
Trajectories of the Prevalence of Sarcopenia in the Pre- and Post-Stroke Periods: A Systematic Review

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol Registration
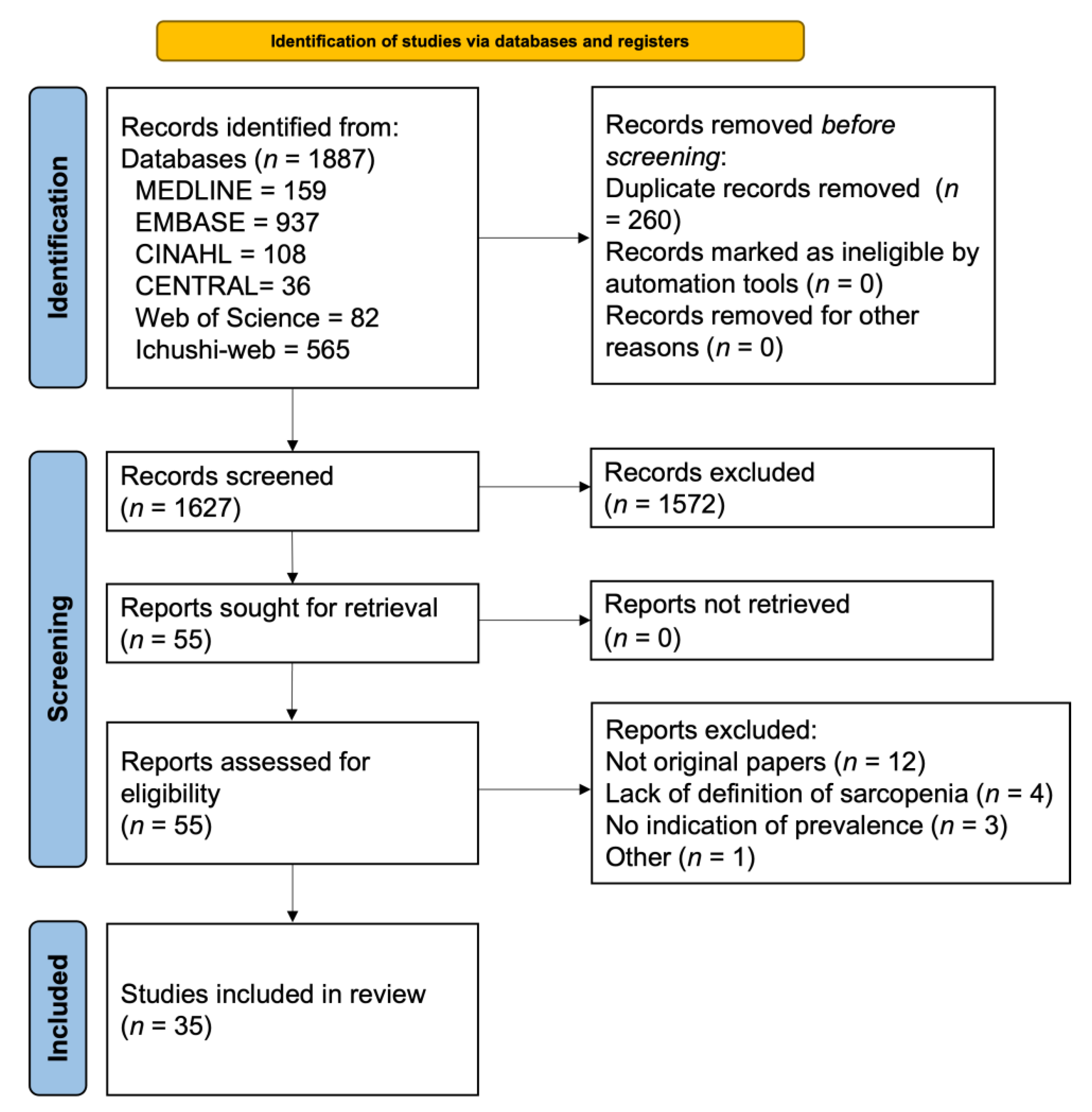
2.2. Study Search and Selection
2.3. Eligibility Criteria
2.4. Data Extraction
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Martone, A.M.; Bianchi, L.; Abete, P.; Bellelli, G.; Bo, M.; Cherubini, A.; Di Bari, M.; Maggio, M.; Manca, G.M.; Marzetti, E.; et al. The incidence of sarcopenia among hospitalized older patients: Results from the Glisten study. J. Cachexia. Sarcopenia Muscle 2017, 8, 907–914. [Google Scholar] [CrossRef]
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef]
- Toyoda, K.; Yoshimura, S.; Nakai, M.; Koga, M.; Sasahara, Y.; Sonoda, K.; Kamiyama, K.; Yazawa, Y.; Kawada, S.; Sasaki, M.; et al. Twenty-Year Change in Severity and Outcome of Ischemic and Hemorrhagic Strokes. JAMA Neurol. 2022, 79, 61–69. [Google Scholar] [CrossRef]
- Sennfält, S.; Norrving, B.; Petersson, J.; Ullberg, T. Long-Term Survival and Function after Stroke: A Longitudinal Observational Study from the Swedish Stroke Register. Stroke 2019, 50, 53–61. [Google Scholar] [CrossRef]
- Scherbakov, N.; Sandek, A.; Doehner, W. Stroke-Related Sarcopenia: Specific Characteristics. J. Am. Med. Dir. Assoc. 2015, 16, 272–276. [Google Scholar] [CrossRef]
- Scherbakov, N.; Von Haehling, S.; Anker, S.D.; Dirnagl, U.; Doehner, W. Stroke induced Sarcopenia: Muscle wasting and disability after stroke. Int. J. Cardiol. 2013, 170, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Yoshimura, Y.; Abe, T. Phase Angle as an Indicator of Baseline Nutritional Status and Sarcopenia in Acute Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106220. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kubo, H.; Kanai, M.; Yamamoto, M.; Okakita, M.; Suzuki, H.; Shimada, S.; Mase, K. Reliability and validity of measuring temporal muscle thickness as the evaluation of sarcopenia risk and the relationship with functional outcome in older patients with acute stroke. Clin. Neurol. Neurosurg. 2021, 201, 106444. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Yoshimua, Y.; Imai, R.; Sato, Y. A Combined Assessment Method of Phase Angle and Skeletal Muscle Index to Better Predict Functional Recovery after Acute Stroke. J. Nutr. Health Aging 2022, 26, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, I.H.; Heo, J.N.; Baik, M.; Park, H.; Lee, H.S.; Nam, H.S.; Kim, Y.D. Impact of Sarcopenia on Functional Outcomes Among Patients With Mild Acute Ischemic Stroke and Transient Ischemic Attack: A Retrospective Study. Front. Neurol. 2022, 13, 841945. [Google Scholar] [CrossRef] [PubMed]
- Bellelli, G.; Zambon, A.; Volpato, S.; Abete, P.; Bianchi, L.; Bo, M.; Cherubini, A.; Corica, F.; Di Bari, M.; Maggio, M.; et al. The association between delirium and sarcopenia in older adult patients admitted to acute geriatrics units: Results from the GLISTEN multicenter observational study. Clin. Nutr. 2018, 37, 1498–1504. [Google Scholar] [CrossRef] [PubMed]
- Kanai, M.; Nozoe, M.; Ohtsubo, T.; Yasumoto, I.; Ueno, K. Relationship of Functional Outcome With Sarcopenia and Objectively Measured Physical Activity in Patients With Stroke Undergoing Rehabilitation. J. Aging Phys. Act. 2022, 1–6. [Google Scholar] [CrossRef]
- Shimizu, A.; Fujishima, I.; Maeda, K.; Murotani, K.; Ohno, T.; Nomoto, A.; Nagami, S.; Nagano, A.; Sato, K.; Ueshima, J.; et al. Association between food texture levels consumed and the prevalence of malnutrition and sarcopenia in older patients after stroke. Eur. J. Clin. Nutr. 2022, 76, 1576–1582. [Google Scholar] [CrossRef]
- Shimizu, A.; Fujishima, I.; Maeda, K.; Murotani, K.; Ohno, T.; Nomoto, A.; Nagami, S.; Nagano, A.; Sato, K.; Ueshima, J.; et al. Delayed Dysphagia May Be Sarcopenic Dysphagia in Patients After Stroke. J. Am. Med. Dir. Assoc. 2021, 22, 2527–2533.e1. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S. Improvement in Oral Health Enhances the Recovery of Activities of Daily Living and Dysphagia after Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105961. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Elevated Creatinine-Based Estimated Glomerular Filtration Rate is Associated with Increased Risk of Sarcopenia, Dysphagia, and Reduced Functional Recovery after Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105491. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Yamanouchi, A.; Matsushita, T.; Nishioka, E.; Mori, N.; Taguchi, S. Validity of calf circumference for estimating skeletal muscle mass for the patients after stroke. Nutrition 2021, 82, 111028. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Low Hemoglobin Levels are Associated with Sarcopenia, Dysphagia, and Adverse Rehabilitation Outcomes After Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105405. [Google Scholar] [CrossRef] [PubMed]
- Nagano, F.; Yoshimura, Y.; Bise, T.; Shimazu, S.; Shiraishi, A. Muscle mass gain is positively associated with functional recovery in patients with sarcopenia after stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105017. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associ-ated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients: Implications for oral sarcopenia. Clin. Nutr. 2018, 37, 204–207. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Shimizu, A.; Nagano, A.; Ueshima, J.; Sato, K.; Murotani, K. Calf circumference value for sarcopenia screening among older adults with stroke. Arch. Gerontol. Geriatr. 2020, 93, 104290. [Google Scholar] [CrossRef]
- Matsushita, T.; Nishioka, S.; Taguchi, S.; Yamanouchi, A. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 1124–1128. [Google Scholar] [CrossRef]
- Tanaka, R.; Yoshimura, Y.; Shimazu, S.; Kitahara, K. Sarcopenia-induced reduction of instrumental activities of daily living among stroke patients discharged to home (Japanese). Sagyoryoho 2021, 40, 730–737. [Google Scholar]
- Ito, Y.; Nomura, S.; Yoshimura, Y. Incidence of new-onset sarcopenia and associated factors in stroke patients on a con-valescent rehabilitation ward (Japanese). JSPEN 2021, 3, 28–35. [Google Scholar]
- Yoshimura, Y.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Systemic Inflammation in the Recovery Stage of Stroke: Its Association with Sarcopenia and Poor Functional Rehabilitation Outcomes. Prog. Rehabil. Med. 2018, 3, 20180011. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kubo, H.; Kanai, M.; Yamamoto, M.; Shimada, S.; Mase, K. Sarcopenia risk and diabetes mellitus are independent factors for lower limb muscle strength in older patients with acute stroke: A cross-sectional study. Nutrition 2021, 84, 111025. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kanai, M.; Kubo, H.; Yamamoto, M.; Shimada, S.; Mase, K. Prestroke sarcopenia and functional outcomes in elderly patients who have had an acute stroke: A prospective cohort study. Nutrition 2019, 66, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kanai, M.; Kubo, H.; Yamamoto, M.; Shimada, S.; Mase, K. Prestroke Sarcopenia and Stroke Severity in Elderly Patients with Acute Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 2228–2231. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuki, M.; Hirayama, K.; Otsuki, M. Development and Internal Validation of a Nomogram to Predict Post-Stroke Fatigue After Discharge. J. Stroke Cerebrovasc. Dis. 2021, 30, 105484. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The Prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Inoue, T.; Ueshima, J.; Nagano, A.; Kawase, F. Prevalence of sarcopenia through the life course including pre and post stroke. Figshare J. Contrib. 2022. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Population of the Older Adults. Statistics Bureau of Japan. Available online: https://www.stat.go.jp/english/data/jinsui/tsuki/index.html (accessed on 1 November 2022).
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bise, T.; Shimazu, S.; Tanoue, M.; Tomioka, Y.; Araki, M.; Nishino, T.; Kuzuhara, A.; Takatsuki, F. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: A randomized controlled trial. Nutrition 2019, 58, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.S.; Ivey, F.M.; Serra, M.C.; Hartstein, J.; Hafer-Macko, C.E. Sarcopenia and Physical Function in Middle-Aged and Older Stroke Survivors. Arch. Phys. Med. Rehabil. 2017, 98, 495–499. [Google Scholar] [CrossRef]
- Arasaki, K.; Igarashi, O.; Ichikawa, Y.; Machida, T.; Shirozu, I.; Hyodo, A.; Ushijima, R. Reduction in the motor unit number estimate (MUNE) after cerebral infarction. J. Neurol. Sci. 2006, 250, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.L.; Polkey, M.I.; Bath, P.M.W.; Moxham, J. Quadriceps muscle weakness following acute hemiplegic stroke. Clin. Rehabil. 2001, 15, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Huppertz, V.; Guida, S.; Holdoway, A.; Strilciuc, S.; Baijens, L.; Schols, J.M.G.A.; van Helvoort, A.; Lansink, M.; Muresanu, D.F. Impaired Nutritional Condition After Stroke From the Hyperacute to the Chronic Phase: A Systematic Review and Meta-Analysis. Front. Neurol. 2022, 12, 2459. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of malnutrition in older adults: A multinational perspective using the mini nutritional assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef]
- Hunnicutt, J.L.; Gregory, C.M. Skeletal muscle changes following stroke: A systematic review and comparison to healthy individuals. Top. Stroke Rehabil. 2017, 24, 463–471. [Google Scholar] [CrossRef]
- Fini, N.A.; Holland, A.E.; Keating, J.; Simek, J.; Bernhardt, J. How physically active are people following stroke? Systematic review and quantitative synthesis. Phys. Ther. 2017, 97, 707–717. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Decreased Tongue Pressure is Associated with Sarcopenia and Sarcopenic Dysphagia in the Elderly. Dysphagia 2015, 30, 80–87. [Google Scholar] [CrossRef]
- Aarden, J.J.; Reijnierse, E.M.; van der Schaaf, M.; van der Esch, M.; Reichardt, L.A.; van Seben, R.; Bosch, J.A.; Twisk, J.W.R.; Maier, A.B.; Engelbert, R.H.H.; et al. Longitudinal Changes in Muscle Mass, Muscle Strength, and Physical Performance in Acutely Hospitalized Older Adults. J. Am. Med. Dir. Assoc. 2021, 22, 839–845.e1. [Google Scholar] [CrossRef] [PubMed]
- Yao, R.; Yao, L.; Yuan, C.; Gao, B.-L. Accuracy of Calf Circumference Measurement, SARC-F Questionnaire, and Ishii’s Score for Screening Stroke-Related Sarcopenia. Front. Neurol. 2022, 13, 880907. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Im, S.; Park, G.Y. Ultrasound evaluation of the rectus femoris for sarcopenia in patients with early subacute stroke. J. Clin. Med. 2021, 10, 3010. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Huang, K.C.; Han, D.S. Segmental body composition transitions in stroke patients: Trunks are different from extremities and strokes are as important as hemiparesis. Clin. Nutr. 2020, 39, 1968–1973. [Google Scholar] [CrossRef] [PubMed]
- Aydin, T.; Kesikta, F.N.; Oren, M.M.; Erdogan, T.; Ahisha, Y.C.; Kizilkurt, T.; Corum, M.; Karacan, I.; Öztürk, S.; Bahat, G. Sarcopenia in patients following stroke: An overlooked problem. Int. J. Rehabil. Res. 2021, 44, 269–275. [Google Scholar] [CrossRef]
- Jang, Y.; Im, S.; Han, Y.; Koo, H.; Sohn, D.; Park, G.Y. Can initial sarcopenia affect poststroke rehabilitation outcome? J. Clin. Neurosci. 2020, 71, 113–118. [Google Scholar] [CrossRef]
- Park, S.; Ham, J.O.; Lee, B.K. A positive association between stroke risk and sarcopenia in men aged ≥ 50 years, but not women: Results from the Korean National Health and Nutrition Examination Survey 2008–2010. J. Nutr. Health Aging 2014, 18, 806–812. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Cognitive impairment is independently associated with definitive and possible sarcopenia in hospitalized older adults: The prevalence and impact of comorbidities. Geriatr. Gerontol. Int. 2017, 17, 1048–1056. [Google Scholar] [CrossRef]
- Shibazaki, K.; Wakutani, Y.; Takao, Y. Sarcopenia in acute ischemic stroke patients (Japanese). JPN J. Strok. 2021, 43, 409–415. [Google Scholar] [CrossRef]
- Tanaka, K.; Tanaka, K.; Kose, T.; Takahashi, M.; Kamasaki, D.; Ota, H. Prevalence and characteristics of sarcopenia in acute stroke patients (Japanese). Rigakuryoho Saga 2021, 7, 21–27. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria (Screening Tool) | Study Region, Number of Studies | |
|---|---|---|
| Asia, n = 32 | Europe, n = 2 | |
| AWGS or AWGS2019 | 17 | 0 |
| EWGSOP 2 | 7 | 2 |
| SARC-F | 5 | 0 |
| FNIH | 1 | 0 |
| Others | 2 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, T.; Ueshima, J.; Kawase, F.; Kobayashi, H.; Nagano, A.; Murotani, K.; Saino, Y.; Maeda, K. Trajectories of the Prevalence of Sarcopenia in the Pre- and Post-Stroke Periods: A Systematic Review. Nutrients 2023, 15, 113. https://doi.org/10.3390/nu15010113
Inoue T, Ueshima J, Kawase F, Kobayashi H, Nagano A, Murotani K, Saino Y, Maeda K. Trajectories of the Prevalence of Sarcopenia in the Pre- and Post-Stroke Periods: A Systematic Review. Nutrients. 2023; 15(1):113. https://doi.org/10.3390/nu15010113
Chicago/Turabian StyleInoue, Tatsuro, Junko Ueshima, Fumiya Kawase, Haruko Kobayashi, Ayano Nagano, Kenta Murotani, Yoko Saino, and Keisuke Maeda. 2023. "Trajectories of the Prevalence of Sarcopenia in the Pre- and Post-Stroke Periods: A Systematic Review" Nutrients 15, no. 1: 113. https://doi.org/10.3390/nu15010113
APA StyleInoue, T., Ueshima, J., Kawase, F., Kobayashi, H., Nagano, A., Murotani, K., Saino, Y., & Maeda, K. (2023). Trajectories of the Prevalence of Sarcopenia in the Pre- and Post-Stroke Periods: A Systematic Review. Nutrients, 15(1), 113. https://doi.org/10.3390/nu15010113