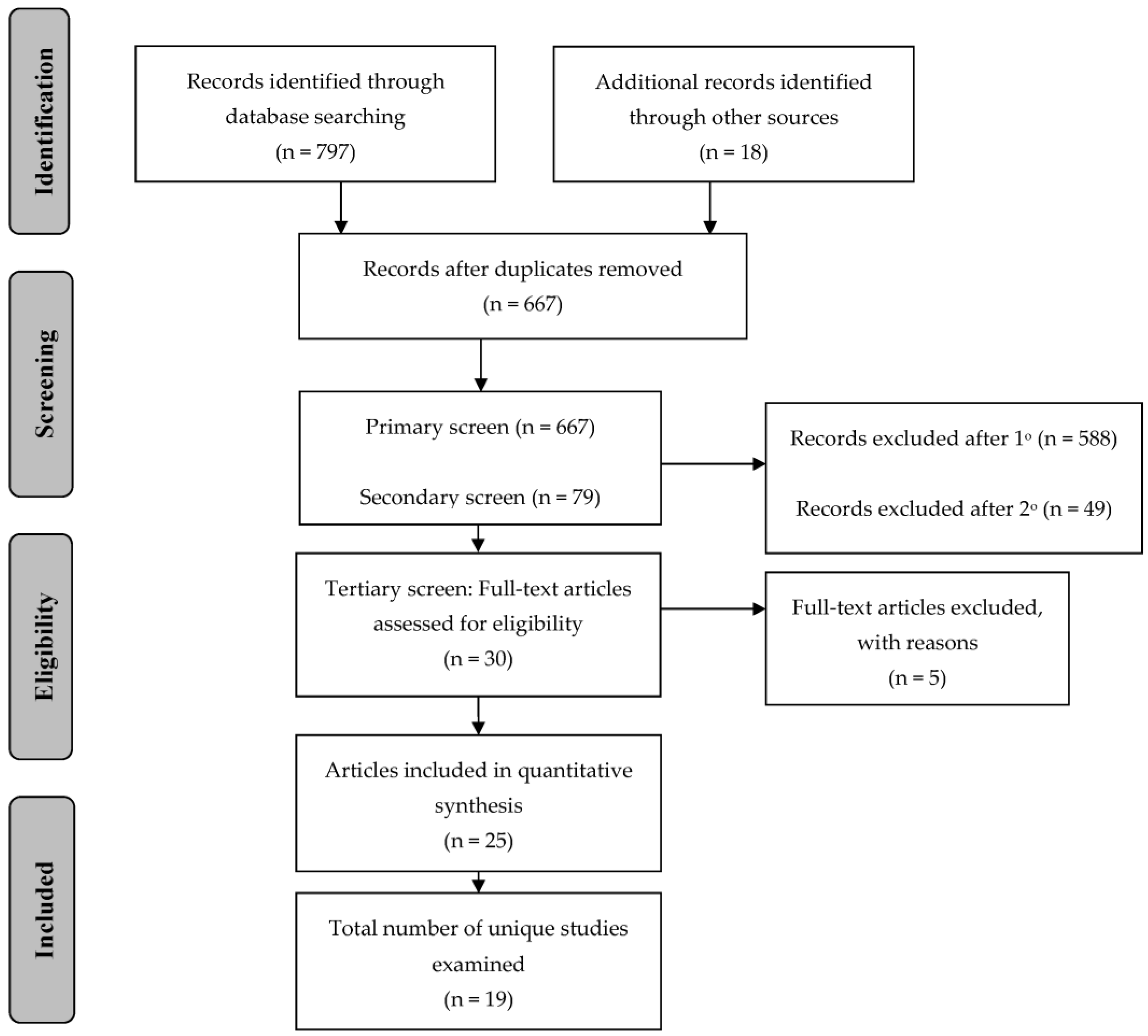
2.3. Screening Protocol
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Definition of “Youth” and “Peer”
3. Results
3.1. Overview of the Intervention Trials
3.2. Training of Youth Mentors and Peer Mentors
3.3. Child and Adolescent Participant Outcomes
3.3.1. Biometric Outcomes
3.3.2. Nutrition Outcomes
Nutrition Outcomes: Dietary Intake
3.3.3. Physical Activity Outcomes
Physical Activity Outcomes: Physical Activity Behaviors
3.4. Youth and Peer Mentors Outcomes
3.4.1. Biometric Outcomes
3.4.2. Nutrition Outcomes
3.4.3. Physical Activity Outcomes
3.5. Process Evaluation
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
Appendix A.1. B’more Healthy Communities for Kids (BHCK) [34]
Appendix A.2. Challenge! [29,35]
Appendix A.3. Cool Girls, Inc. [36]
Appendix A.4. Fluids Used Effectively for Living (FUEL) [37]
Appendix A.5. Girls Active Project [38,39]
Appendix A.6. HealthCorps [41]
Appendix A.7. Healthy Buddies [42]
Appendix A.8. Heart Healthy Kids Program (H2K) [43]
Appendix A.9. Just for Kids! [44,45]
Appendix A.10. Mentoring to Be Active (MBA) [46]
Appendix A.11. Peer Education about Weight Steadiness [50]
Appendix A.12. Peer-Led Physical Activity iNtervention for Adolescent Girls (PLAN-A) [48,49]
Appendix A.13. Slice of Life [51]
Appendix A.14. Students for Nutrition and Exercise (SNaX) [52]
Appendix A.15. Trying Alternative Cafeteria Options in Schools (TACOS) [15,53]
Appendix A.16. Teens Eating for Energy and Nutrition at School (TEENS) [16,54,55]
Appendix A.17. The WISH Study [56]
References
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Childhood and Adult Obesity in the United States, 2011–2012. J. Am. Med. Assoc. 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Bryan, S.; Afful, J.; Carroll, M.; Te-Ching, C.; Orlando, D.; Fink, S.; Fryar, C. NHSR 158. National Health and Nutrition Examination Survey 2017–March 2020 Pre-pandemic Data Files; NHSR: Hyattsville, MD, USA, 2021. [CrossRef]
- Halfon, N.; Larson, K.; Slusser, W. Associations Between Obesity and Comorbid Mental Health, Developmental, and Physical Health Conditions in a Nationally Representative Sample of US Children Aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Taras, H.; Potts-Datema, W. Obesity and Student Performance at School. J. Sch. Health 2005, 75, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, J.; Semmler, C.; Carnell, S.; Van Jaarsveld, C.H.; Wardle, J. Continuity and stability of eating behaviour traits in children. Eur. J. Clin. Nutr. 2008, 62, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice Hall: Engelwood, NJ, USA, 1986. [Google Scholar]
- Bandura, A. Social Learning Theory; Prentice Hall: Engelwood, NJ, USA, 1977. [Google Scholar]
- McGuire, W.J. Inducing Resistance to Persuasion: Some Contemporary Approaches; Elesiver: Amsterdam, The Netherlands, 1964; pp. 191–212. [Google Scholar] [CrossRef]
- Baric, L.; Harrison, A. Social Pressure and Health Education. J. Inst. Health Educ. 1977, 15, 12–18. [Google Scholar] [CrossRef]
- Lindsey, B.J. Peer Education: A Viewpoint and Critique. J. Am. Coll. Health 1997, 45, 187–189. [Google Scholar] [CrossRef]
- Mellanby, A.R.; Rees, J.B.; Tripp, J.H. Peer-led and adult-led school health education: A critical review of available comparative research. Health Educ. Res. 2000, 15, 533–545. [Google Scholar] [CrossRef]
- Perry, C.; Kelder, S.; Komro, K. The Social World of Adolescents: Families, Peers, School, and the Community. In Promoting the Health of Adolescents: New Directions for the Twenty-First Century; Millstein, S., Petersen, A., Nightingale, E., Eds.; Oxford University Press, Inc.: New York, NY, USA, 1993; pp. 73–96. [Google Scholar]
- French, S.A.; Story, M.; Fulkerson, J.A.; Hannan, P. An Environmental Intervention to Promote Lower-Fat Food Choices in Secondary Schools: Outcomes of the TACOS Study. Am. J. Public Health 2004, 94, 1507–1512. [Google Scholar] [CrossRef]
- Birnbaum, A.S.; Lytle, L.A.; Story, M.; Perry, C.L.; Murray, D.M. Are Differences in Exposure to a Multicomponent School-Based Intervention Associated with Varying Dietary Outcomes in Adolescents? Health Educ. Behav. 2002, 29, 427–443. [Google Scholar] [CrossRef]
- Black, D.R.; Tobler, N.S.; Sciacca, J.P. Peer helping/involvement: An efficacious way to meet the challenge of reducing alcohol, tobacco, and other drug use among youth? J. Sch. Health 1998, 68, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Fors, S.W.; Jarvis, S. Evaluation of a Peer-Led Drug Abuse Risk Reduction Project for Runaway/Homeless Youths. J. Drug Educ. 1995, 25, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Klepp, K.-I.; Halper, A.; Perry, C.L. The Efficacy of Peer Leaders in Drug Abuse Prevention. J. Sch. Health 1986, 56, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Komro, K.A.; Perry, C.L.; Murray, D.M.; Veblen-Mortenson, S.; Williams, C.L.; Anstine, P.S. Peer-Planned Social Activities for Preventing Alcohol Use among Young Adolescents. J. Sch. Health 1996, 66, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Orpinas, P.; Parcel, G.S.; Mcalister, A.; Frankowski, R. Violence prevention in middle schools: A pilot evaluation. J. Adolesc. Health 1995, 17, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.L. Prevention of Alcohol Use and Abuse in Adolescence: Teacher- vs Peer-led Intervention. Crisis 1989, 10, 52–61. [Google Scholar]
- Sawyer, R.G.; Pinciaro, P.; Bedwell, D. How Peer Education Changed Peer Sexuality Educators’ Self-Esteem, Personal Development, and Sexual Behavior. J. Am. Coll. Health 1997, 45, 211–217. [Google Scholar] [CrossRef]
- Beier, S.R.; Rosenfeld, W.D.; Spitalny, K.C.; Zansky, S.M.; Bontempo, A.N. The Potential Role of an Adult Mentor in Influencing High-Risk Behaviors in Adolescents. Arch. Pediatr. Adolesc. Med. 2000, 154, 327–331. [Google Scholar] [CrossRef]
- Zimmerman, M.A.; Bingenheimer, J.B.; Notaro, P.C. Natural Mentors and Adolescent Resiliency: A Study with Urban Youth. Am. J. Community Psychol. 2002, 30, 221–243. [Google Scholar] [CrossRef]
- DuBois, D.L.; Silverthorn, N. Natural Mentoring Relationships and Adolescent Health: Evidence from a National Study. Am. J. Public Health 2005, 95, 518–524. [Google Scholar] [CrossRef]
- Klaw, E.L.; Rhodes, J.E. Mentor Relationships and the Career Development of Pregnant and Parenting African-American Teenagers. Psychol. Women Q. 1995, 19, 551–562. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.E.; Grossman, J.B.; Resch, N.L. Agents of change: Pathways through which mentoring relationships influence adolescents’ academic adjustment. Child Dev. 2000, 71, 1662–1671. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Arteaga, S.S.; Sanders, J.; Hager, E.R.; Anliker, J.A.; Gittelsohn, J.; Wang, Y. College Mentors. Health Promot. Pract. 2010, 13, 238–244. [Google Scholar] [CrossRef] [PubMed]
- McHale, F.; Ng, K.; Taylor, S.; Bengoechea, E.; Norton, C.; O’shea, D.; Woods, C. A Systematic Literature Review of Peer-led Strategies for Promoting Physical Activity Levels of Adolescents. Health Educ. Behav. 2021, 49, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.; Gates, M.; Gates, A.; Hanning, R.M. Peer-led nutrition education programs for school-aged youth: A systematic review of the literature. Health Educ. Res. 2015, 31, cyv063. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.E. Improving Youth Mentoring Interventions Through Research-based Practice. Am. J. Community Psychol. 2008, 41, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Trude, A.C.B.; Surkan, P.J.; Cheskin, L.J.; Gittelsohn, J. A multilevel, multicomponent childhood obesity prevention group-randomized controlled trial improves healthier food purchasing and reduces sweet-snack consumption among low-income African-American youth. Nutr. J. 2018, 17, 96. [Google Scholar] [CrossRef]
- Black, M.M.; Hager, E.R.; Le, K.; Anliker, J.; Arteaga, S.S.; DiClemente, C.; Gittelsohn, J.; Magder, L.; Papas, M.; Snitker, S.; et al. Challenge! Health Promotion/Obesity Prevention Mentorship Model among Urban, Black Adolescents. Pediatrics 2010, 126, 280–288. [Google Scholar] [CrossRef]
- Kuperminc, G.P.; Thomason, J.; DiMeo, M.; Broomfield-Massey, K. Cool Girls, Inc.: Promoting the Positive Development of Urban Preadolescent and Early Adolescent Girls. J. Prim. Prev. 2011, 32, 171–183. [Google Scholar] [CrossRef]
- Lo, E.; Coles, R.; Humbert, M.L.; Polowski, J.; Henry, C.J.; Whiting, S.J. Beverage intake improvement by high school students in Saskatchewan, Canada. Nutr. Res. 2008, 28, 144–150. [Google Scholar] [CrossRef] [PubMed]
- McQuinn, S.; Belton, S.; Staines, A.; Sweeney, M.R. Co-design of a school-based physical activity intervention for adolescent females in a disadvantaged community: Insights from the Girls Active Project (GAP). BMC Public Health 2022, 22, 615. [Google Scholar] [CrossRef] [PubMed]
- Harrington, D.M.; Davies, M.J.; Bodicoat, D.; Charles, J.M.; Chudasama, Y.V.; Gorely, T.; Khunti, K.; Rowlands, A.V.; Sherar, L.B.; Tudor-Edwards, R.; et al. A school-based intervention (‘Girls Active’) to increase physical activity levels among 11- to 14-year-old girls: Cluster RCT. Public Health Res. 2019, 7, 1–162. [Google Scholar] [CrossRef]
- Dowd, A.J.; Chen, M.Y.; Jung, M.E.; Beauchamp, M.R. “Go Girls!”: Psychological and behavioral outcomes associated with a group-based healthy lifestyle program for adolescent girls. Transl. Behav. Med. 2014, 5, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Cawley, J.; Cisek-Gillman, L.; Roberts, R.; Cocotas, C.; Smith-Cook, T.; Bouchard, M.; Oz, M. Effect of HealthCorps, a High School Peer Mentoring Program, on Youth Diet and Physical Activity. Child. Obes. 2011, 7, 364–371. [Google Scholar] [CrossRef]
- Stock, S.; Miranda, C.; Evans, S.; Plessis, S.; Ridley, J.; Yeh, S.; Chanoine, J.-P. Healthy Buddies: A Novel, Peer-Led Health Promotion Program for the Prevention of Obesity and Eating Disorders in Children in Elementary School. Pediatrics 2007, 120, e1059–e1068. [Google Scholar] [CrossRef]
- Spencer, R.; Bower, J.; Kirk, S.; Friesen, C.H. Peer Mentoring Is Associated with Positive Change in Physical Activity and Aerobic Fitness of Grades 4, 5, and 6 Students in the Heart Healthy Kids Program. Health Promot. Pract. 2014, 15, 803–811. [Google Scholar] [CrossRef]
- Smith, L.H. Piloting the use of teen mentors to promote a healthy diet and physical activity among children in Appalachia. J. Spéc. Pediatr. Nurs. 2011, 16, 16–26. [Google Scholar] [CrossRef]
- Smith, L.H.; Holloman, C. Comparing the Effects of Teen Mentors to Adult Teachers on Child Lifestyle Behaviors and Health Outcomes in Appalachia. J. Sch. Nurs. 2013, 29, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.H.; Petosa, R.L.; Laurent, D. Efficacy of “Mentoring to Be Active” on Weight Loss, Body Mass Index, and Body Fat among Obese and Extremely Obese Youth in Rural Appalachia. J. Rural. Health 2019, 36, 77–87. [Google Scholar] [CrossRef]
- Tymms, P.B.; Curtis, S.E.; Routen, A.; Thomson, K.H.; Bolden, D.; Bock, S.C.; Dunn, C.E.; Cooper, A.; Elliott, J.G.; Moore, H.; et al. Clustered randomised controlled trial of two education interventions designed to increase physical activity and well-being of secondary school students: The MOVE Project. BMJ Open 2016, 6, e009318. [Google Scholar] [CrossRef] [PubMed]
- Sebire, S.J.; Banfield, K.; Jago, R.; Edwards, M.J.; Campbell, R.; Kipping, R.; Blair, P.S.; Kadir, B.; Garfield, K.; Matthews, J.; et al. A process evaluation of the PLAN-A intervention (Peer-Led physical Activity iNtervention for Adolescent girls). BMC Public Health 2019, 19, 1203. [Google Scholar] [CrossRef] [PubMed]
- Sebire, S.J.; Jago, R.; Banfield, K.; Edwards, M.J.; Campbell, R.; Kipping, R.; Blair, P.S.; Kadir, B.; Garfield, K.; Matthews, J.; et al. Results of a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Int. J. Behav. Nutr. Phys. Act. 2018, 15, 50. [Google Scholar] [CrossRef] [PubMed]
- Muzaffar, H.; Nikolaus, C.J.; Ogolsky, B.G.; Lane, A.; Liguori, C.; Nickols-Richardson, S.M. Promoting Cooking, Nutrition, and Physical Activity in Afterschool Settings. Am. J. Health Behav. 2019, 43, 1050–1063. [Google Scholar] [CrossRef]
- Perry, C.; Klepp, K.-I.; Halper, A.; Dudovitz, B.; Smyth, M.; Golden, D.; Griffin, G. Promoting healthy eating and physical activity patterns among adolescents: A pilot study of ‘Slice of Life’. Health Educ. Res. 1987, 2, 93–103. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Uyeda, K.; Hawes-Dawson, J.; Klein, D.J.; Schuster, M.A. Preliminary Healthy Eating Outcomes of SNaX, a Pilot Community-Based Intervention for Adolescents. J. Adolesc. Health 2011, 48, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, S.; Story, M.; French, S.A.; Fulkerson, J.A.; Nelson, H. Perceptions of adolescents involved in promoting lower-fat foods in schools: Associations with level of involvement. J. Am. Diet. Assoc. 2005, 105, 247–251. [Google Scholar] [CrossRef]
- Lytle, L.A.; Murray, D.; Perry, C.L.; Story, M.; Birnbaum, A.S.; Kubik, M.Y.; Varnell, S. School-Based Approaches to Affect Adolescents’ Diets: Results from the TEENS Study. Health Educ. Behav. 2004, 31, 270–287. [Google Scholar] [CrossRef]
- Story, M.; Lytle, L.A.; Birnbaum, A.S.; Perry, C.L. Peer-led, school-based nutrition education for young adolescents: Feasibility and process evaluation of the TEENS study. J. Sch. Health 2002, 72, 121–127. [Google Scholar] [CrossRef]
- Carlin, A.; Murphy, M.H.; Nevill, A.; Gallagher, A.M. Effects of a peer-led Walking In ScHools intervention (the WISH study) on physical activity levels of adolescent girls: A cluster randomised pilot study. Trials 2018, 19, 31. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Danielli, S.; Coffey, T.; Ashrafian, H.; Darzi, A. Systematic Review into City Interventions to Address Obesity. EClinicalMedicine 2021, 32, 100710. [Google Scholar] [CrossRef] [PubMed]
- Elvsaas, I.K.Ø.; Giske, L.; Fure, B.; Juvet, L.K. Multicomponent Lifestyle Interventions for Treating Overweight and Obesity in Children and Adolescents: A Systematic Review and Meta-Analyses. J. Obes. 2017, 2017, 5021902. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, B.E.; Novotny, R.; Gittelsohn, J. Multi-Level, Multi-Component Approaches to Community Based Interventions for Healthy Living—A Three Case Comparison. Int. J. Environ. Res. Public Health 2016, 13, 1023. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Design | Setting | Participants | Youth Mentors or Peer Mentors | Intervention | Outcomes | Results |
|---|---|---|---|---|---|---|
| B’more Healthy Communities for Kids (BHCK) [34] | ||||||
| Group randomized controlled trial |
|
| Youth Mentors:
|
|
|
|
| Challenge A [29,35] | ||||||
| Randomized control trial |
|
| Youth Mentors:
|
|
|
|
| In-depth interviews |
| n/a | Youth Mentors:
| n/a | Examination of:
|
|
| Cool Girls, Inc. [36] | ||||||
| Quasi-experimental; convenience sample |
|
| Youth Mentors:
|
|
|
|
| Fluids Used Effectively for Living (FUEL) [37] | ||||||
| Quasi-experimental |
|
| Youth Mentors:
|
|
|
|
| Girls Active Project [38,39] | ||||||
| Cluster randomized control |
|
| Peer Mentor:
|
|
|
|
| Go Girls! [40] | ||||||
| Prospective observational |
|
| Youth Mentors:
|
|
|
|
| HealthCorps [41] | ||||||
| Quasi-experimental |
|
| Youth Mentors:
|
|
|
|
| Healthy Buddies A [42] | ||||||
| Quasi-experimental |
|
| Youth Mentors:
|
|
|
|
| Heart Healthy Kids Program (H2K) [43] | ||||||
| Quasi-experimental |
|
| Peer mentors:
|
|
|
|
| Just for Kids! A [44,45] | ||||||
| Randomized control trial |
|
| Youth Mentors:
| After-school program with nutrition education and physical activity |
|
|
| Randomized control trial |
|
| Youth Mentors:
|
|
|
|
| Mentoring to Be Active (MBA) A [46] | ||||||
| Group randomized controlled trial |
|
| Peer Mentor
|
|
|
|
| MOVE Project [47] | ||||||
| Cluster randomized controlled trial |
|
| Youth Mentors:
|
|
|
|
| Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A) [48,49] | ||||||
| Cluster randomized controlled trial |
|
| Peer Mentor n = 53
|
|
|
|
| Process evaluation |
|
|
|
|
|
|
| Peer Education About Weight Steadiness (PAWS) A [50] | ||||||
| Cluster randomized control |
|
| Peer mentors:
|
|
|
|
| Slice of Life [51] | ||||||
| Group randomized controlled trial |
|
| Peer mentors:
|
|
|
|
| Students for Nutrition and eXercise (SNaX) A [52] | ||||||
| Quasi-experimental |
|
| Peer mentors:
|
|
|
|
| Trying Alternative Cafeteria Options in Schools (TACOS) A [15,53] | ||||||
| Group randomized control trial |
|
| Peer mentors:
|
|
|
|
| Two-group post-test |
|
| Peer mentors:
|
|
|
|
| Teens Eating for Energy and Nutrition at School (TEENS) A [16,54,55] | ||||||
| Group randomized control trial; sub-study of the TEENS project |
|
| Peer mentors:
|
|
|
|
| Group randomized control trial |
|
| Peer mentors:
|
|
|
|
| Process evaluation of a group randomized control trial; sub-study of the TEENS project |
| n/a | Peer Mentors:
| n/a |
|
|
| Walking In ScHools (WISH) A [56] | ||||||
| Randomized control trial |
|
| Youth Mentors
|
|
|
|
| Study | Randomization Process | Deviations from Intended Intervention (Intervention Assignment) | Deviations from Intended Intervention (Intervention Adherence) | Missing Outcome Data | Measurement of Outcome | Selection of Reported Results | Overall Risk of Bias Judgement |
|---|---|---|---|---|---|---|---|
| B’more Healthy Communities for Kids (BHCK) [34] | Low Risk | Low Risk | Low Risk | Some Concerns | Some Concerns | Low Risk | Some Concerns |
| Challenge! [29,35] | Low Risk | Some Concerns | Low Risk | Some Concerns | Low Risk | Low Risk | Some Concerns |
| Cool Girls, Inc. [36] | Higk Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | High Risk |
| Fluids Used Effectively for Living (FUEL) [37] | High Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | High Risk |
| Girls Active Project [38,39] | Low Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| Go Girls! [40] | High Risk | Some Concerns | Some Concerns | Low Risk | Some Concerns | Low Risk | High Risk |
| HealthCorps [41] | High Risk | Some Concerns | Some Concerns | High Risk | Low Risk | Low Risk | High Risk |
| Healthy Buddies [42] | High Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | High Risk |
| Heart Healthy Kids Program (H2K) [43] | High Risk | Some Concerns | Some Concerns | Some Concerns | Low Risk | Low Risk | High Risk |
| Just for Kids! [44,45] | Low Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| Mentoring to Be Active (MBA) [46] | Low Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| MOVE Project [47] | Low Risk | Some Concerns | Some Concerns | Some Concerns | Low Risk | Low Risk | Some Concerns |
| Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A) [48,49] | Low Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| Peer Education About Weight Steadiness (PAWS) [50] | Low Risk | Some Concerns | Low Risk | High Risk | Low Risk | Low Risk | High Risk |
| Slice of Life [51] | Some Concerns | Some Concerns | High Risk | Low Risk | Low Risk | Low Risk | High Risk |
| Students for Nutrition and eXercise (SNaX) [52] | High Risk | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | High Risk |
| Trying Alternative Cafeteria Options in Schools (TACOS) [15,53] | Some Concerns | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| Teens Eating for Energy and Nutrition at School (TEENS) [16,54,55] | Some Concerns | Some Concerns | Some Concerns | Low Risk | Low Risk | Low Risk | Some Concerns |
| WISH [56] | Low Risk | Some Concerns | Some Concerns | Low Risk | Some Concerns | Low Risk | Some Concerns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavelle, M.A.; Knopp, M.; Gunther, C.W.; Hopkins, L.C. Youth and Peer Mentor Led Interventions to Improve Biometric-, Nutrition, Physical Activity, and Psychosocial-Related Outcomes in Children and Adolescents: A Systematic Review. Nutrients 2023, 15, 2658. https://doi.org/10.3390/nu15122658
Lavelle MA, Knopp M, Gunther CW, Hopkins LC. Youth and Peer Mentor Led Interventions to Improve Biometric-, Nutrition, Physical Activity, and Psychosocial-Related Outcomes in Children and Adolescents: A Systematic Review. Nutrients. 2023; 15(12):2658. https://doi.org/10.3390/nu15122658
Chicago/Turabian StyleLavelle, Margaret A., Miriam Knopp, Carolyn W. Gunther, and Laura C. Hopkins. 2023. "Youth and Peer Mentor Led Interventions to Improve Biometric-, Nutrition, Physical Activity, and Psychosocial-Related Outcomes in Children and Adolescents: A Systematic Review" Nutrients 15, no. 12: 2658. https://doi.org/10.3390/nu15122658
APA StyleLavelle, M. A., Knopp, M., Gunther, C. W., & Hopkins, L. C. (2023). Youth and Peer Mentor Led Interventions to Improve Biometric-, Nutrition, Physical Activity, and Psychosocial-Related Outcomes in Children and Adolescents: A Systematic Review. Nutrients, 15(12), 2658. https://doi.org/10.3390/nu15122658