
Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation


 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
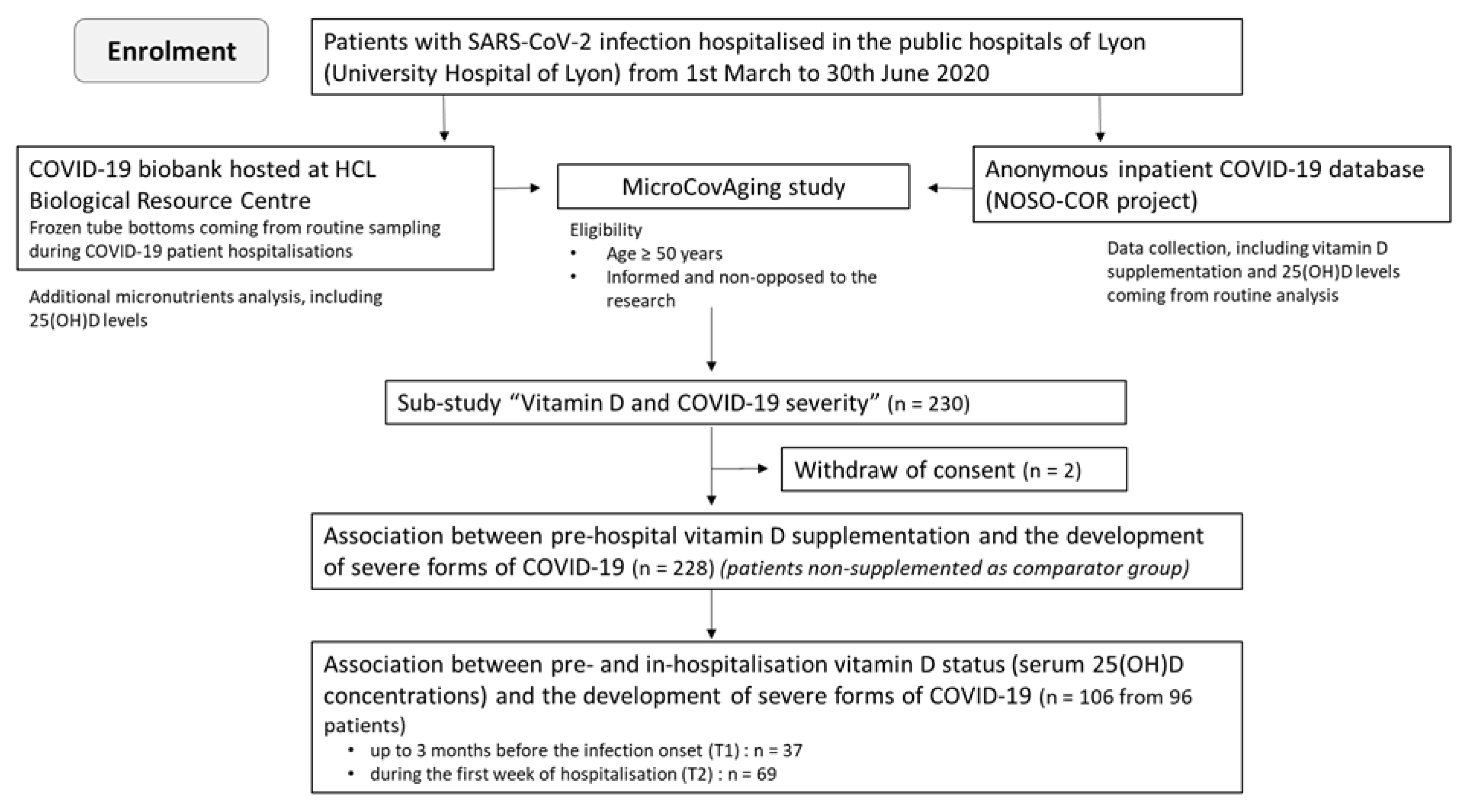
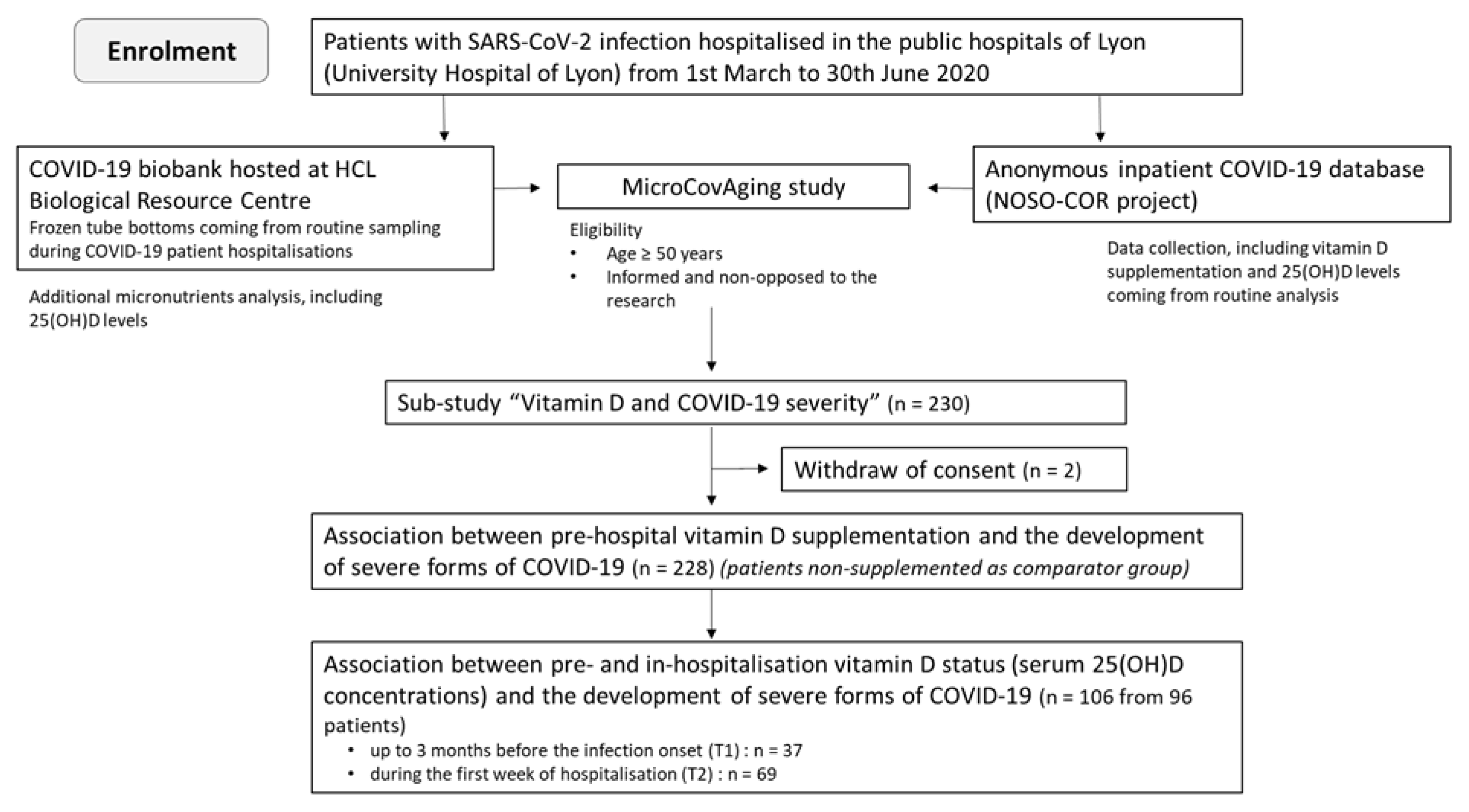
2.1. Study Design and Participants’ Profile
2.2. Data Collection
2.3. Pre-Hospital Vitamin D Supplementation
2.4. Serum Concentrations of 25(OH)D and Vitamin D Status
2.5. Study Clinical Endpoints of COVID-19 Disease Severity
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Patient Demographics and Comorbidities
3.2. Clinical Outcomes
3.3. Laboratory Parameters
3.4. Pre-Hospital Vitamin D Supplementation
3.5. Association between Pre-Hospital Vitamin D Supplementation and Clinical Outcomes
3.6. Association between Serum Concentrations of 25(OH)D and Clinical Outcomes
3.7. Association between Vitamin D Status and Clinical Outcomes
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why Does COVID-19 Disproportionately Affect Older People? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2021, 11, 1793. [Google Scholar] [CrossRef] [PubMed]
- Bonafè, M.; Prattichizzo, F.; Giuliani, A.; Storci, G.; Sabbatinelli, J.; Olivieri, F. Inflamm-Aging: Why Older Men Are the Most Susceptible to SARS-CoV-2 Complicated Outcomes. Cytokine Growth Factor Rev. 2020, 53, 33–37. [Google Scholar] [CrossRef]
- Damayanthi, H.D.W.T.; Prabani, K.I.P. Nutritional Determinants and COVID-19 Outcomes of Older Patients with COVID-19: A Systematic Review. Arch. Gerontol. Geriatr. 2021, 95, 104411. [Google Scholar] [CrossRef]
- Richardson, D.P.; Lovegrove, J.A. Nutritional Status of Micronutrients as a Possible and Modifiable Risk Factor for COVID-19: A UK Perspective. Br. J. Nutr. 2021, 125, 678–684. [Google Scholar] [CrossRef]
- Bilezikian, J.P.; Bikle, D.; Hewison, M.; Lazaretti-Castro, M.; Formenti, A.M.; Gupta, A.; Madhavan, M.V.; Nair, N.; Babalyan, V.; Hutchings, N.; et al. MECHANISMS IN ENDOCRINOLOGY: Vitamin D and COVID-19. Eur. J. Endocrinol. 2020, 183, R133–R147. [Google Scholar] [CrossRef]
- Griffin, G.; Hewison, M.; Hopkin, J.; Kenny, R.; Quinton, R.; Rhodes, J.; Subramanian, S.; Thickett, D. Vitamin D and COVID-19: Evidence and Recommendations for Supplementation. R. Soc. Open Sci. 2020, 7, 201912. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Griffin, G.; Kenny, R.A. Perspective: Vitamin D Deficiency and COVID-19 Severity—Plausibly Linked by Latitude, Ethnicity, Impacts on Cytokines, ACE2 and Thrombosis. J. Intern. Med. 2021, 289, 97–115. [Google Scholar] [CrossRef]
- Basit, S. Vitamin D in Health and Disease: A Literature Review. Br. J. Biomed. Sci. 2013, 70, 161–172. [Google Scholar] [CrossRef]
- Greiller, C.; Martineau, A. Modulation of the Immune Response to Respiratory Viruses by Vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prietl, B.; Treiber, G.; Pieber, T.; Amrein, K. Vitamin D and Immune Function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D Supplementation to Prevent Acute Respiratory Tract Infections: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolliffe, D.A.; Camargo, C.A.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Bischoff-Ferrari, H.A.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D Supplementation to Prevent Acute Respiratory Infections: A Systematic Review and Meta-Analysis of Aggregate Data from Randomised Controlled Trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Kara, M.; Ekiz, T.; Ricci, V.; Kara, Ö.; Chang, K.-V.; Özçakar, L. “Scientific Strabismus” or Two Related Pandemics: Coronavirus Disease and Vitamin D Deficiency. Br. J. Nutr. 2020, 124, 736–741. [Google Scholar] [CrossRef] [PubMed]
- NIH. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; NIH: Stapleton, NY, USA, 2020; Volume 2019, p. 130. Available online: Https://Covid19treatmentguidelines.Nih.Gov/ (accessed on 13 April 2022).
- Martineau, A.R.; Forouhi, N.G. Vitamin D for COVID-19: A Case to Answer? Lancet Diabetes Endocrinol. 2020, 8, 735–736. [Google Scholar] [CrossRef]
- Annweiler, C.; Beaudenon, M.; Gautier, J.; Simon, R.; Dubée, V. COvid-19 and High-Dose VITamin D Supplementation TRIAL in High-Risk Older Patients (COVIT-TRIAL): Study Protocol for a Randomized Controlled Trial. Trials 2020, 21, 1031. [Google Scholar] [CrossRef]
- Ferrari, D.; Locatelli, M.; Briguglio, M.; Lombardi, G. Is There a Link between Vitamin D Status, SARS-CoV-2 Infection Risk and COVID-19 Severity? Cell Biochem. Funct. 2021, 39, 35–47. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G. Vitamin D Insufficiency: Definition, Diagnosis and Management. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 669–684. [Google Scholar] [CrossRef]
- Bouillon, R. Comparative Analysis of Nutritional Guidelines for Vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Meehan, M.; Penckofer, S. The Role of Vitamin D in the Aging Adult. J. Aging Gerontol. 2014, 2, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Skrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? 1,2. Am. J. Clin. Nutr 2016, 103, 1033–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breysse, C.; Guillot, P.; Berrut, G. Étude de La Supplémentation En Vitamine D Chez Les Personnes de plus de 65 Ans En Médecine Générale. Geriatr. Psychol. Neuropsychiatr. Vieil. 2015, 13, 123–132. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef]
- Saadatian-Elahi, M.; Picot, V.; Hénaff, L.; Pradel, F.K.; Escuret, V.; Dananché, C.; Elias, C.; Endtz, H.P.; Vanhems, P. Protocol for a Prospective, Observational, Hospital-Based Multicentre Study of Nosocomial SARS-CoV-2 Transmission: NOSO-COR Project. BMJ Open 2020, 10, e039088. [Google Scholar] [CrossRef]
- Benhamou, C.; Souberbielle, J.; Cortet, B. La Vitamine D Chez l’adulte: Recommandations Du GRIO. Presse Med. 2011, 40, 673–682. [Google Scholar] [CrossRef]
- Silva, M.C.; Furlanetto, T.W. Does Serum 25-Hydroxyvitamin D Decrease during Acute-Phase Response? A Systematic Review. Nutr. Res. 2015, 35, 91–96. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Avis Relatif à L’actualisation de la Liste des Facteurs de Risque de Forme Grave de COVID-19. 2020, pp. 1–34. Available online: http://Www.Rpfc.Fr/Espacepro/Wp-Content/Pdf/Avis HCSP Grippe et Antiviraux Patients Extra-Hospitalier-09-11-12.Pdf (accessed on 20 March 2022).
- El Rais, H.; Aflak-Kattar, M.; Bleistein, L. Parcours Hospitaliers Des Patients Atteints de La COVID-19 de Mars 2020 à Janvier 2021. Les Dossiers de la DREES 2021, 79, 1–43. [Google Scholar]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Pouw, N.; de Maat, J.; van Veerman, K.; Oever, J.; ten Janssen, N.; Abbink, E.; Reijers, M.; de Mast, Q.; Hoefsloot, W.; van Crevel, R.; et al. Clinical Characteristics and Outcomes of 952 Hospitalized COVID-19 Patients in the Netherlands: A Retrospective Cohort Study. PLoS ONE 2021, 16, e0248713. [Google Scholar] [CrossRef] [PubMed]
- Daneshkhah, A.; Agrawal, V.; Eshein, A.; Subramanian, H.; Roy, H.K.; Backman, V. Evidence for Possible Association of Vitamin D Status with Cytokine Storm and Unregulated Inflammation in COVID-19 Patients. Aging Clin. Exp. Res. 2020, 32, 2141–2158. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the Immune System. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Fakhoury, H.M.A.; Kvietys, P.R.; Shakir, I.; Shams, H.; Grant, W.B.; Alkattan, K. Lung-Centric Inflammation of COVID-19: Potential Modulation by Vitamin D. Nutrients 2021, 13, 2216. [Google Scholar] [CrossRef]
- Ter Horst, R.; Jaeger, M.; Smeekens, S.P.; Oosting, M.; Swertz, M.A.; Li, Y.; Kumar, V.; Diavatopoulos, D.A.; Jansen, A.F.M.; Lemmers, H.; et al. Host and Environmental Factors Influencing Individual Human Cytokine Responses. Cell 2016, 167, 1111–1124.e13. [Google Scholar] [CrossRef] [Green Version]
- Teshome, A.; Adane, A.; Girma, B.; Mekonnen, Z.A. The Impact of Vitamin D Level on COVID-19 Infection: Systematic Review and Meta-Analysis. Front. Public Heal. 2021, 9, 169. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D Deficiency Aggravates COVID-19: Systematic Review and Meta-Analysis. Crit. Rev. Food Sci. Nutr. 2020, 62, 1308–1316. [Google Scholar] [CrossRef]
- Barassi, A.; Pezzilli, R.; Mondoni, M.; Rinaldo, R.F.; DavÌ, M.; Cozzolino, M.; Melzi D’Eril, G.V.; Centanni, S. Vitamin D in Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Patients with Non-Invasive Ventilation Support. Panminerva Med. 2021. [Google Scholar] [CrossRef]
- Bassatne, A.; Basbous, M.; Chakhtoura, M.; El Zein, O.; Rahme, M.; El-Hajj Fuleihan, G. The Link between COVID-19 and VItamin D (VIVID): A Systematic Review and Meta-Analysis. Metab. Clin. Exp. 2021, 119, 154753. [Google Scholar] [CrossRef]
- Fassio, A.; Adami, G.; Rossini, M.; Giollo, A.; Caimmi, C.; Bixio, R.; Viapiana, O.; Milleri, S.; Gatti, M.; Gatti, D. Pharmacokinetics of Oral Cholecalciferol in Healthy Subjects with Vitamin D Deficiency: A Randomized. Nutrients 2020, 12, 1553. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; MacEdo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Leaf, D.E.; Ginde, A.A. Vitamin D3 to Treat COVID-19: Different Disease, Same Answer. JAMA 2021, 325, 1047–1048. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total Patients | COVID-19 Survivors | COVID-19-Related Death | Severe COVID-19 (Including Death) * | ICU Admission ** | |
|---|---|---|---|---|---|
| (n = 228) | 85% (193/228) | 15% (35/228) | 46% (105/228) | 37% (84/228) | |
| Median age (IQR) | 78 years (68–87) | 76 years (66–87) | 82 years (76–86) | 73 years (66–82) | 71 years (64–77) |
| Age ≥ 70 years % (n) | 72% (164/228) | 68% (132/193) | 91% (32/35) | 67% (70/105) | 56% (47/84) |
| Age ≥ 80 years % (n) | 43% (99/228) | 41% (80/193) | 54% (19/35) | 27% (28/105) | 14% (12/84) |
| Sex ratio (male/female) | 1.3 (129/99) | 1.1 (101/92) | 4.0 (28/7) | 2.2 (72/33) | 2.5 (60/24) |
| Living in institutions % (n) | 25% (56/228) | 24% (47/193) | 26% (9/35) | 19% (20/105) | 6% (5/84) |
| Median BMI (IQR) | 25.7 kg/m2 (22.1–29.1) n = 224 *** | 25.9 kg/m2 (22.2–29.1) n = 190 | 24.7 kg/m2 (20.6–27.6) n = 34 | 26.7 kg/m2 (23.8–30.4) n = 104 | 27.3 kg/m2 (24.5–31.2) n = 84 |
| BMI < 18.5 kg/m2 % (n) | 8% (19/224) | 8% (15/190) | 12% (4/34) | 5% (5/104) | 2% (2/84) |
| BMI ≥ 35 kg/m2 % (n) | 7% (16/224) | 6% (11/190) | 15% (5/34) | 12% (12/104) | 12% (10/84) |
| Arterial hypertension % (n) | 56% (127/228) | 54% (104/193) | 66% (23/35) | 59% (62/105) | 56% (47/84) |
| Cardiac diseases % (n) | 36% (83/228) | 35% (68/193) | 43% (15/35) | 29% (30/105) | 25% (21/84) |
| Diabetes mellitus (types 1 & 2) % (n) | 32% (74/228) | 34% (65/193) | 26% (9/35) | 33% (35/105) | 36% (30/84) |
| Neuro-muscular diseases % (n) | 19% (43/228) | 21% (40/193) | 9% (3/35) | 12% (13/105) | 13% (11/84) |
| Neuro-cognitive disorders % (n) | 19% (43/228) | 19% (37/193) | 18% (6/35) | 10% (11/105) | 1% (1/84) |
| Renal diseases % (n) | 14% (31/228) | 14% (27/193) | 11% (4/35) | 9% (9/105) | 8% (7/84) |
| Pulmonary diseases % (n) | 13% (30/228) | 12% (24/193) | 17% (6/35) | 15% (16/105) | 11% (9/84) |
| Solid-organ cancers (diagnosed < 1 year ago) % (n) | 8% (19/228) | 8% (15/193) | 11% (4/35) | 8% (8/105) | 5% (4/84) |
| Immunodeficiency diseases % (n) | 7% (15/228) | 6% (12/193) | 9% (3/35) | 9% (9/105) | 8% (7/84) |
| Haematological cancers (diagnosed < 1 year ago) % (n) | 4% (9/228) | 4% (8/193) | 3% (1/35) | 2% (2/105) | 1% (1/84) |
| Multiples comorbidities (≥2) % (n) | 63% (144/228) | 63% (122/193) | 63% (22/35) | 57% (60/105) | 52% (44/84) |
| Severe COVID-19, Including Death (n = 105) | Non-Severe COVID-19 (n = 123) | p Value ** | |
|---|---|---|---|
| CRP (mg/L) * | 179 (111–271) (n = 104) | 81 (46–140) (n = 122) | <0.001 |
| LDH (U/L) * | 352 (269–488) (n = 23) | 240 (198–281) (n = 27) | <0.001 |
| Leukocyte (giga/L) * | 15.5 (11.4–19.1) (n = 105) | 9.25 (7.10–11.61) (n = 121) | <0.001 |
| Neutrophilic polynuclear (giga/L) * | 12.6 (9.21–15.5) (n = 105) | 7,09 (4.78–9.24) (n = 121) | <0.001 |
| Lymphocyte (giga/L) * | 0.5 (0.41–0.77) (n = 105) | 0.77 (0.54–1.16) (n = 121) | <0.001 |
| Platelets (giga/L) * | 422 (330–541) (n = 105) | 353 (284–450) (n = 121) | 0.003 |
| Fibrinogen (g/L) * | 7.61 (6.32–9.17) (n = 103) | 5.41 (4.08–7.14) (n = 104) | <0.001 |
| D-dimer (μg/L) * | 1879 (1136–5123) (n = 93) | 1170 (673–2407) (n = 58) | 0.004 |
| Albumin (g/L) * | 19.7 (16–23.9) (n = 98) | 28.5 (25.4–32.8) (n = 119) | <0.001 |
| Subgroups | Pre-Hospital Vitamin D Supplementation | COVID-19-Related Death (n) | Severe COVID-19, Including Death (n) | ICU Admission (n) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p value * | No | Yes | p value * | No | Yes | p value * | ||
| All patients | No | 134 | 28 | 0.231 | 76 | 86 | 0.001 | 88 | 74 | <0.001 |
| Yes | 59 | 7 | 47 | 19 | 56 | 10 | ||||
| Total (n) | 193 | 35 | 123 | 105 | 144 | 84 | ||||
| Stratified by gender | ||||||||||
| Males | No | 80 | 22 | 1.000 | 42 | 60 | 0.198 | 50 | 52 | 0.054 |
| Yes | 21 | 6 | 15 | 12 | 19 | 8 | ||||
| Females | No | 54 | 6 | 0.240 | 34 | 26 | 0.010 | 38 | 22 | <0.001 |
| Yes | 38 | 1 | 32 | 7 | 37 | 2 | ||||
| Stratified by gender and age | ||||||||||
| Males ≥ 70 years | No | 44 | 21 | 0.608 | 27 | 38 | 0.245 | 36 | 29 | 0.229 |
| Yes | 19 | 6 | 14 | 11 | 18 | 7 | ||||
| Males < 70 years | No | 36 | 1 | 1.000 | 15 | 22 | 1.000 | 14 | 23 | 1.000 |
| Yes | 2 | 0 | 1 | 1 | 1 | 1 | ||||
| Females ≥ 70 years | No | 33 | 4 | 0.358 | 23 | 14 | 0.121 | 28 | 9 | 0.046 |
| Yes | 36 | 1 | 30 | 7 | 35 | 2 | ||||
| Females < 70 years | No | 21 | 2 | 1.000 | 11 | 12 | 0.480 | 10 | 13 | 0.220 |
| Yes | 2 | 0 | 2 | 0 | 2 | 0 | ||||
| Death (n = 35/228) (Yes/No) | ||||||||
| univariate | multivariate | |||||||
| Variable | Crude OR | 95% CI | p-value | Crude OR | 95% CI | p-value | ||
| BMI * | 2.806 | 0.909 | 8.665 | 0.0729 | 4.727 | 1.248 | 17.911 | 0.0223 |
| Age ** | 4.929 | 1.453 | 16.725 | 0.0105 | 7.586 | 2.083 | 27.627 | 0.0021 |
| Sex *** | 0.275 | 0.114 | 0.659 | 0.0038 | 0.263 | 0.102 | 0.672 | 0.0053 |
| VD supp | 0.568 | 0.235 | 1.373 | 0.2090 | 0.448 | 0.167 | 1.207 | 0.1124 |
| Admission to an ICU (n = 84/228) (Yes/No) | ||||||||
| univariate | multivariate | |||||||
| Variable | Crude OR | 95% CI | p-value | Crude OR | 95% CI | p-value | ||
| BMI * | 3.017 | 1.055 | 8.632 | 0.0395 | 2.948 | 0.923 | 9.418 | 0.0681 |
| Age ** | 0.293 | 0.161 | 0.535 | <0.0001 | 0.386 | 0.200 | 0.745 | 0.0046 |
| Sex *** | 0.368 | 0.207 | 0.654 | 0.0007 | 0.373 | 0.198 | 0.702 | 0.0022 |
| VD supp | 0.212 | 0.101 | 0.445 | <0.0001 | 0.341 | 0.155 | 0.751 | 0.0076 |
| Severe form (n = 105/228) (Yes/No) | ||||||||
| univariate | multivariate | |||||||
| Variable | Crude OR | 95% CI | p-value | Crude OR | 95% CI | p-value | ||
| BMI * | 3.783 | 1.181 | 12.117 | 0.0251 | 4.017 | 1.179 | 13.689 | 0.0262 |
| Age ** | 0.617 | 0.345 | 1.104 | 0.1035 | 0.841 | 0.442 | 1.599 | 0.5972 |
| Sex *** | 0.396 | 0.230 | 0.682 | 0.0008 | 0.414 | 0.232 | 0.739 | 0.0029 |
| VD supp | 0.357 | 0.193 | 0.661 | 0.0011 | 0.426 | 0.217 | 0.838 | 0.0135 |
| 25(OH)D (nmol/L) | COVID-19-Related Death | Severe COVID-19, Including Death | ICU Admission | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Time points * | |||||||||
| T1 (n = 37) | No | Yes | p value ** | No | Yes | p value ** | No | Yes | p value ** |
| 25(OH)D (IQR) | 72 (56–86) | 62 (52–70) | 0.376 | 74 (56–86) | 67 (52–72) | 0.374 | 71 (56–85) | 63 (50–80) | 0.520 |
| n | 31 | 6 | 27 | 10 | 32 | 5 | |||
| T2 (n = 69) | No | Yes | p value ** | No | Yes | p value ** | No | Yes | p value ** |
| 25(OH)D (IQR) | 61 (35–85) | 53 (40–107) | 0.694 | 60 (37–85) | 68 (33–94) | 0.809 | 60 (37–89) | 59 (28–75) | 0.469 |
| n | 61 | 8 | 53 | 16 | 63 | 6 | |||
| Vitamin D Status * (GRIO Guidelines) | COVID-19-Related Death | Severe COVID-19, Including Death | ICU Admission | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Time point T1 | No | Yes | p value ** | No | Yes | p value ** | No | Yes | p value ** | |
| Deficiency (n) | No | 30 | 6 | 1.000 | 26 | 10 | 1.000 | 31 | 5 | 1.000 |
| Yes | 1 | 0 | 1 | 0 | 1 | 0 | ||||
| Insufficiency (n) | No | 14 | 1 | 0.368 | 13 | 2 | 0.153 | 14 | 1 | 0.629 |
| Yes | 17 | 5 | 14 | 8 | 18 | 4 | ||||
| Time point T2 | No | Yes | p value ** | No | Yes | p value ** | No | Yes | p value ** | |
| Deficiency (n) | No | 51 | 8 | 0.592 | 46 | 13 | 0.687 | 54 | 5 | 1.000 |
| Yes | 10 | 0 | 7 | 3 | 9 | 1 | ||||
| Insufficiency (n) | No | 24 | 3 | 1.000 | 19 | 8 | 0.385 | 25 | 2 | 1.000 |
| Yes | 37 | 5 | 34 | 8 | 38 | 4 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parant, F.; Bouloy, J.; Haesebaert, J.; Bendim’red, L.; Goldet, K.; Vanhems, P.; Henaff, L.; Gilbert, T.; Cuerq, C.; Blond, E.; et al. Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation. Nutrients 2022, 14, 1641. https://doi.org/10.3390/nu14081641
Parant F, Bouloy J, Haesebaert J, Bendim’red L, Goldet K, Vanhems P, Henaff L, Gilbert T, Cuerq C, Blond E, et al. Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation. Nutrients. 2022; 14(8):1641. https://doi.org/10.3390/nu14081641
Chicago/Turabian StyleParant, François, Justin Bouloy, Julie Haesebaert, Lamia Bendim’red, Karine Goldet, Philippe Vanhems, Laetitia Henaff, Thomas Gilbert, Charlotte Cuerq, Emilie Blond, and et al. 2022. "Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation" Nutrients 14, no. 8: 1641. https://doi.org/10.3390/nu14081641
APA StyleParant, F., Bouloy, J., Haesebaert, J., Bendim’red, L., Goldet, K., Vanhems, P., Henaff, L., Gilbert, T., Cuerq, C., Blond, E., Bost, M., & Bonnefoy, M. (2022). Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation. Nutrients, 14(8), 1641. https://doi.org/10.3390/nu14081641