
The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Formulation of the Research Question
2.2. Systematic Searching Strategy
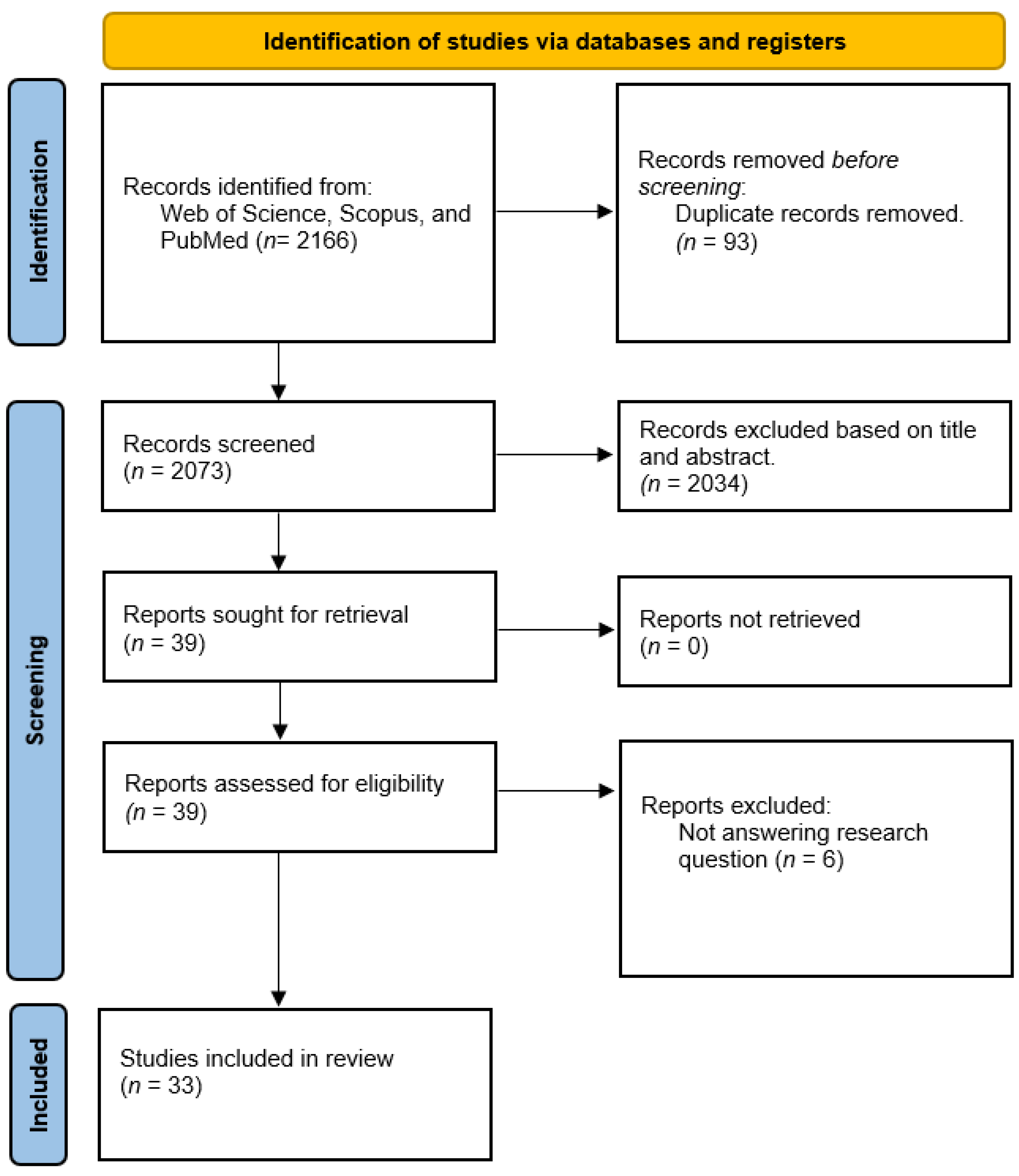
2.3. Identification
2.4. Screening by Using Inclusion and Exclusion Criteria
2.5. Eligibility
2.6. Quality Assessment
2.7. Data Abstraction and Analysis
3. Results
3.1. Background of the Included Studies
3.2. Outcome Summary of Vitamin D Deficiency among T2DM Patients
4. Discussion
4.1. Vitamin D Deficiency and Mental Health
4.2. Vitamin D Deficiency and Microvascular Complications
4.3. Vitamin D Deficiency and Macrovascular Complications
4.4. Vitamin D Deficiency and Metabolic Syndrome
4.5. Vitamin D Deficiency and Risk of Obesity
4.6. Vitamin D Deficiency and Blood Pressure
4.7. Vitamin D Deficiency and Glycaemic Control
4.8. Vitamin D Deficiency and Nerve-Related Complications
4.9. Vitamin D Deficiency and Musculoskeletal Complications
4.10. Vitamin D Deficiency and Quality of Life
4.11. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maia, F.A.; Oliveira, L.M.M.; Almeida, M.T.C.; Alves, M.R.; De Araújo Saeger, V.S.; Da Silva, V.B.; De Oliveira, V.S.D.; Junior, H.M.; Brito, M.F.S.F.; Da Silveira, M.F. Autism Spectrum Disorder and Postnatal Factors: A Case-Control Study in Brazil. Rev. Paul. Pediatr. 2019, 37, 398–405. [Google Scholar] [CrossRef]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global Prevalence and Disease Burden of Vitamin D Deficiency: A Roadmap for Action in Low- and Middle-Income Countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D Supplementation Guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef]
- WHO Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 3 May 2023).
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global Estimates of Diabetes Prevalence for 2017 and Projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and Chronic Diseases. Aging Dis. 2017, 8, 346–353. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D Deficiency and Diabetes. Biochem. J. 2017, 474, 1321–1332. [Google Scholar] [CrossRef]
- Klahold, E.; Penna-Martinez, M.; Bruns, F.; Seidl, C.; Wicker, S.; Badenhoop, K. Vitamin D in Type 2 Diabetes: Genetic Susceptibility and the Response to Supplementation. Horm. Metab. Res. 2020, 52, 492–499. [Google Scholar] [CrossRef]
- Isa, Z.M.; Nordin, N.R.M.; Mahmud, M.H.; Hashim, S. An Update on Vitamin D Deficiency Status in Malaysia. Nutrients 2022, 14, 567. [Google Scholar] [CrossRef]
- Laird, E.; Ward, M.; McSorley, E.; Strain, J.J.; Wallace, J. Vitamin D and Bone Health; Potential Mechanisms. Nutrients 2010, 2, 693–724. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A Global Perspective for Health. Dermatoendocrinology 2013, 5, 51–108. [Google Scholar] [CrossRef]
- Shin, M.H.; Lee, Y.; Kim, M.K.; Lee, D.H.; Chung, J.H. UV Increases Skin-Derived 1α,25-Dihydroxyvitamin D3 Production, Leading to MMP-1 Expression by Altering the Balance of Vitamin D and Cholesterol Synthesis from 7-Dehydrocholesterol. J. Steroid Biochem. Mol. Biol. 2019, 195, 105449. [Google Scholar] [CrossRef]
- Shin, Y.H.; Shin, H.J.; Lee, Y.J. Vitamin D Status and Childhood Health. Korean J. Pediatr. 2013, 56, 417–423. [Google Scholar] [CrossRef]
- Höbaus, J.; Thiem, U.; Hummel, D.M.; Kallay, E. Role of Calcium, Vitamin D, and the Extrarenal Vitamin D Hydroxylases in Carinogenesis. Anti Cancer Agents Med. Chem. (Former. Curr. Med. Chem. Anti Cancer Agents) 2013, 13, 20–35. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef]
- Christakos, S.; Ajibade, D.V.; Dhawan, P.; Fechner, A.J.; Mady, L.J. Vitamin D: Metabolism. Endocrinol. Metab. Clin. N. Am. 2010, 39, 243–253. [Google Scholar] [CrossRef]
- Cantorna, M.T.; Zhu, Y.; Froicu, M.; Wittke, A. Vitamin D Status, 1,25-Dihydroxyvitamin D3, and the Immune System. Am. J. Clin. Nutr. 2004, 80, 1717S–1720S. [Google Scholar] [CrossRef]
- Gil, Á.; Plaza-Diaz, J.; Mesa, M.D. Vitamin D: Classic and Novel Actions. Ann. Nutr. Metab. 2018, 72, 87–95. [Google Scholar] [CrossRef]
- Al Shoumer, K.; Al-Essa, T. Is There a Relationship between Vitamin D with Insulin Resistance and Diabetes Mellitus? World J. Diabetes 2015, 6, 1057. [Google Scholar] [CrossRef]
- Marino, R.; Misra, M. Extra-Skeletal Effects of Vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef]
- Bukhary, N.B.I.; Isa, Z.M.; Shamsuddin, K.; Lin, K.G.; Mahdy, Z.A.; Hassan, H.; Yeop, N.S.H. Risk Factors for Antenatal Hypovitaminosis D in an Urban District in Malaysia. BMC Pregnancy Childbirth 2016, 16, 4–13. [Google Scholar] [CrossRef]
- Saffian, S.M.; Jamil, N.A.; Tahir, N.A.M.; Hatah, E. Vitamin D Insufficiency Is High in Malaysia: A Systematic Review and Meta-Analysis of Studies on Vitamin D Status in Malaysia. Front. Nutr. 2022, 9, 2861. [Google Scholar] [CrossRef]
- Arafat, E.S.; Taha, I.M.; Kattan, S.W.; Babteen, N.A.; Fawzy, I. Associations between Vitamin D and Type 2 Diabetes Mellitus: The Role of Vitamin D Receptor and Binding Protein. J. Diabetes Mellit. 2020, 10, 222–235. [Google Scholar] [CrossRef]
- Alam, U.; Arul-Devah, V.; Javed, S.; Malik, R.A. Vitamin D and Diabetic Complications: True or False Prophet? Diabetes Ther. 2016, 7, 11–26. [Google Scholar] [CrossRef]
- Sheth, J.J.; Shah, A.; Sheth, F.J.; Trivedi, S.; Lele, M.; Shah, N.; Thakor, P.; Vaidya, R. Does Vitamin D Play a Significant Role in Type 2 Diabetes? BMC Endocr. Disord. 2015, 15, 5. [Google Scholar] [CrossRef]
- Smart, H.; AlGhareeb, A.M.; Smart, S.A. 25-Hydroxyvitamin D Deficiency: Impacting Deep-Wound Infection and Poor Healing Outcomes in Patients with Diabetes. Adv. Ski. Wound Care 2019, 32, 321–328. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; John, P.A. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Hong, Q.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT): User Guide 2018. McGill 2018, 204, 1–10. [Google Scholar]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; Mu, P. Conducting Systematic Reviews of Association (Etiology): The Joanna Briggs Institute’s Approach. Int. J. Evid. Based. Healthc. 2015, 13, 163–169. [Google Scholar] [CrossRef]
- Darraj, H.; Badedi, M.; Poore, K.R.; Hummadi, A.; Khawaji, A.; Solan, Y.; Zakri, I.; Sabai, A.; Darraj, M.; Mutawwam, D.A.; et al. Vitamin D Deficiency and Glycemic Control among Patients with Type 2 Diabetes Mellitus in Jazan City, Saudi Arabia. Diabetes Metab. Syndr. Obes. 2022, 12, 853–862. [Google Scholar] [CrossRef]
- Tang, W.; Chen, L.; Ma, W.; Chen, D.; Wang, C.; Gao, Y.; Ran, X. Association between Vitamin D Status and Diabetic Foot in Patients with Type 2 Diabetes Mellitus. J. Diabetes Investig. 2022, 13, 1213–1221. [Google Scholar] [CrossRef]
- Wang, F.; Zhou, L.; Zhu, D.; Yang, C. A Retrospective Analysis of the Relationship between 25-OH-Vitamin D and Diabetic Foot Ulcer. Diabetes Metab. Syndr. Obes. 2022, 15, 1347–1355. [Google Scholar] [CrossRef]
- Geng, T.; Lu, Q.; Wan, Z.; Guo, J.; Liu, L.; Pan, A.; Liu, G. Association of Serum 25-Hydroxyvitamin D Concentrations with Risk of Dementia among Individuals with Type 2 Diabetes: A Cohort Study in the UK Biobank. PLoS Med. 2022, 19, e1003906. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.H.; Mohd, M.; Dar, I.H.; Bhat, J.A. Role of Vitamin D Deficiency in Type 2 Diabetes: Association or Coincidence? Clin. Diabetol. 2021, 10, 188–194. [Google Scholar] [CrossRef]
- Salih, Y.A.; Rasool, M.T.; Ahmed, I.H.; Mohammed, A.A. Impact of Vitamin D Level on Glycemic Control in Diabetes Mellitus Type 2 in Duhok. Ann. Med. Surg. 2021, 64, 102208. [Google Scholar] [CrossRef] [PubMed]
- Assy, M.H.; Draz, N.A.; Fathy, S.E.; Hamed, M.G. Impact of Vitamin D Level in Diabetic People with Peripheral Neuropathy. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 117. [Google Scholar] [CrossRef]
- Mendoza-Garcés, L.; Velázquez-Alva, M.C.; Cabrer-Rosales, M.F.; Arrieta-Cruz, I.; Gutiérrez-Juárez, R.; Irigoyen-Camacho, M.E. Vitamin D Deficiency Is Associated with Handgrip Strength, Nutritional Status and T2DM in Community-Dwelling Older Mexican Women: A Cross-Sectional Study. Nutrients 2021, 13, 736. [Google Scholar] [CrossRef]
- Aghamohammadzadeh, N.; Dolatkhah, N.; Hashemian, M.; Shakouri, S.K.; Hasanpour, S. The Relationship between Serum 25-Hydroxy Vitamin D and Blood Pressure and Quality of Life in Overweight and Obese Patients with Type 2 Diabetes Mellitus Compared with Healthy Subjects. Casp. J. Intern. Med. 2020, 11, 267–277. [Google Scholar] [CrossRef]
- Xiao, Y.; Wei, L.; Xiong, X.; Yang, M.; Sun, L. Association between Vitamin D Status and Diabetic Complications in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study in Hunan China. Front. Endocrinol. 2020, 11, 564738. [Google Scholar] [CrossRef]
- Dai, J.; Yu, M.; Chen, H.; Chai, Y. Association between Serum 25-OH-Vitamin D and Diabetic Foot Ulcer in Patients with Type 2 Diabetes. Front. Nutr. 2020, 7, 109. [Google Scholar] [CrossRef]
- Ahmed, L.H.M.; Butler, A.E.; Dargham, S.R.; Latif, A.; Robay, A.; Chidiac, O.M.; Jayyousi, A.; Al Suwaidi, J.; Crystal, R.G.; Atkin, S.L.; et al. Association of Vitamin D2 and D3 with Type 2 Diabetes Complications. BMC Endocr. Disord. 2020, 20, 65. [Google Scholar] [CrossRef]
- Samefors, M.; Scragg, R.; Nystrom, F.H.; Östgren, C.J. Is There an Association between Serum 25(OH)D3 and Mental Well-Being in Patients with Type 2 Diabetes? Results from a Cohort Study in Primary Care. Hormones 2020, 19, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Fan, D.; Yin, F. The Relationship between Vitamin D Status and Visceral Fat Accumulation in Males with Type 2 Diabetes. J. Nutr. Sci. Vitaminol. 2020, 66, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Liu, J.; Zhou, X.; Ding, H.; Xu, J.; Yang, B.; Sun, B.; Xiao, D.; Yu, J.; Gong, Q. Correlation Analysis between Serum Vitamin D Levels and Lower Extremity Macrovascular Complications in Individuals with Type 2 Diabetes Mellitus. J. Diabetes Res. 2019, 2019, 251829. [Google Scholar] [CrossRef] [PubMed]
- Parveen, R.; Kapur, P.; Venkatesh, S.; Agarwal, N.B. Attenuated Serum 25-Hydroxyvitamin D and Vitamin D Binding Protein Associated with Cognitive Impairment in Patients with Type 2 Diabetes. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1763–1772. [Google Scholar] [CrossRef]
- Yuan, J.; Jia, P.; Hua, L.; Xin, Z.; Yang, J.K. Vitamin D Deficiency Is Associated with Risk of Developing Peripheral Arterial Disease in Type 2 Diabetic Patients. BMC Cardiovasc. Disord. 2019, 19, 145. [Google Scholar] [CrossRef]
- Xie, S.; Huang, L.; Cao, W.; Hu, Y.; Sun, H.; Cao, L.; Liu, K.; Liu, C. Association between Serum 25-Hydroxyvitamin D and Diabetic Kidney Disease in Chinese Patients with Type 2 Diabetes. PLoS ONE 2019, 14, e0214728. [Google Scholar] [CrossRef]
- Karau, P.B.; Kirna, B.; Amayo, E.; Joshi, M.; Ngare, S.; Muriira, G. The Prevalence of Vitamin D Deficiency among Patients with Type 2 Diabetes Seen at a Referral Hospital in Kenya. Pan Afr. Med. J. 2019, 34, 38. [Google Scholar] [CrossRef]
- Alcubierre, N.; Castelblanco, E.; Martínez-Alonso, M.; Granado-Casas, M.; Esquerda, A.; Traveset, A.; Martinez-Gonzalez, D.; Franch-Nadal, J.; Mauricio, D. Vitamin D Deficiency Is Associated with Poorer Satisfaction with Diabetes-Related Treatment and Quality of Life in Patients with Type 2 Diabetes: A Cross-Sectional Study. Health Qual. Life Outcomes 2018, 16, 44. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, H.; Meng, P.; Han, Y. Association between Low Serum 25-Hydroxyvitamin D and Depression in a Large Sample of Chinese Patients with Type 2 Diabetes Mellitus. J. Affect. Disord. 2017, 224, 56–60. [Google Scholar] [CrossRef]
- Saif-Elnasr, M.; Ibrahim, I.M.; Alkady, M.M. Role of Vitamin D on Glycemic Control and Oxidative Stress in Type 2 Diabetes Mellitus. J. Res. Med. Sci. 2017, 22, 22. [Google Scholar] [CrossRef]
- Guo, L.; Gao, Z.; Ge, H. Effects of Serum 25-HydroxyvitaminD Level on Decreased Bone Mineral Density at Femoral Neck and Total Hip in Chinese Type 2 Diabetes. PLoS ONE 2017, 12, e0188894. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.H.; Wei, T.M.; Qian, L.Y.; Ma, Y.; Lao, D.B.; Yao, B.; Pang, J. Association between Serum 25-Hydroxyvitamin D and Carotid Atherosclerotic Plaque in Chinese Type 2 Diabetic Patients. Medicine 2017, 96, e6445. [Google Scholar] [CrossRef] [PubMed]
- Raelene, E.M.; Lenhard, M.J.; Pohlig, R.T. Vitamin D insufficiency is associated with reduced parasympathetic nerve fiber function in type 2 diabetes. Endocr. Pract. 2017, 21, 174–181. [Google Scholar] [CrossRef]
- Pan, G.T.; Guo, J.F.; Mei, S.L.; Zhang, M.X.; Hu, Z.Y.; Zhong, C.K.; Zeng, C.Y.; Liu, X.H.; Ma, Q.H.; Li, B.Y.; et al. Vitamin D Deficiency in Relation to the Risk of Metabolic Syndrome in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus. J. Nutr. Sci. Vitaminol. 2016, 62, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Okada, Y.; Tanaka, Y. Incidence of Vitamin D Deficiency and Its Relevance to Bone Metabolism in Japanese Postmenopausal Women with Type 2 Diabetes Mellitus. Intern. Med. 2015, 54, 1599–1604. [Google Scholar] [CrossRef]
- Zoppini, G.; Galletti, A.; Targher, G.; Brangani, C.; Pichiri, I.; Trombetta, M.; Negri, C.; de Santi, F.; Stoico, V.; Cacciatori, V.; et al. Lower Levels of 25-Hydroxyvitamin D3 Are Associated with a Higher Prevalence of Microvascular Complications in Patients with Type 2 Diabetes. BMJ Open Diabetes Res. Care 2015, 3, e000058. [Google Scholar] [CrossRef]
- Kajbaf, F.; Mentaverri, R.; Diouf, M.; Fournier, A.; Kamel, S.; Lalau, J.D. The Association between 25-Hydroxyvitamin D and Hemoglobin A1c Levels in Patients with Type 2 Diabetes and Stage 1-5 Chronic Kidney Disease. Int. J. Endocrinol. 2014, 2014, 142468. [Google Scholar] [CrossRef]
- Tiwari, S.; Pratyush, D.D.; Gupta, B.; Dwivedi, A.; Chaudhary, S.; Rayicherla, R.K.; Gupta, S.K.; Singh, S.K. Prevalence and Severity of Vitamin D Deficiency in Patients with Diabetic Foot Infection. Br. J. Nutr. 2013, 109, 99–102. [Google Scholar] [CrossRef]
- Gandhe, M.B.; Jain, K.; Gandhe, S.M. Evaluation of 25(OH) Vitamin D3 with Reference to Magnesium Status and Insulin Resistance in T2DM. J. Clin. Diagn. Res. 2013, 7, 2438–2441. [Google Scholar] [CrossRef]
- Kostoglou-Athanassiou, I.; Athanassiou, P.; Gkountouvas, A.; Kaldrymides, P. Vitamin D and Glycemic Control in Diabetes Mellitus Type 2. Ther. Adv. Endocrinol. Metab. 2013, 4, 122–128. [Google Scholar] [CrossRef]
- Payne, J.F.; Ray, R.; Watson, D.G.; Delille, C.; Rimler, E.; Cleveland, J.; Lynn, M.J.; Tangpricha, V.; Srivastava, S.K. Vitamin D Insufficiency in Diabetic Retinopathy. Endocr. Pract. 2012, 18, 2, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Millen, A.E.; Sahli, M.W.; Nie, J.; LaMonte, M.J.; Lutsey, P.L.; Klein, B.E.K.; Mares, J.A.; Meyers, K.J.; Andrews, C.A.; Klein, R. Adequate Vitamin D Status Is Associated with the Reduced Odds of Prevalent Diabetic Retinopathy in African Americans and Caucasians. Cardiovasc. Diabetol. 2016, 15, 128. [Google Scholar] [CrossRef] [PubMed]
- Alcubierre, N.; Valls, J.; Rubinat, E.; Cao, G.; Esquerda, A.; Traveset, A.; Granado-Casas, M.; Jurjo, C.; Mauricio, D. Vitamin D Deficiency Is Associated with the Presence and Severity of Diabetic Retinopathy in Type 2 Diabetes Mellitus. J. Diabetes Res. 2015, 2015, 374178. [Google Scholar] [CrossRef] [PubMed]
- Catoi, A.F.; Iancu, M.; Parvu, A.E.; Cecan, A.D.; Bidian, C.; Chera, E.I.; Pop, I.D.; Macri, A.M. Relationship between 25 Hydroxyvitamin D, Overweight/Obesity Status, Pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model. Nutrients 2021, 25, 2889. [Google Scholar] [CrossRef] [PubMed]
- Majeed, F. Low Levels of Vitamin D an Emerging Risk for Cardiovascular Diseases: A Review. Int. J. Health Sci. 2017, 11, 71–76. [Google Scholar]
- Amsah, N.; Isa, Z.; Ahmad, N. Biopsychosocial and Nutritional Factors of Depression among Type 2 Diabetes Mellitus Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 191, 4888. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, X.; Jia, Y.; Wen, Y.; Cheng, S.; Meng, P.; Li, C.; Zhang, H.; Pan, C.; Zhang, J.; et al. Vitamin D and the Risks of Depression and Anxiety: An Observational Analysis and Genome-Wide Environment Interaction Study. Nutrients 2021, 13, 3343. [Google Scholar] [CrossRef]
- Dogan-Sander, E.; Mergl, R.; Willenberg, A.; Baber, R.; Wirkner, K.; Riedel-Heller, S.G.; Röhr, S.; Schmidt, F.M.; Schomerus, G.; Sander, C. Inflammation and the Association of Vitamin D and Depressive Symptomatology. Nutrients 2021, 13, 1972. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Altieri, B.; Penna-Martinez, M.; Badenhoop, K. Focus on Vitamin D and the Adrenal Gland. Horm. Metab. Res. 2015, 47, 239–246. [Google Scholar] [CrossRef]
- Jahrami, H.; Bragazzi, N.L.; Grant, W.B.; Alfarra, H.S.M.; Alfara, W.S.M.; Mashalla, S.; Saif, Z. Vitamin D Doses from Solar Ultraviolet and Dietary Intakes in Patients with Depression: Results of a Case-Control Study. Nutrients 2020, 12, 2587. [Google Scholar] [CrossRef]
- Omidian, M.; Mahmoudi, M.; Abshirini, M.; Eshraghian, M.R.; Javanbakht, M.H.; Zarei, M.; Hasani, H.; Djalali, M. Effects of Vitamin D Supplementation on Depressive Symptoms in Type 2 Diabetes Mellitus Patients: Randomized Placebo-Controlled Double-Blind Clinical Trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2375–2380. [Google Scholar] [CrossRef] [PubMed]
- Boyuk, B.; Atalay, H.; Degirmencioglu, S.; Altay, M.; Guzel, S.; Celebi, A.; Ekizoglu, I.; Ayar, Y. Is There a Relation between Serum Vitamin D Level and Microvascular Comlications in Type 2 Diabetes. Eurasian J. Med. Oncol. 2017, 1, 190–196. [Google Scholar] [CrossRef]
- Bajaj, S.; Singh, R.P.; Dwivedi, N.C.; Singh, K.; Gupta, A.; Mathur, M. Vitamin D Levels and Microvascular Complications in Type 2 Diabetes. Indian J. Endocrinol. Metab. 2014, 18, 537–541. [Google Scholar] [CrossRef]
- Zhao, J.Y.; Dong, J.J.; Wang, H.P.; Shang, H.X.; Zhang, D.M.; Liao, L. Efficacy and Safety of Vitamin D3 in Patients with Diabetic Nephropathy: A Meta-Analysis of Randomized Controlled Trials. Chin. Med. J. 2014, 127, 2837–2843. [Google Scholar] [PubMed]
- Derakhshanian, H.; Shab-Bidar, S.; Speakman, J.R.; Nadimi, H.; Djafarian, K. Vitamin D and Diabetic Nephropathy: A Systematic Review and Meta-Analysis. Nutrition 2015, 31, 1189–1194. [Google Scholar] [CrossRef]
- Shehab, D.; Al-Jarallah, K.; Mojiminiyi, O.A.; Al Mohamedy, H.; Abdella, N.A. Does Vitamin D Deficiency Play a Role in Peripheral Neuropathy in Type 2 Diabetes? Diabet. Med. 2012, 29, 43–49. [Google Scholar] [CrossRef]
- Yammine, K.; Hayek, F.; Assi, C. Is There an Association between Vitamin D and Diabetic Foot Disease? A Meta-Analysis. Wound Repair Regen. 2020, 28, 90–96. [Google Scholar] [CrossRef]
- Fahed, G.; Aoun, L.; Zerdan, M.B.; Allam, S.; Zerdan, M.B.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; García-Recio, E.; De Luna-Bertos, E.; Ruiz, C.; Illescas-Montes, R. Role of Vitamin d in the Metabolic Syndrome. Nutrients 2021, 13, 830. [Google Scholar] [CrossRef]
- Faraji, S.; Alizadeh, M. Mechanistic Effects of Vitamin D Supplementation on Metabolic Syndrome Components in Patients with or without Vitamin D Deficiency. J. Obes. Metab. Syndr. 2021, 29, 270–280. [Google Scholar] [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Pichiah, P.B.T.; Cha, Y.S. Vitamin D and Metabolic Diseases: Growing Roles of Vitamin D. J. Obes. Metab. Syndr. 2018, 27, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front. Endocrinol. 2019, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.E.; Kong, J.; Zhang, W.; Szeto, F.L.; Ye, H.; Deb, D.K.; Brady, M.J.; Li, Y.C. Targeted Expression of Human Vitamin D Receptor in Adipocytes Decreases Energy Expenditure and Induces Obesity in Mice. J. Biol. Chem. 2011, 286, 33804–33810. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, S.; Jeppesen, P.B. Body Mass Index, Vitamin d, and Type 2 Diabetes: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1182. [Google Scholar] [CrossRef]
- Ullah, M.I.; Uwaifo, G.I.; Nicholas, W.C.; Koch, C.A. Does Vitamin D Deficiency Cause Hypertension? Current Evidence from Clinical Studies and Potential Mechanisms. Int. J. Endocrinol. 2010, 2010, 579640. [Google Scholar] [CrossRef]
- Rafiq, S.; Jeppesen, P.B. Vitamin D Deficiency Is Inversely Associated with Homeostatic Model Assessment of Insulin Resistance. Nutrients 2021, 13, 4358. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Vatanparast, H.; Mazidi, M.; Kimball, S.M. Vitamin D Supplementation, Glycemic Control, and Insulin Resistance in Prediabetics: A Meta-Analysis. J. Endocr. Soc. 2018, 2, 687–709. [Google Scholar] [CrossRef]
- Wrzosek, M.; Lukaszkiewicz, J.; Wrzosek, M.; Jakubczyk, A.; Matsumoto, H.; Piatkiewicz, P.; Radziwon-Zaleska, M.; Wojnar, M.; Nowicka, G. Vitamin D and the Central Nervous System. Pharmacol. Rep. 2013, 65, 271–278. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D Deficiency 2.0: An Update on the Current Status Worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- van de Peppel, J.; van Leeuwen, J.P.T.M. Vitamin D and Gene Networks in Human Osteoblasts. Front. Physiol. 2014, 5, 137. [Google Scholar] [CrossRef] [PubMed]
- Kocak, M.Z.; Aktas, G.; Atak, B.; Bilgin, S.; Kurtkulagi, O.; Duman, T.T.; Ozcil, I.E. The Association between Vitamin D Levels and Handgrip Strength in Elderly Men. Acta Endocrinol. 2020, 16, 263–266. [Google Scholar] [CrossRef]
- Zhang, J.-L.; Poon, C.C.-W.; Wong, M.-S.; Li, W.-X.; Guo, Y.-X.; Zhang, Y. Vitamin D Supplementation Improves Handgrip Strength in Postmenopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2022, 13, 863448. [Google Scholar] [CrossRef]
- Thapa, S.; Pyakurel, P.; Baral, D.D.; Jha, N. Health-Related Quality of Life among People Living with Type 2 Diabetes: A Community Based Cross-Sectional Study in Rural Nepal. BMC Public Health 2019, 19, 1171. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Study Location | Study Design | Sample Size | Findings | End Outcome |
|---|---|---|---|---|---|
| Darraj et al., 2022 [30] | Saudi Arabia | Cross-sectional | 380 patients of T2DM | Vitamin D deficiency is highly prevalent in people with T2DM and is associated with poor glycaemic control. | Glycaemic control |
| Tang et al., 2022 [31] | China | Case–control study | 1721 T2DM patients | A low serum vitamin D level was significantly associated with a higher prevalence of diabetic foot ulcer (DFU) among Chinese patients with T2DM. | Diabetic foot ulcer |
| Wang et al., 2022 [32] | China | Case–control study | 429 T2DM patients | The study confirms that 25-OH-vitamin D is closely correlated with DFU. | Diabetic foot ulcer |
| Geng et al., 2022 [33] | United Kingdom | Cohort | 13,486 individuals (>60 years) with T2DM | Lower serum levels of 25(OH)D were significantly associated with a higher risk of all-cause dementia, Alzheimer’s disease, and vascular dementia. | Cognitive impairment |
| Bhat et al., 2021 [34] | India | Case–control study | 108 cases of T2DM and 101 healthy controls | There is an inverse association between vitamin D and glycaemic control in T2DM patients. | Glycaemic control |
| Salih et al., 2021 [35] | Iraq | Case–control | Total number of 310 participants were included, 155 with T2DM and 155 patients without T2DM | The serum 25(OH)D levels were significantly lower in patients with poor glycaemic control compared to those with adequate glycaemic control and in individuals with diabetes duration of more than 5 years. | Glycaemic control |
| Assy et al., 2021 [36] | Egypt | Case–control | 80 T2DM patients | There is an inverse relationship between vitamin D levels and neuropathy scores. | Diabetic neuropathy |
| Mendoza et al., 2021 [37] | Mexico | Cross-sectional study | A total of 116 women ≥ 60 years old with T2DM | The findings showed a relationship between a low circulating level of vitamin D and a decrease in handgrip strength. | Decrease in handgrip strength |
| Aghamohammadzadeh et al., 2020 [38] | Iran | Case–control | 80 overweight/obese subjects with T2DM, and 77 healthy subjects | There was an inverse association between serum concentrations of 25-hydroxyvitamin D and diastolic blood pressure and the physical health subscale of quality of life in individuals with T2DM. | Blood pressure, quality of life (physical health subscale) |
| Xiao et al., 2020 [39] | China | Cross-sectional | 4284 Chinese patients with T2DM | The present study firstly indicated that VDD was significantly associated with a higher prevalence of DFU among Chinese T2DM patients. | Diabetic foot ulcer |
| Dai et al., 2020 [40] | China | Case–control | 51 patients of T2DM | Low serum 25-OH-vitamin D level was associated with DFU in T2DM patients. | Diabetic foot ulcer |
| Ahmed et al., 2020 [41] | Qatar | Cohort study | 496 Qatari subjects, 274 with and 222 without T2DM participated in the study | Vitamin D2 was related to hypertension and dyslipidaemia, while vitamin D3 was associated with diabetic retinopathy. | Hypertension, dyslipidaemia, diabetic retinopathy |
| Samefors et al., 2020 [42] | Sweden | Cohort study | Data of 761 patients aged 55–66 years | The study found an inverse association between 25(OH)D3 and mental health in patients with T2DM at baseline. | Mental health |
| Liu et al., 2020 [43] | China | Cross-sectional study | 128 adult males with T2DM | There was a significant relationship between vitamin D level and visceral fat accumulation in males with T2DM. | Increase in visceral fat accumulation in males |
| Yang et al., 2019 [44] | China | Case–control | 590 T2DM patients | A low serum 25(OH)D concentration is an independent risk factor for lower extremity vascular pathological changes and acts as a prognostic index for lower extremity atherosclerotic disease in T2DM patients. | Lower extremity atherosclerotic disease |
| Parveen et al., 2019 [45] | India | Case–control study | Total of 88 T2DM | Serum 25(OH)D was significantly associated with cognitive impairment in T2DM patients. | Cognitive impairment |
| Yuan et al., 2019 [46] | China | Cross-sectional | 1018 T2DM patients | In T2DM patients, lower serum vitamin D levels were associated with an increased risk of peripheral arterial disease. | Peripheral arterial disease |
| Xie et al., 2019 [47] | China | Cross-sectional study | 351 patients with T2DM | Vitamin D insufficiency or deficiency was independently associated with diabetic kidney disease in T2DM. | Diabetic kidney disease |
| Karau et al., 2019 [48] | Kenya | Cross-sectional study | 156 T2DM patients | This study found a significant inverse correlation between vitamin D and glycaemic control and body mass index. | Glycaemic control, body mass index |
| Alcubierre et al., 2018 [49] | Spain | Cross-sectional | A total of 292 T2DM patients | The study shows the association between vitamin D deficiency and diabetes-specific quality of life in patients with T2DM. | Quality of life |
| Wang et al., 2017 [50] | China | Cross-sectional study | 2786 patients with T2DM recruited from a Chinese diabetes registry. | A significant negative association between serum levels of 25 (OH)D and depression in Chinese patients with T2DM. | Mental health |
| Saif et al., 2017 [51] | Egypt | Case–control | 30 male patients with T2DM and 20 healthy controls | There was a significant inverse relationship between serum vitamin D levels and HbA1c in T2DM patients. | Glycaemic control |
| Guo et al., 2017 [52] | China | Case–control | 368 T2DM, and 300 non-diabetic control subjects | The findings showed a positive correlation between the 25(OH)D level and the bone mass density in T2DM patients. | Bone mineral density |
| Ding et al., 2017 [53] | China | Cross-sectional | 210 T2DM patients | Low serum 25(OH)D concentration was significantly associated with carotid atherosclerotic plaque in T2DM. | Carotid atherosclerotic plaque |
| Raelene et al., 2017 [54] | United States | Cross-sectional | 50 individuals with T2DM | The findings showed that 25(OH)D insufficiency is associated with reduced parasympathetic nerve function, particularly in younger persons with T2DM. | Reduced parasympathetic nerve function |
| Pan et al., 2016 [55] | China | Cross-sectional | 270 T2DM patients aged more than 50 years old | Vitamin D deficiency is associated with related metabolic syndrome among T2DM over 50 years old. | Metabolic syndrome |
| Mori et al., 2015 [56] | Japan | Cross-sectional | 170 postmenopausal women with T2DM | There was a significant positive correlation between 25(OH)D and the radial bone mineral density. | Radial bone mineral density |
| Zoppini et al., 2015 [57] | Italy | Cross-sectional | 715 outpatients with T2DM | Among patients with T2DM, lower levels of 25-hydroxyvitamin D are associated with a higher prevalence of microvascular complications (retinopathy and/or nephropathy). | Microvascular complications (retinopathy and/or nephropathy) |
| Kajbaf et al., 2014 [58] | France | Cross-sectional | 542 medical records of patients with T2DM | There is an association between vitamin D and HbA1c. | Glycaemic control |
| Tiwari et al., 2013 [59] | India | Case–control | 125 T2DM patients and 164 control patients | Severe vitamin D deficiency (<25 nmol/L) is a risk factor for diabetic foot infections. | Diabetic foot infection |
| Gandhe et al., 2013 [60] | India | Case–control | 30 T2DM subjects with 30 healthy controls. | There is a significant inverse association between vitamin D status and insulin levels in T2DM patients. | Insulin resistant |
| Kostoglou Athanassiou et al., 2013 [61] | Greece | Case–control | 120 T2DM and 120 controls | Vitamin D levels appeared to be lower in T2DM patients compared to the control group, with vitamin D levels associated with glycaemic control in T2DM patients. | Glycaemic control |
| Payne et al., 2012 [62] | United States | Cross-sectional study | A total of 221 patients. | Vitamin D may play a role in the pathogenesis of diabetic retinopathy. | Diabetic retinopathy |
| Outcome of Vitamin D Deficiency among T2DM Patients | Studies | |
|---|---|---|
| Mental health | Mental health well-being | [42,50] |
| Cognitive impairment | [33,45] | |
| Microvascular complications | Diabetes retinopathy | [41,57,62,63,64] |
| Diabetic neuropathy | [36,57] | |
| Diabetic nephropathy | [47] | |
| Diabetic foot ulcer | [31,32,39,40,59] | |
| Macrovascular complications | Carotid arterial plaque | [53] |
| Peripheral arterial disease | [44,46] | |
| Metabolic syndrome | Metabolic syndrome | [55] |
| Risk of obesity | Increased body mass index | [48] |
| Visceral fat accumulation | [43] | |
| Blood pressure | Hypertension | [41] |
| Increased diastolic pressure | [38] | |
| Dyslipidaemia | Dyslipidaemia | [41] |
| Glycaemic control | Poor glycaemic control | [30,34,35,48,51,58,61] |
| Insulin resistant | [60,65] | |
| Nerve related | Reduced parasympathetic nerve | [54] |
| Musculoskeletal related | Bone mineral density | [52,56] |
| Decreased handgrip | [37] | |
| Quality of life | Reduced quality of life | [38,49] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Md Isa, Z.; Amsah, N.; Ahmad, N. The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review. Nutrients 2023, 15, 2310. https://doi.org/10.3390/nu15102310
Md Isa Z, Amsah N, Ahmad N. The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review. Nutrients. 2023; 15(10):2310. https://doi.org/10.3390/nu15102310
Chicago/Turabian StyleMd Isa, Zaleha, Norizzati Amsah, and Norfazilah Ahmad. 2023. "The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review" Nutrients 15, no. 10: 2310. https://doi.org/10.3390/nu15102310
APA StyleMd Isa, Z., Amsah, N., & Ahmad, N. (2023). The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review. Nutrients, 15(10), 2310. https://doi.org/10.3390/nu15102310