
Self-Assessment of INTERHEART Risk Stratification among the Middle-Aged Community in Malaysia

 , and
, and
Abstract
1. Introduction
2. Subjects and Methods
2.1. Study Design and Setting
2.2. Survey Instrument
2.3. Participation Eligibility
2.4. Survey Invitation and Informed Consent
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions and Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health Malaysia. Clinical Practice Guidelines on Primary and Secondary Prevention of Cardiovascular Disease; Ministry of Health Malaysia: Putrajaya, Malaysia, 2017.
- Firus Khan, A.Y.; Ramli, A.S.; Abdul Razak, S.; Mohd Kasim, N.A.; Chua, Y.A.; Ul-Saufie, A.Z.; Jalaludin, M.A.; Nawawi, H. The Malaysian HEalth and WellBeing AssessmenT (MyHEBAT) Study Protocol: An Initiation of a National Registry for Extended Cardiovascular Risk Evaluation in the Community. Int. J. Environ. Res. Public Health 2022, 19, 11789. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-K.; Ma, J.; Chan, K.Q.; Cheong, Y.; Hong, W.-L.; Ong, R.; Tay, W.; Chua, A.L. Pulse oximeter as a home assessment tool: Knowledge and user experience among the community in Malaysia during the COVID-19 pandemic. Asian Pac. J. Trop. Med. 2022, 15, 213–219. [Google Scholar] [CrossRef]
- Badawy, M.A.E.M.D.; Naing, L.; Johar, S.; Ong, S.; Rahman, H.A.; Tengah, D.S.N.A.P.; Chong, C.L.; Tuah, N.A.A. Evaluation of cardiovascular diseases risk calculators for CVDs prevention and management: Scoping review. BMC Public Health 2022, 22, 1742. [Google Scholar] [CrossRef] [PubMed]
- McGorrian, C.; Yusuf, S.; Islam, S.; Jung, H.; Rangarajan, S.; Avezum, A.; Prabhakaran, D.; Almahmeed, W.; Rumboldt, Z.; Budaj, A.; et al. Estimating modifiable coronary heart disease risk in multiple regions of the world: The INTERHEART Modifiable Risk Score. Eur. Heart J. 2011, 32, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Philip, J.; Salim, Y.; Shun Fu, L.; Quazi, I.; Koon, T.; Sumathy, R.; Rajeev, G.; Annika, R.; Scott, A.L.; Alvaro, A.; et al. Prognostic validation of a non-laboratory and a laboratory based cardiovascular disease risk score in multiple regions of the world. Heart 2018, 104, 581. [Google Scholar] [CrossRef]
- Selvarajah, S.; Kaur, G.; Haniff, J.; Cheong, K.C.; Hiong, T.G.; van der Graaf, Y.; Bots, M.L. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int. J. Cardiol. 2014, 176, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Noor Hassim, I.; Norazman, M.R.; Diana, M.; Khairul Hazdi, Y.; Rosnah, I. Cardiovascular risk assessment between urban and rural population in Malaysia. Med. J. Malays. 2016, 71, 331–337. [Google Scholar]
- Trautwein, E.A.; McKay, S. The Role of Specific Components of a Plant-Based Diet in Management of Dyslipidemia and the Impact on Cardiovascular Risk. Nutrients 2020, 12, 2671. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska, E.; Białek-Dratwa, A.; Janota, B.; Kowalski, O. Dietary Therapy in Prevention of Cardiovascular Disease (CVD)-Tradition or Modernity? A Review of the Latest Approaches to Nutrition in CVD. Nutrients 2022, 14, 2649. [Google Scholar] [CrossRef] [PubMed]
- Chiavaroli, L.; Nishi, S.K.; Khan, T.A.; Braunstein, C.R.; Glenn, A.J.; Mejia, S.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Jenkins, D.J.A.; et al. Portfolio Dietary Pattern and Cardiovascular Disease: A Systematic Review and Meta-analysis of Controlled Trials. Prog. Cardiovasc. Dis. 2018, 61, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Macho-González, A.; Garcimartín, A.; López-Oliva, M.E.; Bastida, S.; Benedí, J.; Ros, G.; Nieto, G.; Sánchez-Muniz, F.J. Can Meat and Meat-Products Induce Oxidative Stress? Antioxidants 2020, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Siew-Keah, L.; Hann, K.; Hoe, S.; En, L.; Chin, L.; Chan, M.; Kang, T.; Ang-Lim, C. Awareness and perceived barriers in practicing healthy living to prevent hypertension among young adults in Malaysia. Asian Pac. J. Trop. Med. 2022, 15, 542–550. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. National Health and Morbidity Survey 2019 Non-Communicable Diseases, Healthcare Demand, and Health Literacy; National Institutes of Health (NIH) Ministry of Health Malaysia: Shah Alam, Malaysia, 2019.
- Lim, K.H.; Lim, H.L.; Teh, C.H.; Kee, C.C.; Heng, P.P.; Cheah, Y.K.; Mohd Ghazali, S. Secondhand smoke (SHS) exposure at home and at the workplace among non-smokers in Malaysia: Findings from the Global Adult Tobacco Survey 2011. Tob. Induc. Dis. 2018, 16, 49. [Google Scholar] [CrossRef] [PubMed]
- Barnoya, J.; Glantz, S.A. Cardiovascular effects of secondhand smoke: Nearly as large as smoking. Circulation 2005, 111, 2684–2698. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhu, B.; Xu, S.; Bi, Y.; Liu, Y.; Shi, J. A cross country comparison for the burden of cardiovascular disease attributable to tobacco exposure in China, Japan, USA and world. BMC Public Health 2020, 20, 888. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- Kaufmann, R.; Babb, S.; O’Halloran, A.; Asman, K.; Bishop, E.; Tynan, M.; Caraballo, R.; Pechacek, T.; Bernert, J.; Blount, B. Vital signs: Nonsmokers’ exposure to secondhand smoke-United States, 1999–2008. Morb. Mortal. Wkly. Rep. 2010, 59, 1141–1146. [Google Scholar]



{kind=link}
{kind=link}
| n (%) | INTERHEART Risk Mean Score (SD) | |
|---|---|---|
| Age Group | ||
| 40–45 | 213 (35.4) | 9.6 (5.6) |
| 46–50 | 143 (23.8) | 9.8 (6.2) |
| 51–55 | 127 (21.1) | 9.2 (4.9) |
| 56–60 | 119 (19.8) | 11.3 (6.9) # |
| Gender | ||
| Male | 241 (40.0) | 12.4 (6.3) * |
| Female | 361 (60.0) | 8.3 (5.0) |
| BMI | ||
| Underweight | 32 (5.3) | 9.1 (6.2) |
| Normal | 372 (61.8) | 8.7 (5.2) |
| Overweight | 147 (24.4) | 11.52 (5.9) |
| Obese | 51 (8.5) | 14.53 (7.1) ### |
| Area of residence | ||
| Urban | 552 (91.7) | 9.9 (5.8) |
| Rural | 50 (8.3) | 9.5 (6.6) |
| Monthly household income | ||
| Low (RM < 4850) | 214 (35.5) | 10.05 (6.2) |
| Medium (RM 4850–10,970) | 261 (43.4) | 10.03 (5.9) |
| High (RM > 10,970) | 127 (21.1) | 9.34 (5.4) |
| Nature of occupation based on level of physical activity | ||
| Unemployed | 45 (7.5) | 8.7 (5.9) |
| Retiree | 58 (9.6) | 9.2 (7.2) |
| Manual/labour workers/requires high physical activity during working hours | 55 (9.1) | 12.1 (5.9) # |
| Office and desk-bound workers/requires less physical activity during working hours | 288 (47.8) | 9.6 (5.7) |
| Service-based/requires moderate physical activity during working hours | 156 (25.9) | 10.2 (5.6) |
| Occupation related to health care | ||
| Yes | 52 (8.6) | 9.8 (5.9) |
| No | 550 (91.4) | 9.9 (5.9) |
| Marital status | ||
| Single | 108 (17.9) | 10.4 (6.5) |
| Married | 462 (76.7) | 9.8 (5.7) |
| Divorced/widowed | 32 (5.3) | 10.4 (6.7) |
| Educational level | ||
| No formal/primary education | 36 (6.0) | 11.9 (6.7) # |
| Secondary education | 196 (32.6) | 10.7 (6.3) # |
| Tertiary education | 370 (61.5) | 9.3 (5.5) |
| Received any informative poster or brochure related to CVD | ||
| Yes | 206 (47.3) | 10.0 (5.9) |
| No | 317 (52.7) | 9.8 (5.9) |
| Aware of self-assessment tools that helps to predict CVD risk | ||
| Yes | 205 (34.1) | 9.1 (5.6) |
| No | 397 (65.9) | 10.3 (6.0) * |
| Undergone routine medical check-ups | ||
| Yes | 87 | 8.75 (5.5) * |
| No | 515 | 10.10 (6.0) |
| Risk Indicator | β | SE | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age | 0.034 | 0.037 | −0.038 | 0.105 | 0.358 |
| Gender | −3.257 | 0.478 | −4.196 | −2.318 | <0.001 *** |
| BMI | 0.332 | 0.055 | 0.224 | 0.441 | <0.001 *** |
| Area of residence | −0.256 | 0.803 | −1.832 | 1.321 | 0.750 |
| Monthly household income | −0.995 | 0.570 | −2.116 | 0.125 | 0.081 |
| Nature of occupation based on level of physical activity | 0.460 | 0.809 | −1.128 | 2.048 | 0.570 |
| Health-care related occupation | 0.157 | 0.788 | −1.390 | 1.703 | 0.843 |
| Marital status | −0.525 | 0.587 | −1.678 | 0.627 | 0.371 |
| Educational level | −1.040 | 0.502 | −2.026 | −0.054 | 0.039 * |
| Risk Factor (Risk Score) | Total (N = 602) | Male n (%) (n = 241) | Female n (%) (n = 361) | p-Value (Chi-Square; Male vs. Female) |
|---|---|---|---|---|
| Smoking status | ||||
| I never smoked (0) | 509 (84.5) | 159 (66.0) | 350 (97.0) | p < 0.001 |
| I am a former smoker (last smoked more than 12 months ago) (2) | 40 (6.6) | 35 (19.5) | 5 (1.4) | |
| I am a current smoker or I smoked regularly in the last 12 months, and I smoke | 53 (8.8) | 47 (19.5) | 6 (1.7) | |
| 1–5 cigarettes per day (2) | 12 | 10 (21.3) | 2 (33.3) | NS |
| 6–10 cigarettes per day (4) | 20 | 17 (36.2) | 3 (50.0) | |
| 11–15 cigarettes per day (6) | 7 | 7 (14.9) | 0 (0.0) | |
| 16–20 cigarettes per day (7) | 12 | 11 (23.4) | 1 (16.7) | |
| >21 cigarettes per day (11) | 2 | 2 (4.3) | 0 (0.0) | |
| Second hand smoke | ||||
| Over the past 12 months, what has been your typical exposure to other people’s tobacco smoke? | ||||
| Less than 1 h or exposure per week or no exposure (0) | 277 (46) | 112 (46.5) | 165 (45.7) | NS |
| OR One or more hours of second-hand smoke exposure per week (2) | 325 (54) | 129 (53.5) | 196 (54.3) | |
| Average of hours per week | 2.77 h | 3.91 h *** | 1.62 h | |
| Diabetes | ||||
| Do you have diabetes mellitus? | ||||
| Yes (6) | 39 (6.5) | 23 (9.5) | 16 (4.4) | p < 0.05 |
| No or unsure (0) | 563 (93.5) | 218 (90.5) | 345 (95.6) | |
| High blood pressure | ||||
| Do you have high blood pressure? | ||||
| Yes (5) | 93 (15.5) | 50 (20.7) | 43 (11.9) | p < 0.01 |
| No or unsure (0) | 509 (84.5) | 191 (79.3) | 318 (88.1) | |
| Family history | ||||
| Have either or both of your biological parents had a heart attack? | ||||
| Yes (4) | 130 (21.6) | 59 (24.5) | 71 (19.7) | NS |
| No or unsure (0) | 472 (78.4) | 182 (75.5) | 290 (80.3) | |
| Waist-to-hip ratio | ||||
| Quartile 1: Less than 0.873 (0) | 364 (60.5) | 77 (32.0) | 287 (79.5) | p < 0.001 |
| Quartile 2 and 3: 0.873–0.963 (2) | 181 (30) | 120 (49.8) | 61 (16.9) | |
| Quartile 4: greater than or =0.964 (4) | 57 (9.5) | 44 (18.3) | 13 (3.6) | |
| Psychosocial factors | ||||
| How often have you felt work or home life stress in the last year? | ||||
| Never or some periods (0) | 453 (75.3) | 186 (77.2) | 267 (74) | NS |
| OR Several periods of stress or permanent stress (3) | 149 (24.8) | 55 (22.8) | 94 (26) | |
| During the past 12 months, was there ever a time when you felt sad, blue, or depressed for two weeks or more in a row? | ||||
| Yes (3) | 157 (26.1) | 62 (25.7) | 95 (26.3) | NS |
| No (0) | 445 (73.9) | 179 (74.3) | 266 (73.7) | |
| Dietary factors | ||||
| Do you eat salty food or snacks one or more times a day? | ||||
| Yes (1) | 199 (33.1) | 81 (33.6) | 118 (32.7) | NS |
| No (0) | 403 (66.9) | 160 (66.4) | 243 (67.3) | |
| Do you eat deep fried foods or snacks or fast foods 3 or more times a week? | ||||
| Yes (1) | 227 (37.7) | 107 (44.4) | 120 (33.2) | p < 0.01 |
| No (0) | 375 (62.3) | 134 (55.6) | 241 (66.8) | |
| Do you eat fruit one or more times daily? | ||||
| Yes (0) | 413 (68.6) | 155 (64.3) | 258 (71.5) | NS |
| No (1) | 189 (31.4) | 86 (35.7) | 103 (28.5) | |
| Do you eat vegetables one or more times daily? | ||||
| Yes (0) | 413 (68.6) | 155 (64.3) | 258 (71.5) | NS |
| No (1) | 189 (31.4) | 86 (35.7) | 103 (28.5) | |
| Do you eat meat and/or poultry 2 or more times daily? | ||||
| Yes (2) | 366 (60.8) | 168 (69.7) | 198 (54.8) | p < 0.001 |
| No (0) | 236 (39.2) | 73 (30.3) | 163 (45.2) | |
| Physical activity | ||||
| How active are you during your leisure time? | ||||
| I am mainly sedentary or perform mild exercise (requiring minimal effort) (2) | 355 (59) | 124 (51.5) | 231 (64) | p < 0.05 |
| OR I perform moderate or strenuous physical activity in my leisure time (0) | 247 (41) | 117 (48.5) | 130 (36) | |
| INTERHEART Risk | ||||
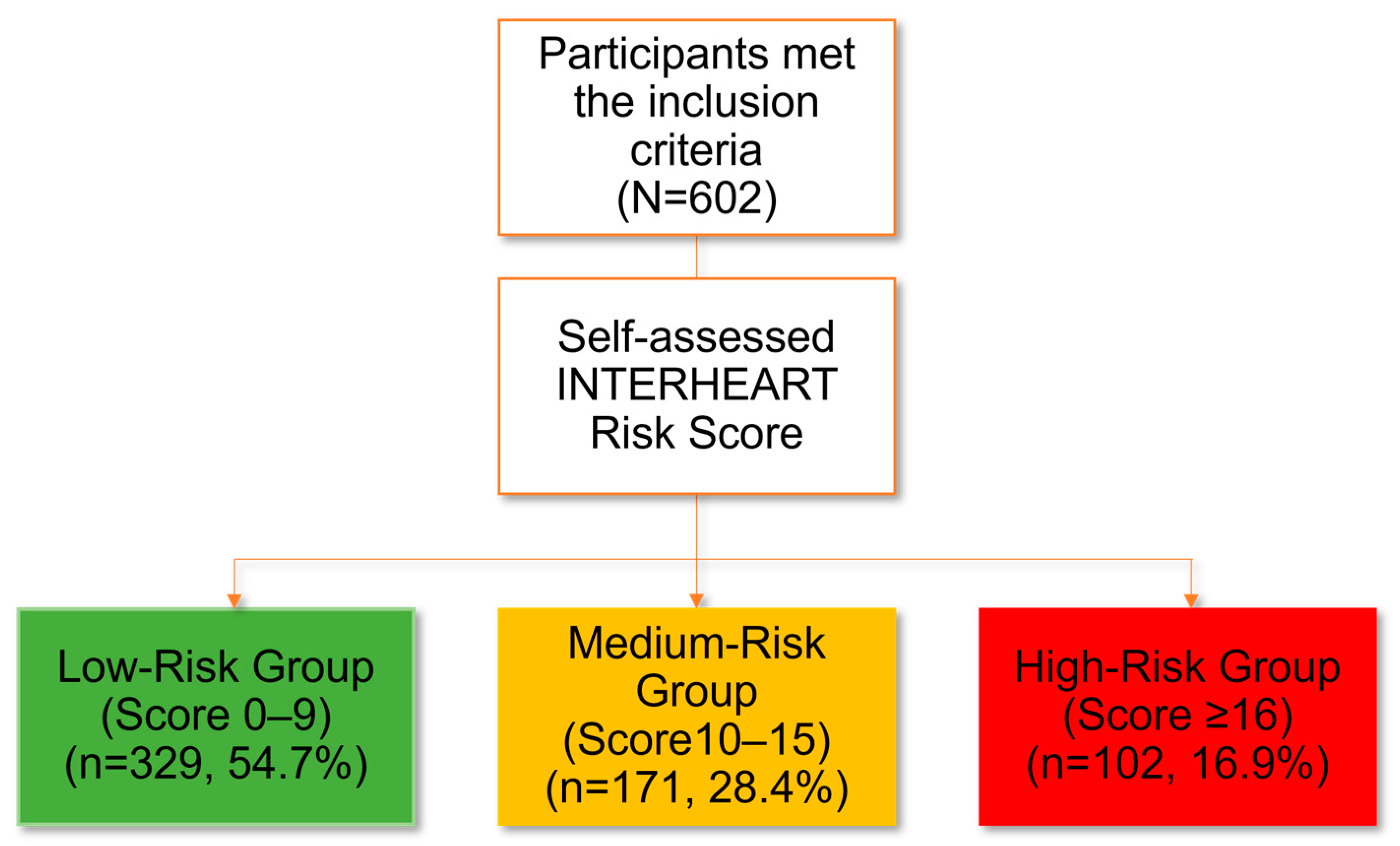
| Low risk (Score of 0–9) | 329 (54.6) | 86 (35.7) | 243 (67.3) | p < 0.001 |
| Medium risk (Score of 10–15) | 171 (28.4) | 86 (35.7) | 85 (23.5) | |
| High risk (Score ≥ 16) | 102 (16.9) | 69 (28.6) | 33 (9.1) | |
| Risk Factor (Risk Score) | Labour Workers (n,%) (n = 55) | Desk-Bound Workers (n,%) (n = 288) | p-Value (Chi-Square, Manual vs. Office) |
|---|---|---|---|
| Smoking status | |||
| I never smoked (0) | 34 (61.8) | 255 (88.5) | p < 0.001 |
| I am a former smoker (last smoked more than 12 months ago) (2) | 6 (10.9) | 15 (5.2) | |
| I am a current smoker or I smoked regularly in the last 12 months, and I smoke | 15 (27.3) | 18 (6.3) | |
| 1–5 cigarettes per day (2) | 1 (6.7) | 4 (26.7) | p < 0.05 |
| 6–10 cigarettes per day (4) | 5 (33.3) | 8 (53.3) | |
| 11–15 cigarettes per day (6) | 5 (33.3) | 0 (0.0) | |
| 16–20 cigarettes per day (7) | 4 (26.7) | 2 (13.3) | |
| >21 cigarettes per day (11) | 0 (0.0) | 1 (6.7) | |
| Second hand smoke | |||
| Over the past 12 months, what has been your typical exposure to other people’s tobacco smoke? | |||
| Less than 1 h or exposure per week or no exposure (0) | 31 (56.4) | 131 (45.5) | NS (0.139) |
| OR One or more hours of second-hand smoke exposure per week (2) | 24 (43.6) | 157 (54.5) | |
| Average of hours per week | 2.86 h *** | 1.6 h | - |
| Diabetes | |||
| Do you have diabetes mellitus? | |||
| Yes (6) | 6 (10.9) | 17 (5.9) | NS |
| No or unsure (0) | 49 (89.1) | 271 (94.1) | |
| High blood pressure | |||
| Do you have high blood pressure? | |||
| Yes (5) | 13 (23.6) | 40 (13.9) | NS |
| No or unsure (0) | 42 (76.4) | 248 (86.1) | |
| Family history | |||
| Have either or both of your biological parents had a heart attack? | |||
| Yes (4) | 14 (25.5) | 59 (20.5) | NS |
| No or unsure (0) | 41 (74.5) | 229 (79.5) | |
| Waist-to-hip ratio | |||
| Quartile 1: Less than 0.873 (0) | 28 (50.9) | 182 (63.2) | NS |
| Quartile 2 and 3: 0.873–0.963 (2) | 20 (36.4) | 79 (27.4) | |
| Quartile 4: greater than or =0.964 (4) | 7 (12.7) | 27 (9.4) | |
| Psychosocial factors | |||
| How often have you felt work or home life stress in the last year? | |||
| Never or some periods (0) | 44 (80.0) | 200 (69.5) | NS |
| OR Several periods of stress or permanent stress (3) | 11 (20.0) | 88 (30.5) | |
| During the past 12 months, was there ever a time when you felt sad, blue, or depressed for two weeks or more in a row? | |||
| Yes (3) | 11 (20.0) | 81 (28.1) | NS |
| No (0) | 44 (80.0) | 207 (71.9) | |
| Dietary factors | |||
| Do you eat salty food or snacks one or more times a day? | |||
| Yes (1) | 17 (30.9) | 101 (35.1) | NS |
| No (0) | 38 (69.1) | 187 (64.9) | |
| Do you eat deep fried foods or snacks or fast foods 3 or more times a week? | |||
| Yes (1) | 15 (27.3) | 113 (39.2) | NS |
| No (0) | 40 (72.7) | 175 (60.8) | |
| Do you eat fruit one or more times daily? | |||
| Yes (0) | 29 (52.7) | 204 (70.8) | p < 0.01 |
| No (1) | 26 (47.3) | 84 (29.2) | |
| Do you eat vegetables one or more times daily? | |||
| Yes (0) | 29 (52.7) | 204 (70.8) | p < 0.01 |
| No (1) | 26 (47.3) | 84 (29.2) | |
| Do you eat meat and/or poultry 2 or more times daily? | |||
| Yes (2) | 36 (65.5) | 177 (61.5) | NS |
| No (0) | 19 (34.5) | 111 (38.5) | |
| Physical activity | |||
| How active are you during your leisure time? | |||
| I am mainly sedentary or perform mild exercise (requiring minimal effort) (2) | 29 (52.7) | 177 (61.5) | NS |
| OR I perform moderate or strenuous physical activity in my leisure time (0) | 26 (47.3) | 111 (38.5) | |
| INTERHEART Risk Stratification | |||
| Low risk (Score of 0–9) | 19 (34.5) | 167 (58.0) | p < 0.001 |
| Medium risk (Score of 10–15) | 16 (29.1) | 83 (28.8) | |
| High risk (Score ≥ 16) | 20 (36.4) | 38 (13.2) | |
| Occupation/Educational Level | No formal Education/Primary Education (n) | Secondary Education (n) | Tertiary Education (n) | Chi-Square, p-Value |
|---|---|---|---|---|
| Labour workers | 12 | 34 | 9 | p < 0.001 |
| Desk-bound workers | 3 | 64 | 221 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-K.; Chua, A.-L.; Fong, C.H.Y.; Ban, B.C.H.; Ng, W.L.; Kong, J.F.; Chew, Y.-L.; Liew, K.B. Self-Assessment of INTERHEART Risk Stratification among the Middle-Aged Community in Malaysia. Nutrients 2023, 15, 2382. https://doi.org/10.3390/nu15102382
Lee S-K, Chua A-L, Fong CHY, Ban BCH, Ng WL, Kong JF, Chew Y-L, Liew KB. Self-Assessment of INTERHEART Risk Stratification among the Middle-Aged Community in Malaysia. Nutrients. 2023; 15(10):2382. https://doi.org/10.3390/nu15102382
Chicago/Turabian StyleLee, Siew-Keah, Ang-Lim Chua, Clement Heng Yew Fong, Brian Cong Hao Ban, Wen Ling Ng, Jing Feng Kong, Yik-Ling Chew, and Kai Bin Liew. 2023. "Self-Assessment of INTERHEART Risk Stratification among the Middle-Aged Community in Malaysia" Nutrients 15, no. 10: 2382. https://doi.org/10.3390/nu15102382
APA StyleLee, S.-K., Chua, A.-L., Fong, C. H. Y., Ban, B. C. H., Ng, W. L., Kong, J. F., Chew, Y.-L., & Liew, K. B. (2023). Self-Assessment of INTERHEART Risk Stratification among the Middle-Aged Community in Malaysia. Nutrients, 15(10), 2382. https://doi.org/10.3390/nu15102382