
Comparable Analysis of Acute Changes in Vascular Tone after Coffee versus Energy Drink Consumption

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
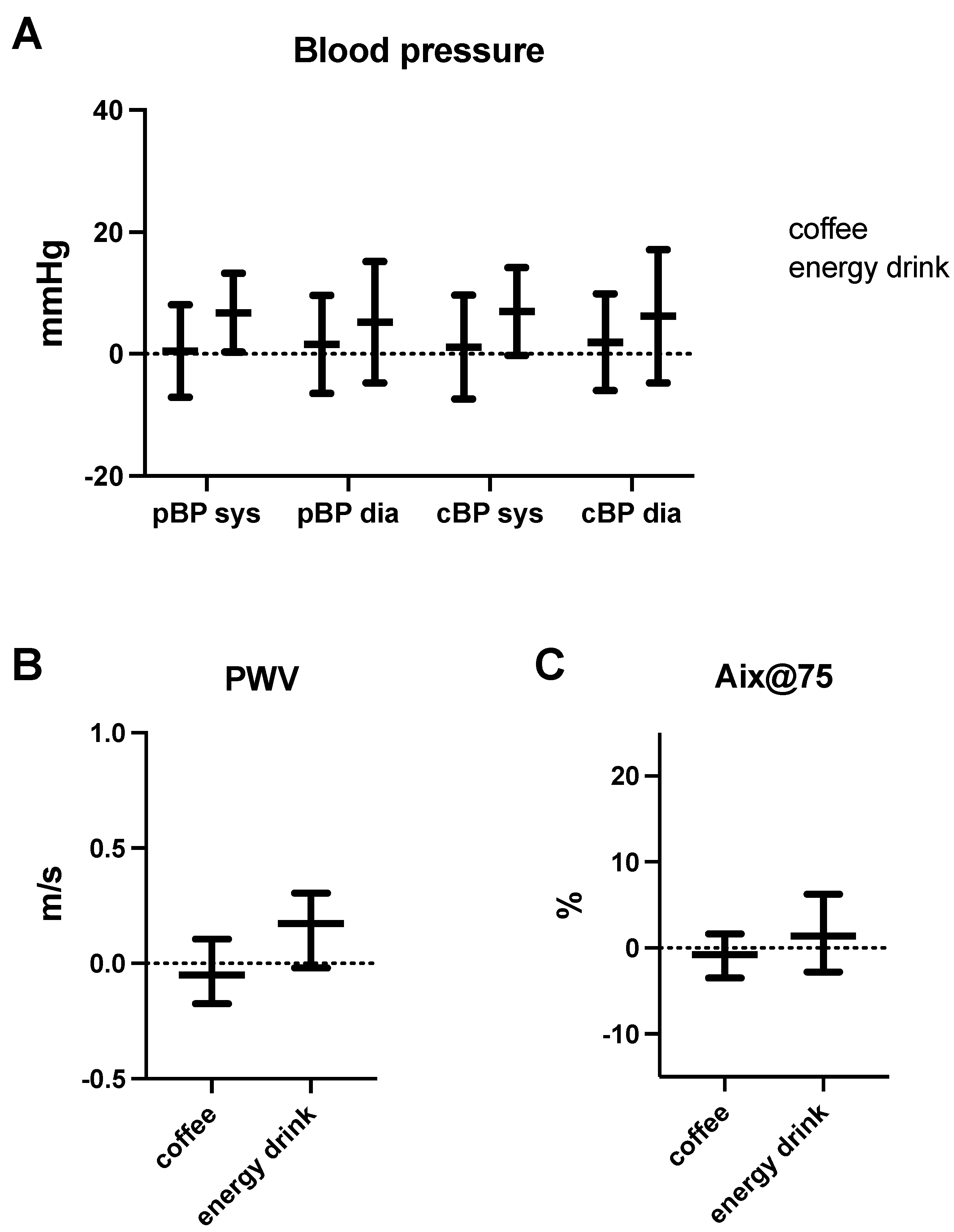
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reyes, C.M.; Cornelis, M.C. Caffeine in the Diet: Country-Level Consumption and Guidelines. Nutrients 2018, 10, 1772. [Google Scholar] [CrossRef] [Green Version]
- Cappelletti, S.; Piacentino, D.; Sani, G.; Aromatario, M. Caffeine: Cognitive and physical performance enhancer or psychoactive drug? Curr. Neuropharmacol. 2015, 13, 71–88. [Google Scholar] [CrossRef] [Green Version]
- Simon, J.; Fung, K.; Raisi-Estabragh, Z.; Aung, N.; Khanji, M.Y.; Kolossvary, M.; Merkely, B.; Munroe, P.B.; Harvey, N.C.; Piechnik, S.K.; et al. Light to moderate coffee consumption is associated with lower risk of death: A UK Biobank study. Eur. J. Prev. Cardiol. 2022, 20, zwac008. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; Bhatti, S.K.; Patil, H.R.; DiNicolantonio, J.J.; Lucan, S.C.; Lavie, C.J. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality. J. Am. Coll Cardiol. 2013, 62, 1043–1051. [Google Scholar] [CrossRef] [Green Version]
- Freedman, N.D.; Park, Y.; Abnet, C.C.; Hollenbeck, A.R.; Sinha, R. Association of coffee drinking with total and cause-specific mortality. N. Engl. J. Med. 2012, 366, 1891–1904. [Google Scholar] [CrossRef]
- Ludwig, I.A.; Clifford, M.N.; Lean, M.E.; Ashihara, H.; Crozier, A. Coffee: Biochemistry and potential impact on health. Food Funct. 2014, 5, 1695–1717. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Kalman, J.M.; Kistler, P.M. Caffeine and Arrhythmias: Time to Grind the Data. JACC Clin. Electrophysiol. 2018, 4, 425–432. [Google Scholar] [CrossRef]
- Mangi, M.A.; Rehman, H.; Rafique, M.; Illovsky, M. Energy Drinks and the Risk of Cardiovascular Disease: A Review of Current Literature. Cureus 2017, 9, e1322. [Google Scholar] [CrossRef] [Green Version]
- Mansia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; et al. 2007 ESH-ESC Guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2007, 16, 135–232. [Google Scholar] [CrossRef]
- Del Giorno, R.; Scanzio, S.; De Napoli, E.; Stefanelli, K.; Gabutti, S.; Troiani, C.; Gabutti, L. Habitual coffee and caffeinated beverages consumption is inversely associated with arterial stiffness and central and peripheral blood pressure. Int. J. Food Sci. Nutr. 2022, 73, 106–115. [Google Scholar] [CrossRef]
- Riksen, N.P.; Rongen, G.A.; Smits, P. Acute and long-term cardiovascular effects of coffee: Implications for coronary heart disease. Pharmacol. Ther. 2009, 121, 185–191. [Google Scholar] [CrossRef]
- Karatzis, E.; Papaioannou, T.G.; Aznaouridis, K.; Karatzi, K.; Stamatelopoulos, K.; Zampelas, A.; Papamichael, C.; Lekakis, J.; Mavrikakis, M. Acute effects of caffeine on blood pressure and wave reflections in healthy subjects: Should we consider monitoring central blood pressure? Int. J. Cardiol. 2005, 98, 425–430. [Google Scholar] [CrossRef]
- Mahmud, A.; Feely, J. Acute effect of caffeine on arterial stiffness and aortic pressure waveform. Hypertension 2001, 38, 227–231. [Google Scholar] [CrossRef] [Green Version]
- Ioakeimidis, N.; Tzifos, V.; Vlachopoulos, C.; Terentes-Printzios, D.; Georgakopoulos, C.; Tousoulis, D. Acute effect of coffee on aortic stiffness and wave reflections in healthy individuals: Differential effect according to habitual consumption. Int. J. Food Sci. Nutr. 2018, 69, 870–881. [Google Scholar] [CrossRef]
- Nehlig, A. Interindividual Differences in Caffeine Metabolism and Factors Driving Caffeine Consumption. Pharmacol. Rev. 2018, 70, 384–411. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.A.; Occiano, A.; Nguyen, T.A.; Chan, A.; Sky, J.C.; Bhattacharyya, M.; O’Dell, K.M.; Shek, A.; Nguyen, N.N. Electrocardiographic and blood pressure effects of energy drinks and Panax ginseng in healthy volunteers: A randomized clinical trial. Int. J. Cardiol. 2016, 218, 318–323. [Google Scholar] [CrossRef]
- Waldron, M.; Patterson, S.D.; Tallent, J.; Jeffries, O. The Effects of Oral Taurine on Resting Blood Pressure in Humans: A Meta-Analysis. Curr. Hypertens. Rep. 2018, 20, 81. [Google Scholar] [CrossRef] [Green Version]
- Genovesi, S.; Giussani, M.; Orlando, A.; Orgiu, F.; Parati, G. Salt and Sugar: Two Enemies of Healthy Blood Pressure in Children. Nutrients 2021, 13, 697. [Google Scholar] [CrossRef]
- Mansoori, S.; Kushner, N.; Suminski, R.R.; Farquhar, W.B.; Chai, S.C. Added Sugar Intake is Associated with Blood Pressure in Older Females. Nutrients 2019, 11, 2060. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; O’Rourke, M.F.; Safar, M.E.; Baou, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and meta-analysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, I.B.; Fuchs, S.A.; Jansen, I.M.; Spratt, J.C.; Murray, G.D.; Cockcroft, J.R.; Webb, D.J. Reproducibility of pulse wave velocity and augmentation index measured by pulse wave analysis. J. Hypertens. 1998, 16, 2079–2084. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total (23) | Female (12) | Male (11) | |
|---|---|---|---|
| Age | 31.1 (27.3, 35.2) | 30.6 (26.1, 34.9) | 31.1 (28.7, 35.2) |
| Height (cm) | 170 (167.5, 182,5) | 167.5 (164.0, 170.0) | 183 (179.0, 185.0) |
| Weight (kg) | 70 (62.0, 85.0) | 62 (60.0, 72.0) | 84 (70.8, 87.5) |
| BMI (kg/m2) | 23.7 (21.7, 26.0) | 22.8 (21.4, 25.5) | 25.7 (22.4, 26.0) |
| Coffee (240 mg Caffeine, 120 mL) | ||
| Coffee | ||
| Before | After | |
| HR (bpm) | 79.6 (72.3, 84.8) | 76.4 (72.0, 83.1) |
| pBP sys (mmHg) | 125.8 (115.8, 132.0) | 125.4 (117.0, 131.4) |
| pBP dia (mmHg) | 80.9 (68.1, 91.2) | 83.7 (72.7, 88.7) |
| pBP mean (mmHg) | 98.3 (86.2, 106.9) | 99.2 (90.7, 104.8) |
| cBP sys (mmHg) | 113.7 (104.2, 120.7) | 112.8 (104.8, 120.3) |
| cBP dia (mmHg) | 82.6 (69.3, 93.1) | 85.0 (76.9, 90.9) |
| PWV (m/s) | 5.56 (5.19, 5.88) | 5.43 (5.11, 5.96) |
| Aix@75 (%) | 17.5 (13.1, 20.8) | 16.1 (13.5, 21.5) |
| AugP (mmHg) | 4.22 (3.66, 7.13) | 4.50 (3.00, 6.75) |
| Energy Drink (240 mg caffeine, 750 mL) | ||
| Energy Drink | ||
| Before | After | |
| HR (bpm) | 78.0 (67.5, 83.2) | 73.3 (67.8, 78.7) |
| pBP sys (mmHg) | 120.8 (114.8, 126.5) | 127.4 (120.0, 133.5) |
| pBP dia (mmHg) | 76.8 (69.8, 82.6) | 82.0 (74.5, 90.0) |
| pBP mean (mmHg) | 93.5 (86.5, 102.5) | 101.3 (95.8, 105.8) |
| cBP sys (mmHg) | 110.4 (102.2, 115.3) | 114.7 (109.8, 125.8) |
| cBP dia (mmHg) | 77.6 (72.0, 84.6) | 84.4 (76.5, 93.4) |
| PWV (m/s) | 5.39 (5.04, 5.92) | 5.62 (5.24, 6.21) |
| Aix@75 (%) | 15.2 (9.0, 23.3) | 18.5 (12.0, 26.0) |
| AugP (mmHg) | 4.20 (2.50, 8.00) | 5.50 (3.00, 10.75) |
| Water (0 mg caffeine, 750 mL) | ||
| Water | ||
| Before | After | |
| HR (bpm) | 74.5 (67.7, 76.4) | 66.8 (62.7, 69.1) |
| pBP sys (mmHg) | 112.6 (105.1, 126.7) | 119.6 (113.0, 131.5) |
| pBP dia (mmHg) | 74.9 (65.5, 101.9) | 79.2 (75.1, 87.8) |
| pBP mean (mmHg) | 89.9 (81.4, 111.8) | 94.3 (91.4, 105.1) |
| cBP sys (mmHg) | 105.7 (98.2, 122.6) | 111.0 (107.5, 118.7) |
| cBP dia (mmHg) | 76.2 (66.8, 103.0) | 79.9 (76.3, 91.3) |
| PWV (m/s) | 5.92 (5.41, 6.73) | 5.96 (5.58, 6.96) |
| Aix@75 (%) | 14.4 (4.2, 28.9) | 12.8 (7.5, 25.3) |
| AugP (mmHg) | 4.00 (1.28, 9.50) | 4.13 (2.74, 10.13) |
| Coffee | Energy Drink | p-Value | p-Value (adj.) | |
|---|---|---|---|---|
| HR (bpm) | −2.28 | −4.60 | 0.166 | 0.516 |
| pBP sys (mmHg) | −0.91 | +6.35 | 0.013 | 0.131 |
| pBP dia (mmHg) | +1.00 | +4.00 | 0.276 | 0.575 |
| pBP mean (mmHg) | −0.43 | +5.25 | 0.016 | 0.145 |
| cBP sys (mmHg) | −1.63 | +7.00 | 0.017 | 0.145 |
| cBP dia (mmHg) | +0.85 | +3.07 | 0.248 | 0.575 |
| PWV (m/s) | −0.04 | +0.17 | 0.042 | 0.257 |
| Aix@75 (%) | −0.78 | +1.40 | 0.098 | 0.421 |
| AugP (mmHg) | −0.23 | +0.95 | 0.087 | 0.421 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schüttler, D.; Hamm, W.; Kellnar, A.; Brunner, S.; Stremmel, C. Comparable Analysis of Acute Changes in Vascular Tone after Coffee versus Energy Drink Consumption. Nutrients 2022, 14, 1888. https://doi.org/10.3390/nu14091888
Schüttler D, Hamm W, Kellnar A, Brunner S, Stremmel C. Comparable Analysis of Acute Changes in Vascular Tone after Coffee versus Energy Drink Consumption. Nutrients. 2022; 14(9):1888. https://doi.org/10.3390/nu14091888
Chicago/Turabian StyleSchüttler, Dominik, Wolfgang Hamm, Antonia Kellnar, Stefan Brunner, and Christopher Stremmel. 2022. "Comparable Analysis of Acute Changes in Vascular Tone after Coffee versus Energy Drink Consumption" Nutrients 14, no. 9: 1888. https://doi.org/10.3390/nu14091888
APA StyleSchüttler, D., Hamm, W., Kellnar, A., Brunner, S., & Stremmel, C. (2022). Comparable Analysis of Acute Changes in Vascular Tone after Coffee versus Energy Drink Consumption. Nutrients, 14(9), 1888. https://doi.org/10.3390/nu14091888