
The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Search
2.2. Study Selection and Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
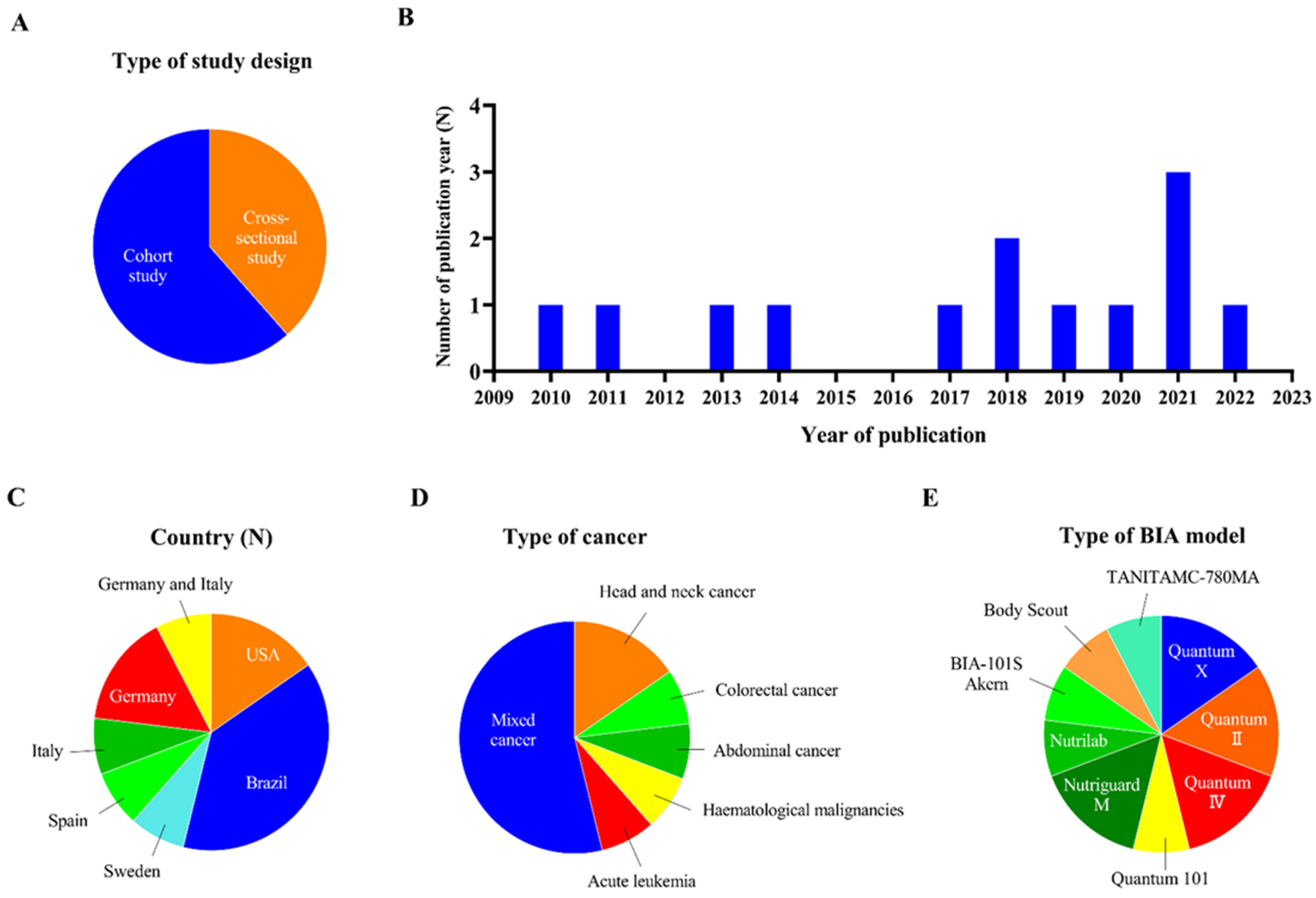
3.1. Study Selection and Description of Studies
3.2. Quality Assessment
3.3. Relationship between SPA and Nutrition Status
3.4. Relationship between SPA and Clinical Outcomes
3.4.1. Relationship between SPA and Complications
3.4.2. Relationship between SPA and Survival
3.5. Comparison of the Predictive Ability of SPA and PA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Rimer, B.K.; Winer, E.P. Weight gain in women diagnosed with breast cancer. J. Am. Diet Assoc. 1997, 97, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Galvão, D.A.; Spry, N.A.; Taaffe, D.R.; Newton, R.U.; Stanley, J.; Shannon, T.; Rowling, C.; Prince, R. Changes in muscle, fat and bone mass after 36 weeks of maximal androgen blockade for prostate cancer. BJU Int. 2008, 102, 44–47. [Google Scholar] [CrossRef]
- Hardee, J.P.; Counts, B.R.; Carson, J.A. Understanding the Role of Exercise in Cancer Cachexia Therapy. Am. J. Lifestyle Med. 2017, 13, 46–60. [Google Scholar] [CrossRef]
- Thomson, Z.O.; Reeves, M.M. Can weight gain be prevented in women receiving treatment for breast cancer? A systematic review of intervention studies. Obes. Rev. 2017, 18, 1364–1373. [Google Scholar] [CrossRef]
- Deluche, E.; Leobon, S.; Desport, J.C.; Venat-Bouvet, L.; Usseglio, J.; Tubiana-Mathieu, N. Impact of body composition on outcome in patients with early breast cancer. Support Care Cancer 2018, 26, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Smith, M.R. Changes in fat and lean body mass during androgen-deprivation therapy for prostate cancer. Urology 2004, 63, 742–745. [Google Scholar] [CrossRef]
- Ebadi, M.; Mazurak, V.C. Evidence and mechanisms of fat depletion in cancer. Nutrients 2014, 6, 5280–5297. [Google Scholar] [CrossRef]
- Gangadharan, A.; Choi, S.E.; Hassan, A.; Ayoub, N.M.; Durante, G.; Balwani, S.; Kim, Y.H.; Pecora, A.; Goy, A.; Suh, K.S. Protein calorie malnutrition, nutritional intervention and personalized cancer care. Oncotarget 2017, 8, 24009–24030. [Google Scholar] [CrossRef]
- Aktas, A.; Walsh, D.; Galang, M.; O′Donoghue, N.; Rybicki, L.; Hullihen, B.; Schleckman, E. Underrecognition of Malnutrition in Advanced Cancer: The Role of the Dietitian and Clinical Practice Variations. Am. J. Hosp. Palliat. Care 2017, 34, 547–555. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Pena, N.F.; Mauricio, S.F.; Rodrigues, A.M.S.; Carmo, A.S.; Coury, N.C.; Correia, M.I.T.D.; Generoso, S.V. Association Between Standardized Phase Angle, Nutrition Status, and Clinical Outcomes in Surgical Cancer Patients. Nutr. Clin. Pract. 2019, 34, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Lee, Y.J.; Yang, J.H.; Kim, C.M.; Choi, W.S. The Association between Phase Angle of Bioelectrical Impedance Analysis and Survival Time in Advanced Cancer Patients: Preliminary Study. Korean J. Fam. Med. 2014, 35, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Ehresman, J.; Ahmed, A.K.; Schilling, A.; Pennington, Z.; Lubelski, D.; Cottrill, E.; Goodwin, M.L.; Liddy, A.; Abu-Bonsrah, N.; Goodwin, C.R.; et al. Preoperative Nutrition Consults Associated with Decreased Postoperative Complication Rate and Decreased Length of Hospital Stay After Spine Metastasis Surgery. World Neurosurg. 2020, 133, e173–e179. [Google Scholar] [CrossRef]
- Longo, C.J.; Fitch, M.I.; Loree, J.M.; Carlson, L.E.; Turner, D.; Cheung, W.Y.; Gopaul, D.; Ellis, J.; Ringash, J.; Mathews, M.; et al. Patient and family financial burden associated with cancer treatment in Canada: A national study. Support Care Cancer 2021, 29, 3377–3386. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhang, L.; Fu, Y.; Wang, M.; Zhang, L. Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1327. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Ozorio, G.A.; Barão, K.; Forones, N.M. Cachexia Stage, Patient-Generated Subjective Global Assessment, Phase Angle, and Handgrip Strength in Patients with Gastrointestinal Cancer. Nutr. Cancer 2017, 69, 772–779. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Lammersfeld, C.A. Bioelectrical impedance phase angle as a prognostic indicator in advanced pancreatic cancer. Br. J. Nutr. 2004, 92, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cruz, P.E.; Dos Santos, R.; Silva, T.B.; Crovador, C.S.; Nascimento, M.S.; Hall, S.; Fajardo, J.; Bruera, E.; Hui, D. Longitudinal temporal and probabilistic prediction of survival in a cohort of patients with advanced cancer. J. Pain Symptom Manage. 2014, 48, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.; Barros, A.J.; Post, C.L.; Waitzberg, D.L.; Heymsfield, S.B. Can bioelectrical impedance analysis identify malnutrition in preoperative nutrition assessment? Nutrition. 2003, 19, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Price, K.L.; Earthman, C.P. Update on body composition tools in clinical settings: Computed tomography, ultrasound, and bioimpedance applications for assessment and monitoring. Eur. J. Clin. Nutr. 2019, 73, 187–193. [Google Scholar] [CrossRef] [PubMed]
- do Amaral Paes, T.C.; de Oliveira, K.C.C.; de Carvalho Padilha, P.; Peres, W.A.F. Phase angle assessment in critically ill cancer patients: Relationship with the nutritional status, prognostic factors and death. J. Crit. Care 2018, 44, 430–435. [Google Scholar] [CrossRef]
- Visser, M.; van Venrooij, L.M.; Wanders, D.C.; de Vos, R.; Wisselink, W.; van Leeuwen, P.A.; de Mol, B.A. The bioelectrical impedance phase angle as an indicator of undernutrition and adverse clinical outcome in cardiac surgical patients. Clin. Nutr. 2012, 31, 981–986. [Google Scholar] [CrossRef]
- Mullie, L.; Obrand, A.; Bendayan, M.; Trnkus, A.; Ouimet, M.C.; Moss, E.; Chen-Tournoux, A.; Rudski, L.G.; Afilalo, J. Phase Angle as a Biomarker for Frailty and Postoperative Mortality: The BICS Study. J. Am. Heart Assoc. 2018, 7, e008721. [Google Scholar] [CrossRef]
- Zhou, S.; Yu, Z.; Shi, X.; Zhao, H.; Dai, M.; Chen, W. The Relationship between Phase Angle, Nutrition Status, and Complications in Patients with Pancreatic Head Cancer. Int. J. Environ. Res. Public Health 2022, 19, 6426. [Google Scholar] [CrossRef]
- Sat-Muñoz, D.; Martínez-Herrera, B.E.; González-Rodríguez, J.A.; Gutiérrez-Rodríguez, L.X.; Trujillo-Hernández, B.; Quiroga-Morales, L.A.; Alcaráz-Wong, A.A.; Dávalos-Cobián, C.; Solórzano-Meléndez, A.; Flores-Carlos, J.D.; et al. Phase Angle, a Cornerstone of Outcome in Head and Neck Cancer. Nutrients 2022, 14, 3030. [Google Scholar] [CrossRef]
- Uccella, S.; Mele, M.C.; Quagliozzi, L.; Rinninella, E.; Nero, C.; Cappuccio, S.; Cintoni, M.; Gasbarrini, A.; Scambia, G.; Fagotti, A. Assessment of preoperative nutritional status using BIA-derived phase angle (PhA) in patients with advanced ovarian cancer: Correlation with the extent of cytoreduction and complications. Gynecol. Oncol. 2018, 149, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Władysiuk, M.S.; Mlak, R.; Morshed, K.; Surtel, W.; Brzozowska, A.; Małecka-Massalska, T. Bioelectrical impedance phase angle as a prognostic indicator of survival in head-and-neck cancer. Curr. Oncol. 2016, 23, e481–e487. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: Phase angle and impedance ratio. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobäus, N.; Zocher, D.; Bosy-Westphal, A.; Szramek, A.; Scheufele, R.; Smoliner, C.; Pirlich, M. Cutoff percentiles of bioelectrical phase angle predict functionality, quality of life, and mortality in patients with cancer. Am. J. Clin. Nutr. 2010, 92, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Matthews, L.; Bates, A.; Wootton, S.A.; Levett, D. The use of bioelectrical impedance analysis to predict post-operative complications in adult patients having surgery for cancer: A systematic review. Clin. Nutr. 2021, 40, 2914–2922. [Google Scholar] [CrossRef] [PubMed]
- Sukackiene, D.; Rimsevicius, L.; Miglinas, M. Standardized Phase Angle for Predicting Nutritional Status of Hemodialysis Patients in the Early Period After Deceased Donor Kidney Transplantation. Front. Nutr. 2022, 9, 803002. [Google Scholar] [CrossRef]
- Genton, L.; Norman, K.; Spoerri, A.; Pichard, C.; Karsegard, V.L.; Herrmann, F.R.; Graf, C.E. Bioimpedance-Derived Phase Angle and Mortality Among Older People. Rejuvenation Res. 2017, 20, 118–124. [Google Scholar] [CrossRef]
- Jansen, A.K.; Gattermann, T.; da Silva Fink, J.; Saldanha, M.F.; Dias Nascimento Rocha, C.; de Souza Moreira, T.H.; Silva, F.M. Low standardized phase angle predicts prolonged hospitalization in critically ill patients. Clin. Nutr. ESPEN 2019, 34, 68–72. [Google Scholar] [CrossRef]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2021, 41, 3106–3114. [Google Scholar] [CrossRef]
- Roccamatisi, L.; Gianotti, L.; Paiella, S.; Casciani, F.; De Pastena, M.; Caccialanza, R.; Bassi, C.; Sandini, M. Preoperative standardized phase angle at bioimpedance vector analysis predicts the outbreak of antimicrobial-resistant infections after major abdominal oncologic surgery: A prospective trial. Nutrition 2021, 86, 111184. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, 160. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Hong, Q.N. Combining the power of stories and the power of numbers: Mixed methods research and mixed studies reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Paiva, S.I.; Borges, L.R.; Halpern-Silveira, D.; Assunção, M.C.; Barros, A.J.; Gonzalez, M.C. Standardized phase angle from bioelectrical impedance analysis as prognostic factor for survival in patients with cancer. Support Care Cancer 2010, 19, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, L.; Silander, E.; Bosaeus, I.; Hammerlid, E. Bioelectrical phase angle at diagnosis as a prognostic factor for survival in advanced head and neck cancer. Eur. Arch. Otorhinolaryngol. 2018, 275, 2379–2386. [Google Scholar] [CrossRef]
- Hui, D.; Bansal, S.; Morgado, M.; Dev, R.; Chisholm, G.; Bruera, E. Phase angle for prognostication of survival in patients with advanced cancer: Preliminary findings. Cancer 2014, 120, 2207–2214. [Google Scholar] [CrossRef]
- Yates, S.J.; Lyerly, S.; Manuel, M.; Tooze, J.A.; Klepin, H.D.; Powell, B.L.; Dralle, S.; Uprety, A.; Pardee, T.S. The prognostic value of standardized phase angle in adults with acute leukemia: A prospective study. Cancer Med. 2020, 9, 2403–2413. [Google Scholar] [CrossRef]
- Paixão, E.M.S.; Gonzalez, M.C.; Nakano, E.Y.; Ito, M.K.; Pizato, N. Weight loss, phase angle, and survival in cancer patients undergoing radiotherapy: A prospective study with 10-year follow-up. Eur. J. Clin. Nutr. 2021, 75, 823–828. [Google Scholar] [CrossRef]
- Urbain, P.; Birlinger, J.; Ihorst, G.; Biesalski, H.K.; Finke, J.; Bertz, H. Body mass index and bioelectrical impedance phase angle as potentially modifiable nutritional markers are independent risk factors for outcome in allogeneic hematopoietic cell transplantation. Ann. Hematol. 2013, 92, 111–119. [Google Scholar] [CrossRef]
- Maurício, S.F.; Xiao, J.; Prado, C.M.; Gonzalez, M.C.; Correia, M.I.T.D. Different nutritional assessment tools as predictors of postoperative complications in patients undergoing colorectal cancer resection. Clin. Nutr. 2018, 37, 1505–1511. [Google Scholar] [CrossRef]
- León-Idougourram, S.; Pérez-Gómez, J.M.; Muñoz Jiménez, C.; L-López, F.; Manzano García, G.; Molina Puertas, M.J.; Herman-Sánchez, N.; Alonso-Echague, R.; Calañas Continente, A.; Gálvez Moreno, M.Á.; et al. Morphofunctional and Molecular Assessment of Nutritional Status in Head and Neck Cancer Patients Undergoing Systemic Treatment: Role of Inflammasome in Clinical Nutrition. Cancers 2022, 14, 494. [Google Scholar] [CrossRef]
- Härter, J.; Orlandi, S.P.; Gonzalez, M.C. Nutritional and functional factors as prognostic of surgical cancer patients. Support Care Cancer 2017, 25, 2525–2530. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Caraccia, M.; Klersy, C.; Cappello, S.; Turri, A.; Borioli, V.; Stobäus, N.; Giannoni, A.; Arcaini, L.; Benazzo, M.; et al. Validation of a new prognostic body composition parameter in cancer patients. Clin. Nutr. 2021, 40, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Abd Aziz, N.A.S.; Teng, N.I.M.F.; Abdul Hamid, M.R.; Ismail, N.H. Assessing the nutritional status of hospitalized elderly. Clin. Interv. Aging 2017, 12, 1615–1625. [Google Scholar] [CrossRef] [PubMed]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M.; Academy Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J. Parenter. Enteral. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. JPEN J. Parenter. Enteral. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef]
- Yasui-Yamada, S.; Oiwa, Y.; Saito, Y.; Aotani, N.; Matsubara, A.; Matsuura, S.; Tanimura, M.; Tani-Suzuki, Y.; Kashihara, H.; Nishi, M.; et al. Impact of phase angle on postoperative prognosis in patients with gastrointestinal and hepatobiliary-pancreatic cancer. Nutrition 2020, 79–80, 110891. [Google Scholar] [CrossRef]
- Małecka-Massalska, T.; Mlak, R.; Smolen, A.; Morshed, K. Bioelectrical impedance phase angle and subjective global assessment in detecting malnutrition among newly diagnosed head and neck cancer patients. Eur. Arch. Otorhinolaryngol. 2016, 273, 1299–1305. [Google Scholar] [CrossRef]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical impedance phase angle in clinical practice: Implications for prognosis in advanced colorectal cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef]
- de Almeida, C.; Penna, P.M.; Pereira, S.S.; Rosa, C.O.B.; Franceschini, S.D.C.C. Relationship between Phase Angle and Objective and Subjective Indicators of Nutritional Status in Cancer Patients: A Systematic Review. Nutr. Cancer 2021, 73, 2201–2210. [Google Scholar] [CrossRef]
- Pereira, M.M.E.; Queiroz, M.D.S.C.; de Albuquerque, N.M.C.; Rodrigues, J.; Wiegert, E.V.M.; Calixto-Lima, L.; de Oliveira, L.C. The Prognostic Role of Phase Angle in Advanced Cancer Patients: A Systematic Review. Nutr. Clin. Pract. 2018, 33, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Cardinal, T.R.; Wazlawik, E.; Bastos, J.L.; Nakazora, L.M.; Scheunemann, L. Standardized phase angle indicates nutritional status in hospitalized preoperative patients. Nutr. Res. 2010, 30, 594–600. [Google Scholar] [CrossRef] [PubMed]
- De Groot, L.M.; Lee, G.; Ackerie, A.; van der Meij, B.S. Malnutrition Screening and Assessment in the Cancer Care Ambulatory Setting: Mortality Predictability and Validity of the Patient-Generated Subjective Global Assessment Short form (PG-SGA SF) and the GLIM Criteria. Nutrients 2020, 12, 2287. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Pereira, S.L.; Luo, M.; Matheson, E.M. Evaluation of Blood Biomarkers Associated with Risk of Malnutrition in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 829. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Pugliese, G.; Laudisio, D.; de Alteriis, G.; Graziadio, C.; Colao, A.; Savastano, S. Phase Angle as an Easy Diagnostic Tool of Meta-Inflammation for the Nutritionist. Nutrients 2021, 13, 1446. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Bossola, M.; Bellantone, R.; Rossi Fanelli, F. Therapy of muscle wasting in cancer: What is the future? Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 459–466. [Google Scholar] [CrossRef]
- Pérez Camargo, D.A.; Allende Pérez, S.R.; Verastegui Avilés, E.; Rivera Franco, M.M.; Meneses García, A.; Herrera Gómez, Á.; Urbalejo Ceniceros, V.I. Assessment and Impact of Phase Angle and Sarcopenia in Palliative Cancer Patients. Nutr. Cancer 2017, 69, 1227–1233. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C.; Barros, A.J. Bioelectrical impedance analysis in clinical practice: A new perspective on its use beyond body composition equations. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 311–317. [Google Scholar] [CrossRef]
- Toso, S.; Piccoli, A.; Gusella, M.; Menon, D.; Bononi, A.; Crepaldi, G.; Ferrazzi, E. Altered tissue electric properties in lung cancer patients as detected by bioelectric impedance vector analysis. Nutrition 2000, 16, 120–124. [Google Scholar] [CrossRef]
- Grundmann, O.; Yoon, S.L.; Williams, J.J. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients--a comprehensive review. Eur. J. Clin. Nutr. 2015, 69, 1290–1297. [Google Scholar] [CrossRef]
- Boroughs, L.K.; DeBerardinis, R.J. Metabolic pathways promoting cancer cell survival and growth. Nat. Cell Biol. 2015, 17, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Arab, A.; Karimi, E.; Vingrys, K.; Shirani, F. Is phase angle a valuable prognostic tool in cancer patients′ survival? A systematic review and meta-analysis of available literature. Clin. Nutr. 2021, 40, 3182–3190. [Google Scholar] [CrossRef] [PubMed]
- Grunicke, H.H. The cell membrane as a target for cancer chemotherapy. Eur. J. Cancer 1991, 27, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lu, Y.; Qin, Z.; Guo, H.; Chen, W.; Ding, T.; Tang, J.; Zhang, H. Stereotactic Body Radiotherapy and Conventional Radiotherapy Induce Cytoskeleton Extension and Enlargement of Cell Morphology in Non-Small Cell Lung Cancer. Dose-Response 2021, 19, 15593258211064499. [Google Scholar] [CrossRef]
- Mattiello, R.; Amaral, M.A.; Mundstock, E.; Ziegelmann, P.K. Reference values for the phase angle of the electrical bioimpedance: Systematic review and meta-analysis involving more than 250,000 subjects. Clin. Nutr. 2020, 39, 1411–1417. [Google Scholar] [CrossRef]
- Genton, L.; Herrmann, F.R.; Spörri, A.; Graf, C.E. Association of mortality and phase angle measured by different bioelectrical impedance analysis (BIA) devices. Clin. Nutr. 2018, 37, 1066–1069. [Google Scholar] [CrossRef]
- Nescolarde, L.; Lukaski, H.; De Lorenzo, A.; de-Mateo-Silleras, B.; Redondo-Del-Río, M.P.; Camina-Martín, M.A. Different displacement of bioimpedance vector due to Ag/AgCl electrode effect. Eur. J. Clin. Nutr. 2016, 70, 1401–1407. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Step | Search Strategy |
|---|---|
| #1 | “Phase Angle” OR “Standardized Phase Angle” |
| #2 | Neoplasms OR Neoplasia OR Neoplasias OR Neoplasm OR Tumors OR Tumor OR Cancer OR Cancers OR Malignancy OR Malignancies OR “Malignant Neoplasms” OR “Malignant Neoplasm” OR “Neoplasm, Malignant” OR “Neoplasms, Malignant” OR “Benign Neoplasms” OR “Neoplasms, Benign” OR “Benign Neoplasm” OR “Neoplasm, Benign” |
| #3 | #1 AND #2 |
| First Author/ Year | Country | Cancer Location/ Sample Size | Gender [Male(%)] | Age (Years) | BMI [Kg/m2(%)] | Treatment Methods |
|---|---|---|---|---|---|---|
| Pena, 2019 [13] | Brazil | Mixed, 121 | 52.9% | 58.8 ± 12.5 | / 3 | Surgical |
| Axelsson, 2018 [45] | Sweden | HNC 2, 128 | 68% | 61.4 ± 11.2 | 24.9 ± 3.8 | Surgery, chemoradiation |
| Hui, 2014 [46] | USA | Mixed, 222 | 41% | 55 | / 3 | Parenteral hydration |
| Yates, 2020 [47] | USA | AL 1, 100 | 44% | 59 ± 14.6 | 29.7 ± 7.1 | Intensive induction chemotherapy |
| Paiva, 2011 [44] | Brazil | Mixed, 195 | 38% | 58 ± 12.9 | 26.5 ± 5.1 | First chemotherapy |
| Paixao, 2021 [48] | Brazil | Mixed, 62 | 39% | 54.5 | 25.3 | Radiotherapy |
| Urbain, 2013 [49] | Germany | Haematological Malignancies, 105 | 62.9% | 56.1 ± 10.9 | 25.9 ± 4.1 | Allogeneic hematopoietic cell transplantation |
| Norman, 2010 [34] | Germany | Mixed, 399 | 52.1% | 63.0 ± 11.8 | 24.9 ± 4.8 | / 3 |
| Maurício, 2018 [50] | Brazil | Colorectal, 84 | 46.4% | 61.6 ± 13.1 | / 3 | Surgery, neoadjuvant |
| Leon-Idougourram, 2022 [51] | Spain | HNC 2, 45 | 37.8% | 64.5 | / 3 | Surgery, radiotherapy, chemotherapy |
| Harter, 2017 [52] | Brazil | Mixed, 60 | 56.7% | 18–39 (18.3), 40–59 (36.7), ≥ 60 (45) | <18.5 (1.7), 18.5–24.9 (30), 25–29.9 (43.3), ≥30 (25) | Elective surgery |
| Roccamatisi, 2021 [40] | Italy | Abdominal, 182 | 57.7% | 67 ± 11 | 24.9 ± 4.2 | Scheduled to undergo surgical |
| Cereda, 2021 [53] | Italy, Germany | Mixed, 1084 | 61.7% 54.8% | 64.8 ± 11.6 61.7 ± 12.2 | 23.3 ± 4.4 24.4 ± 4.1 | / 3 |
| First Author/ Year | Model of BIA 1 | Time of Assessment | Time of Follow-Up | Cut-Off Value of PA | Cut-Off Value of SPA 2 | Reference Population | Study Design |
|---|---|---|---|---|---|---|---|
| Pena, 2019 [13] | Quantum X; RJL Systems, Clinton, MI | 1 day before surgery | From 1 day after surgery to discharge or death | / 3 | −1.65° | Brazilian | Cohort |
| Axelsson, 2018 [45] | BIA-101S Akern; RJL Systems, Detroit, MI, USA | Time of diagnosis | As long as possible | 5.95° | −1.65° | German | Cross- sectional |
| Hui, 2014 [46] | Quantum IV; RJL Systems, Clinton Township, Mich | Time of admission | Median: 118 days | 4.4° | 5th | / 3 | Cross- sectional |
| Yates, 2020 [47] | Quantum IV; RJL Systems | Time of diagnosis | 60 days | / 3 | −0.948° | / 3 | Cross- sectional |
| Paiva, 2011 [44] | Quantum 101; RJL Systems | Before first chemotherapy | 3 years and 2 months | / 3 | −1.65° | Brazilian | Cross- sectional |
| Paixao, 2021 [48] | Quantum II; RJL Systems | Before first RT | 10 years | / 3 | −1.65° | / 3 | Cross- sectional |
| Urbain, 2013 [49] | Body Scout, Fresenius Medical Care, Germany | / 3 | 2 years | 5.06° | 25th: −2.26° | German | Cohort |
| Norman, 2010 [34] | Nutriguard M; Data Input GmbH, Darmstadt, Germany | Within 48 h of admission | 6 months | 5th | 5th | / 3 | Cohort |
| Maurício, 2018 [50] | Quantum X; RJL Systems, Michigan, USA | 1 day before surgery | / 3 | / 3 | −1.65° | Brazilian | Cohort |
| Leon-Idougourram, 2022 [51] | TANITA MC-780 MA | / 3 | / 3 | / 3 | −1.65° | / 3 | Cohort |
| Harter, 2017 [52] | Quantum II; RJL Systems | Within 48 h after admission | / 3 | / 3 | −1.65° | / 3 | Cohort |
| Roccamatisi, 2021 [40] | Nutrilab; Akern, Florence, Italy | At 08:00 on the day before scheduled surgery | Within 30 d after discharge | 5° | 0.3° | / 3 | Cohort |
| Cereda, 2021 [53] | Nutriguard M; data Input Gmbh, Darmstadt Germany | Italian: diagnosis German: different stages of cancer | 1 year | / 3 | −1.65° | / 3 | Cohort |
| Study | Cut-Off Value | Nutritional Indicators Related to SPA 9 | Main Findings |
|---|---|---|---|
| Pena, 2019 [13] | −1.65° | PT-SGA 7, HGS 3, MAC 5, MMA 6 | Patients with SPA 9 < −1.65 had greater chance of malnourishment with low PT-SGA 7, MAC 5, MMA 6, and HGS 3. |
| Yates, 2020 [47] | 25th: −0.948° | Albumin | SPA 9 < −0.948 was positively related to albumin. |
| Norman, 2010 [34] | 5th | PT-SGA 7, EORTC 2 | SPA 9 below 5th percentile value emerged as a significant predictor for malnutrition and impaired functional status in generalized linear model regression analyses. |
| Leon-Idougourram, 2022 [51] | −1.65° | Arm circumference, calf circumference, BMI 1, CRP 8, IL-6 4, thigh adipose tissue | Serum CRP 8 and IL-6 4 were most reliable parameters for determining patients with decreased SPA 9. |
| Cereda, 2021 [53] | −1.65° | HGS 3, BMI 1, weight loss | In patients with SPA 9 < −1.65, worse nutritional and functional status were observed. |
| Study | Cut-Off Value | Type of Complications | Definition of Complications | Main Findings |
|---|---|---|---|---|
| Pena, 2019 [13] | −1.65° | Infectious complications; Non-infectious complications | Bulletin of the American College of Surgeons | Patients with SPA1 < −1.65 presented more infectious complications, but there was no association between SPA 1 and other complications. SPA 1 was only one significant predictor of infectious complications. |
| Harter, 2017 [52] | −1.65° | Postoperative complications | Clavien–Dindo classification | SPA 1 was significantly lower among those who had severe postoperative complications. |
| Maurício, 2018 [50] | −1.65° | Postoperative complications | Clavien–Dindo classification | SPA 1 showed no association with postoperative complications in cancer patients. |
| Roccamatisi, 2021 [40] | 0.3° | Infectious complications | Clavien–Dindo classification | SPA 1 was significantly lower in patients with infectious complications. SPA 1 < 0.3 was the only independent variable for infectious complications. |
| Study | Cut-Off Value | Type of Survival | Main Findings |
|---|---|---|---|
| Pena, 2019 [13] | −1.65° | Survival | There was no association between SPA 3 and survival. |
| Urbain, 2013 [49] | 25th: −2.26° | 2-year survival | SPA 3 < −2.26 was a significant independent predictor for 2-year survival in cancer patients. |
| Axelsson, 2018 [45] | −1.65° | 5-year survival | SPA 3 < −1.65 was a significant prognostic indicator for 5-year survival in cancer patients. |
| Hui, 2014 [46] | 5th | OS 1 | SPA 3 below 5th percentile value was found to be significantly related to OS 1. |
| Yates, 2020 [47] | −0.948° | OS 1, 30-day mortality, 60-day mortality | SPA 3 < −0.948 was positively related to OS 1, while there was no relationship between SPA 3 and 30-day or 60-day mortality in cancer patients. |
| Paiva, 2011 [44] | −1.65° | Survival | SPA 3 < −1.65 was a significant determining indicator of higher mortality in cancer patients. |
| Paixao, 2021 [48] | −1.65° | Survival | SPA 3 was not related to survival in cancer patients during RT 2. |
| Norman, 2010 [34] | 5th | 6-month survival | SPA 3 below 5th percentile value was an independent predictor for 6-month mortality of cancer patients. |
| Cereda, 2021 [53] | −1.65° | 1-year survival | SPA 3 < −1.65 was positively related to 1-year survival of German cohort and Italian cohort after adjusting in cancer patients. |
| Study | Cut-Off Value of PA 1 | Cut-Off Value of SPA 2 | p Value or AUC 3 of PA 1 | p Value or AUC 3 of SPA 2 | Comparison |
|---|---|---|---|---|---|
| Nutritionalstatus | |||||
| Norman, 2010 [34] | 5th | 5th | / | / | SPA 2 > PA 1 |
| Hui, 2014 [46] | 4.4° | 5th | HGS: p < 0.001; Maximal inspiratory pressure: p = 0.001; serum albumin: p < 0.001; fat-free mass: p < 0.001; fat-free mass index: p < 0.001. | HGS: p = 0.03; Maximal inspiratory pressure: p = 0.60; serum albumin: p = 0.001; fat-free mass: p = 0.02; fat-free mass index: p = 0.001. | SPA 2 < PA 1 |
| Clinical outcomes | |||||
| Complications | |||||
| Roccamatisi, 2021 [40] | 5° | 0.3° | p = 0.661 | p = 0.032 | SPA 2 > PA 1 |
| Survival | |||||
| Norman, 2010 [34] | 5th | 5th | / | / | SPA 2 > PA 1 |
| Paixao, 2021 [48] | / | −1.65° | Univariate analysis: p = 0.216;Adjusted analysis: p = 0.427 | Univariate analysis: p =0.527; Adjusted analysis: p = 0.221 | SPA 2 > PA 1 |
| Axelsson, 2018 [45] | 5.95° | −1.65° | AUC 3 = 0.73 | AUC 3 = 0.66 | SPA 2 < PA 1 |
| Hui, 2014 [46] | 4.4° | 5th | p = 0.28 | p = 0.11 | SPA 2 > PA 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, N.; Zhang, J.; Cheng, S.; Liang, B. The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature. Nutrients 2023, 15, 50. https://doi.org/10.3390/nu15010050
Jiang N, Zhang J, Cheng S, Liang B. The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature. Nutrients. 2023; 15(1):50. https://doi.org/10.3390/nu15010050
Chicago/Turabian StyleJiang, Nan, Jiaxin Zhang, Siming Cheng, and Bing Liang. 2023. "The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature" Nutrients 15, no. 1: 50. https://doi.org/10.3390/nu15010050
APA StyleJiang, N., Zhang, J., Cheng, S., & Liang, B. (2023). The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature. Nutrients, 15(1), 50. https://doi.org/10.3390/nu15010050