
Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study †

 ,
,  ,
,  ,
,  ,
,  ,
,  , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Procedures and Data Collection
Socio-Demographic and Anthropometric Information
2.3. Procedures, Dietary Survey and Data Collection
2.4. Quantification of Sugar Consumption
2.4.1. Selection of Food Products and Brands
2.4.2. Classification and Quantification of Sugars in Food
- -
- Foods without added sugars: It was considered that 100% of the total sugars listed in the FCT are intrinsic.
- -
- Foods with added sugars: In cases where the percentage of added sugars was declared on the ingredient list of the nutritional labelling, the amount of added sugars was directly calculated and the amount of intrinsic sugars was estimated by difference with the total sugars content declared. In those cases where the percentage of added sugars was not declared, the intrinsic sugars content was calculated based on the content of each of the ingredients in the product, using the nutritional composition obtained from the FCT [27]. The above referred amount was subtracted from the total sugars content of the nutritional product labeling to estimate the added sugar content. Next, the weight percentages for both types of sugars were estimated, so that X% INTRINSIC and X% ADDED were applied to the total sugars of the FCT of each coded food.
- Subgroup of milks (natural, standard milks and adapted milk formulas): Given the focus of this article on this food subgroup, the intrinsic and added sugars provided by these foods were calculated directly with the % of intrinsic and added sugars estimated for the specific type and brand of milk consumed by each participant.
- The rest of food the groups apart from the milk subgroup: The intake of intrinsic and added sugars provided by these foods was calculated from the average % of intrinsic and added sugars calculated for the brands according to their proportion of consumption.
- -
- Foods considered properly as added sugar: Due to their nutritional characteristics and according to current legislation, white sugar, brown sugar and honey were considered 100% added sugars.
2.5. Statistical Analysis
3. Results
3.1. Usual Intake of Intrinsic and Added Sugars in Children
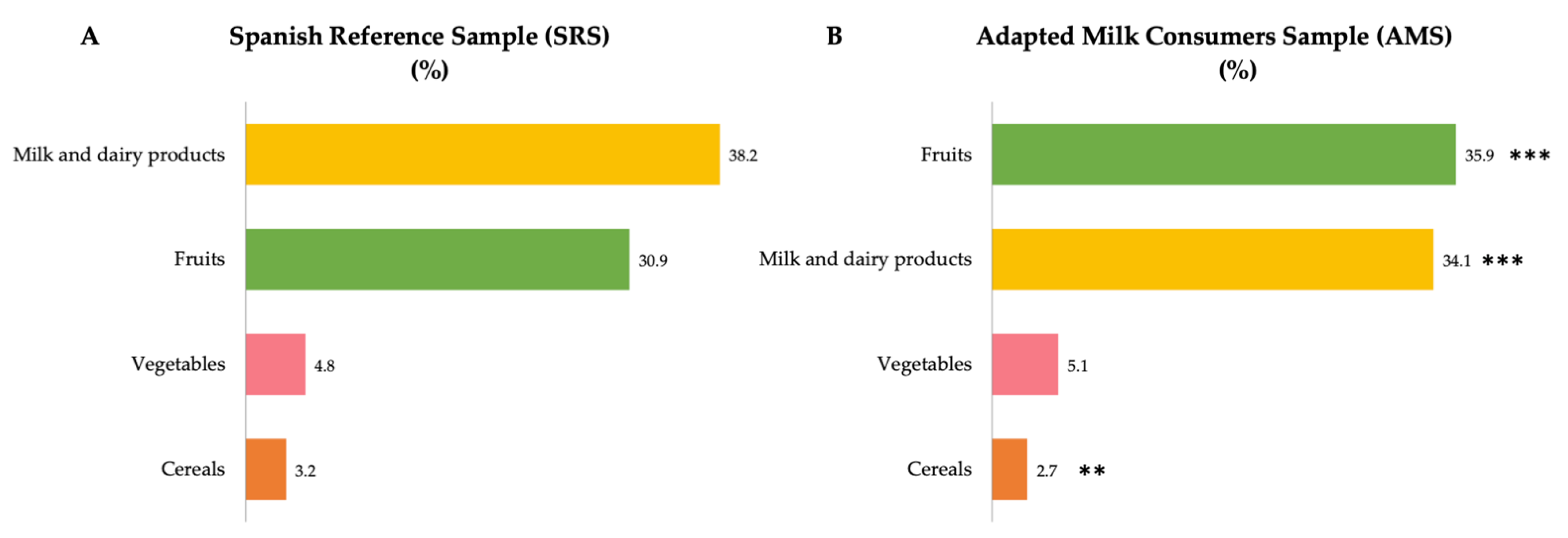
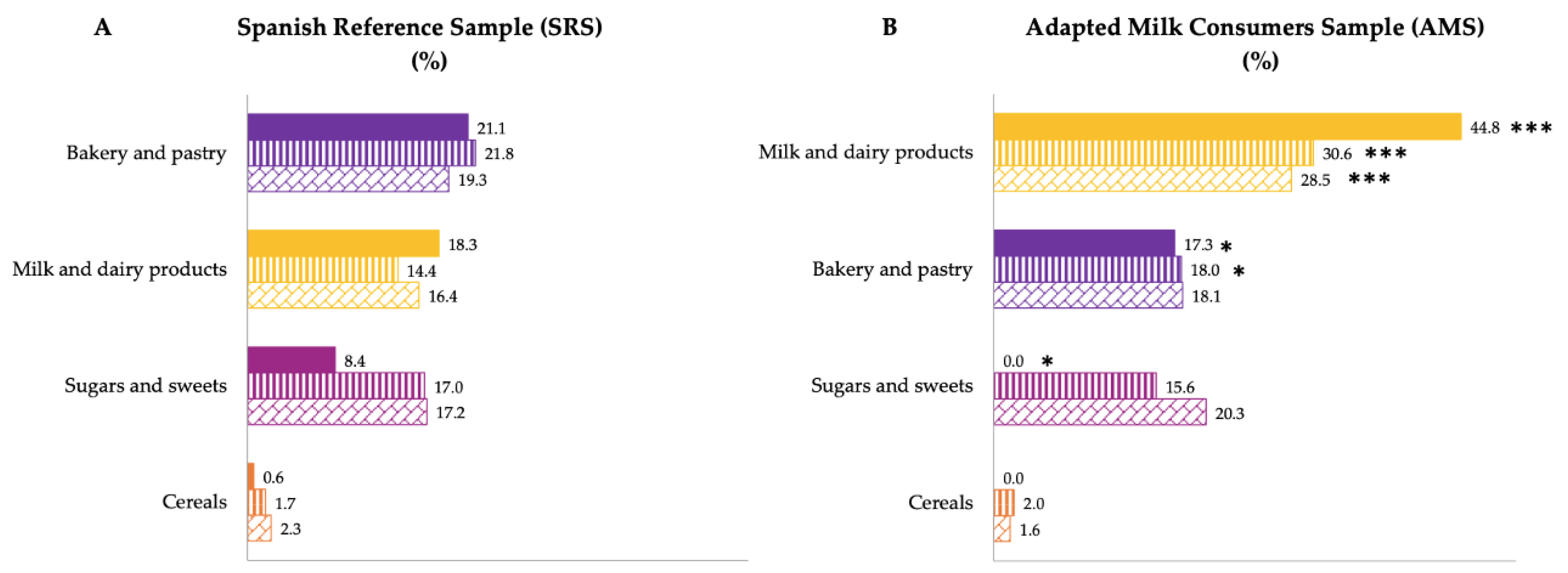
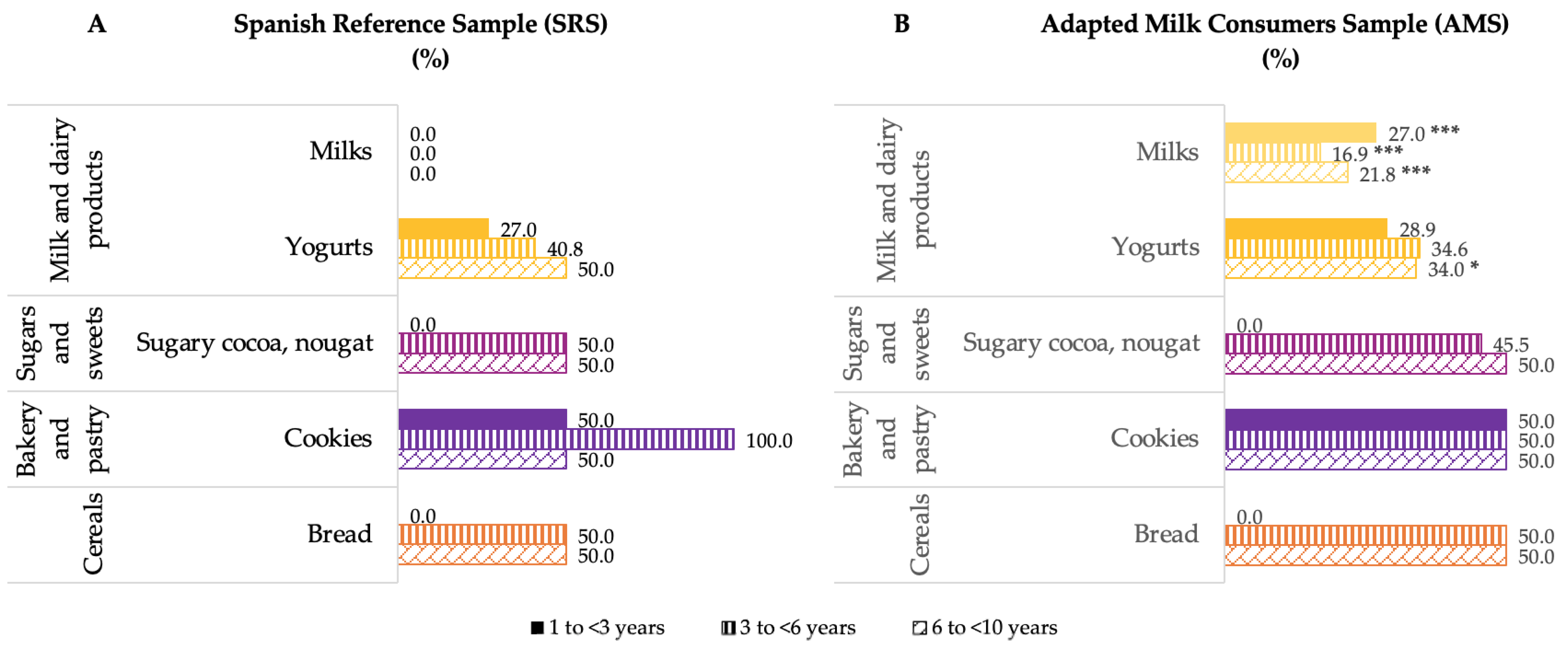
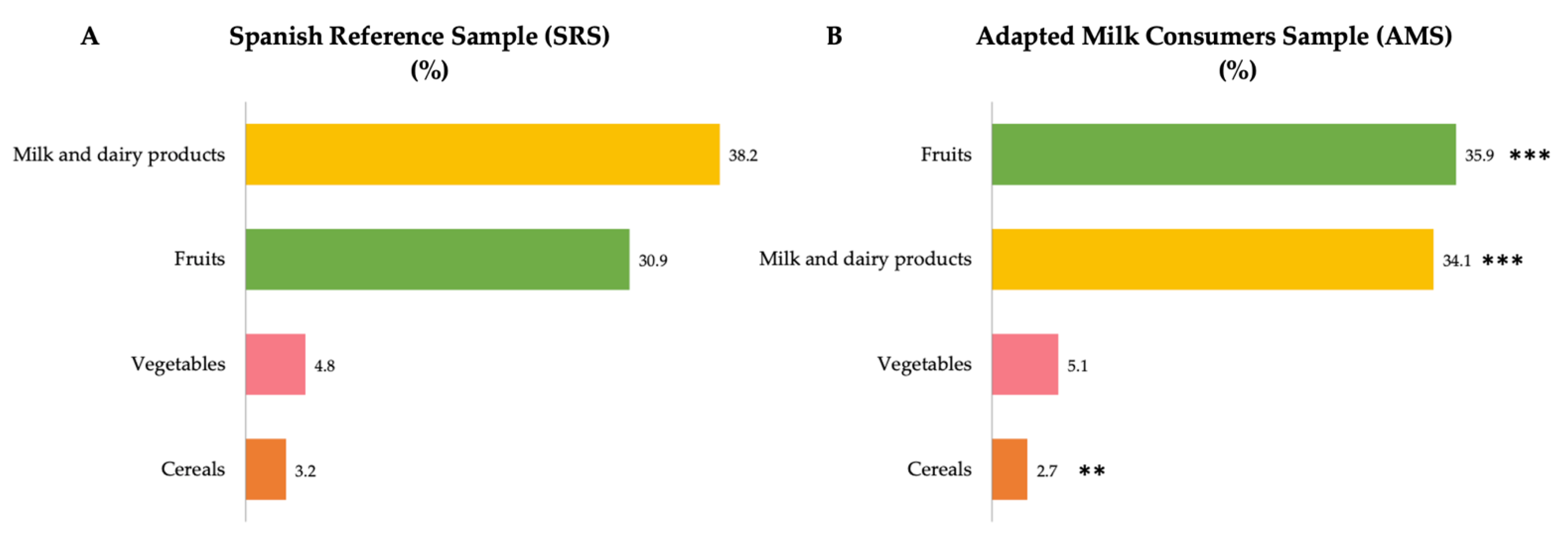
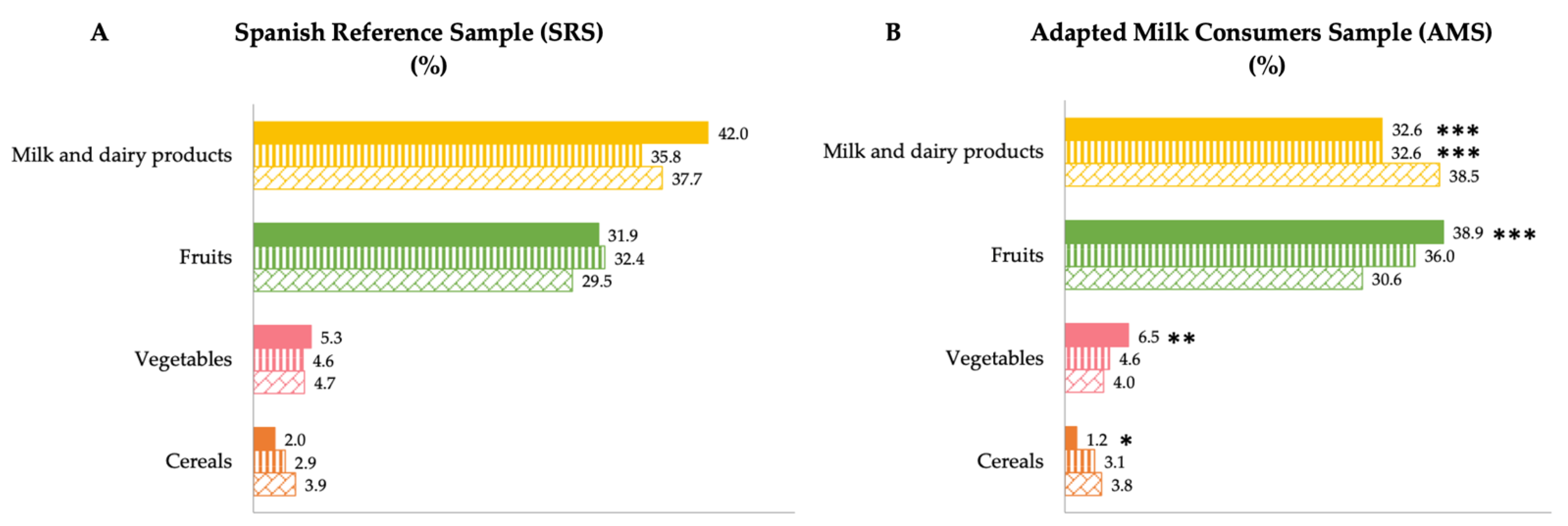
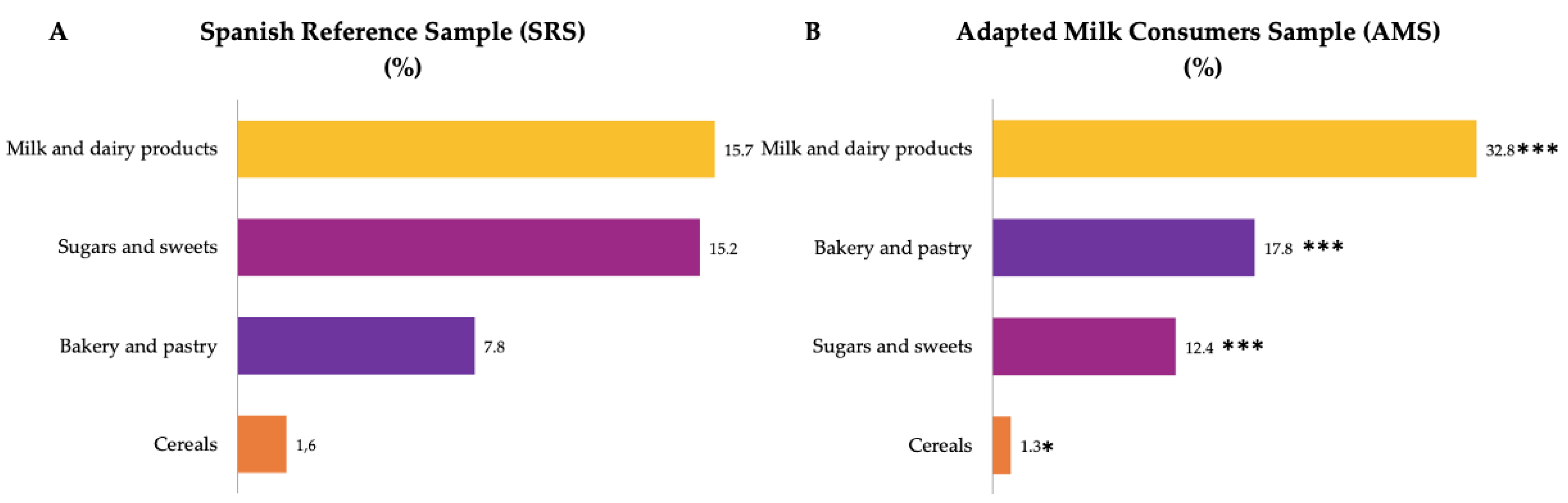
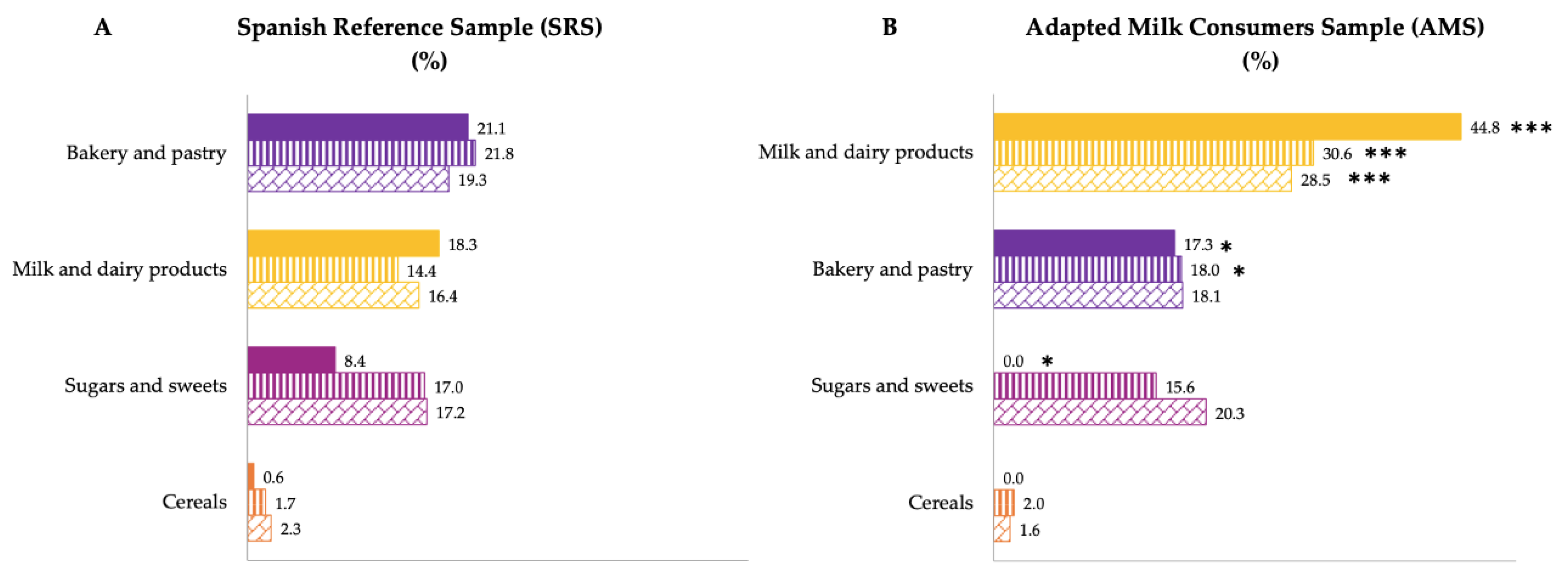
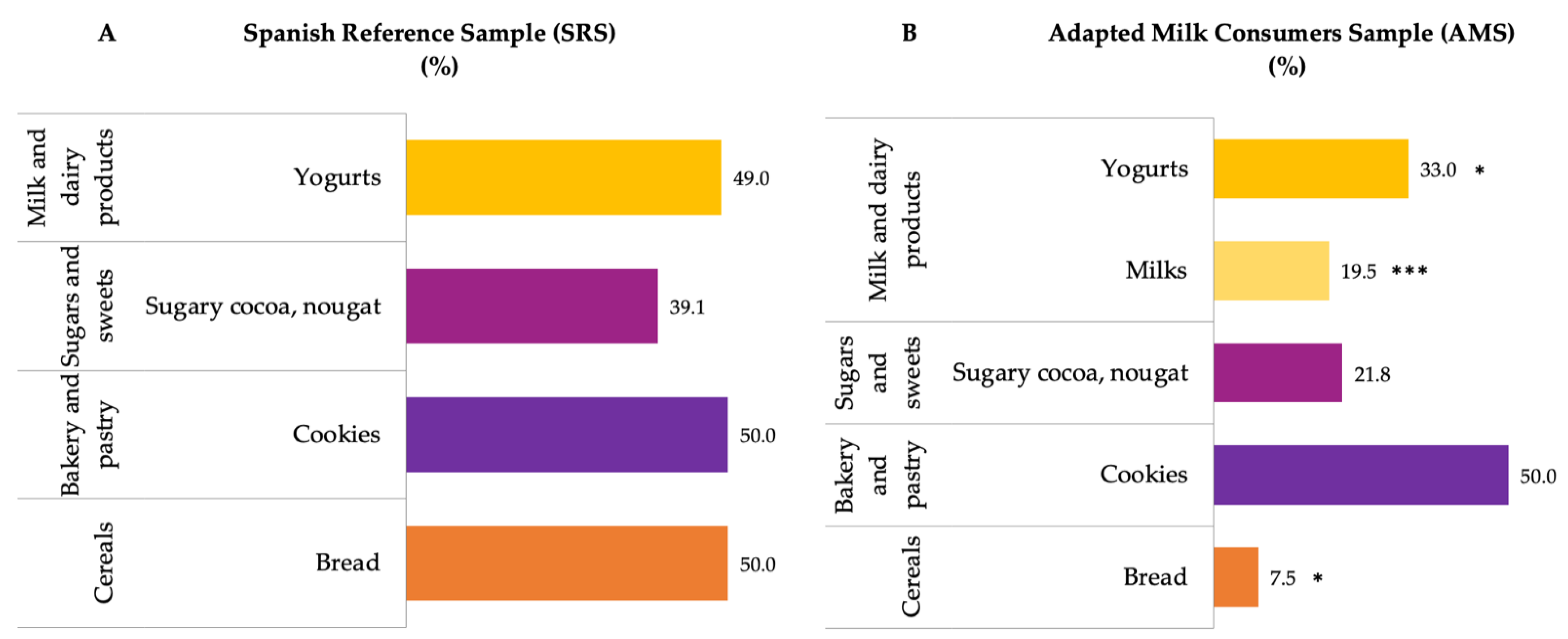
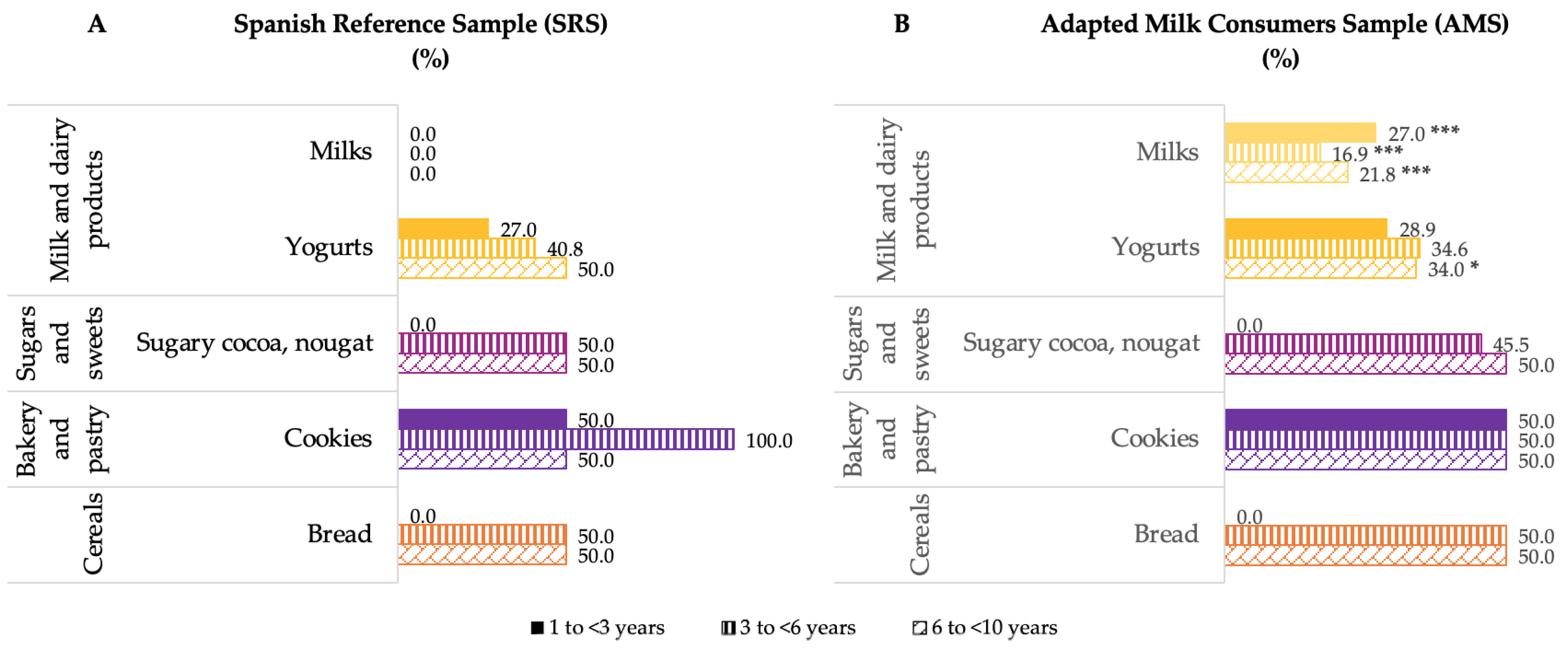
3.2. Contribution of Food and Beverage Groups to Reported Intakes of Intrinsic and Added Sugar
4. Discussion
4.1. Usual Intrinsic and Added Sugar Intake in Children
4.2. Contribution of Food and Beverage Groups to Reported Intakes of Intrinsic and Added Sugars
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Estudio ALADINO 2019: Estudio Sobre Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España 2019. Agencia Española de Seguridad Alimentaria y Nutrición. Ministerio de Consumo. Madrid, 2020. 2020. Available online: https://www.aesan.gob.es/AECOSAN/web/subhomes/nutricion/aecosan_nutricion.htm (accessed on 10 June 2021).
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- Stanner, S.A.; Spiro, A. Public health rationale for reducing sugar: Strategies and challenges. Nutr. Bull. 2020, 45, 253–270. [Google Scholar] [CrossRef]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A. Sugar in Infants, Children and Adolescents: A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatric Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies. Scientific opinion on dietary reference values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar]
- SACN Carbohydrates and Health Report. The Scientific Advisory Committee on Nutrition Recommendations on Carbohydrates, Including Sugars and Fibre; Public Health England: Norwich, England, 2015. [Google Scholar]
- Services, Department of Agriculture of United States of America USDA. Dietary Guidelines for Americans, 2020–2025. Available online: https://www.dietaryguidelines.gov/ (accessed on 1 July 2021).
- Agencia Española de Seguridad Alimentaria (AESAN). Informe de revisión y actualización de las recomendaciones dietéticas para la población española. Rev. Com. Científico AESAN 2020, 32, 11–57. [Google Scholar]
- Agencia Española de Seguridad Alimentaria (AESAN). Informe sobre objetivos y recomendaciones nutricionales y de actividad física frente a la obesidad en la estrategia NAOS. Rev. Com. Científico AESAN 2014, 19, 95–201. [Google Scholar]
- Gil, Á.; Urrialde, R.; Varela-Moreiras, G. Posicionamiento sobre la definición de azúcares añadidos y su declaración en el etiquetado de los productos alimenticios en España. Nutr. Hosp. 2021, 38, 645–660. [Google Scholar]
- Food and Drug Administration (FDA). Added Sugars: Now Included on the Nutrition Facts Label. Available online: https://www.fda.gov/media/137912/download (accessed on 1 April 2022).
- Ministry of Economy (Mexico). Modification to the Mexican official standard NOM-051-SCFISSAI-2010, General labelling specifi-cations for pre-packaged food and non-alcoholic beverages. Off. J. 2010, 27, 4–40. [Google Scholar]
- EFSA Panel on Nutrition Novel Foods and Food Allergens (NDA). Scientific Opinion advising on the development of harmonised mandatory front-of-pack nutrition labelling and the setting of nutrient profiles for restricting nutrition and health claims on foods. EFSA J. 2021. [Google Scholar]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Ávila, J.M.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary intake of individual (free and intrinsic) sugars and food sources in the Spanish population: Findings from the ANIBES study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Sobaler, A.M.; Aparicio, A.; Rubio, J.; Marcos, V.; Sanchidrián, R.; Santos, S.; Pérez-Farinós, N.; Dal-Re, M.Á.; Villar-Villalba, C.; Yusta-Boyo, M.J. Adequacy of usual macronutrient intake and macronutrient distribution in children and adolescents in Spain: A National Dietary Survey on the Child and Adolescent Population, ENALIA 2013–2014. Eur. J. Nutr. 2019, 58, 705–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agencia Españoma de Seguridad Aliemntaria (AESAN). Collaboration Plan for the Improvement of the Composition of Food and Beverages and Other Measures. 2020. Available online: http://www.aecosan.msssi.gob.es/AECOSAN/docs/documentos/nutricion/Plan_Colaboracion_INGLES.pdf (accessed on 6 June 2021).
- The European Parliament and of the Council. Regulation (EC) no 1924/2006 of the European Parliament and of the Council of 20 December 2006 on Nutrition and Health Claims Made on Foods, the Official Journal of the European Union Intellectual Property Office. 2006. Available online: https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A32006R1924 (accessed on 22 March 2022).
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Ruiz, E.; Valero, T.; Ávila, J.M.; Lara-Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study. Nutrients 2019, 11, 3050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de Crecimiento de Bilbao. Curvas y Tablas de Crecimiento. Estudio Transversal; Fundación Faustino Orbegozo: Bilbao, Spain, 2011. [Google Scholar]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Valero, T.; Ávila, J.M.; Ruiz, E.; Villoslada, F.L.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Energy Intake, Macronutrient Profile and Food Sources of Spanish Children Aged One to <10 Years-Results from the EsNuPI Study. Nutrients 2020, 12, 893. [Google Scholar] [CrossRef] [Green Version]
- Fundación Española de la Nutrición (FEN). Tablas de Medidas Caseras y Raciones Habituales de Consumo. Fundación Española de la Nutrición; FEN: Madrid, Spain, 2013. [Google Scholar]
- López, R.; Martínez de Victoria, E.; Gil, A. Guía Fotográfica de Porciones de Alimentos Consumidos en España. Fundación Iberoamericana de Nutrición. Universidad de Granada: Granada, Spain, 2019. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 19th ed.; Pirámide: Madrid, Spain, 2018. [Google Scholar]
- The European Parliament and of the Council. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004. Off. J. Eur. Union. 2011, 304, 18–63. [Google Scholar]
- Amoutzopoulos, B.; Steer, T.; Roberts, C.; Collins, D.; Page, P. Free and added sugar consumption and adherence to guidelines: The UK National Diet and Nutrition Survey (2014/15–2015/16). Nutrients 2020, 12, 393. [Google Scholar] [CrossRef] [Green Version]
- Marinho, A.R.; Severo, M.; Correia, D.; Lobato, L.; Vilela, S.; Oliveira, A.; Ramos, E.; Torres, D.; Lopes, C. Total, added and free sugar intakes, dietary sources and determinants of consumption in Portugal: The National Food, Nutrition and Physical Activity Survey (IAN-AF 2015–2016). Public Health Nutr. 2020, 23, 869–881. [Google Scholar] [CrossRef]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [Green Version]
- Graffe, M.I.M.; Pala, V.; De Henauw, S.; Eiben, G.; Hadjigeorgiou, C.; Iacoviello, L.; Intemann, T.; Jilani, H.; Molnar, D.; Russo, P.; et al. Dietary sources of free sugars in the diet of European children: The IDEFICS Study. Eur. J. Nutr. 2020, 59, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Sluik, D.; Van Lee, L.; Engelen, A.I.; Feskens, E.J. Total, free, and added sugar consumption and adherence to guidelines: The Dutch National Food Consumption Survey 2007–2010. Nutrients 2016, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C.Y. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newens, K.J.; Walton, J. A review of sugar consumption from nationally representative dietary surveys across the world. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2016, 29, 225–240. [Google Scholar] [CrossRef] [Green Version]
- Herrick, K.A.; Fryar, C.D.; Hamner, H.C.; Park, S.; Ogden, C.L. Added Sugars Intake among US Infants and Toddlers. J. Acad. Nutr. Diet. 2020, 120, 23–32. [Google Scholar] [CrossRef]
- World Health Organization. Fact Sheets, Details, Obesity and Overweight, Facing a Double Burden of Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 22 March 2022).
- Williams, A.S.; Ge, B.; Petroski, G.; Kruse, R.L.; McElroy, J.A.; Koopman, R.J. Socioeconomic Status and Other Factors Associated with Childhood Obesity. J. Am. Board Fam. Med. 2018, 31, 514–521. [Google Scholar] [CrossRef] [Green Version]
- de Bont, J.; Díaz, Y.; Casas, M.; García-Gil, M.; Vrijheid, M.; Duarte-Salles, T. Time Trends and Sociodemographic Factors Associated with Overweight and Obesity in Children and Adolescents in Spain. JAMA Netw. Open 2020, 3, e201171. [Google Scholar] [CrossRef] [Green Version]
- Ocké, M.; de Boer, E.; Brants, H.; van der Laan, J.; Niekerk, M.; van Rossum, C.; Temme, L.; Freisling, H.; Nicolas, G.; Casagrande, C. PANCAKE–Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe. EFSA Supporting Publ. 2012, 9, 339E. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age Group | Boys | Girls | |||
|---|---|---|---|---|---|---|
| n | Median (P25–P75) | n | Median (P25–P75) | |||
| Intrinsic Sugars (g/day) | SRS | 1 to <3 years | 84 | 64.45 (55.1–81.2) | 78 | 64.9 (48.5–81.8) |
| 3 to <6 years | 122 | 64.8 (49.6–77.2) | 122 | 65.8 (52.3–81.5) | ||
| 6 to <10 years | 151 | 67.4 (52.8–82.4) | 150 | 60.7 (47.6–71.9) | ||
| AMS | 1 to <3 years | 144 | 59.4 (48.1–79.6) | 150 | 56.5 (48.7–72.0) * | |
| 3 to <6 years | 128 | 64.4 (53.3–77.4) | 134 | 63.1 (51.4–76.7) | ||
| 6 to <10 years | 99 | 67.5 (49.6–81.8) | 86 | 67.2 (45.7–79.6) | ||
| Added Sugars (g/day) | SRS | 1 to <3 years | 84 | 37.0 (27.8–47.3) | 78 | 36.9 (26.0–42.1), |
| 3 to <6 years | 122 | 37.4 (29.2–46.6) | 122 | 37.2 (28.6–45.7) | ||
| 6 to <10 years | 151 | 41.4 (28.8–52.8) | 150 | 35.9 (26.1–46.7) | ||
| AMS | 1 to <3 years | 144 | 33.8 (26.0–46.1) a | 150 | 32.7 (26.1–40.7) *,a | |
| 3 to <6 years | 128 | 38.6 (30.1–48.3) a,b | 134 | 38.6 (29.8–46.7) b | ||
| 6 to <10 years | 99 | 40.1 (31.2–51.4) b | 86 | 42.9 (28.4–53.3) b | ||
| Group | Age Group | Boys | Girls | |||
|---|---|---|---|---|---|---|
| n | Median (P25–P75) | n | Median (P25–P75) | |||
| Added sugars (%) | SRS | 1 to <3 years | 84 | 12.5 (9.0–15.4) a | 78 | 11.7 (9.1–15.3) a |
| 3 to <6 years | 122 | 10.1 (7.8–12.6) b | 122 | 10.1 (8.6–12.1) a,b | ||
| 6 to <10 years | 151 | 10.1 (7.0–12.1) b | 150 | 9.4 (7.2–11.9) b | ||
| AMS | 1 to <3 years | 144 | 12.2 (9.3–15.7) a | 150 | 11.3 (8.9–14.8) a | |
| 3 to <6 years | 128 | 11.0 (8.3–13.0) b | 134 | 10.3 (8.6–12.3) b | ||
| 6 to <10 years | 99 | 9.8 (7.9–12.5) b | 86 | 11.0 (8.1–12.9) *,a,b | ||
| Group | Age Group | Boys | Girls | |||
|---|---|---|---|---|---|---|
| n | % <10% Total Energy Intake | n | % <10% Total Energy Intake | |||
| Added sugars (%) | SRS | 1 to <3 years | 84 | 27.4 | 78 | 37.2 |
| 3 to <6 years | 122 | 49.2 | 122 | 46.7 | ||
| 6 to <10 years | 151 | 49.7 | 150 | 58.0 | ||
| AMS | 1 to <3 years | 144 | 31.3 | 150 | 34.7 | |
| 3 to <6 years | 128 | 40.6 | 134 | 44.8 | ||
| 6 to <10 years | 99 | 53.5 | 86 | 39.5 * | ||
| Group | Age Group | Boys | Girls | |||
|---|---|---|---|---|---|---|
| n | % <5% Total Energy Intake | n | % <5% Total Energy Intake | |||
| Added sugars (%) | SRS | 1 to <3 years | 84 | 0.0 | 78 | 2.6 |
| 3 to <6 years | 122 | 6.6 | 122 | 3.3 | ||
| 6 to <10 years | 151 | 6.0 | 150 | 7.3 | ||
| AMS | 1 to <3 years | 144 | 1.4 | 150 | 3.3 | |
| 3 to <6 years | 128 | 4.7 | 134 | 1.5 | ||
| 6 to <10 years | 99 | 6.1 | 86 | 2.3 | ||
| Group | Age Group | Underweight (%) | Normal Weight (%) | Overweight (%) | Obesity (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | |||
| Added Sugars (g/day) | SRS | 1 to <3 years | 51 | 36.9 (27.6–45.6) | 153 | 37.2 (28.3–43.1) | 30 | 37.2 (25.4–48.8) | 28 | 39.7 (27.9–46.1) |
| 3 to <6 years | 27 | 32.3 (22.9–46.8) * | 131 | 35.3 (28.2–49.0) | 36 | 41.8 (30.4–55.2) | 17 | 39.8 (24.5–49.5) | ||
| 6 to <10 years | 41 | 35.0 (24.7–47.3) | 149 | 39.6 (28.4–50.5) | 40 | 37.5 (29.2–59.3) | 4 | 30.0 (11.1–58.4) | ||
| AMS | 1 to <3 years | 69 | 34.1 (27.6– 42.8) | 234 | 34.8 (26.8–46.2) | 68 | 34.3 (26.5–42.9) | 43 | 34.0 (29.1–41.6) | |
| 3 to <6 years | 36 | 41.2 (33.0–56.1) | 116 | 38.7 (30.6–50.6) | 22 | 39.3 (31.8–49.4) | 12 | 40.5 (28.8–45.2) | ||
| 6 to <10 years | 23 | 41.8 (23.9–48.5) | 89 | 42.8 (30.5–52.2) | 27 | 36.7 (27.5–51.6) | 2 | 34.5 (25.4–no data) | ||
| Group | Age Group | DK/NO | <600€ Per Month | 600–1000€ Per Month | 1001–1500€ Per Month | 1501–2000€ Per Month | 2001–3000€ Per Month | 3001–4000€ Per Month | >4000€ Per Month | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | n | Median (P25–P75) | |||
| Added Sugars (g/day) | SRS | 1 to <3 years | 68 | 38.7 (28.2–46.5) | 11 | 35.7 (23.2–39.4) | 17 | 33.5 (28.6–44.4) | 43 | 37.5 (26.2–43.9) | 49 | 36.2 (27.5–46.0) | 47 | 38.7 (29.6–44.0) | 25 | 33.2 (25.3–43.7) | 2 | 36.1 (34.5–no data) |
| 3 to <6 years | 57 | 35.3 (25.3–48.0) | 6 | 38.3 (21.8–55.1) | 12 | 42.1 (21.4–59.6) | 27 | 40.7 (32.7–57.2) | 34 | 40.4 (30.1–51.0) | 55 | 31.0 * (24.4–48.3) | 17 | 38.6 (24.2–45.4) | 3 | 35.0 (27.2–no data) | ||
| 6 to <10 years | 59 | 34.6 (24.1–45.9) | 13 | 42.8 (35.2–53.1) | 10 | 38.0 (35.8–43.5) | 32 | 30.3 (27.4–39.3) | 43 | 41.3 (30.0–56.2) | 58 | 43.2 (28.8–55.8) | 17 | 41.4 (32.4–53.3) | 2 | 42.0 (23.1–no data) | ||
| AMS | 1 to <3 years | 111 | 35.2 (28.7–47.3) | 8 | 34.5 (26.6–45.6) | 28 | 31.0 (26.1–45.7) | 45 | 33.4 (25.8–41.4) | 88 | 33.5 (26.6–44.3) | 96 | 34.1 (26.9–46.2 | 36 | 31.1 (24.6–42.1) | 2 | 42.2 (29.5–no data) | |
| 3 to <6 years | 61 | 38.7 (32.5–51.9) | 6 | 39.8 (35.6–62.6) | 13 | 42.7 (30.8–49.5) | 23 | 33.1 (26.3–44.7) | 21 | 43.4 (25.5–57.7) | 43 | 40.6 (33.3–53.1) | 17 | 41.6 (38.6–47.3) | 2 | 36.0 (24.0–no data) | ||
| 6 to <10 years | 34 | 43.1 (30.5–52.2) | 2 | 61.3 (38.2–no data) | 11 | 40.1 (20.5–64.8) | 27 | 32.9 (25.4–44.6) | 25 | 43.4 (33.8–50.8) | 34 | 43.1 (33.9–52.8) | 6 | 52.5 (21.1–62.1) | 2 | 30.8 (23.3–no data) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redruello-Requejo, M.; Samaniego-Vaesken, M.d.L.; Partearroyo, T.; Rodríguez-Alonso, P.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Villoslada, F.L.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients 2022, 14, 1667. https://doi.org/10.3390/nu14081667
Redruello-Requejo M, Samaniego-Vaesken MdL, Partearroyo T, Rodríguez-Alonso P, Soto-Méndez MJ, Hernández-Ruiz Á, Villoslada FL, Leis R, Martínez de Victoria E, Moreno JM, et al. Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients. 2022; 14(8):1667. https://doi.org/10.3390/nu14081667
Chicago/Turabian StyleRedruello-Requejo, Marina, María de Lourdes Samaniego-Vaesken, Teresa Partearroyo, Paula Rodríguez-Alonso, María José Soto-Méndez, Ángela Hernández-Ruiz, Federico Lara Villoslada, Rosaura Leis, Emilio Martínez de Victoria, José Manuel Moreno, and et al. 2022. "Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study" Nutrients 14, no. 8: 1667. https://doi.org/10.3390/nu14081667
APA StyleRedruello-Requejo, M., Samaniego-Vaesken, M. d. L., Partearroyo, T., Rodríguez-Alonso, P., Soto-Méndez, M. J., Hernández-Ruiz, Á., Villoslada, F. L., Leis, R., Martínez de Victoria, E., Moreno, J. M., Ortega, R. M., Ruiz-López, M. D., Gil, Á., & Varela-Moreiras, G. (2022). Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients, 14(8), 1667. https://doi.org/10.3390/nu14081667