
The Impact of Consuming Zinc-Biofortified Wheat Flour on Haematological Indices of Zinc and Iron Status in Adolescent Girls in Rural Pakistan: A Cluster-Randomised, Double-Blind, Controlled Effectiveness Trial

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
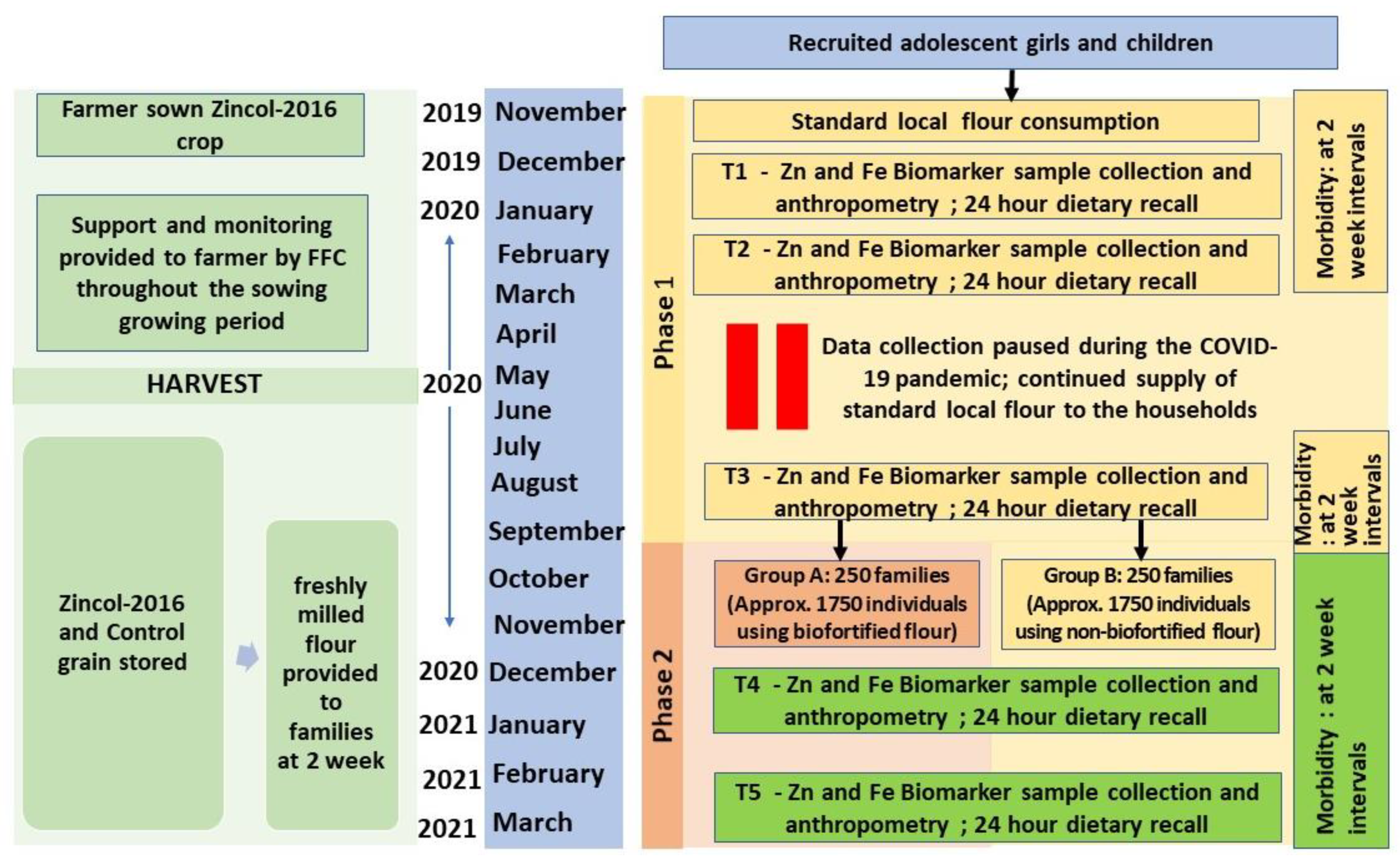
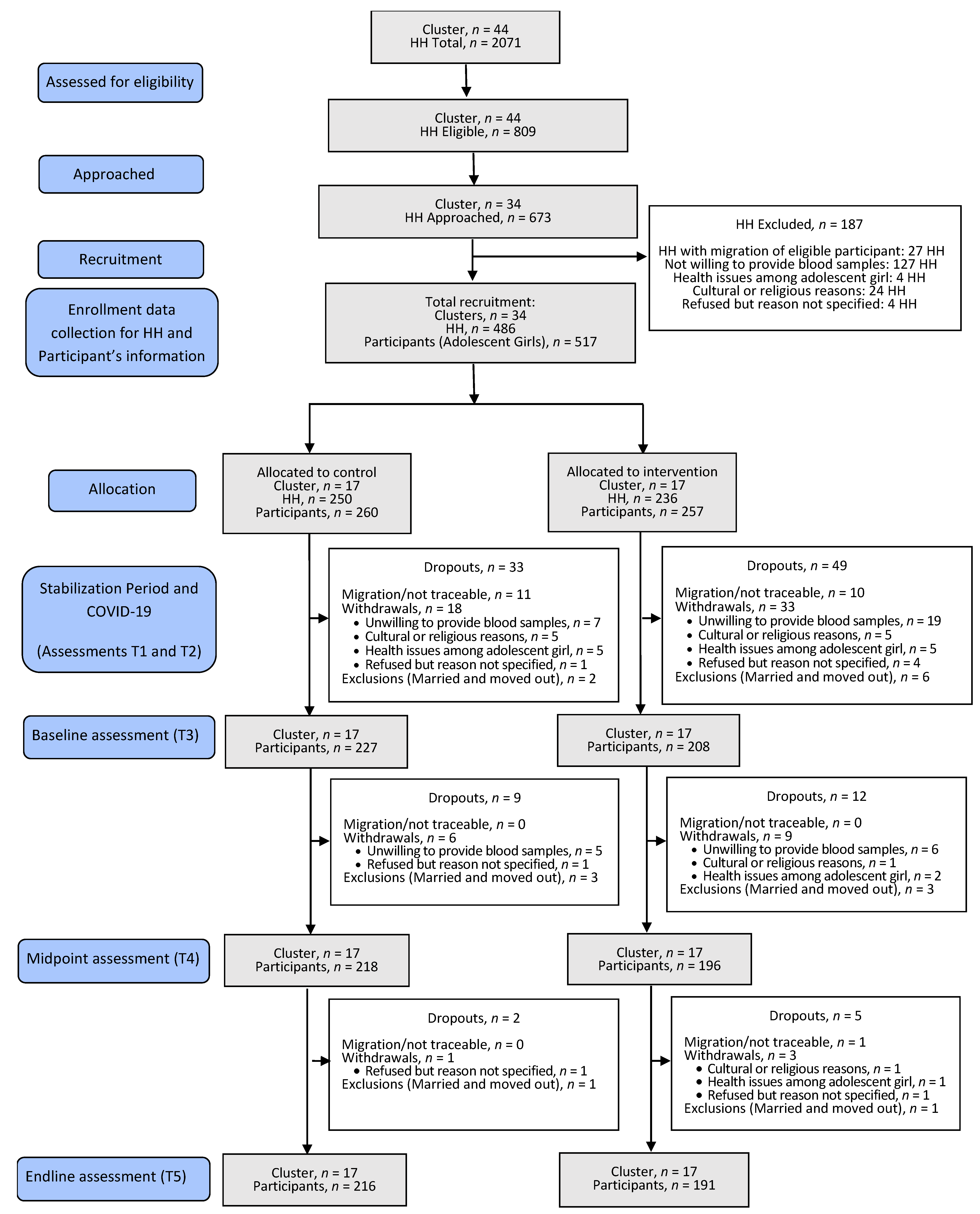
2.1. Setting, Participant Recruitment and Study Design
2.2. Masking
2.3. Local Production of Zincol-2016 Grain for the Intervention
2.4. Mineral Analysis of Grain and Flour
2.5. Field Procedures
Participant Characteristics, Blood Sample and Diet Data Collection Procedures
2.6. Lab Procedures
2.6.1. Haematology
2.6.2. Mineral Analysis
2.6.3. Inflammatory Markers and Iron Status
2.6.4. Adjustments for Inflammation and Cut-Offs for Defining Deficiencies
2.7. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Grain and Flour Analysis
3.3. Impact of Intervention
3.3.1. Contribution to Daily Zinc Intake from Wheat Flour
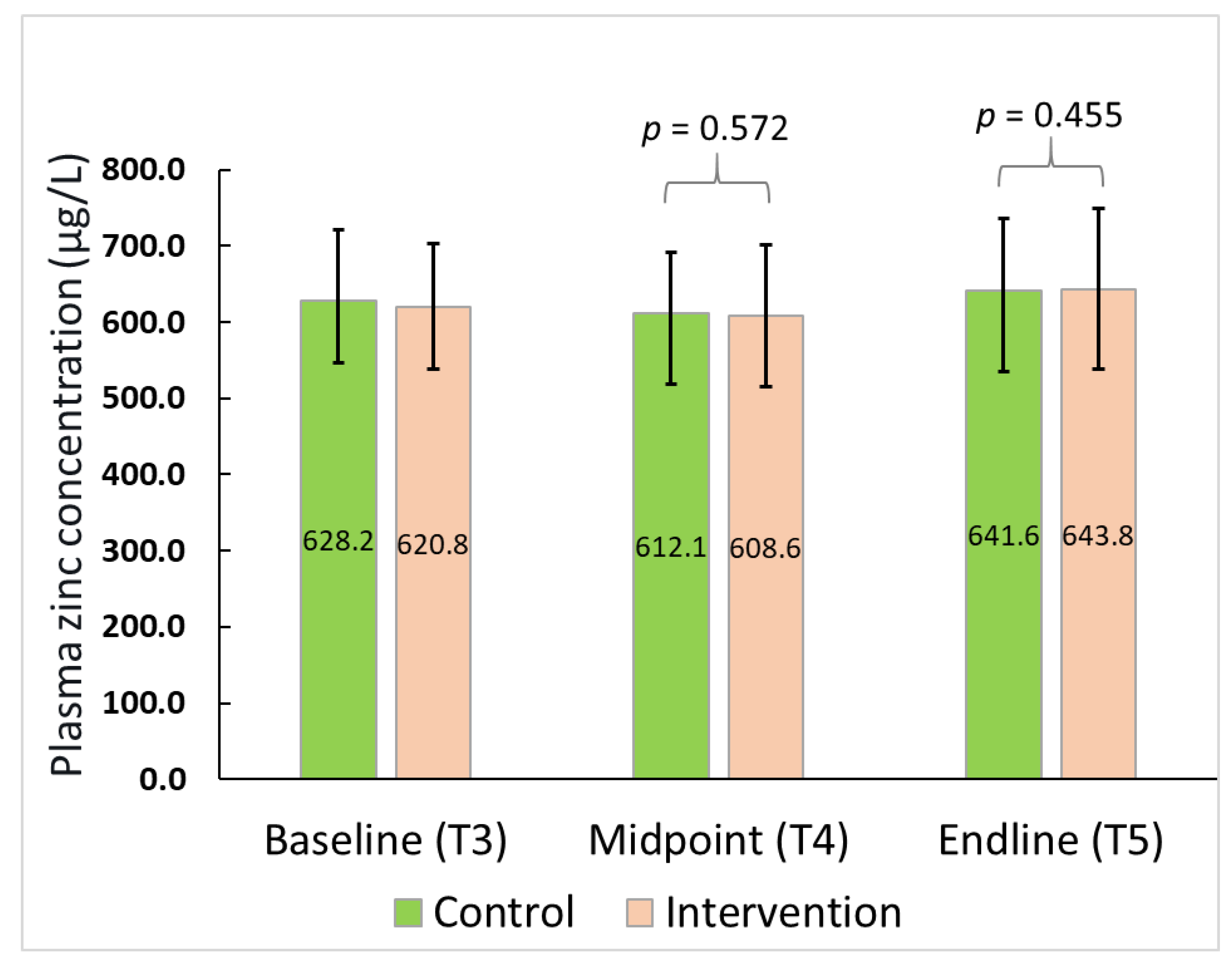
3.3.2. Plasma Zinc Concentration and Prevalence of Zinc Deficiency
3.3.3. Haematology and Adverse Effect
3.3.4. Iron Status
3.3.5. Other Mineral (Selenium and Copper) Status and Inflammatory Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Element | Copper | Zinc | Selenium |
|---|---|---|---|
| Limit of detection (µg/L) | 0.074 | 0.941 | 0.010 |
| Limit of quantification (µg/L) | 0.248 | 3.136 | 0.033 |
| CRM % Recovery | Copper | Zinc | Selenium |
|---|---|---|---|
| Seronorm L-1 (n = 25) | 86.5 | 89.4 | 102.2 |
| Seronorm L-2 (n = 26) | 86.8 | 86.0 | 103.4 |
References
- United Nation Department of Economic and Social Affairs. Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 4 March 2022).
- WHO. Guidelines on Food Fortification with Micronutrients; Allen, L., de Benoist, B., Dary, O., Hurrell, R., Eds.; World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/handle/10665/43412 (accessed on 4 March 2022).
- Wessells, K.R.; Brown, K.H. Estimating the Global Prevalence of Zinc Deficiency: Results Based on Zinc Availability in National Food Supplies and the Prevalence of Stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lönnerdal, B.; Ruel, M.T.; Sandtröm, B.; Wasantwisut, E.; Hotz, C. International zinc nutrition consultative group (izincg) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar] [PubMed]
- Lowe, N.M. Assessing zinc in humans. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Government of Pakistan; UNICEF. National Nutrition Survey 2018. Full Report (3 Volumes) & Key Findings Report. Available online: https://www.unicef.org/pakistan/reports/national-nutrition-survey-2018-full-report-3-volumes-key-findings-report (accessed on 4 March 2022).
- Brazier, A.K.M.; Lowe, N.M.; Zaman, M.; Shahzad, B.; Ohly, H.; McArdle, H.J.; Ullah, U.; Broadley, M.R.; Bailey, E.H.; Young, S.D.; et al. Micronutrient Status and Dietary Diversity of Women of Reproductive Age in Rural Pakistan. Nutrients 2020, 12, 3407. [Google Scholar] [CrossRef]
- Liere, M.V.; Bhutta, Z.A.; Hartvig-Blomberg, J.; Mahmood, S. Embodying the Future: How to Improve the Nutrition Status of Adolescent Girls in Pakistan?; Global Alliance for Improved Nutrition (GAIN). 2017. Available online: https://www.gainhealth.org/sites/default/files/publications/documents/embodying-the-future-how-to-improve-the-nutrition-status-of-adolescent-girls-in-pakistan.pdf (accessed on 6 March 2022).
- Gupta, S.; Brazier, A.K.M.; Lowe, N.M. Zinc deficiency in low- and middle-income countries: Prevalence and approaches for mitigation. J. Hum. Nutr. Diet. 2020, 33, 624–643. [Google Scholar] [CrossRef]
- e-Pact Consortium. Evaluation of the Supporting Nutrition in Pakistan Food Fortification Programme. Midterm Evaluation Report May 2019. Available online: https://www.opml.co.uk/files/2021-07/mid-term-evaluation-report-food-fortification-programme.pdf?noredirect=1 (accessed on 6 March 2022).
- Lowe, N.M.; Zaman, M.; Khan, M.J.; Brazier, A.K.M.; Shahzad, B.; Ullah, U.; Khobana, G.; Ohly, H.; Broadley, M.R.; Zia, M.H.; et al. Biofortified Wheat Increases Dietary Zinc Intake: A Randomised Controlled Efficacy Study of Zincol-2016 in Rural Pakistan. Front. Nutr. 2022, 8, 809783. [Google Scholar] [CrossRef]
- Rehman, A.; Farooq, M.; Ullah, A.; Nadeem, F.; Im, S.Y.; Park, S.K.; Lee, D.-J. Agronomic Biofortification of Zinc in Pakistan: Status, Benefits, and Constraints. Front. Sustain. Food Syst. 2020, 4, 591722. [Google Scholar] [CrossRef]
- Campbell, M.K.; Elbourne, D.R.; Altman, D.G. CONSORT statement: Extension to cluster randomised trials. BMJ 2004, 328, 702–708. [Google Scholar] [CrossRef] [Green Version]
- Lowe, N.M.; Zaman, M.; Moran, V.H.; Ohly, H.; Sinclair, J.; Fatima, S.; Broadley, M.R.; Joy, E.J.M.; Mahboob, U.; Lark, R.M.; et al. Biofortification of wheat with zinc for eliminating deficiency in Pakistan: Study protocol for a cluster-randomised, double-blind, controlled effectiveness study (BIZIFED2). BMJ Open 2020, 10, e039231. [Google Scholar] [CrossRef]
- Hemming, K.; Taljaard, M. Sample size calculations for stepped wedge and cluster randomised trials: A unified approach. J. Clin. Epidemiol. 2016, 69, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, S.M.; Ashby, D.; Kerry, S. Sample size for cluster randomized trials: Effect of coefficient of variation of cluster size and analysis method. Int. J. Epidemiol. 2006, 35, 1292–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.J.; Donner, A.; Klar, N. Developments in cluster randomized trials andStatistics in Medicine. Stat. Med. 2007, 26, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Donner, A.; Klar, N. Pitfalls of and Controversies in Cluster Randomization Trials. Am. J. Public Health 2004, 94, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Zia, M.H.; Ahmed, I.; Bailey, E.H.; Lark, R.M.; Young, S.D.; Lowe, N.M.; Joy, E.J.M.; Wilson, L.; Zaman, M.; Broadley, M.R. Site-Specific Factors Influence the Field Performance of a Zn-Biofortified Wheat Variety. Front. Sustain. Food Syst. 2020, 4, 135. [Google Scholar] [CrossRef]
- Gibson, R.S.; Ferguson, E.L. An Interactive 24-h Recall for Assessing the Adequacy of Iron and Zinc Intakes in Developing Countries; International Food Policy Research Institute (IFPRI) and International Center for Tropical Agriculture (CIAT): Washington, DC, USA; Cali, CA, USA, 2008; Available online: https://www.harvestplus.org/node/544 (accessed on 7 March 2022).
- Badrick, T. Quality leadership and quality control. Clin. Biochem. Rev. 2003, 24, 81–93. [Google Scholar]
- IZiNCG. Adjusting Plasma or Serum Zinc Concentrations for Inflammation International Zinc Nutrition Consultative Group Technical Brief No. 10. 2020. Available online: https://static1.squarespace.com/static/56424f6ce4b0552eb7fdc4e8/t/5e9dff7f491e4343279045b8/1587412866032/IZiNCG_Technical+Brief+BRINDA_20Apr2020_final.pdf (accessed on 7 March 2022).
- World Health Organization. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240000124 (accessed on 7 March 2022).
- Thurnham, D.I.; McCabe, L.D.; Haldar, S.; Wieringa, F.T.; Northrop-Clewes, C.A.; McCabe, G.P. Adjusting plasma ferritin concentrations to remove the effects of subclinical inflammation in the assessment of iron deficiency: A meta-analysis. Am. J. Clin. Nutr. 2010, 92, 546–555. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, F.; Khan, M.R.; Islam, M.; Kabir, I.; Fuchs, G.J. Anaemia and iron deficiency among adolescent schoolgirls in peri-urban Bangladesh. Eur. J. Clin. Nutr. 2000, 54, 678–683. [Google Scholar] [CrossRef] [Green Version]
- WHO. Serum Transferrin Receptor Levels for the Assessment of Iron Status and Iron Deficiency in Populations; WHO/NMH/NHD/EPG/14.6; World Health Organization: Geneva, Switzerland, 2014; Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-EPG-14.6 (accessed on 7 March 2022).
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; No. WHO/NMH/NHD/MNM/11.1; World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/vmnis/indicators/haemoglobin.pdf (accessed on 7 March 2022).
- Lin, C.-N.; Wilson, A.; Church, B.B.; Ehman, S.; Roberts, W.L.; McMillin, G.A. Pediatric reference intervals for serum copper and zinc. Clin. Chim. Acta 2012, 413, 612–615. [Google Scholar] [CrossRef]
- Muntau, A.C.; Streiter, M.; Kappler, M.; Röschinger, W.; Schmid, I.; Rehnert, A.; Schramel, P.; Roscher, A.A. Age-related Reference Values for Serum Selenium Concentrations in Infants and Children. Clin. Chem. 2002, 48, 555–560. [Google Scholar] [CrossRef]
- CDC. Laboratory Procedure Manual. NHANES 2011–2012. Analyte: Complete Blood Count. Matrix: Whole Blood. Method: Complete Blood Count with 5-Part Differential. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/cbc_g_met_he.pdf (accessed on 7 March 2022).
- Longvah, T.; Ananthan, R.; Bhaskarachary, K.; Venkaiah, K. Indian Food Composition Tables; National Institute of Nutrition: Hyderabad, India, 2017. [Google Scholar]
- Liong, E.M.; McDonald, C.M.; Suh, J.; Westcott, J.L.; Wong, C.P.; Signorell, C.; King, J.C. Zinc-Biofortified Wheat Intake and Zinc Status Biomarkers in Men: Randomized Controlled Trial. J. Nutr. 2021, 151, 1817–1823. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.M.; Dykes, F.C.; Skinner, A.-L.; Patel, S.; Warthon-Medina, M.; Decsi, T.; Fekete, K.; Souverein, O.W.; Dullemeijer, C.; Cavelaars, A.E.; et al. EURRECA—Estimating Zinc Requirements for Deriving Dietary Reference Values. Crit. Rev. Food Sci. Nutr. 2013, 53, 1110–1123. [Google Scholar] [CrossRef] [PubMed]
- Jongstra, R.; Hossain, M.; Galetti, V.; Hall, A.G.; Holt, R.R.; Cercamondi, C.I.; Rashid, S.F.; Zimmermann, M.B.; Mridha, M.K.; Wegmueller, R. The effect of zinc-biofortified rice on zinc status of Bangladeshi preschool children: A randomized, double-masked, household-based, controlled trial. Am. J. Clin. Nutr. 2021, 115, 724–737. [Google Scholar] [CrossRef] [PubMed]
- Sazawal, S.; Dhingra, U.; Dhingra, P.; Dutta, A.; Deb, S.; Kumar, J.; Devi, P.; Prakash, A. Efficacy of high zinc biofortified wheat in improvement of micronutrient status, and prevention of morbidity among preschool children and women—A double masked, randomized, controlled trial. Nutr. J. 2018, 17, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zyba, S.J.; Shenvi, S.V.; Killilea, D.W.; Holland, T.C.; Kim, E.; Moy, A.; Sutherland, B.; Gildengorin, V.; Shigenaga, M.K.; King, J.C. A moderate increase in dietary zinc reduces DNA strand breaks in leukocytes and alters plasma proteins without changing plasma zinc concentrations. Am. J. Clin. Nutr. 2017, 105, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.; Bailey, E.H.; Arshad, M.; Ahmed, S.; Watts, M.J.; Stewart, A.G.; Young, S.D. Environmental and human iodine and selenium status: Lessons from Gilgit-Baltistan, North-East Pakistan. Environ. Geochem. Health 2021, 43, 4665–4686. [Google Scholar] [CrossRef]
- Haas, J.D.; Luna, S.V.; Lung’Aho, M.G.; Wenger, M.J.; Murray-Kolb, L.E.; Beebe, S.; Gahutu, J.B.; Egli, I.M. Consuming Iron Biofortified Beans Increases Iron Status in Rwandan Women after 128 Days in a Randomized Controlled Feeding Trial. J. Nutr. 2016, 146, 1586–1592. [Google Scholar] [CrossRef]
- Haas, J.D.; Beard, J.L.; Murray-Kolb, L.E.; Del Mundo, A.M.; Felix, A.; Gregorio, G.B. Iron-Biofortified Rice Improves the Iron Stores of Nonanemic Filipino Women. J. Nutr. 2005, 135, 2823–2830. [Google Scholar] [CrossRef]
- Murray-Kolb, L.E.; Wenger, M.; Scott, S.P.; Rhoten, S.E.; Lungaho, M.; Haas, J.D. Consumption of Iron-Biofortified Beans Positively Affects Cognitive Performance in 18- to 27-Year-Old Rwandan Female College Students in an 18-Week Randomized Controlled Efficacy Trial. J. Nutr. 2017, 147, 2109–2117. [Google Scholar] [CrossRef] [Green Version]
- Kodkany, B.S.; Bellad, R.; Mahantshetti, N.S.; Westcott, J.E.; Krebs, N.F.; Kemp, J.F.; Hambidge, K.M. Biofortification of Pearl Millet with Iron and Zinc in a Randomized Controlled Trial Increases Absorption of These Minerals above Physiologic Requirements in Young Children. J. Nutr. 2013, 143, 1489–1493. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, J.L.; Mehta, S.; Udipi, S.A.; Ghugre, P.S.; Luna, S.V.; Wenger, M.; Murray-Kolb, L.E.; Przybyszewski, E.M.; Haas, J.D. A Randomized Trial of Iron-Biofortified Pearl Millet in School Children in India. J. Nutr. 2015, 145, 1576–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceciliani, F.; Lecchi, C. The Immune Functions of α1Acid Glycoprotein. Curr. Protein Pept. Sci. 2019, 20, 505–524. [Google Scholar] [CrossRef] [PubMed]
- Karakochuk, C.D.; Barr, S.I.; Boy, E.; Bahizire, E.; Tugirimana, P.L.; Akilimali, P.Z.; Houghton, L.A.; Green, T.J. The effect of inflammation on serum zinc concentrations and the prevalence estimates of population-level zinc status among Congolese children aged 6–59 months. Eur. J. Clin. Nutr. 2017, 71, 1467–1470. [Google Scholar] [CrossRef]
- McDonald, C.M.; Suchdev, P.; Krebs, N.F.; Hess, S.Y.; Wessells, K.R.; Ismaily, S.; Rahman, S.; Wieringa, F.T.; Williams, A.M.; Brown, K.H.; et al. Adjusting plasma or serum zinc concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2020, 111, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Lauer, J.M.; McDonald, C.M.; Kisenge, R.; Aboud, S.; Fawzi, W.W.; Liu, E.; Tran, H.Q.; Gewirtz, A.T.; Manji, K.P.; Duggan, C.P. Markers of Systemic Inflammation and Environmental Enteric Dysfunction Are Not Reduced by Zinc or Multivitamins in Tanzanian Infants: A Randomized, Placebo-Controlled Trial. J. Pediatr. 2019, 210, 34–40.e31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousavi, S.M.; Djafarian, K.; Mojtahed, A.; Varkaneh, H.K.; Shab-Bidar, S. The effect of zinc supplementation on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pharmacol. 2018, 834, 10–16. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Shipley, M.J.; Bell, J.A.; Canonico, M.; Elbaz, A.; Kivimäki, M. Association between inflammatory biomarkers and all-cause, cardiovascular and cancer-related mortality. Can. Med. Assoc. J. 2017, 189, E384–E390. [Google Scholar] [CrossRef] [Green Version]
- Fischer, K.; Kettunen, J.; Würtz, P.; Haller, T.; Havulinna, A.S.; Kangas, A.; Soininen, P.; Esko, T.; Tammesoo, M.-L.; Mägi, R.; et al. Biomarker Profiling by Nuclear Magnetic Resonance Spectroscopy for the Prediction of All-Cause Mortality: An Observational Study of 17,345 Persons. PLoS Med. 2014, 11, e1001606. [Google Scholar] [CrossRef]
- Syed, S.; Manji, K.P.; McDonald, C.M.; Kisenge, R.; Aboud, S.; Sudfeld, C.; Locks, L.; Liu, E.; Fawzi, W.W.; Duggan, C.P. Biomarkers of Systemic Inflammation and Growth in Early Infancy are Associated with Stunting in Young Tanzanian Children. Nutrients 2018, 10, 1158. [Google Scholar] [CrossRef] [Green Version]
- Pompano, L.M.; Boy, E. Effects of Dose and Duration of Zinc Interventions on Risk Factors for Type 2 Diabetes and Cardiovascular Disease: A Systematic Review and Meta-Analysis. Adv. Nutr. 2020, 12, 141–160. [Google Scholar] [CrossRef]
- Hussain, S.; Maqsood, M.A.; Miller, L.V. Bioavailable zinc in grains of bread wheat varieties of Pakistan. Cereal Res. Commun. 2012, 40, 62–73. [Google Scholar] [CrossRef]
| Total | Arm 1 (Control in Phase 2) | Arm 2 (Intervention in Phase 2) | p b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | Median (Range) | n (%) | n | Mean (SD) | Median (Range) | n (%) | n | Mean (SD) | Median (Range) | n (%) | ||
| Participant Characteristics: | |||||||||||||
| Age | 517 | 12.1 (1.7) | 12.0 (8.6–15.3) | - | 260 | 12.2 (1.7) | 12.0 (9.3–15.3) | 257 | 12.1 (1.7) | 12.1 (8.6–15.3) | 0.954 | ||
| Attending school | 512 | 259 | 253 | ||||||||||
| Yes | 223 (43.6) | 104 (40.2) | 119 (47.0) | 0.116 | |||||||||
| No | 289 (56.4) | 155 (59.8) | 134 (53.0) | ||||||||||
| Ever attended school | 512 | 259 | 253 | ||||||||||
| Attending school | 223 (43.6) | 104 (40.2) | 119 (47.0) | 0.106 | |||||||||
| School dropout | 115 (22.5) | 54 (20.8) | 61 (24.1) | ||||||||||
| Never been to school | 155 (30.3) | 91 (35.1) | 64 (25.3) | ||||||||||
| Unknown (Missing) | 19 (3.7) | 10 (3.9) | 9 (3.6) | ||||||||||
| Education level c | 512 | 259 | 253 | ||||||||||
| Primary | 185 (36.1) | 80 (30.9) | 105 (41.5) | 0.034 | |||||||||
| Middle | 65 (12.7) | 39 (15.1) | 26 (10.3) | ||||||||||
| High | 12 (2.3) | 7 (2.7) | 5 (2.0) | ||||||||||
| Attending school but level missing | 18 (3.5) | 6 (2.3) | 12 (4.7) | ||||||||||
| School dropout but level unknown | 58 (11.3) | 26 (10.0) | 32 (12.6) | ||||||||||
| Never been to school | 155 (30.3) | 91 (35.1) | 64 (25.3) | ||||||||||
| any info on school/education level missing | 19 (3.7) | 10 (3.9) | 9 (3.6) | ||||||||||
| Menarche attained | 506 | 256 | 250 | 0.580 | |||||||||
| Yes | 235 (46.4) | 122 (47.7) | 113 (45.2) | ||||||||||
| No | 271 (53.6) | 134 (52.3) | 137 (54.8) | ||||||||||
| Household Features: | |||||||||||||
| Household demography d | 486 | 250 | 236 | ||||||||||
| Family Size | 10.5 (4.8) | 9.0 (4.0–36.0) | 10.5 (4.5) | 9.0 (4.0–28.0 | 10.5 (5.0) | 9.0 (4.0–36.0) | 0.993 | ||||||
| No. of young children in HH | 2.1 (1.5) | 2.0 (1.0–10.0) | 2.1 (1.4) | 2.0 (1.0–8.0) | 2.2 (1.6) | 2.0 (1.0–10.0) | 0.735 | ||||||
| No. of older Children in HH | 1.5(1.1) | 1.0 (0.0–8.0) | 1.5 (1.1) | 1.0 (0.0–8.0 | 1.5 (1.1) | 1.0 (0.0–6.0) | 0.717 | ||||||
| No. of adolescents in HH | 3.0(1.6) | 3.0 (0.0–11.0) | 3.0 (1.6) | 3.0 (0.0–10.0) | 2.9 (1.7) | 3.0 (0.0–11.0) | 0.316 | ||||||
| No. of adolescent girls in HH | 1.7(1.1) | 1.0 (0.0–7.0) | 1.8 (1.1) | 2.0 (0.0–6.0) | 1.6 (1.2) | 1.0 (0.0–7.0) | 0.214 | ||||||
| No. of adult males in the HH | 1.9(1.4) | 1.0 (0.0–8.0) | 1.9 (1.4) | 1.0 (0.0–8.0) | 1.9 (1.4) | 1.0 (0.0–8.0) | 0.817 | ||||||
| No. of adult Females in the HH | 2.0(1.3) | 2.0 (0.0–7.0) | 2.0 (1.3) | 2.0 (0.0–6.0) | 2.1 (1.3) | 2.0 (1.0–7.0) | 0.429 | ||||||
| Length of stay in the area | 483 | 249 | 234 | 0.769 | |||||||||
| Less than 5 years | 35(7.2) | 16 (6.4) | 19 (8.1) | ||||||||||
| between 5 to 10 years | 36(7.5) | 19 (7.6) | 17 (7.3) | ||||||||||
| 10 years and above | 412(85.3) | 214 (85.9) | 198 (84.6) | ||||||||||
| Socio-economic status and living conditions | |||||||||||||
| Source of Income e | 486 | 250 | 236 | ||||||||||
| Daily wages | 287 (59.1) | 150 (60.0) | 137 (58.1) | 0.662 | |||||||||
| Farming | 7 (1.4) | 4 (1.6) | 3 (1.3) | 0.761 | |||||||||
| Business | 21 (4.3) | 15 (6.0) | 6 (2.5) | 0.061 | |||||||||
| Govt Job | 53 (10.9) | 23 (9.2) | 30 (12.7) | 0.214 | |||||||||
| Private Job | 93 (19.1) | 49 (19.6) | 44 (18.6) | 0.789 | |||||||||
| Charity | 1 (0.2) | 1 (0.4) | 0 (0.0) | 0.331 | |||||||||
| Pension | 1 (0.2) | 1 (0.4) | 0 (0.0) | 0.331 | |||||||||
| Driver | 1 (0.2) | 1 (0.4) | 0 (0.0) | 0.331 | |||||||||
| Abroad f | 4 (0.8) | 2 (0.8) | 2 (0.8) | 0.954 | |||||||||
| Others (unspecified) | 23(4.7) | 10 (4.0) | 13 (5.5) | 0.434 | |||||||||
| Monthly Income | 485 | 250 | 235 | 0.423 | |||||||||
| HH income <20,000 PKR | 297 (61.2) | 147 (58.8) | 150 (63.8) | ||||||||||
| HH income between 20,000–40,000 PKR | 173 (35.7) | 96 (38.4) | 77 (32.8) | ||||||||||
| HH income >40,000 PKR | 15 (3.1) | 7 (2.8) | 8 (3.4) | ||||||||||
| Monthly Expenditure | 483 | 248 | 235 | 0.477 | |||||||||
| HH with expenditure <20,000 PKR | 228 (47.2) | 112 (45.2) | 116 (49.4) | ||||||||||
| HH with expenditure 20,000–40,000 PKR | 239 (49.5) | 129 (52.0) | 110 (46.8) | ||||||||||
| HH with expenditure >40,000 PKR | 16 (3.3) | 7 (2.8) | 9 (3.8) | ||||||||||
| Possession of Assets e | 454 | 238 | 216 | ||||||||||
| Refrigerator/Freezer | 130 (28.6) | 66 (27.7) | 64 (29.6) | 0.655 | |||||||||
| TV/Cable/Dish | 33 (7.3) | 15 (6.3) | 18 (8.3) | 0.405 | |||||||||
| Solar Panels/UPS | 400 (88.1) | 209 (87.8) | 191 (88.4) | 0.841 | |||||||||
| Motorcar | 39 (8.6) | 19 (8.0) | 20 (9.3) | 0.628 | |||||||||
| Motorcycle | 88 (19.4) | 45 (18.9) | 43 (19.9) | 0.788 | |||||||||
| Rikshaw/Chingchi g | 5 (1.1) | 1(0.4) | 4 (1.9) | 0.144 | |||||||||
| House Ownership | 486 | 250 | 236 | 0.740 | |||||||||
| Own | 395 (81.3) | 200 (80.0) | 195 (82.6) | ||||||||||
| Rent | 72 (14.8) | 40 (16.0) | 32 (13.6) | ||||||||||
| Free tenant | 19 (3.9) | 10 (4.0) | 9 (3.8) | ||||||||||
| Structure of House | 485 | 249 | 236 | 0.765 | |||||||||
| Katcha (mud and straw) | 227 (46.8) | 113 (45.4) | 114 (48.3) | ||||||||||
| Pakka (cemented) | 143 (29.5) | 74 (29.7) | 69 (29.2) | ||||||||||
| Mix of katcha and pakka | 115 (23.7) | 62 (24.9) | 53 (22.5) | ||||||||||
| Number of Rooms house | 481 | 3.1 (1.8) | 3.0 (1.0–11.0) | 248 | 3.2 (1.9) | 3.0 (1.0–11.0) | 233 | 3.0 (1.7) | 3.0 (1.0–11.0) | 0.605 | |||
| Toilet present in House | 486 | 250 | 236 | 0.845 | |||||||||
| Yes | 444 (91.4) | 229 (91.6) | 215 (91.1) | ||||||||||
| No | 42 (8.6) | 21 (8.4) | 21 (8.9) | ||||||||||
| No. of toilets in House | 466 | 1.0 (0.6) | 1.0 (0.0–4.0) | 242 | 1.1 (0.6) | 1.0 (0.0–4.0) | 224 | 1.0 (0.5) | 1.0 (0.0–4.0) | 0.614 | |||
| Food and Water | |||||||||||||
| Meal preparation facility in House | 486 | 250 | 236 | 0.781 | |||||||||
| Purpose-built Kitchen | 9 (1.9) | 6 (2.4) | 3 (1.3) | ||||||||||
| Separate & covered (separate structure with roof) | 313 (64.4) | 163 (65.2) | 150 (63.6) | ||||||||||
| Separate & uncovered (separate structure without roof) | 63 (13.0) | 31 (12.4) | 32 (13.6) | ||||||||||
| within room (inside room living in) | 8 (1.6) | 5 (2.0) | 3 (1.3) | ||||||||||
| Open space (temporary arrangement) | 93 (19.1) | 45 (18.0) | 48 (20.3) | ||||||||||
| Source of drinking water | 484 | 249 | 235 | 0.009 | |||||||||
| Borewell | 438 (90.5) | 234 (94.0) | 204 (86.8) | ||||||||||
| Handpump | 13 (2.7) | 2 (0.8) | 11 (4.7) | ||||||||||
| Pipeline (spring) | 5 (1.0) | 4 (1.6) | 1 (0.4) | ||||||||||
| Neighbour (dependent on neighbours) | 14 (2.9) | 5 (2.0) | 9 (3.8) | ||||||||||
| Others | 14 (2.9) | 4 (1.6) | 10 (4.3) | ||||||||||
| Health | |||||||||||||
| Engagement of HH with the vaccination program | 466 | 243 | 223 | 0.006 | |||||||||
| Yes | 447 (95.9) | 239 (98.4) | 208 (93.3) | ||||||||||
| No | 19 (4.1) | 4 (1.6) | 15 (6.7) | ||||||||||
| Diarrheal incidence among children (1–5 years of age) within HH in past month | 486 | 250 | 236 | 0.974 | |||||||||
| Yes | 196 (40.3) | 101 (40.4) | 95 (40.3) | ||||||||||
| No | 290 (59.7) | 149 (59.6) | 141(59.7) | ||||||||||
| RTI incidence among children 1–5 years within HH in past month | 486 | 250 | 236 | 0.039 | |||||||||
| Yes | 198 (40.7) | 113 (45.2) | 85 (36.0) | ||||||||||
| No | 288 (59.3) | 137 (54.8) | 151 (64.0) | ||||||||||
| RTI incidence among adolescent girls (10–16 years of age) within HH in past month | 486 | 250 | 236 | 0.005 | |||||||||
| Yes | 107 (22.0) | 68 (27.2) | 39 (16.5) | ||||||||||
| No | 379 (78.0) | 182 (72.8) | 197 (83.5) | ||||||||||
| Flour consumption and purchase | |||||||||||||
| Type of flour used | 486 | 250 | 236 | 0.062 | |||||||||
| White | 93 (19.1) | 47 (18.8) | 46 (19.5) | ||||||||||
| Brown | 101(20.8) | 59 (23.6) | 42 (17.8) | ||||||||||
| Mix | 282 (58.0) | 143 (57.2) | 139 (58.9) | ||||||||||
| Brown and white | 9 (1.9) | 1 (0.4) | 8 (3.4) | ||||||||||
| Mix and white | 1(0.2) | 0 (0.0) | 1 (0.4) | ||||||||||
| Source of flour procurement | 486 | 250 | 236 | 0.109 | |||||||||
| Purchase from market | 445 (91.6) | 224 (89.6) | 221 (93.6) | ||||||||||
| Self-grown and purchased from market | 41 (8.4) | 26 (10.4) | 15 (6.4) | ||||||||||
| Monthly flour consumption (Kgs) | 485 | 107.4 (45.1) | 100.0 (10.0–300.0) | 249 | 107.8 (44.2) | 100.0 (40.0–300.0 | 236 | 107.1 (46.1) | 100.0 (10.0–300.0) | 0.882 | |||
| Monthly consumption of other staple h (Kgs) | 443 | 6.7 (8.2) | 4.5 (0.0–120.0) | 230 | 7.2 (10.1) | 4.3 (0.0–120.0) | 213 | 6.2 (5.6) | 5.0 (0.0–40.0) | 0.280 | |||
| Purchase practice for flour (mode of payment) | 479 | 248 | 231 | 0.678 | |||||||||
| Cash | 237 (49.5) | 126 (50.8) | 111 (48.1) | ||||||||||
| Credit | 168 (35.1) | 87 (35.1) | 81 (35.1) | ||||||||||
| Cash and Credit | 74 (15.4) | 35 (14.1) | 39 (16.9) | ||||||||||
| Preferred term of supply in the first six months i | 481 | 247 | 234 | 0.354 | |||||||||
| Flour | 313 (65.1) | 168 (68.0) | 145 (62.0) | ||||||||||
| Cash | 94 (19.5) | 43 (17.4) | 51 (21.8) | ||||||||||
| Coupon | 74 (15.4) | 36 (14.6) | 38 (16.2) | ||||||||||
| n | Total | n | Control | n | Intervention | p * | |
|---|---|---|---|---|---|---|---|
| Plasma zinc concentrations, PZC (µg/L) | 420 | 624.7 ± 88.2 | 221 | 628.2 ± 93.6 | 199 | 620.8 ± 81.7 | 0.893 |
| Zinc deficiency (PZC < 650 µg/L for age < 10 years or 660 µg/L for ≥10 years) | 420 | 289 (68.8) | 221 | 146 (66.1) | 199 | 143 (71.9) | 0.2 |
| Serum iron (µg/L) | 420 | 894.9 (659.1–1110.1) | 221 | 888.5 (672.7–1130.4) | 199 | 910.1 (651.9–1100.8) | 0.824 |
| Serum iron <598 µg/L | 420 | 81(19.3) | 221 | 43 (19.5) | 199 | 38 (19.1) | 0.925 |
| Serum ferritin, SF (ng/mL) $ | 417 | 21.1 (11.3–33.7) | 221 | 22.5 (12.2–35.6) | 196 | 20.1 (11.2–33.5) | 0.552 |
| Storage iron deficiency (SF < 15 ng/mL) | 417 | 147 (35.3) | 221 | 68 (30.8) | 196 | 79 (40.3) | 0.042 |
| Serum transferrin receptor, STFR (mg/L) | 418 | 3.4 (2.9–4.0) | 220 | 3.4 (2.8–4.0) | 198 | 3.4 (3.0–4.1) | 0.267 |
| Functional iron deficiency (SFTR > 4.59 mg/L) | 418 | 56 (13.4) | 220 | 29 (13.2) | 198 | 27 (13.6) | 0.892 |
| Iron deficiency (SF < 15 ng/mL or SFTR > 4.59 mg/L) | 417 | 167 (40.0) | 221 | 80 (36.2) | 196 | 87 (44.4) | 0.089 |
| Haemoglobin, Hb (g/dL) | 419 | 12.8 ± 1.2 | 12.9 ± 1.3 | 200 | 12.8 ± 1.1 | 0.715 | |
| Anaemia (Hb < 11.5 g/dL for < 12 years or < 12.0 g/dL for ≥12 years) | 419 | 69.0 (16.5) | 219 | 39 (17.8) | 200 | 30 (15.0) | 0.439 |
| Iron Deficiency Anaemia (SF < 15 ng/mL or SFTR > 4.59 mg/L and Hb < 11.5 g/dL for <12 years or <12.0 g/dL for 12 years) | 420 | 39 (9.3) | 221 | 22 (10.0) | 199 | 17 (8.5) | 0.619 |
| Anaemia Grade: | 419 | 219 | 200 | 0.651 | |||
| Mild (Hb = 11.0–11.4 g/dL for <12 years or 11.0–11.9 g/dL for ≥12 years) | 43 (10.3) | 23 (10.5) | 20 (10.0) | ||||
| Moderate (Hb = 8.0–10.9 g/dL) | 25 (6.0) | 15 (6.8) | 10 (5.0) | ||||
| Severe (Hb < 8.0 g/dL) | 1 (0.2) | 1(0.5) | 0 (0.0) | ||||
| Non- anaemic (Hb ≥ 11.5 g/dL for <12 years or ≥12.0 g/dL for ≥12 years) | 350 (83.5) | 180 (82.2) | 170 (85.0) | ||||
| Red blood cell count, RBC count (106/µL) | 420 | 4.6 ± 0.5 | 220 | 4.6 ± 0.5 | 200 | 4.6 ± 0.5 | 0.564 |
| RBC count < 3.84 × 106/µL | 420 | 16 (3.8%) | 220 | 7 (3.2%) | 200 | 9 (4.5%) | 0.481 |
| Mean corpuscular volume, MCV (fL) | 417 | 82.1 ± 7.0 | 217 | 82.0 ± 7.5 | 200 | 82.3 ± 6.4 | 0.714 |
| MCV < 74.7 fL | 417 | 41 (9.8%) | 217 | 23 (10.6%) | 200 | 18 (9.0%) | 0.584 |
| Haematocrit, HCT (%) | 420 | 37.5 ± 3.0 | 220 | 37.5 ± 3.1 | 200 | 37.5 ± 2.8 | 0.857 |
| HCT < 33.5% | 420 | 33 (7.9%) | 220 | 21 (9.5%) | 200 | 12(6.0%) | 0.177 |
| Mean corpuscular haemoglobin concentration, MCHC (g/dL) | 420 | 34.2 ± 1.3 | 220 | 34.2 ± 1.3) | 200 | 34.1 ± 1.3 | 0.842 |
| MCHC < 32.3 g/dL | 420 | 34 (8.1) | 220 | 18 (8.2) | 200 | 16 (8.0) | 0.946 |
| C-reactive protein, CRP (mg/dL) | 414 | 0.03 (0.02–0.07) | 219 | 0.03 (0.02–0.06) | 195 | 0.04 (0.02–0.08) | 0.902 |
| CRP >0.5 mg/dL | 414 | 2 (0.5) | 219 | 1 (0.5) | 195 | 1(0.5) | 0.934 |
| Alpha 1-acid glycoprotein, AGP (mg/dL) | 420 | 61.2 (45.5–74.5) | 221 | 58.8 (43.3–71.6) | 199 | 63.7 (48.2–79.6) | 0.052 |
| AGP > 100 mg/dL | 420 | 14.0 (3.3) | 221 | 4 (1.8) | 199 | 10 (5.0) | 0.067 |
| Plasma selenium (µg/L) | 418 | 102.8 ± 13.6 | 220 | 101.6 ± 12.4) | 198 | 104.2 ± 14.7 | 0.020 |
| Selenium deficiency (Plasma selenium < 41.8 μg/L) | 418 | 0 (0.0) | 220 | 0 (0.0) | 198 | 0(0.0) | - |
| Plasma copper (µg/L) | 420 | 930.4 ± 171.3 | 221 | 914.4 ± 183.0 | 199 | 948.1 ± 155.8 | 0.117 |
| Copper deficiency (Plasma copper < 750 μg/L for < 10.3 years; <640 μg/L for 10.3–12.5 y; <570 μg/L for >12.5 y) | 420 | 8 (1.9) | 221 | 7 (3.2) | 199 | 1 (0.5) | 0.046 |
| Copper:Zinc ratio | 420 | 1.5 (1.3–1.7) | 221 | 1.4 (1.2–1.7) | 199 | 1.5 (1.3–1.7) | 0.214 |
| Galaxy n = 75 | Zincol-2016 n = 62 | β (CI) * | t | p | |
|---|---|---|---|---|---|
| Zinc (mg/kg) | 17.0 ± 2.6 | 20.7 ± 5.6 | 3.696 (2.258, 5.134) | 5.083 | <0.001 |
| (16.4–17.6) | (19.2–22.1) | ||||
| Iron (mg/kg) | 23.8 ± 4.7 | 26.8 ± 5.6 | 3.044 (1.293, 4.794) | 3.439 | 0.001 |
| (22.6–24.9) | (25.4–28.2) | ||||
| Copper (mg/kg) | 2.6 ± 0.9 | 2.9 ± 1.2 | 0.344 (−0.019, 0.707) | 1.875 | 0.063 |
| (2.4–2.8) | (2.6–3.2) | ||||
| Selenium (µg/kg) | 45.0 ± 13.2 | 51.3 ± 14.2 | 6.235 (1.610, 10.860) | 2.666 | 0.009 |
| (42.0–48.1) | (47.7–54.9) | ||||
| Calcium (mg/kg) | 326.4 ± 25.3 | 340.3 ± 22.9 | 13.924 (5.702, 22.146) | 3.349 | 0.001 |
| (320.4–332.3) | (334.4–346.1) | ||||
| Phosphorus (g/kg) | 2.2 ± 0.2 | 2.4 ± 0.2 | |||
| (2.2–2.3) | (2.3–2.4) | 0.169 (0.093, 0.245) | 4.405 | <0.001 |
| Wheat Bread Consumption (g/Day) | Zinc (mg/Day) | Iron (mg/Day) | Phytate (mg/Day) | |||||
|---|---|---|---|---|---|---|---|---|
| FCD * | Galaxy | Zincol-2016 | FCD* | Galaxy | Zincol-2016 | FCD * | ||
| Mean ± SD | 541 ± 134 | 7.8 ± 2.0 | 6.9 ± 1.7 | 8.4 ± 2.1 | 12.3 ± 3.1 | 9.6 ± 2.4 | 10.9 ± 2.7 | 1584 ± 397.1 |
| Median (Range) | 525 (212–1114) | 7.7 (3.0–16.2) | 6.7 (2.7–14.2) | 8.1 (3.3–17.3) | 12.0 (4.6–25.4) | 9.4 (3.8–19.9) | 10.6 (4.3–22.4) | 1548 (589–3270) |
| Time Points | n | Control | n | Intervention | X2 | β (CI) * | t | p | |
|---|---|---|---|---|---|---|---|---|---|
| Zinc deficiency prevalence *, n (%) | |||||||||
| Baseline | 221 | 146 (66.1) | 199 | 143(71.9) | 1.639 | 0.200 | |||
| Midpoint | 213 | 159 (74.6) | 192 | 141(73.4) | 0.077 | 0.781 | |||
| Endline | 214 | 129 (60.3) | 188 | 121 (64.4) | 0.709 | 0.400 | |||
| Plasma zinc concentration **, Mean ± SD | |||||||||
| Baseline | 146 | 581.8 ± 54.5 | 143 | 581.9 ± 51.2 | |||||
| Midpoint | 140 | 591.9 ± 69.1 | 136 | 584.2 ± 77.2 | −2.563(−24.156, 19.030) | −0.242 | 0.810 | ||
| Endline | 142 | 613.3 ± 79.8 | 134 | 619.3 ± 103.5 | 11.085 (−19.865, 42.035) | 0.733 | 0.470 |
| Outcomes | Time Points | n | Control | n | Intervention | β (95%CI) * | X2 | t | p |
|---|---|---|---|---|---|---|---|---|---|
| Serum iron (µg/L) | Baseline | 221 | 888.5 (672.7–1130.4) | 199 | 910.1 (651.9–1100.8) | ||||
| Midpoint | 213 | 877.2 (632.3–1104.3) | 192 | 894.5 (676.0–1127.2) | 33.539 (−43.606, 110.684) | 0.879 | 0.385 | ||
| Endline | 214 | 856.7 (610.9–1077.5) | 188 | 828.1 (552.9–1060.6) | −28.302 (91.397, 34.793) | −0.921 | 0.365 | ||
| Serum iron < 598 µg/L | Baseline | 221 | 43 (19.5) | 199 | 38 (19.1) | 0.009 | 0.925 | ||
| Midpoint | 213 | 45 (21.1) | 192 | 35 (18.2) | 0.535 | 0.465 | |||
| Endline | 214 | 49 (22.9) | 188 | 54 (28.7) | 1.783 | 0.182 | |||
| Serum Ferritin, SF (ng/mL) $ | Baseline | 221 | 22.5 (12.2–35.6) | 196 | 20.1 (11.2–33.5) | ||||
| Midpoint | 212 | 26.2 (15.2–40.5) | 194 | 23.1 (14.2–33.8) | −3.525 (−8.254, 1.203) | −1.515 | 0.139 | ||
| Endline | 213 | 17.4 (9.2–31.2) | 188 | 17.8 (7.3–29.5) | −3.549 (−8.622, 1.523) | −1.418 | 0.165 | ||
| Storage iron deficiency (SF <15 ng/mL) | Baseline | 221 | 68 (30.8) | 196 | 79 (40.3) | 4.139 | 0.042 | ||
| Midpoint | 212 | 49 (23.1) | 194 | 50 (25.8) | 0.389 | 0.533 | |||
| Endline | 213 | 88 (41.3) | 188 | 80 (42.6) | 0.063 | 0.802 | |||
| Serum Transferrin Receptor, STFR (mg/L) | Baseline | 220 | 3.4 (2.8–4.0) | 198 | 3.4 (3.0–4.1) | ||||
| Midpoint | 212 | 3.3 (2.9–3.9) | 191 | 3.4 (3.0–4.0) | −0.005 (−0.241, 0.232) | −0.040 | 0.968 | ||
| Endline | 210 | 3.2 (2.8–3.8) | 187 | 3.3 (2.7–4.1) | 0.112 (−0.178, 0.403) | 0.779 | 0.440 | ||
| Functional iron deficiency (SFTR > 4.59 mg/L) | Baseline | 220 | 29 (13.2) | 198 | 27 (13.6) | 0.019 | 0.892 | ||
| Midpoint | 212 | 26 (12.3) | 191 | 19 (9.9) | 0.544 | 0.461 | |||
| Endline | 210 | 26 (12.4) | 187 | 32 (17.1) | 1.775 | 0.183 | |||
| Iron deficiency (SF < 15 ng/mL or SFTR > 4.59 mg/L) | Baseline | 221 | 80 (36.2) | 196 | 87 (44.4) | 2.901 | 0.089 | ||
| Midpoint | 209 | 60 (28.7) | 192 | 57 (29.7) | 0.046 | 0.829 | |||
| Endline | 213 | 90 (42.3) | 188 | 88 (46.8) | 0.839 | 0.360 | |||
| Iron Deficiency anaemia (SF <15 ng/mL or SFTR > 4.59 mg/L and Hb < 11.5 g/dL for <12 years or <12.0 g/dL for ≥12 years) | Baseline | 221 | 22 (10.0) | 199 | 17 (8.5) | 0.248 | 0.619 | ||
| Midpoint | 213 | 16 (7.5) | 195 | 13 (13.9) | 0.110 | 0.740 | |||
| Endline | 213 | 23 (10.8) | 188 | 25 (13.3) | 0.592 | 0.442 |
| Outcomes | Time Points | n | Control | n | Intervention | β (95%CI) * | X2 | t | p * |
|---|---|---|---|---|---|---|---|---|---|
| Plasma copper (µg/L) | Baseline | 221 | 914.4 ± 183.0 | 199 | 948.1 ± 155.8 | ||||
| Midpoint | 213 | 926.3 ± 139.3 | 191 | 961.3 ± 154.5 | 16.882 (−7.130, 40.894) | 1.447 | 0.160 | ||
| Endline | 214 | 871.0 ± 147.3 | 187 | 907.9 ± 155.9 | 18.562 (−10.056, 47.180) | 1.326 | 0.195 | ||
| Copper deficiency (plasma copper < 750 μg/L for <10.3 years; <640 μg/L for 10.3–12.5 years; <570 μg/L for >12.5 years) | Baseline | 221 | 7 (3.2) | 199 | 1 (0.5) | 3.980 | 0.046 | ||
| Midpoint | 213 | 2 (0.9) | 191 | 1 (0.5) | 0.236 | 0.627 | |||
| Endline | 214 | 10 (4.7) | 187 | 2 (1.1) | 4.464 | 0.035 | |||
| Plasma selenium (µg/L) | Baseline | 220 | 101.6 ± 12.4 | 198 | 104.2 ± 14.7 | ||||
| Midpoint | 213 | 98.5 ± 13.1 | 192 | 101.4 ± 12.7 | 0.960 (−2.637, 4.556) | 0.536 | 0.595 | ||
| Endline | 213 | 95.7 ± 12.1 | 188 | 96.0 ± 13.4 | −0.270 (−3.483, 2.943) | −0.170 | 0.866 | ||
| Copper:zinc ratio | Baseline | 221 | 1.4 (1.2–1.7) | 199 | 1.5 (1.3–1.7) | ||||
| Midpoint | 213 | 1.5 (1.3–1.7) | 191 | 1.6 (1.4–1.8) | 0.032 (−0.026, 0.090) | 1.116 | 0.273 | ||
| Endline | 214 | 1.4 (1.2–1.6) | 187 | 1.4 (1.3–1.6) | 0.024 (−0.032, 0.081) | 0.876 | 0.388 | ||
| C-reactive protein, CRP (mg/dL) | Baseline | 219 | 0.03 (0.02–0.06) | 195 | 0.04 (0.02–0.08) | ||||
| Midpoint | 213 | 0.030 (0.02–0.05) | 194 | 0.03 (0.02–0.06) | 0.005 (−0.014, 0.023) | 0.535 | 0.597 | ||
| Endline | 212 | 0.03 (0.02–0.05) | 186 | 0.03 (0.02–0.07) | 0.005 (−0.011, 0.021) | 0.603 | 0.552 | ||
| CRP > 0.5 mg/dL | Baseline | 219 | 1 (0.5) | 195 | 1 (0.5) | 0.007 | 0.934 | ||
| Midpoint | 213 | 0 (0.0) | 194 | 2 (1.0) | 2.207 | 0.137 | |||
| Endline | 212 | 1 (0.5) | 186 | 1 (0.5) | 0.009 | 0.926 | |||
| Alpha 1-acid glycoprotein, AGP (mg/dL) | Baseline | 221 | 58.8 (43.3–71.6) | 199 | 63.7 (48.2–79.6) | ||||
| Midpoint | 214 | 66.5 (55.6–80.5) | 194 | 66.4 (56.3–79.7) | 0.552 (−4.001, 5.106) | 0.246 | 0.807 | ||
| Endline | 214 | 69.5 (57.5–83.0) | 188 | 63.7 (52.8–76.8) | −4.548 (−8.921, −0.175) | −2.148 | 0.042 | ||
| AGP > 100 mg/dL | Baseline | 221 | 4 (1.8) | 199 | 10 (5.0) | 3.359 | 0.067 | ||
| Midpoint | 214 | 12 (5.6) | 194 | 17 (8.8) | 1.534 | 0.215 | |||
| Endline | 214 | 14 (6.5) | 188 | 5 (2.7) | 3.350 | 0.067 |
| Copper | Selenium | C-Reactive Protein | Alpha-1-Acid Glycoprotein | Copper:Zinc Ratio | ||
|---|---|---|---|---|---|---|
| Copper | rs | 1.000 | 0.166 ** | 0.216 ** | 0.252 ** | 0.744 ** |
| n | 2169 | 2160 | 2123 | 2163 | 2168 | |
| Selenium | rs | 0.166 ** | 1.000 | 0.062 ** | −0.001 | −0.005 |
| n | 2160 | 2165 | 2119 | 2158 | 2159 | |
| C-Reactive Protein | rs | 0.216 ** | 0.062 ** | 1.000 | 0.456 ** | 0.189 ** |
| n | 2123 | 2119 | 2154 | 2150 | 2122 | |
| Alpha-1-Acid Glycoprotein | rs | 0.252 ** | −0.001 | 0.456 ** | 1.000 | 0.222 ** |
| n | 2163 | 2158 | 2150 | 2193 | 2162 | |
| Copper:Zinc ratio | rs | −0.573 ** | −0.086 ** | 0.222 ** | 0.090 ** | 1.000 |
| n | 2168 | 2153 | 2162 | 2152 | 2168 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, S.; Zaman, M.; Fatima, S.; Shahzad, B.; Brazier, A.K.M.; Moran, V.H.; Broadley, M.R.; Zia, M.H.; Bailey, E.H.; Wilson, L.; et al. The Impact of Consuming Zinc-Biofortified Wheat Flour on Haematological Indices of Zinc and Iron Status in Adolescent Girls in Rural Pakistan: A Cluster-Randomised, Double-Blind, Controlled Effectiveness Trial. Nutrients 2022, 14, 1657. https://doi.org/10.3390/nu14081657
Gupta S, Zaman M, Fatima S, Shahzad B, Brazier AKM, Moran VH, Broadley MR, Zia MH, Bailey EH, Wilson L, et al. The Impact of Consuming Zinc-Biofortified Wheat Flour on Haematological Indices of Zinc and Iron Status in Adolescent Girls in Rural Pakistan: A Cluster-Randomised, Double-Blind, Controlled Effectiveness Trial. Nutrients. 2022; 14(8):1657. https://doi.org/10.3390/nu14081657
Chicago/Turabian StyleGupta, Swarnim, Mukhtiar Zaman, Sadia Fatima, Babar Shahzad, Anna K. M. Brazier, Victoria H. Moran, Martin R. Broadley, Munir H. Zia, Elizabeth H. Bailey, Lolita Wilson, and et al. 2022. "The Impact of Consuming Zinc-Biofortified Wheat Flour on Haematological Indices of Zinc and Iron Status in Adolescent Girls in Rural Pakistan: A Cluster-Randomised, Double-Blind, Controlled Effectiveness Trial" Nutrients 14, no. 8: 1657. https://doi.org/10.3390/nu14081657
APA StyleGupta, S., Zaman, M., Fatima, S., Shahzad, B., Brazier, A. K. M., Moran, V. H., Broadley, M. R., Zia, M. H., Bailey, E. H., Wilson, L., Khan, I. M., Sinclair, J. K., & Lowe, N. M. (2022). The Impact of Consuming Zinc-Biofortified Wheat Flour on Haematological Indices of Zinc and Iron Status in Adolescent Girls in Rural Pakistan: A Cluster-Randomised, Double-Blind, Controlled Effectiveness Trial. Nutrients, 14(8), 1657. https://doi.org/10.3390/nu14081657