
Relationship between Serum 25-Hydroxyvitamin D Level and Risk of Recurrent Stroke

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Participants and Setting
2.2. Outcome Measures
2.3. Serum 25(OH)D Levels and Other Independent Variables
3. Statistical Analysis
4. Results
5. Discussion
6. Strength and Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Khanevski, A.N.; Bjerkreim, A.T.; Novotny, V.; Næss, H.; Thomassen, L.; Logallo, N.; Kvistad, C.E.; The NOR-STROKE Study Group. Recurrent ischemic stroke: Incidence, predictors, and impact on mortality. Acta Neurol. Scand. 2019, 140, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flach, C.; Muruet, W.; Wolfe, C.D.; Bhalla, A.; Douiri, A. Risk and Secondary Prevention of Stroke Recurrence: A Population-Base Cohort Study. Stroke 2020, 51, 2435–2444. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S. Stroke in the21stCentury: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.H.; Ntaios, G. “Novel Clinical Concepts in Thrombosis”: Integrated Care for Stroke Management—Easy as ABC. Thromb. Haemost. 2021, 122, 316–319. [Google Scholar] [CrossRef]
- Zhou, R.; Wang, M.; Huang, H.; Li, W.; Hu, Y.; Wu, T. Lower Vitamin D Status Is Associated with an Increased Risk of Ischemic Stroke: A Systematic Review and Meta-Analysis. Nutrition 2018, 10, 277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jani, R.; Mhaskar, K.; Tsiampalis, T.; Kassaw, N.A.; González, M.; Ángel, M.; Panagiotakos, D.B. Circulating 25-hydroxy-vitamin D and the risk of cardiovascular diseases. Systematic review and meta-analysis of prospective cohort studies. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3282–3304. [Google Scholar] [CrossRef]
- Shi, H.; Chen, H.; Zhang, Y.; Li, J.; Fu, K.; Xue, W.; Teng, W.; Tian, L. 25-Hydroxyvitamin D level, vitamin D intake, and risk of stroke: A dose-response meta-analysis. Clin. Nutr. 2020, 39, 2025–2034. [Google Scholar] [CrossRef]
- Su, C.; Jin, B.; Xia, H.; Zhao, K. Association between Vitamin D and Risk of Stroke: A PRISMA-Compliant Systematic Review and Meta-Analysis. Eur. Neurol. 2021, 84, 399–408. [Google Scholar] [CrossRef]
- Qiu, H.; Wang, M.; Mi, D.; Zhao, J.; Tu, W.; Liu, Q. Vitamin D status and the risk of recurrent stroke and mortality in ischemic stroke patients: Data from a 24-month follow-up study in China. J. Nutr. Health Aging 2017, 21, 766–771. [Google Scholar] [CrossRef]
- Huang, H.; Zheng, T.; Wang, S.; Wei, L.; Wang, Q.; Sun, Z. Serum 25-hydroxyvitamin D predicts early recurrent stroke in ischemic stroke patients. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 908–914. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siniscalchi, A.; Lochner, P.; Anticoli, S.; Chirchiglia, D.; De Sarro, G.; Gallelli, L. What is the Current Role for Vitamin D and the Risk of Stroke? Curr. Neurovascular Res. 2019, 16, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Yarlagadda, K.; Ma, N.; Doré, S. Vitamin D and Stroke: Effects on Incidence, Severity, and Outcome and the Potential Benefits of Supplementation. Front. Neurol. 2020, 11, 384. [Google Scholar] [CrossRef]
- Michos, E.D.; Carson, K.A.; Schneider, A.L.C.; Lutsey, P.L.; Xing, L.; Sharrett, A.R.; Alonso, A.; Coker, L.H.; Gross, M.; Post, W.; et al. Vitamin D and Subclinical Cerebrovascular Disease: The Atherosclerosis Risk in Communities brain magnetic resonance imaging study. JAMA Neurol. 2014, 71, 863. [Google Scholar] [CrossRef] [Green Version]
- Berridge, M.J. Vitamin D deficiency and diabetes. Biochem. J. 2017, 474, 1321–1332. [Google Scholar] [CrossRef]
- Kheiri, B.; Abdalla, A.; Osman, M.; Ahmed, S.; Hassan, M.; Bachuwa, G. Vitamin D deficiency and risk of cardiovascular diseases: A narrative review. Clin. Hypertens. 2018, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Makariou, S.; Michel, P.; Tzoufi, M.; Challa, A.; Milionis, H. Vitamin D and Stroke: Promise for Prevention and Better Outcome. Curr. Vasc. Pharmacol. 2014, 12, 117–124. [Google Scholar] [CrossRef]
- Drüeke, T.B.; Massy, Z.A. Role of vitamin D in vascular calcification: Bad guy or good guy? Nephrol. Dial. Transplant. 2012, 27, 1704–1707. [Google Scholar] [CrossRef] [Green Version]
- Ji, W.; Zhou, H.; Wang, S.; Cheng, L.; Fang, Y. Low serum levels of 25-hydroxyvitamin D are associated with stroke recurrence and poor functional outcomes in patients with ischemic stroke. J. Nutr. Health Aging 2016, 21, 892–896. [Google Scholar] [CrossRef]
- Welles, C.C.; Whooley, M.A.; Karumanchi, S.A.; Hod, T.; Thadhani, R.; Berg, A.H.; Ix, J.H.; Mukamal, K.J. Vitamin D deficiency and cardiovascular events in patients with coronary heart disease: Data from the Heart and Soul Study. Am. J. Epidemiol. 2014, 179, 1279–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolmos, M.; Christoffersen, L.; Kruuse, C. Recurrent Ischemic Stroke—A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2021, 30, 105935. [Google Scholar] [CrossRef] [PubMed]
- Talelli, P.; Greenwood, R.J. Review: Recurrent stroke: Where do we stand with the secondary prevention of noncardioembolic ischaemic strokes? Ther. Adv. Cardiovasc. Dis. 2008, 2, 387–405. [Google Scholar] [CrossRef] [PubMed]
- Fewell, Z.; Smith, G.D.; Sterne, J.A.C. The Impact of Residual and Unmeasured Confounding in Epidemiologic Studies: A Simulation Study. Am. J. Epidemiol. 2007, 166, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Fraser, W.D.; Tang, J.C.Y.; Dutton, J.J.; Schoenmakers, I. Vitamin D Measurement, the Debates Continue, New Analytes Have Emerged, Developments Have Variable Outcomes. Calcif. Tissue Res. 2019, 106, 3–13. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Characteristics | Total Participants (n = 6824) | Stroke Recurrence during Follow-Up | ||
|---|---|---|---|---|
| Yes (n = 388) | No (n = 6436) | p-Value | ||
| Age: mean (SD), years | 60.6 (6.9) | 61.9 (6.4) | 60.6 (6.9) | <0.01 |
| Female sex: n (%) | 2783 (40.8) | 136 (35.1) | 2647 (41.1) | 0.02 |
| BMI: mean (SD), kg/m2 | 28.8 (5.1) | 28.5 (4.9) | 28.9 (5.1) | 0.13 |
| Smoking: n (%) | ||||
| Never | 2747 (40.6) | 140 (36.4) | 2607 (40.9) | 0.05 |
| Former | 2915 (43.1) | 167 (43.4) | 2748 (43.1) | |
| Current | 1097 (16.2) | 78 (20.3) | 1019 (16.0) | |
| Alcohol drinking: n (%) | ||||
| Never | 446 (6.6) | 28 (7.3) | 418 (6.5) | 0.83 |
| Former | 588 (8.7) | 32 (8.3) | 556 (8.7) | |
| Current | 5761 (84.8) | 326 (84.5) | 5435 (84.8) | |
| White ethnicity: n (%) | 6465 (95.3) | 367 (94.8) | 6098 (95.3) | 0.68 |
| With college or university degree: n (%) | 567 (8.5) | 31 (8.2) | 536 (8.5) | 0.83 |
| Physical activity (≥600 MET min per week): n (%) | 3792 (73.1) | 196 (66.9) | 3596 (73.5) | 0.01 |
| Comorbidity: n (%) | ||||
| Atrial fibrillation | 535 (7.8) | 39 (10.1) | 496 (7.7) | 0.10 |
| Hypertension | 4222 (61.9) | 269 (69.3) | 3953 (61.4) | <0.01 |
| Hypercholesterolemia | 2996 (43.9) | 188 (48.5) | 2808 (43.6) | 0.06 |
| Diabetes | 1003 (14.7) | 92 (23.7) | 911 (14.2) | <0.01 |
| Heart failure | 206 (3.0) | 17 (4.4) | 189 (2.9) | 0.11 |
| Medication and supplementation intake: n (%) | ||||
| NSAIDs | 694 (10.2) | 38 (9.8) | 656 (10.2) | 0.80 |
| Antihypertensive drugs | 4075 (59.8) | 259 (66.8) | 3816 (59.4) | <0.01 |
| Antidiabetic drugs | 763 (11.2) | 76 (19.6) | 687 (10.7) | <0.01 |
| Statins | 4462 (65.4) | 274 (70.6) | 4188 (65.1) | 0.03 |
| Anticoagulants | 631 (9.2) | 51 (13.1) | 580 (9.0) | <0.01 |
| Vitamins | 1934 (28.7) | 110 (28.6) | 1824 (28.7) | 0.99 |
| Minerals and other dietary supplementation | 2685 (39.6) | 144 (37.5) | 2541 (39.7) | 0.39 |
| Serum 25(OH)D: mean (SD), nmol/L | 46.5 (22.4) | 45.6 (25.9) | 46.5 (22.1) | 0.48 |
| Outcome/Analysis | No. of Events/No. of Patients | 25(OH)D Level, in nmol/L 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 20 | 30 | 40 | 50 | 60 | 70 | 80 | |||
| Main analysis | ||||||||||
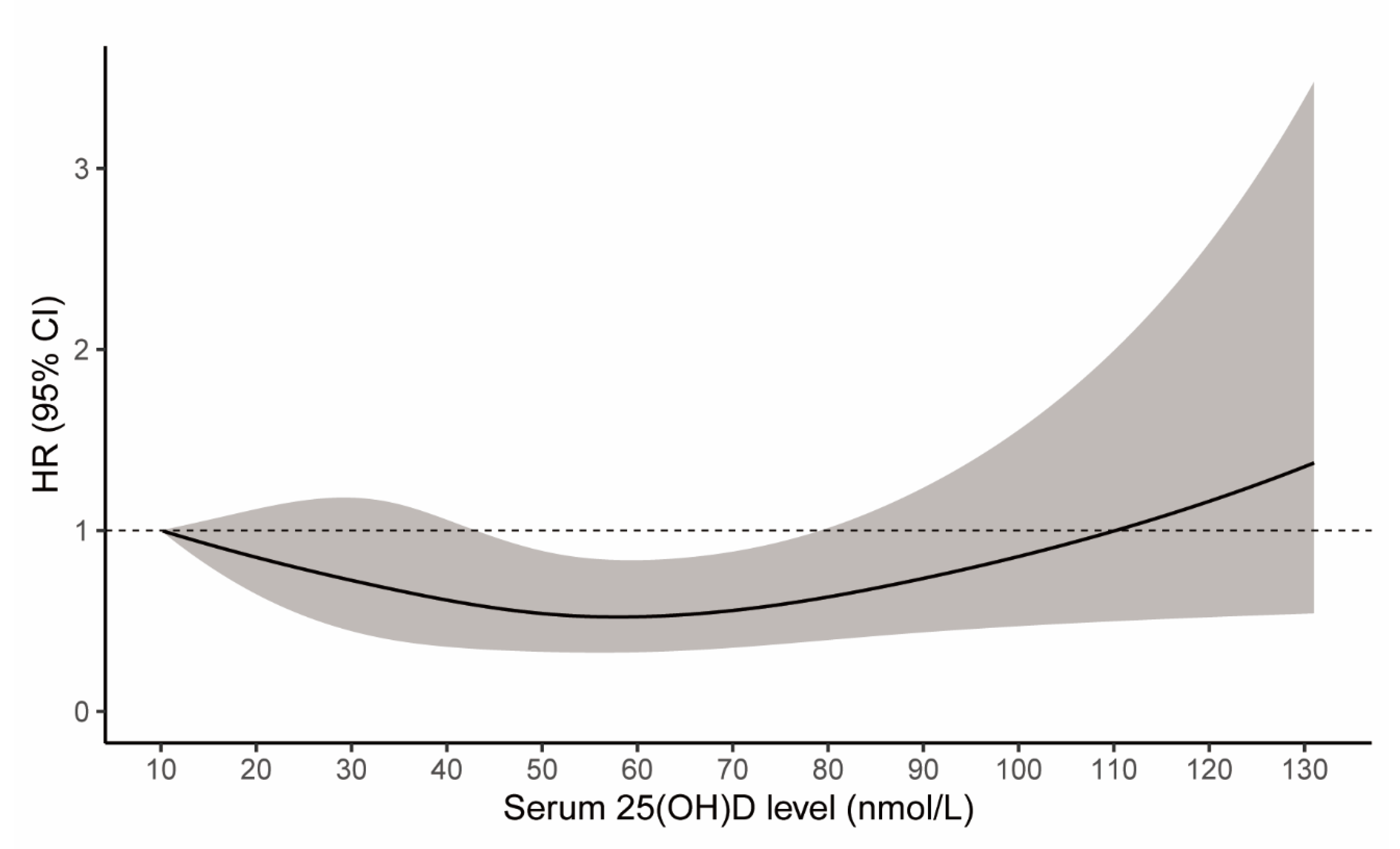
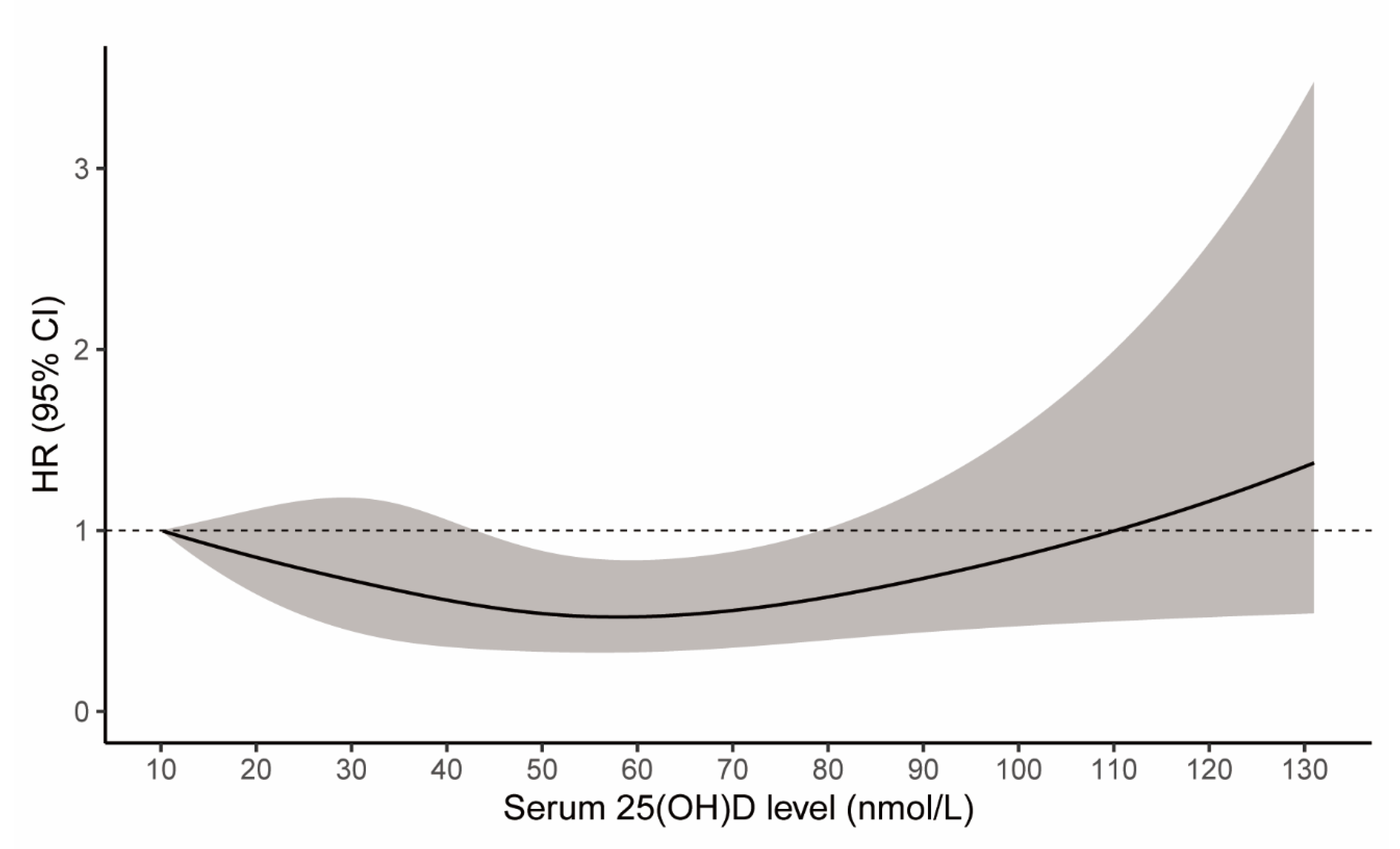
| Primary outcome | Total recurrent stroke | 388/6824 | Ref | 0.85 (0.65–1.12) | 0.72 (0.44–1.18) | 0.62 (0.36–1.06) | 0.54 (0.33–0.89) | 0.52 (0.33–0.84) | 0.56 (0.35–0.88) | 0.63 (0.39–1.01) |
| Secondary outcome | Ischemic stroke | 250/6824 | Ref | 0.91 (0.64–1.28) | 0.82 (0.44–1.54) | 0.75 (0.37–1.51) | 0.70 (0.37–1.32) | 0.69 (0.38–1.26) | 0.72 (0.40–1.31) | 0.79 (0.43–1.44) |
| Hemorrhagic stroke | 87/6824 | Ref | 0.64 (0.36–1.13) | 0.44 (0.16–1.21) | 0.38 (0.12–1.16) | 0.40 (0.15–1.09) | 0.42 (0.16–1.06) | 0.40 (0.16–1.02) | 0.38 (0.14–1.02) | |
| Subgroup analysis | ||||||||||
| By sex | Males | 252/4041 | Ref | 1.01 (0.73–1.41) | 0.99 (0.54–1.80) | 0.88 (0.45–1.72) | 0.74 (0.40–1.37) | 0.70 (0.39–1.25) | 0.76 (0.43–1.35) | 0.91 (0.51–1.63) |
| Females | 136/2783 | Ref | 0.54 (0.33–0.88) | 0.33 (0.14–0.78) | 0.29 (0.11–0.72) | 0.32 (0.14–0.74) | 0.34 (0.16–0.74) | 0.31 (0.14–0.67) | 0.25 (0.11–0.60) | |
| By age | <65 years | 205/4355 | Ref | 0.85 (0.58–1.24) | 0.71 (0.36–1.37) | 0.56 (0.28–1.12) | 0.45 (0.24–0.85) | 0.43 (0.23–0.79) | 0.47 (0.25–0.86) | 0.56 (0.30–1.04) |
| ≥65 years | 183/2469 | Ref | 0.86 (0.58–1.28) | 0.75 (0.36–1.57) | 0.68 (0.28–1.64) | 0.66 (0.29–1.48) | 0.66 (0.31–1.39) | 0.68 (0.33–1.41) | 0.72 (0.34–1.52) | |
| Serum 25(OH)D Level | Recurrent Stroke | ||
|---|---|---|---|
| No. of Events/No. of Patients | HR (95% CI) 1 | p-Value | |
| Defined by quartile 2 | |||
| 1st quartile | 117/1719 | Ref | - |
| 2nd quartile | 92/1707 | 0.77 (0.56–1.07) | 0.12 |
| 3rd quartile | 86/1693 | 0.68 (0.48–0.96) | 0.03 |
| 4th quartile | 93/1705 | 0.77 (0.55–1.08) | 0.13 |
| Defined by status | |||
| Deficiency (<25 nmol/L) | 97/1239 | Ref | - |
| Insufficiency (25–50 nmol/L) | 149/2906 | 0.60 (0.44–0.81) | < 0.01 |
| Sufficiency (>50 nmol/L) | 142/2679 | 0.59 (0.43–0.82) | < 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, G.; Li, L.; Adachi, J.D.; Wang, R.; Ye, Z.; Liu, X.; Thabane, L.; Lip, G.Y.H. Relationship between Serum 25-Hydroxyvitamin D Level and Risk of Recurrent Stroke. Nutrients 2022, 14, 1908. https://doi.org/10.3390/nu14091908
Li G, Li L, Adachi JD, Wang R, Ye Z, Liu X, Thabane L, Lip GYH. Relationship between Serum 25-Hydroxyvitamin D Level and Risk of Recurrent Stroke. Nutrients. 2022; 14(9):1908. https://doi.org/10.3390/nu14091908
Chicago/Turabian StyleLi, Guowei, Likang Li, Jonathan D. Adachi, Ruoting Wang, Zebing Ye, Xintong Liu, Lehana Thabane, and Gregory Y. H. Lip. 2022. "Relationship between Serum 25-Hydroxyvitamin D Level and Risk of Recurrent Stroke" Nutrients 14, no. 9: 1908. https://doi.org/10.3390/nu14091908
APA StyleLi, G., Li, L., Adachi, J. D., Wang, R., Ye, Z., Liu, X., Thabane, L., & Lip, G. Y. H. (2022). Relationship between Serum 25-Hydroxyvitamin D Level and Risk of Recurrent Stroke. Nutrients, 14(9), 1908. https://doi.org/10.3390/nu14091908