
Energy Drinks and Adverse Health Events in Children and Adolescents: A Literature Review

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
3. Results
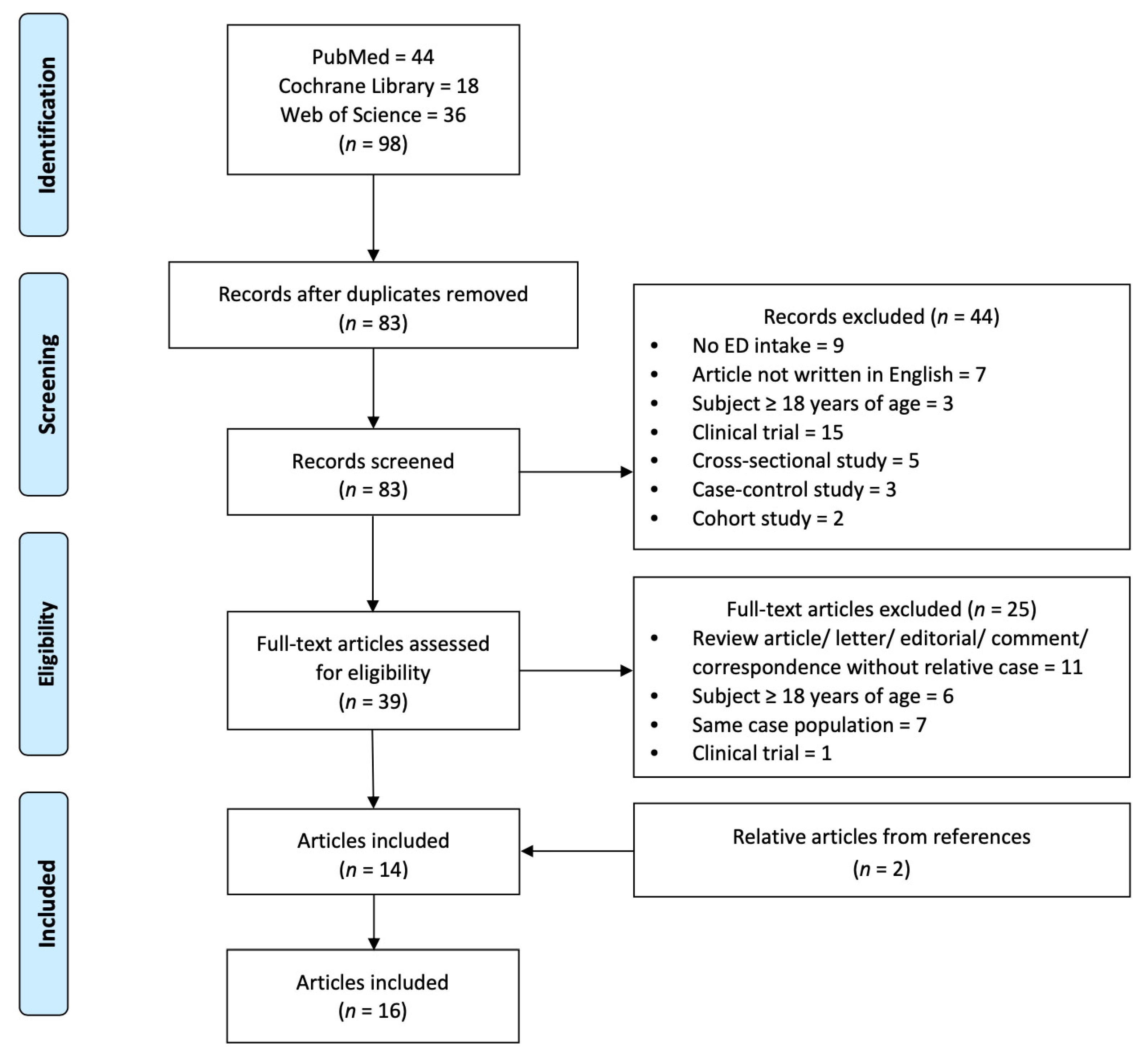
3.1. Record Selection
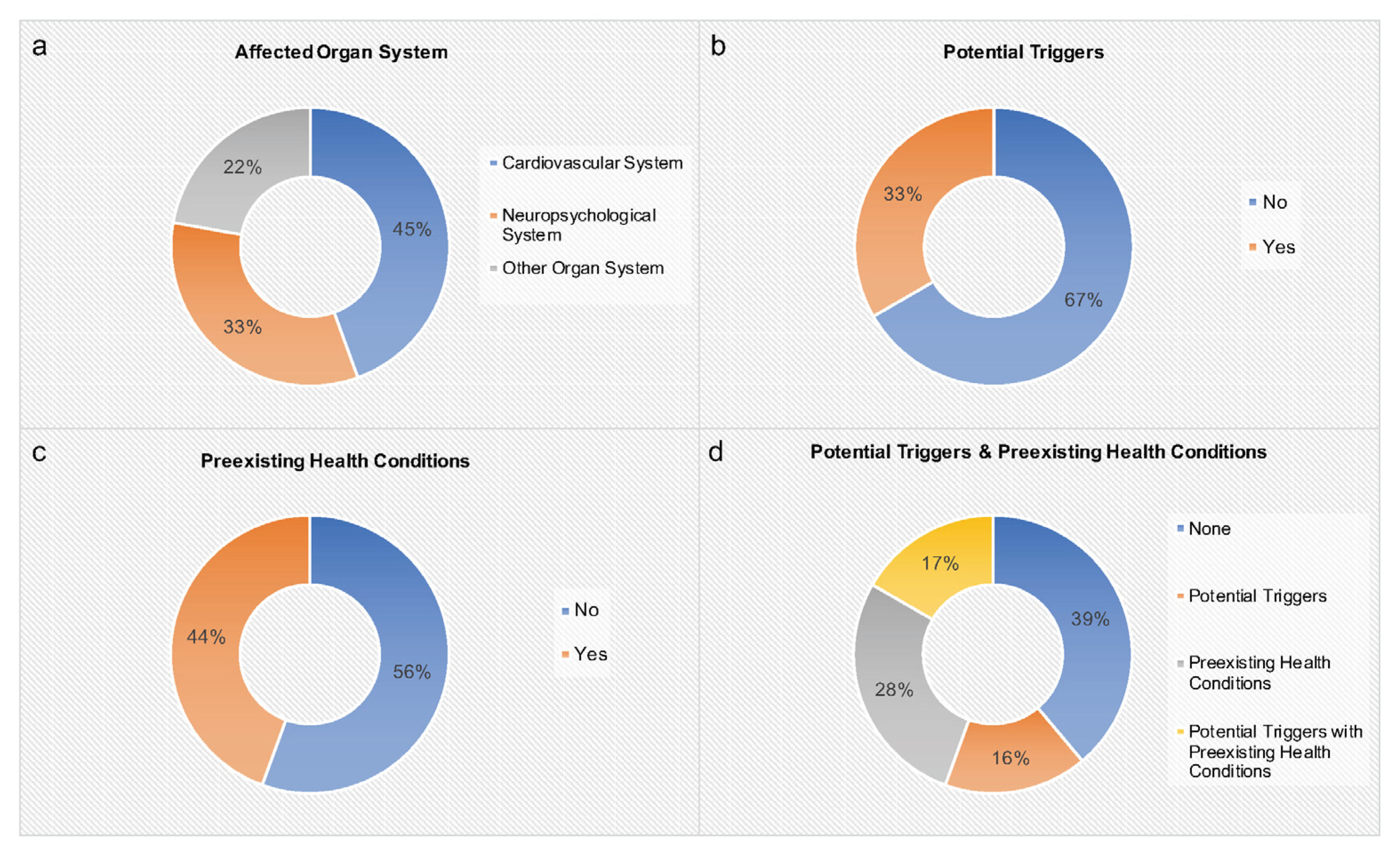
3.2. Summary of Included Cases
4. Discussion
4.1. Effects of Enery Drinks on the Pediatric Cardiovascular System
4.2. Effects of Energy Drinks on the Pediatric Neuropsychiatric System
4.3. Effects of Energy Drinks on Other Pediatric Organ Systems
4.3.1. Hepatic System
4.3.2. Renal System
4.3.3. Skin
4.4. Prevention of Adverse Health Events Associated with Energy Drink Consumption
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hampton, T. Energy Drinks Pose Worrisome Risks to Adolescents’ Cardiovascular Health. Circulation 2016, 134, 1052–1053. [Google Scholar] [CrossRef] [PubMed]
- Sankararaman, S.; Syed, W.; Medici, V.; Sferra, T.J. Impact of Energy Drinks on Health and Well-being. Curr. Nutr. Rep. 2018, 7, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Hellín, J.; Varillas-Delgado, D. Energy Drinks and Sports Performance, Cardiovascular Risk, and Genetic Associations; Future Prospects. Nutrients 2021, 13, 715. [Google Scholar] [CrossRef]
- Grasser, E.K.; Miles-Chan, J.L.; Charrière, N.; Loonam, C.R.; Dulloo, A.G.; Montani, J.-P. Energy Drinks and Their Impact on the Cardiovascular System: Potential Mechanisms. Adv. Nutr. 2016, 7, 950–960. [Google Scholar] [CrossRef]
- Zucconi, S.; Volpato, C.; Adinolfi, F.; Gandini, E.; Gentile, E.; Loi, A.; Fioriti, L. Gathering consumption data on specific consumer groups of energy drinks. EFSA Support. Publ. 2013, 10, 394E. [Google Scholar] [CrossRef]
- Mattson, M.E. Update on Emergency Department Visits Involving Energy Drinks: A Continuing Public Health Concern. In The CBHSQ Report; Substance Abuse and Mental Health Services Administration (US): Rockville, MD, USA, 2013; pp. 1–7. [Google Scholar]
- Seifert, S.M.; Seifert, S.A.; Schaechter, J.L.; Bronstein, A.C.; Benson, B.E.; Hershorin, E.R.; Arheart, K.L.; Franco, V.I.; Lipshultz, S.E. An analysis of energy-drink toxicity in the National Poison Data System. Clin. Toxicol. 2013, 51, 566–574. [Google Scholar] [CrossRef]
- Ehlers, A.; Marakis, G.; Lampen, A.; Hirsch-Ernst, K.I. Risk assessment of energy drinks with focus on cardiovascular parameters and energy drink consumption in Europe. Food Chem. Toxicol. 2019, 130, 109–121. [Google Scholar] [CrossRef]
- Shah, S.A.; Szeto, A.; Farewell, R.; Shek, A.; Fan, D.; Quach, K.N.; Bhattacharyya, M.; Elmiari, J.; Chan, W.; O’Dell, K.; et al. Impact of High Volume Energy Drink Consumption on Electrocardiographic and Blood Pressure Parameters: A Randomized Trial. J. Am. Heart Assoc. 2019, 8, e011318. [Google Scholar] [CrossRef]
- Basrai, M.; Schweinlin, A.; Menzel, J.; Mielke, H.; Weikert, C.; Dusemund, B.; Putze, K.; Watzl, B.; Lampen, A.; Bischoff, S.C. Energy Drinks Induce Acute Cardiovascular and Metabolic Changes Pointing to Potential Risks for Young Adults: A Randomized Controlled Trial. J. Nutr. 2019, 149, 441–450. [Google Scholar] [CrossRef]
- Shah, S.A.; Chu, B.W.; Lacey, C.S.; Riddock, I.C.; Lee, M.; Dargush, A.E. Impact of Acute Energy Drink Consumption on Blood Pressure Parameters: A Meta-analysis. Ann. Pharmacother. 2016, 50, 808–815. [Google Scholar] [CrossRef]
- Oberhoffer, F.S.; Li, P.; Jakob, A.; Dalla-Pozza, R.; Haas, N.A.; Mandilaras, G. Energy Drinks: Effects on Blood Pressure and Heart Rate in Children and Teenagers. A Randomized Trial. Front. Cardiovasc. Med. 2022, 9, 862041. [Google Scholar] [CrossRef] [PubMed]
- Oberhoffer, F.S.; Dalla-Pozza, R.; Jakob, A.; Haas, N.A.; Mandilaras, G.; Li, P. Energy drinks: Effects on pediatric 24-h ambulatory blood pressure monitoring. A randomized trial. Pediatr Res. 2023. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Mandilaras, G.; Jakob, A.; Dalla-Pozza, R.; Haas, N.A.; Oberhoffer, F.S. Energy Drinks and Their Acute Effects on Arterial Stiffness in Healthy Children and Teenagers: A Randomized Trial. J. Clin. Med. 2022, 11, 2087. [Google Scholar] [CrossRef] [PubMed]
- Oberhoffer, F.S.; Li, P.; Jakob, A.; Dalla-Pozza, R.; Haas, N.A.; Mandilaras, G. Energy Drinks Decrease Left Ventricular Efficiency in Healthy Children and Teenagers: A Randomized Trial. Sensors 2022, 22, 7209. [Google Scholar] [CrossRef]
- Mandilaras, G.; Li, P.; Dalla-Pozza, R.; Haas, N.A.; Oberhoffer, F.S. Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial. Cells 2022, 11, 498. [Google Scholar] [CrossRef]
- Polat, N.; Ardıç, I.; Akkoyun, M.; Vuruşkan, E. Spontaneous coronary artery dissection in a healthy adolescent following consumption of caffeinated “energy drinks”. Turk. Kardiyol. Dern Ars. 2013, 41, 738–742. [Google Scholar] [CrossRef]
- Dufendach, K.A.; Horner, J.M.; Cannon, B.C.; Ackerman, M.J. Congenital type 1 long QT syndrome unmasked by a highly caffeinated energy drink. Heart Rhythm 2012, 9, 285–288. [Google Scholar] [CrossRef]
- Di Rocco, J.R.; During, A.; Morelli, P.J.; Heyden, M.; Biancaniello, T.A. Atrial fibrillation in healthy adolescents after highly caffeinated beverage consumption: Two case reports. J. Med. Case Rep. 2011, 5, 18. [Google Scholar] [CrossRef]
- Usman, A.; Jawaid, A. Hypertension in a young boy: An energy drink effect. BMC Res. Notes 2012, 5, 591. [Google Scholar] [CrossRef]
- Terlizzi, R.; Rocchi, C.; Serra, M.; Solieri, L.; Cortelli, P. Reversible postural tachycardia syndrome due to inadvertent overuse of Red Bull. Clin. Auton. Res. 2008, 18, 221–223. [Google Scholar] [CrossRef]
- Wilson, R.E.; Kado, H.S.; Samson, R.; Miller, A.B. A case of caffeine-induced coronary artery vasospasm of a 17-year-old male. Cardiovasc. Toxicol. 2012, 12, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Butragueño Laiseca, L.; Toledo del Castillo, B.; Miranda Herrero, M.C. Energy drinks as a trigger factor for seizures in paediatric patients: A case report. Neurología 2019, 34, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Staikoglou, N.; Polanagnostaki, A.; Lamprou, V.; Chartampilas, E.; Pavlou, E.; Tegos, T.; Finitsis, S. Posterior cerebral artery dissection after excessive caffeine consumption in a teenager. Radiol. Case Rep. 2022, 17, 2081–2084. [Google Scholar] [CrossRef]
- Babu, K.M.; Zuckerman, M.D.; Cherkes, J.K.; Hack, J.B. First-Onset Seizure After Use of an Energy Drink. Pediatr. Emerg. Care 2011, 27, 539–540. [Google Scholar] [CrossRef]
- Yamada-Takeda, M.; Patel, A.; Fenton, G. Energy Drink-Induced Breakthrough Seizure in a Patient on Valproic Acid-Considering Herbal Safety in Epilepsy. J. Pharm. Pract. 2019, 32, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Samanta, D. Reversible cerebral vasoconstriction syndrome: Another health hazard of energy drinks? Clin. Pediatr. 2015, 54, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Quadri, S.; Harding, L.; Lillig, M. An Energy Drink-Induced Manic Episode in an Adolescent. Prim. Care Companion CNS Disord. 2018, 20, 18102318. [Google Scholar] [CrossRef]
- Apestegui, C.A.; Julliard, O.; Ciccarelli, O.; Duc, D.K.; Lerut, J. Energy drinks: Another red flag for the liver allograft. Liver Transpl. 2011, 17, 1117–1118. [Google Scholar] [CrossRef]
- Robin, S.; Buchanan, R.; Poole, R. Energy drinks and adolescents—A hepatic health hazard? J. Hepatol. 2018, 68, 856–857. [Google Scholar] [CrossRef]
- Schöffl, I.; Kothmann, J.F.; Schöffl, V.; Rupprecht, H.D.; Rupprecht, T. “Vodka energy”: Too much for the adolescent nephron? Pediatrics 2011, 128, e227–e231. [Google Scholar] [CrossRef]
- Yazdi, A.S.; Mayser, P.; Sander, C.A. Lichen aureus with clonal T cells in a child possibly induced by regular consumption of an energy drink. J. Cutan. Pathol. 2008, 35, 960–962. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Tuttle, T.D.; Higgins, C.L. Energy beverages: Content and safety. Mayo Clin. Proc. 2010, 85, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Frankel, D.S. Arrhythmogenic effects of energy drinks. J. Cardiovasc. Electrophysiol. 2017, 28, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, E.A.; Lacey, C.S.; Aaron, M.; Kolasa, M.; Occiano, A.; Shah, S.A. Randomized Controlled Trial of High-Volume Energy Drink Versus Caffeine Consumption on ECG and Hemodynamic Parameters. J. Am. Heart Assoc. 2017, 6, e004448. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Occiano, A.; Nguyen, T.A.; Chan, A.; Sky, J.C.; Bhattacharyya, M.; O’Dell, K.M.; Shek, A.; Nguyen, N.N. Electrocardiographic and blood pressure effects of energy drinks and Panax ginseng in healthy volunteers: A randomized clinical trial. Int. J. Cardiol. 2016, 218, 318–323. [Google Scholar] [CrossRef]
- Kozik, T.M.; Shah, S.; Bhattacharyya, M.; Franklin, T.T.; Connolly, T.F.; Chien, W.; Charos, G.S.; Pelter, M.M. Cardiovascular responses to energy drinks in a healthy population: The C-energy study. Am. J. Emerg. Med. 2016, 34, 1205–1209. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on the safety of caffeine. EFSA J. 2015, 13, 4102. [Google Scholar]
- Guan, L.; Miao, P. The effects of taurine supplementation on obesity, blood pressure and lipid profile: A meta-analysis of randomized controlled trials. Eur. J. Pharmacol. 2020, 885, 173533. [Google Scholar] [CrossRef]
- Sun, Q.; Wang, B.; Li, Y.; Sun, F.; Li, P.; Xia, W.; Zhou, X.; Li, Q.; Wang, X.; Chen, J.; et al. Taurine Supplementation Lowers Blood Pressure and Improves Vascular Function in Prehypertension: Randomized, Double-Blind, Placebo-Controlled Study. Hypertension 2016, 67, 541–549. [Google Scholar] [CrossRef]
- van Koert, R.R.; Bauer, P.R.; Schuitema, I.; Sander, J.W.; Visser, G.H. Caffeine and seizures: A systematic review and quantitative analysis. Epilepsy Behav. 2018, 80, 37–47. [Google Scholar] [CrossRef]
- Lipton, R.B.; Diener, H.-C.; Robbins, M.S.; Garas, S.Y.; Patel, K. Caffeine in the management of patients with headache. J. Headache Pain 2017, 18, 107. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.A.; Hoirisch-Clapauch, S.; Nardi, A.E.; Freire, R.C. Panic Disorder and Chronic Caffeine Use: A Case-control Study. Clin. Pract. Epidemiol. Ment. Health 2019, 15, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Alsunni, A.A. Energy Drink Consumption: Beneficial and Adverse Health Effects. Int. J. Health Sci. 2015, 9, 468–474. [Google Scholar] [CrossRef]
- Babu, K.M.; Church, R.J.; Lewander, W. Energy Drinks: The New Eye-Opener for Adolescents. Clin. Pediatr. Emerg. Med. 2008, 9, 35–42. [Google Scholar] [CrossRef]
- Guze, S.B. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV). Am. J. Psychiatry 1995, 152, 1228. [Google Scholar]
- Moussa, M.; Hansz, K.; Rasmussen, M.; Gillman, C.; Pollard, C.; Kwak, E.; Izsak, E. Cardiovascular Effects of Energy Drinks in the Pediatric Population. Pediatr. Emerg. Care 2021, 37, 578–582. [Google Scholar] [CrossRef]
- Nordt, S.P.; Vilke, G.M.; Clark, R.F.; Cantrell, F.L.; Chan, T.C.; Galinato, M.; Nguyen, V.; Castillo, E.M. Energy Drink Use and Adverse Effects Among Emergency Department Patients. J. Community Health 2012, 37, 976–981. [Google Scholar] [CrossRef]
- Schwartz, D.L.; Gilstad-Hayden, K.; Carroll-Scott, A.; Grilo, S.A.; McCaslin, C.; Schwartz, M.; Ickovics, J.R. Energy drinks and youth self-reported hyperactivity/inattention symptoms. Acad. Pediatr. 2015, 15, 297–304. [Google Scholar] [CrossRef]
- Turnbull, D.; Rodricks, J.V.; Mariano, G.F.; Chowdhury, F. Caffeine and cardiovascular health. Regul. Toxicol. Pharmacol. 2017, 89, 165–185. [Google Scholar] [CrossRef]
- Van Batenburg-Eddes, T.; Lee, N.C.; Weeda, W.D.; Krabbendam, L.; Huizinga, M. The potential adverse effect of energy drinks on executive functions in early adolescence. Front. Psychol. 2014, 5, 457. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for niacin. EFSA J. 2014, 12, 3759. [Google Scholar] [CrossRef]
- Schneider, M.B.; Benjamin, H.J.; Committee on Nutrition and the Council on Sports Medicine and Fitness. Sports Drinks and Energy Drinks for Children and Adolescents: Are They Appropriate? Pediatrics 2011, 127, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Sheka, A.C.; Adeyi, O.; Thompson, J.; Hameed, B.; Crawford, P.A.; Ikramuddin, S. Nonalcoholic Steatohepatitis: A Review. JAMA 2020, 323, 1175–1183. [Google Scholar] [CrossRef]
- Greene, E.; Oman, K.; Lefler, M. Energy drink-induced acute kidney injury. Ann. Pharmacother. 2014, 48, 1366–1370. [Google Scholar] [CrossRef] [PubMed]
- Deighan, C.J.; Wong, K.M.; McLaughlin, K.J.; Harden, P. Rhabdomyolysis and acute renal failure resulting from alcohol and drug abuse. QJM 2000, 93, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, F. Emerging risk factors and markers of chronic kidney disease progression. Nat. Rev. Nephrol. 2009, 5, 677–689. [Google Scholar] [CrossRef]
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics 2011, 127, 511–528. [Google Scholar] [CrossRef]
- Lithuania Bans Sale of Energy Drinks to Minors. 2015. Available online: https://www.lrt.lt/en/news-in-english/19/43504/lithuania-bans-sale-of-energy-drinks-to-minors (accessed on 2 March 2023).
- Broadcasting, L.P. Minors-People Less than 18 Years Old-Will No Longer Be Able to Buy Energy Drinks as the Saeima on Thursday Adopted Amendments to Energy Drink Circulation Law, Reported LSM’s Latvian-Language Service. 2016. Available online: https://eng.lsm.lv/article/society/society/latvia-bans-energy-drink-sales-to-minors.a165212/ (accessed on 2 March 2023).



{kind=link}
{kind=link}
| Search Number | Queries |
|---|---|
| Queries in PubMed | |
| #1 | Search (Energy drink * [tw]) |
| #2 | Search (Child * [tw])]) OR (Adolescen * [tw]) OR (Teen * [tw]) OR (Youth * [tw]) |
| #3 | Search (case report * [tw]) OR (Case Reports [Publication Type]) OR (Comment [Publication Type]) OR (Letter [Publication Type]) |
| #4 | #1 AND #2 AND #3 |
| Queries in Cochrane | |
| #1 | (“energy drink *”): ti, ab, kw |
| #2 | (“child *”): ti, ab, kw OR (“adolescen *”): ti, ab, kw OR (“teen *”): ti, ab, kw OR (“youth *”): ti, ab, kw |
| #3 | (“case report *”): ti, ab, kw OR (comment): pt OR MeSH descriptor: [Editorial] explode all trees OR (“editorial): pt OR MeSH descriptor: [Letter] explode all trees OR (“letter”): pt |
| #4 | #1 AND #2 AND #3 |
| Queries in Web of Science | |
| #1 | TS = (Energy drink *) |
| #2 | TS = (child *) OR TS = (adolescen *) OR TS = (teen *) OR TS = (youth *) |
| #3 | TS = (case report *) |
| #4 | #1 AND #2 AND #3 |
| Author, Year | Age, Sex | Clinical Presentation | ED Consumption Behavior | Abnormal Results | Diagnosis | Potential Triggers | Preexisting Health Conditions | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Cardiovascular system | |||||||||
| Polat et al., 2013 [17] | 13, M | Acute mid-sternal chest pain | An ED (80 mg caffeine) for the first time the night before admission | Cardiac auscultation: S4 gallop; ECG: 2–3 mm ST-segment elevations in leads II, III, aVF and V3 through V5; dynamic T-wave changes in leads V3–V5 24 h after the onset; TEE: LVEF about 54% with moderate apical hypokinesis; coronary angiography: extensive dissection with a visible tear from the distal part of the LAD artery | SCAD with STEMI | None | None | Acetylsalicylic acid, subcutaneous enoxaparin, sublingual nitroglycerin, enalapril, metoprolol | Complete remission |
| Dufendach et al., 2012 [18] | 13, F | Palpitations, chest pain, shakiness, and dizziness | At least 1 16 oz ED (160 mg caffeine) every other day for 2 weeks prior to presentation | ECG: idiopathic extreme QT-prolongation; genetic testing: LQT1-causative mutation (G179S-KCNQ1) | Type 1 LQTS | None | Two “possible” fainting episodes | Beta-blockers | Partial remission |
| Di Rocco et al., 2011 [19] | 14, M | Persistent “heart fluttering” | Unknown ED amount the day before presentation | Irregular HR of 130/min with a 1/6 vibratory systolic ejection murmur; ECG: narrow-complex tachycardia with atrial fibrillation and occasional atrial flutter | Arrhythmia | Running race | None | Digoxin | Complete remission |
| Di Rocco et al., 2011 [19] | 16, M | Intoxication, vomiting after minor head trauma | Unknown ED amount mixed with vodka the day prior to admission | Irregular HR of 160/min; ECG: chaotic atrial tachycardia and atrial fibrillation with rapid ventricular response; blood ethanol level: 155 mg/dL | Arrhythmia | Alcohol, baseline stimulant medication (amphetamine, dextroamphetamine, montelukast, loratadine, doxycycline) | ADHD, asthma, allergies | A bolus of normal saline and intravenous fluid support | Complete remission |
| Usman et al., 2012 [20] | 16, M | Palpitations for one week and elevated BP | 80–100 ED cans in two weeks, at least 3 ED cans the day prior to presentation | BP: 150/95 mmHg; regular pulse of 110/min | Arterial hypertension; sinus tachycardia | None | None | None | Complete remission |
| Terlizzi et al., 2008 [21] | 16, F | Three months of orthostatic intolerance and episodes of transient loss of consciousness | 4–5 ED cans per day one week before symptom manifestation | A sharp increase in HR during head up tilt test from 88 to 128 bpm, at the 22nd minute BP and HR decreased and the patient referred dizziness, blurred vision, and malaise | Postural tachycardia syndrome | None | None | None | Complete remission |
| Own institutional experience | 16, F | Collapse, unconsciousness | Multiple ED cans days prior to event | Refractory ventricular fibrillation | Refractory ventricular fibrillation, circulatory failure, consecutive hypoxic brain damage | Lack of sleep, anxiety | History of myocarditis (confirmed by biopsy) | CPR, ECMO | Fatal outcome |
| Wilson et al., 2012 [22] | 17, M | Acute chest pain with radiation to the left arm | 5–7 ED cans (560–800 mg caffeine) the night prior to admission | ECG: Diffuse ST-segment elevations in leads II, III, AVF, V3–V6, and ST-segment depressions in leads V1 and AVR; elevated WBC; reduced potassium and bicarbonate; elevated CK and troponin T; TEE: LVEF at 50% with apical hypokinesis | Acute coronary artery vasospasm | None | Questionable myopericarditis | Acetylsalicylic acid, nitroglycerin, diltiazem | Complete remission |
| Neuropsychological system | |||||||||
| Butragueño Laiseca et al., 2019 [23] | 8, M | Paraesthesia around the oral commissure, clonus and commissure deviation, difficulty speaking and retaining saliva | 1 ED on daily basis, increased intake the week prior to admission | Electroencephalography: bihemispheric epileptiform activity, predominantly during non-REM sleep | Rolandic epilepsy | None | None | Oxcarbazepine | No remission |
| Staikoglou et al., 2022 [24] | 14, M | Dysarthria, headache, mild right-hand weakness, hypesthesia and right optic field deficits | 2 L of ED within 10 h prior to admission | BP: 190/120 mmHg, HR: 116/min, MRI: a typical “string and pearls” sign of the left P2 and P3 posterior cerebral artery segment | Brain ischemia secondary to dissection of posterior cerebral artery | None | None | Anticoagulation therapy | Partial remission |
| Babu et al., 2011 [25] | 15, M | Tonic-clonic seizure, postictal state, repeated vomiting | 2 ED bottles and a cup of coffee within 2 h | Temperature: 38.1 °C; pulse: 120/min, respiratory rate: 40/min; reduced potassium; serum caffeine level: 99 µg/mL; brain MRI: mild ethmoid sinus disease | Tonic-clonic seizure | Additional consumption of a cup of coffee | Seasonal allergies | Intravenous lorazepam, intravenous ondansetron and normal saline | Complete remission |
| Yamada-Takeda et al., 2019 [26] | 16, M | Breakthrough seizure | 9 g ED powder 2 times per day | A significant drop of valproic acid; probable drug-herb interaction (score of drug interaction probability scale: 5) | Breakthrough seizure | None | Generalized epilepsy and seizure-free for 2 years with divalproex extended-release | None | Complete remission |
| Samanta D, 2015 [27] | 16, M | Thunderclap headache, vomiting, left leg numbness and gait difficulty | 4 × 8 oz ED can (320 mg caffeine) several hours before the onset of symptoms | Tachycardia, brisk deep tendon reflexes of the left knee and ankle, positive Babinski sign of the left side; brain MRI: numerous cortical and subcortical foci of abnormally restricted diffusion; MR angiography: diffuse luminal irregularity with intermittent narrowing of distal branches of posterior cerebral artery | Reversible cerebral vasoconstriction syndrome | None | None | Oral analgetic and antiemetic medication, verapamil | Complete remission |
| Quadri et al., 2018 [28] | 17, F | New onset mania for 5 days | 1 or 2 16 oz ED containers (300–600 mg caffeine) per day over 7 days prior to admission | Urine drug screen: positive for cannabis; quantitative THC: 198 ng/mL | Caffeine-induced bipolar disorder | Prior cannabis use | None | Olanzapine | Partial remission |
| Other organ systems | |||||||||
| Apestegui et al., 2011 [29] | 16, M | Jaundiced | 15 cans of ED within 3 days 2 weeks before the first hepatitis episode; 3 cans of ED within 4 h 2 days prior to the second hepatitis episode | Elevated AST, ALT, BIL and GGT; biopsy sample: severe perivenular hepatocellular necrosis, major centrilobular and portal inflammation, minor signs of endotheliitis and cholangitis | Cholestatic hepatitis | None | Liver transplantation due to biliary tumor, retransplantation due to biliary tract lesions | Unchanged low-dose tacrolimus monotherapy | Partial remission |
| Robin et al., 2017 [30] | 17, M | Elevated ALT | Chronic consumption of 6 × 500 mL ED cans per day | Elevated ALT up to 274 U/L; ultrasound: moderate liver steatosis; liver biopsy: moderate steatosis and mild steatohepatitis | NASH | None | Fatigue | Change of diet and lifestyle | Partial remission |
| Schöffl et al., 2011 [31] | 17, M | Vomiting, dizziness, hyperventilating and capsular pain over both kidneys | 3 L ED (780 mg caffeine and 4600 mg taurine) mixed with 1 L vodka (380 g alcohol) over the course of an evening | Tachycardiac with an HR of 110/min, transient hypertension, serum creatinine: 6.9 mg/dL, urine sediment revealed acute tubular necrosis | Acute renal failure | Alcohol, 2 × 100 m running races | None | Hemodialysis, enalapril | Complete remission |
| Yazdi et al., 2008 [32] | 11, M | Asymptomatic lesions at both upper and lower extremities for 5 months | 1 ED daily | Physical examination: multiple ochre macules and patches with central petechiae localized on limbs and the lower abdomen; biopsy: epidermal acanthosis with intra-epidermal collection of lymphocytes; iron-stain detection of hemosiderin: lymphocytic infiltrate of the upper dermis containing hemosiderin deposits and extravasal erythrocytes adjacent to dermal blood vessels; PCR of T-cell receptor-γ: clonal rearrangement | Lichen aureus | None | None | ED abstinence | Complete remission |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.; Haas, N.A.; Dalla-Pozza, R.; Jakob, A.; Oberhoffer, F.S.; Mandilaras, G. Energy Drinks and Adverse Health Events in Children and Adolescents: A Literature Review. Nutrients 2023, 15, 2537. https://doi.org/10.3390/nu15112537
Li P, Haas NA, Dalla-Pozza R, Jakob A, Oberhoffer FS, Mandilaras G. Energy Drinks and Adverse Health Events in Children and Adolescents: A Literature Review. Nutrients. 2023; 15(11):2537. https://doi.org/10.3390/nu15112537
Chicago/Turabian StyleLi, Pengzhu, Nikolaus Alexander Haas, Robert Dalla-Pozza, André Jakob, Felix Sebastian Oberhoffer, and Guido Mandilaras. 2023. "Energy Drinks and Adverse Health Events in Children and Adolescents: A Literature Review" Nutrients 15, no. 11: 2537. https://doi.org/10.3390/nu15112537
APA StyleLi, P., Haas, N. A., Dalla-Pozza, R., Jakob, A., Oberhoffer, F. S., & Mandilaras, G. (2023). Energy Drinks and Adverse Health Events in Children and Adolescents: A Literature Review. Nutrients, 15(11), 2537. https://doi.org/10.3390/nu15112537