
Developing Healthy Lifestyle Behaviors in Early Age—An Intervention Study in Kindergartens


Abstract
1. Introduction
Background and Purpose
- The quality of the children’s mid-morning snack and water consumption.
- Children’s ability to explain how they feel about their bodies following physical exercise.
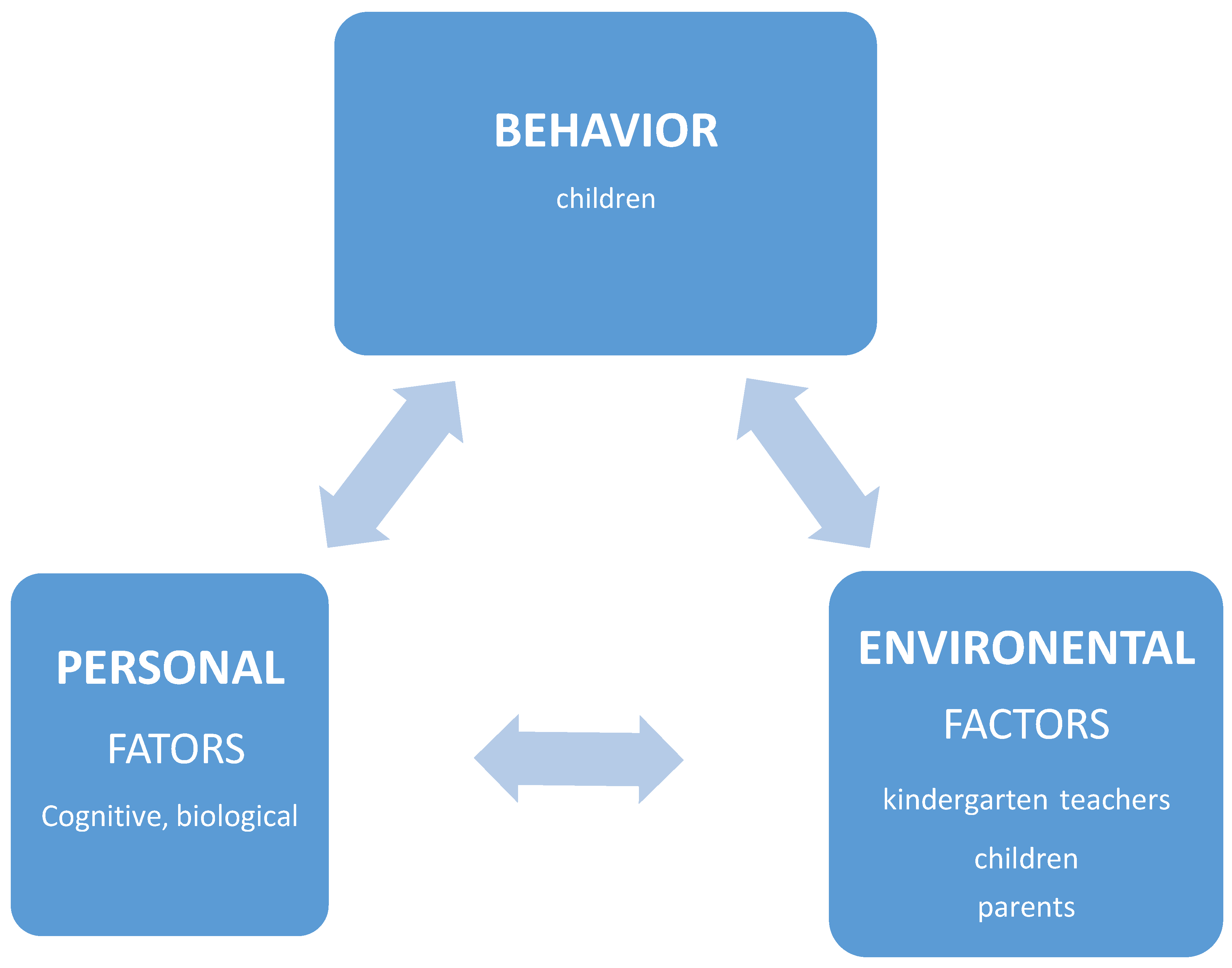
- Indirectly, parent involvement through the children, indicated by changing the quality of the children’s mid-morning snack and water consumption—thus showing that the children were acting as “agents of change”.
2. Materials and Methods
2.1. Setting
2.1.1. For Kindergarten Teachers
- Adopting sensible eating and drinking habits through menu diversification towards the Mediterranean diet pattern, prudent food choices and promoting self-control [34,35]. Emphasis was placed on increasing fruit, vegetable and water consumption and improving the quality of the mid-morning snack brought to school [36,37,38].
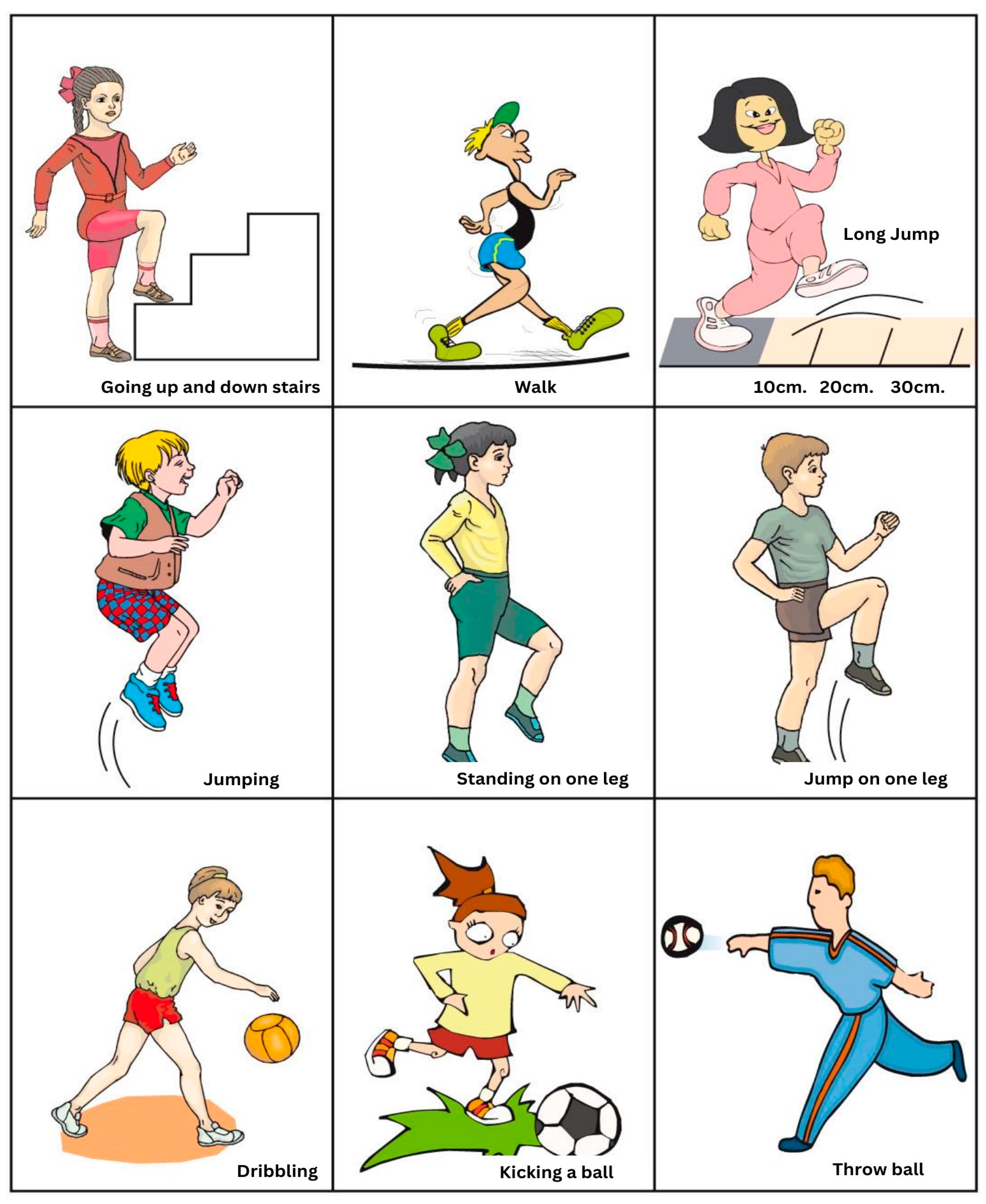
- Encouraging physical exercise in line with the Physical Exercise Curriculum for Kindergartens, encouraging teachers to be active and develop basic motor skills in the children such as walking, running, twisting in different directions, at different speeds, jumping and landing, rolling and balancing the body, shooting at targets, ball control and dribbling [39].
- The use of logical-mathematical language skills related to measurements such as: counting, concepts, quantity, time, speed, strength, representations in diagrams and monitoring charts, classification processes, comparisons, cause-effect relationships, drawing relevant conclusions, reasoning, and problem solving [40,41]. The educational environment illustrated these topics through wall diagrams, charts and computer graphics. Teaching modules encouraged activity in an experiential manner such as: using food groups to build food pyramids, preparing salads, documenting the amount of vegetables, fruits, and water consumed, as well as encouraging more physical exercise by counting and measuring steps.
2.1.2. For Kindergarten Children
2.2. Participants and Assignment of Groups
2.3. Measurements
3. Results
3.1. Data Analysis
3.2. Results
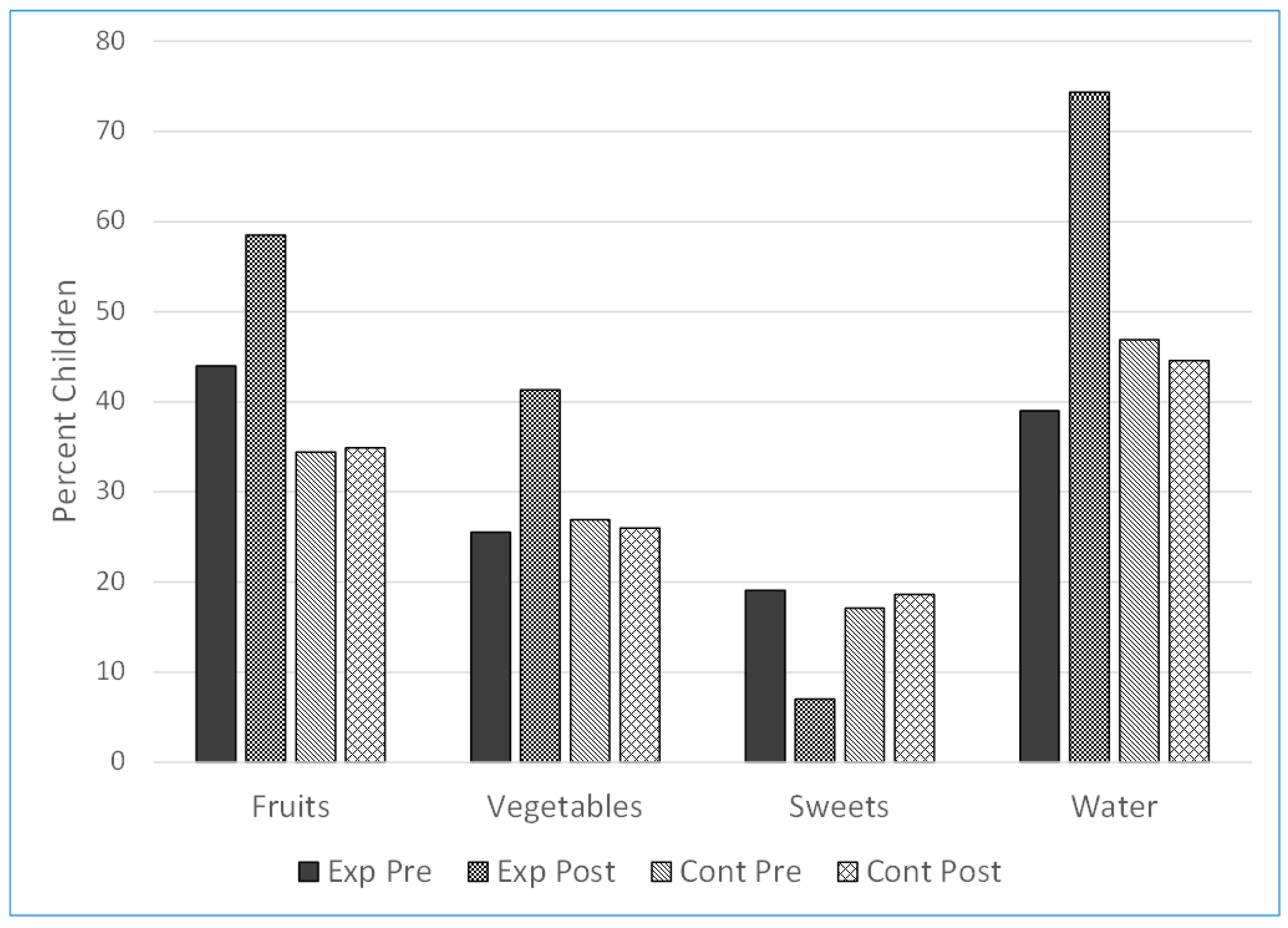
3.2.1. Pupils’ Nutrition Habits (in Accordance with Previous Publication) [46]
3.2.2. Pupils’ Attitudes to Physical Activity
- (1)
- Physical aspects: e.g., heart function, breathing, sweating, thirst, fever, fatigue, difficulty. e.g., easy/not difficult, not tired.
- (2)
- A total of 80% of the children referred to the physical aspect (e.g., cardiac activity, perspiration, breathing, heat, fatigue) such as “My heart is beating a lot’’, “My body got hot”, “I felt tiredness in my heart”.Emotional aspects: e.g., positive—fun, competence, motivation; negative—not like (do not want/not good/annoying), difficult to manage.A total of 47% of the children expressed themselves in emotional terms. Most of them voiced enjoyment, fun and capability such as: “I can do more”.
- (3)
- Cognitive aspects: the use of language and concepts of mathematical logic (argument, reason, result), the use of images. A total of 47% of the children made cognitive references that included the use of mathematical-logical concepts and images such as “many times it was hard to go up and go down” or “my heart beats twice as fast”, sound arguments such as “I had fun because I jumped a lot” and cause–effect relationships such as “if I jump, then my feet hurt”.
- (4)
- Energy expenditure’ aspects: The responses were classified as follows: 1. Description—a non-scientific explanation, such as “I had a lot of fun”; 2. Scientific description—such as: “my heart is beating strongly:, “I felt heavy breathing”, “It was hard and I was sweating ‘‘, “My blood was flowing fast”, “My body becomes warm”; 3. Scientific description with additional information on enjoyment from the activity—such as: “my heart beats quickly and I want more”, “my body heats up and it was fun”, “I also enjoyed it and I was thirsty”, “I ran and jumped easily, but I’m really sweating”.
4. Discussion
- Principles of the Intervention Program—Nutrition
- Physical Activity
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 2012, 307, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Patterson, C.M.; Oldenburg, B. Implications of diet and nutrition for growth and prevalence of anaemia in rural preschool-aged children in Shandong Province, China. Asia Pac. J. Clin. Nutr. 2000, 9, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Janicke, D.M.; Mitchell, T.B.; Basch, M.C.; Ding, K.; Jones, L.C.; Pinto, S.; Moorman, E.L.; Reynolds, C.M.; Gonzalez-Louis, R.C.; Wolock, E.R.; et al. Meta-analysis of lifestyle modification interventions addressing overweight and obesity in preschool-age children. Health Psychol. 2021, 40, 631–641. [Google Scholar] [CrossRef] [PubMed]
- De Bock, F.; Breitenstein, L.; Fischer, J.E. Positive impact of a pre-school-based nutritional intervention on children’s fruit and vegetable intake: Results of a cluster-randomized trial. Public Health Nutr. 2012, 15, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Konda, S.; Giri, P.; Otiv, A. Prevention of overweight and obesity in preschool children: An updated review. Int. J. Res. Med. Sci. 2014, 2, 1. [Google Scholar] [CrossRef]
- Canoy, D.; Yang, T.O. Obesity in children: Bariatric surgery. Clin. Evid. 2015, 2015, 0325. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Obesity prevalence among low-income, preschool-aged children—United States, 1998–2008. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 769–773. [Google Scholar]
- Piaget, J. The Development of Thought: Equilibration of Cognitive Structures; Rosin, A., Translator; Viking Press: New York, NY, USA, 1977. [Google Scholar]
- Vlaev, I.; Taylor, M.J.; Taylor, D.; Gately, P.; Gunn, L.H.; Abeles, A.; Kerkadi, A.; Lothian, J.; Jreige, S.K.; Alsaadi, A.; et al. Testing a multicomponent lifestyle intervention for combatting childhood obesity. BMC Public Health 2021, 21, 824. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Rawal, T.; van Schayck, O.C.P.; Willeboordse, M.; Arora, M.; Bhaumik, S.; Bhagra, A.; Bhagra, S.; Muris, J.W.M.; Tandon, N. How to promote a healthy lifestyle among schoolchildren: Development of an intervention module (i-PROMISe). Public Health Pract. 2022, 3, 100262. [Google Scholar] [CrossRef]
- Koletzko, B.; Fishbein, M.; Lee, W.S.; Moreno, L.; Mouane, N.; Mouzaki, M.; Verduci, E. Prevention of childhood obesity: A position paper of the global federation of international societies of paediatric gastroenterology, hepatology and nutrition (FISPGHAN). J. Pediatr. Gastroenterol. Nutr. 2020, 70, 702–710. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsec, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 166. [Google Scholar] [CrossRef]
- Nash, R.; Patterson, K.; Flittner, A.; Elmer, S.; Osborne, R. School-Based Health Literacy Programs for Children (2-16 Years): An International Review. J. Sch. Health 2021, 91, 632–649. [Google Scholar] [CrossRef]
- Gelman, R.; Tucker, M.F. Further investigations of the young child’s conception of number. Child Dev. 1975, 46, 167. [Google Scholar] [CrossRef]
- Vygotsky, L. Mind in Society: Development of Higher Psychological Processes; Vygotsky, L.S., Cole, M., Jolm-Steiner, V., Scribner, S., Souberman, E., Eds.; Harvard University Press: Cambridge, MA, USA, 1978. [Google Scholar]
- Klein, P.S.; Yablon, Y.B. From Research to Practice in Early Childhood Education; Convened by the Initiative of Research for Educational Practice; The Israel Academy of Sciences and Humanities: Jerusalem, Israel; The Ministry of Education and Yad HaNadiv: Jerusalem, Israel, 2008. (In Hebrew) [Google Scholar]
- Kamii, C.; Rummelsburg, J.; Kari, A. Teaching arithmetic to low-performing, low-SES first graders. J. Math. Behav. 2005, 24, 39–50. [Google Scholar] [CrossRef]
- Diamond, C.; Saintonge, S.; August, P.; Azrack, A. The development of building wellnessTM, a youth health literacy program. J Health Commun. 2011, 16 (Suppl. S3), 103–118. [Google Scholar] [CrossRef]
- Kolo, C.; Masur, U.; Emre, M.; Kreulich, K. Higher Education 2030: From Future Skills in Higher Education to the Future Skills of Higher Education Managers; Hochschule Macromedia: Berlin, Germany, 2021. [Google Scholar]
- Nash, R.; Cruickshank, V.; Pill, S.; MacDonald, A.; Coleman, C.; Elmer, S. HealthLit4Kids: Dilemmas associated with student health literacy development in the primary school setting. Health Educ. J. 2021, 80, 173–186. [Google Scholar] [CrossRef]
- Mouratidou, T.; Miguel, M.L.; Androutsos, O.; Manios, Y.; De Bourdeaudhuij, I.; Cardon, G.; Kulaga, Z.; Socha, P.; Galcheva, V.; Iotova, V.; et al. Tools, harmonization and standardization procedures of the impact and outcome evaluation indices obtained during a kindergarten-based, family-involved intervention to prevent obesity in early childhood: The ToyBox-study. Obes Rev. 2014, 15 (Suppl. S3), 53–60. [Google Scholar] [CrossRef]
- Kobel, S.; Henle, L.; Laemmle, C.; Wartha, O.; Szagun, B.; Steinacker, J.M. Intervention Effects of a Kindergarten-Based Health Promotion Programme on Motor Abilities in Early Childhood. Front. Public Health 2020, 8, 219. [Google Scholar] [CrossRef]
- Lindsay, A.R.; Starrett, A.; Brian, A.; Byington, T.A.; Lucas, J.; Sigman-Grant, M. Preschoolers build fundamental motor skills critical to an active lifestyle: The all 4 kids© intervention study. Int. J. Environ. Res. Public Health 2020, 17, 3098. [Google Scholar] [CrossRef] [PubMed]
- Meshkovska, B.; Scheller, D.A.; Wendt, J.; Jilani, H.; Scheidmeir, M.; Stratil, J.M.; Nanna Lien on behalf of the PEN Consortium. Barriers and facilitators to implementation of direct fruit and vegetables provision interventions in kindergartens and schools: A qualitative systematic review applying the consolidated framework for implementation research (CFIR). Int. J. Behav. Nutr. Phys. Act. 2022, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Maccoby, E.E. Social Development: Psychological Growth and the Parent-Child Relationship; Harcourt Brace Jovanovich: New York, NY, USA, 1980. [Google Scholar]
- Mikkelsen, M.V.; Husby, S.; Skov, L.R.; Perez-Cueto, F.J.A. A systematic review of types of healthy eating interventions in preschools. Nutr. J. 2014, 13, 56. [Google Scholar] [CrossRef] [PubMed]
- Janicke, D.M.; Steele, R.G.; Gayes, L.A.; Lim, C.S.; Clifford, L.M.; Schneider, E.M.; Carmody, J.K.; Westen, S. Systematic review and meta-analysis of comprehensive behavioral family lifestyle interventions addressing pediatric obesity. J. Pediatr. Psychol. 2014, 39, 809–825. [Google Scholar] [CrossRef] [PubMed]
- Flinchum, B.M. Early childhood movement programs. J. Phys. Educ. Recreat. Dance 1988, 59, 62–64. [Google Scholar] [CrossRef]
- Hendy, H.M.; Raudenbush, B. Effectiveness of teacher modeling to encourage food acceptance in preschool children. Appetite 2000, 34, 61–76. [Google Scholar] [CrossRef]
- Fisher, A.; Reilly, J.J.; Kelly, L.A.; Montgomery, C.; Williamson, A.; Paton, J.Y.; Grant, S.T.A.N. Fundamental movement skills and habitual physical activity in young children. Med. Sci. Sports Exerc. 2005, 37, 684–688. [Google Scholar] [CrossRef]
- Manios, Y.; Grammatikaki, E.; Androutsos, O.; Chinapaw, M.J.M.; Gibson, E.L.; Buijs, G.; Iotova, V.; Socha, P.; Annemans, L.; Wildgruber, A.; et al. A systematic approach for the development of a kindergarten-based intervention for the prevention of obesity in preschool age children: The ToyBox-study. Obes. Rev. 2012, 13 (Suppl. S1), 3–12. [Google Scholar] [CrossRef]
- Fox, M.K.; Condon, E.; Briefel, R.R.; Reidy, K.C.; Deming, D.M. Food consumption patterns of young preschoolers: Are they starting off on the right path? J. Am. Diet. Assoc. 2010, 110, S52–S59. [Google Scholar] [CrossRef]
- Siega-Riz, A.M.; Deming, D.M.; Reidy, K.C.; Fox, M.K.; Condon, E.; Briefel, R.R. Food consumption patterns of infants and toddlers: Where are we now? J. Am. Diet. Assoc. 2010, 110, S38–S51. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Heimendinger, J.; Patterson, B.H.; Subar, A.F.; Kessler, R.; Pivonka, E. Psychosocial factors associated with fruit and vegetable consumption. Am. J. Health Promot. 1995, 10, 98–104. [Google Scholar] [CrossRef]
- Lowe, C.F.; Horne, P.J.; Tapper, K.; Bowdery, M.; Egerton, C. Effects of a peer modelling and rewards-based intervention to increase fruit and vegetable consumption in children. Eur. J. Clin. Nutr. 2004, 58, 510–522. [Google Scholar] [CrossRef]
- Spill, M.K.; Birch, L.L.; Roe, L.S.; Rolls, B.J. Eating vegetables first: The use of portion size to increase vegetable intake in preschool children. Am. J. Clin. Nutr. 2010, 91, 1237–1243. [Google Scholar] [CrossRef]
- Ministry of Education, Department of Planning and Curriculum Development. The Physical Education Curriculum for Kindergarten in State and State-Religious Education. Jerusalem. 2007. Available online: https://meyda.education.gov.il/files/PreSchool/Gan001148new.pdf (accessed on 11 January 2023).
- Gelman, R.; Gallistel, C.R. The Child’s Understanding of Number; Harvard University: Cambridge, MA, USA, 1978. [Google Scholar]
- Swartz, R.J.; Parks, S. Infusing the Teaching of Critical and Creative Thinking into Content Instruction: A Lesson Design Handbook for the Elementary Grades; Critical Thinking Press & Software: Pacific Grove, CA, USA, 1994. [Google Scholar]
- Cook, A.; Friday, J.E. Pyramid Servings Intakes in the United States 1999–2002, 1 Day; US Department of Agriculture: Washington DC, USA; Agricultural Research Service: Washington DC, USA; Community Nutrition Research Group: Washington DC, USA, 2005; Volume 3.
- O’Connor, T.M.; Yang, S.-J.; Nicklas, T.A. Beverage intake among preschool children and its effect on weight status. Pediatrics 2006, 118, e1010-8. [Google Scholar]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13 y in the United States: Analyses of 2005–2010 NHANES data. Nutr. J. 2013, 12, 85. [Google Scholar] [CrossRef]
- Zucker, D.M.; Lakatos, E.; Webber, L.S.; Murray, D.M.; McKinlay, S.M.; Feldman, H.A.; Kelder, S.H.; Nader, P.R. Statistical design of the Child and Adolescent Trial for Cardiovascular Health (CATCH): Implications of cluster randomization. Control Clin. Trials 1995, 16, 96–118. [Google Scholar] [CrossRef]
- Jakobovich, R.; Shoval, E.; Berry, E.M.; Shulruf, B. Supporting children to act as change agents for parents in preparing their lunch box. AJEC 2019, 44, 153–165. [Google Scholar] [CrossRef]
- Nixon, C.A.; Moore, H.J.; Douthwaite, W.; Gibson, E.L.; Vogele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Summerbell, C.D. Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: A systematic review. Obes. Rev. 2012, 13 (Suppl. S10), 106–117. [Google Scholar] [CrossRef]
- Hardy, L.L.; King, L.; Kelly, B.; Farrell, L.; Howlett, S. Munch and Move: Evaluation of a preschool healthy eating and movement skill program. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 80. [Google Scholar] [CrossRef]
- Schlam, T.R.; Wilson, N.L.; Shoda, Y.; Mischel, W.; Ayduk, O. Preschoolers’ delay of gratification predicts their body mass 30 years later. J. Pediatr. 2013, 162, 90–93. [Google Scholar] [CrossRef]
- Nemet, D.; Geva, D.; Pantanowitz, M.; Igbaria, N.; Meckel, Y.; Eliakim, A. Long term effects of a health promotion intervention in low socioeconomic Arab- Israeli kindergartens. BMC Pediatr. 2013, 13, 45. [Google Scholar] [CrossRef]
- Matvienko, O. Impact of a nutrition education curriculum on snack choices of children ages six and seven years. J. Nutr. Educ. Behav. 2007, 39, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Díaz, E.N.; Le, Q.; Campos, D.; Reyes, J.M.; Wright, J.A.; Greaney, M.L.; Lindsay, A.C. Central American Parents’ Preferences for Content and Modality for a Family-Centered Intervention to Promote Healthful Energy Balance-Related Behaviors of Their Preschool-Age Children. Int. J. Environ. Res. Public Health 2022, 19, 5080. [Google Scholar] [CrossRef] [PubMed]
- Nordlund, S.; McPhee, P.G.; Gabarin, R.; Deacon, C.; Mbuagbaw, L.; Morrison, K.M. Effect of obesity treatment interventions in preschool children aged 2–6 years: A systematic review and meta-analysis. BMJ Open 2022, 12, e053523. [Google Scholar] [CrossRef] [PubMed]
- Kieslinger, K.; Wartha, O.; Pollatos, O.; Steinacker, J.M.; Kobel, S. Parental Self-Efficacy-A Predictor of Children’s Health Behaviors? Its Impact on Children’s Physical Activity and Screen Media Use and Potential Interaction Effect Within a Health Promotion Program. Front. Psychol. 2021, 12, 712796. [Google Scholar] [CrossRef]
- Patrick, H.; Nicklas, T.A. A Review of Family and Social Determinants of Children’s Eating Patterns and Diet Quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef]
- Cools, W.; De Martelaer, K.; Samaey, C.; Andries, C. Fundamental movement skill performance of preschool children in relation to family context. J. Sports Sci. 2011, 29, 649–660. [Google Scholar] [CrossRef]
- Lerner-Geva, L.; Bar-Zvi, E.; Levitan, G.; Boyko, V.; Reichman, B.; Pinhas-Hamiel, O. An intervention for improving the lifestyle habits of kindergarten children in Israel: A cluster-randomised controlled trial investigation. Public Health Nutr. 2015, 18, 1537–1544. [Google Scholar] [CrossRef]
- Herbert, B.; Strauß, A.; Mayer, A.; Duvinage, K.; Mitschek, C.; Koletzko, B. Implementation process and acceptance of a setting based prevention programme to promote healthy lifestyle in preschool children. Health Educ. J. 2013, 72, 363–372. [Google Scholar] [CrossRef]
- Dernini, S.; Berry, E.M. Mediterranean diet: From a healthy diet to a sustainable dietary pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef]
- Logan, S.W.; Scrabis-Fletcher, K.; Modlesky, C.; Getchell, N. The relationship between motor skill proficiency and body mass index in preschool children. Res. Q. Exerc. Sport 2011, 82, 442–448. [Google Scholar] [CrossRef]
- Council on Sports Medicine and Fitness, Council on School Health. Active healthy living: Prevention of childhood obesity through increased physical activity. Pediatrics 2006, 117, 1834–1842. [Google Scholar] [CrossRef]
- Welk, G.J.; Jackson, A.W.; Morrow, J.R.; Haskell, W.H.; Meredith, M.D.; Cooper, K.H. The association of health-related fitness with indicators of academic performance in Texas schools. Res. Q. Exerc. Sport 2010, 81, S16–S23. [Google Scholar] [CrossRef]
- Nubani-Husseini, M.; Berry, E.M.; Abdeen, Z.; Donchin, M. Dietary patterns and physical activity among Palestinian female schoolchildren in East Jerusalem. South East. Eur. J. Public Health (SEEJPH) 2016, 5. [Google Scholar] [CrossRef]
- Bröder, J.; Okan, O.; Bauer, U.; Schlupp, S.; Pinheiro, P. Advancing perspectives on health literacy in childhood and youth. Health Promot. Int. 2020, 35, 575–585. [Google Scholar] [CrossRef]
- Auld, M.E.; Allen, M.P.; Hampton, C.; Montes, J.H.; Sherry, C.; Mickalide, A.D.; Logan, R.A.; Alvarado-Little, W.; Parson, K. Health literacy and health education in schools: Collaboration for action. NAM Perspect. 2020. [Google Scholar] [CrossRef]
- Levin-Zamir, D.; Lemish, D.; Gofin, R. Media Health Literacy (MHL): Development and measurement of the concept among adolescents. Health Educ. Res. 2011, 26, 323–335. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Characteristics of an Effective Health Education Curriculum. 2013. Available online: CDC.gov (accessed on 23 March 2023).




{kind=link}
{kind=link}
{kind=link}
| Theme | Topics |
|---|---|
| Health Education and Promotion |
|
| Nutrition |
|
| Physical Activity |
|
| Imparting skills for logical and mathematical thinking |
|
| Kindergartens | Intervention Group (42) | Comparison Group (32) | |||
|---|---|---|---|---|---|
| Percent (SD) | Percent (SD) | ||||
| Number of Children | 842 | 1048 | |||
| Boys | 55.7 | NS * | 56.3 | 454 | 436 |
| Girls | 44.3 | NS | 43.7 | 352 | 347 |
| Number of children in class | (6.2) | NS | (7.5) | 26.3 | 25.0 |
| Experience of the teachers (year) | (9.2) | NS | (9.7) | 14.0 | 14.5 |
| Sector of Kindergarten | |||||
| National—Secular | 47.6 | 75.0 | 24 | 20 | |
| National—Religious | 52.4 | 25.0 | 8 | 22 | |
| Socio-Economic Status of school population | |||||
| Low—Low-Middle | 47.6 | 56.3 | 18 | 20 | |
| High-middle—High | 52.4 | 43.8 | 14 | 22 | |
| Intervention Group | Comparison Group | |||||
|---|---|---|---|---|---|---|
| Sandwich Content | Difference in % | post N = 653 | pre N = 740 | Difference in % | post N = 730 | pre N = 734 |
| Change% | N (%) | N (%) | Change % | N (%) | N (%) | |
| Cheese | +6.1 ** | 273 * (41.8) | 264 (35.7) | +0.5 | 221 (30.3) | 219 (29.8) |
| Chocolate Spread | −12.0 *** | 64 ** (9.8) | 161 (21.8) | +0.2 | (5.1) | (4.9) |
| Humus | +3.6 ** | 102 * (15.6) | 89 (12.0) | +2.0 | 87 (11.9) | 73 (9.9) |
| Egg | +0.5 | 53 (8.1) | 56 (7.6) | +0.8 | 58 (7.9) | 52 (7.1) |
| Salami | +1.4 | 37 (5.7) | 32 (4.3) | −1.9 | 51 (7.0) | 65 (8.9) |
| Tuna | +2.7 ** | 47 * (7.2) | 33 (4.5) | −1.2 | 36 (4.9) | 45 (6.1) |
| Intervention Group | Comparison Group | |||||
|---|---|---|---|---|---|---|
| Difference % | post N = 648 | pre N = 728 | Difference% | post N = 719 | pre N = 722 | |
| N (%) | N (%) | N (%) | N (%) | |||
| Bread only—no filling | +0.7 | 31 (4.8) | 30 (4.1) | +0.7 | 35 (4.9) | 30 (4.2) |
| Preferred (healthy) content | +14.1 *** | 517 (79.8) | 478 (65.7) | +0.4 | 460 (63.9) | 459 (63.5) |
| Sweet spreads | −14.8 *** | 100 (15.4) | 220 (30.2) | −1.1 | 224 (31.2) | 233 (32.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakobovich, R.; Berry, E.M.; Levita, A.; Levin-Zamir, D. Developing Healthy Lifestyle Behaviors in Early Age—An Intervention Study in Kindergartens. Nutrients 2023, 15, 2615. https://doi.org/10.3390/nu15112615
Jakobovich R, Berry EM, Levita A, Levin-Zamir D. Developing Healthy Lifestyle Behaviors in Early Age—An Intervention Study in Kindergartens. Nutrients. 2023; 15(11):2615. https://doi.org/10.3390/nu15112615
Chicago/Turabian StyleJakobovich, Ronit, Elliot M. Berry, Asia Levita, and Diane Levin-Zamir. 2023. "Developing Healthy Lifestyle Behaviors in Early Age—An Intervention Study in Kindergartens" Nutrients 15, no. 11: 2615. https://doi.org/10.3390/nu15112615
APA StyleJakobovich, R., Berry, E. M., Levita, A., & Levin-Zamir, D. (2023). Developing Healthy Lifestyle Behaviors in Early Age—An Intervention Study in Kindergartens. Nutrients, 15(11), 2615. https://doi.org/10.3390/nu15112615