
Association of Abnormal Iron Status with the Occurrence and Prognosis of Peritoneal Dialysis-Related Peritonitis: A Longitudinal Data-Based 10-Year Retrospective Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
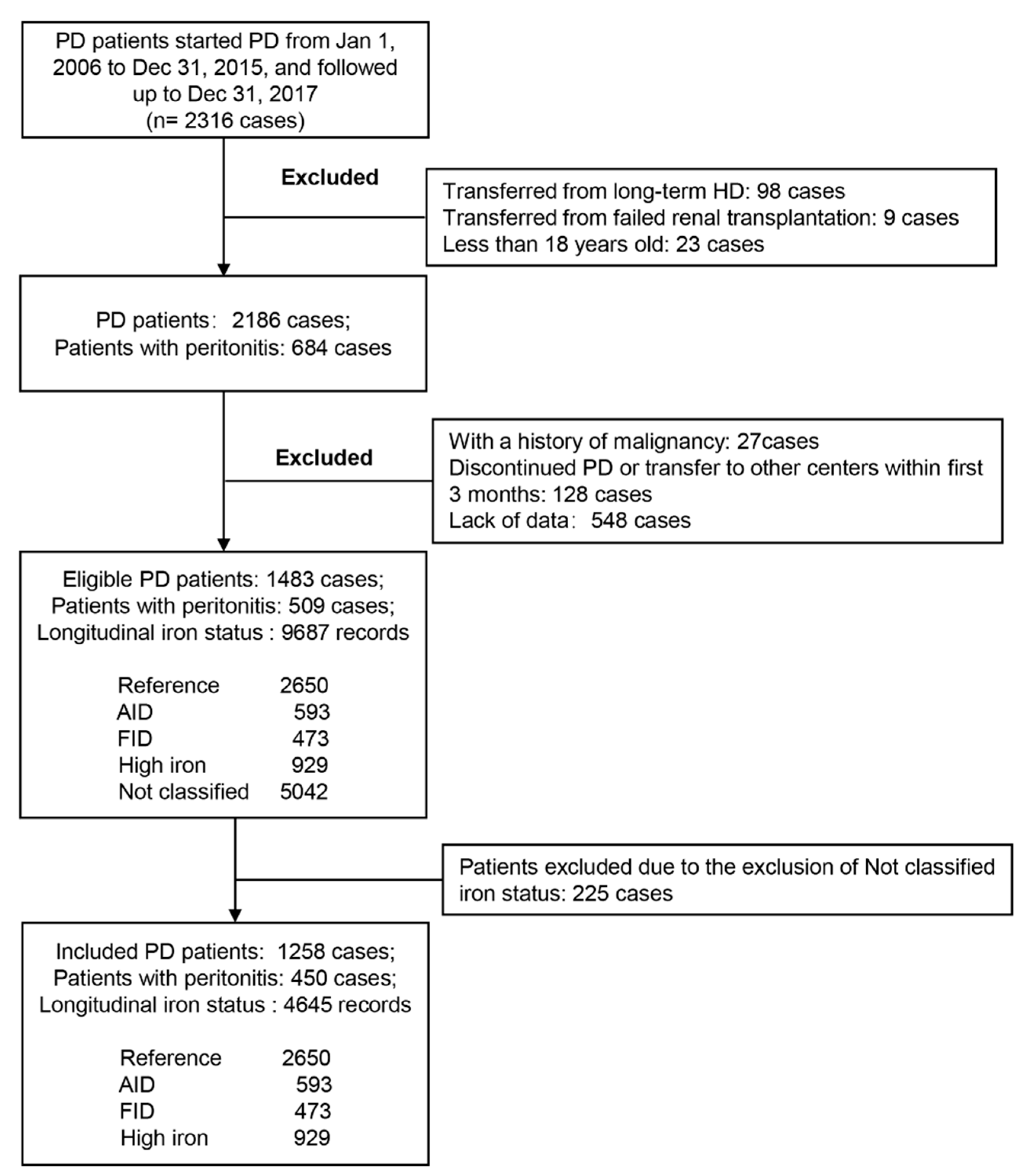
2.1. Study Population
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analyses
3. Results
3.1. Clinical Characteristics between Different Iron Groups at Baseline
3.2. Baseline Iron Status Was Not Associated with the Occurrence of Peritonitis
3.3. Relationship between Longitudinal Iron Status and the Occurrence of Peritonitis
3.4. Relationship between Longitudinal Iron Status and the Prognosis of Peritonitis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Afzali, B.; Goldsmith, D.J. Intravenous iron therapy in renal failure: Friend and foe? J. Nephrol. 2004, 17, 487–495. [Google Scholar] [PubMed]
- Issad, B.; Griuncelli, M.; Verger, C.; Rostoker, G. What do we learn about the “Anemia Module” of the French language peritoneal dialysis? Interest and results. Bull Dial. Domic. 2019, 2, 143–149. [Google Scholar] [CrossRef]
- Locatelli, F.; Barany, P.; Covic, A.; De Francisco, A.; Del, V.L.; Goldsmith, D.; Horl, W.; London, G.; Vanholder, R.; Van Biesen, W. Kidney Disease: Improving Global Outcomes guidelines on anaemia management in chronic kidney disease: A European Renal Best Practice position statement. Nephrol. Dial. Transplant. 2013, 28, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Rostoker, G.; Griuncelli, M.; Ghali, N.; Beaudreuil, S.; Cohen, Y.; Issad, B. Hepatic iron load differs strikingly between peritoneal dialysis and hemodialysis patients. Bull Dial. Domic. 2019, 2, 181–189. [Google Scholar] [CrossRef]
- Perlman, R.L.; Zhao, J.; Fuller, D.S.; Bieber, B.; Li, Y.; Pisoni, R.L.; Robinson, B.M.; Johnson, D.W.; Kawanishi, H.; Davies, S.J.; et al. International Anemia Prevalence and Management in Peritoneal Dialysis Patients. Perit. Dial. Int. 2019, 39, 539–546. [Google Scholar] [CrossRef]
- Babitt, J.L.; Eisenga, M.F.; Haase, V.H.; Kshirsagar, A.V.; Levin, A.; Locatelli, F.; Malyszko, J.; Swinkels, D.W.; Tarng, D.C.; Cheung, M.; et al. Controversies in optimal anemia management: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2021, 99, 1280–1295. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; Li, P.K. Peritoneal Dialysis-Associated Peritonitis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1100–1105. [Google Scholar] [CrossRef]
- Aldriwesh, M.; Al-Dayan, N.; Barratt, J.; Freestone, P. The Iron Biology Status of Peritoneal Dialysis Patients May Be a Risk Factor for Development of Infectious Peritonitis. Perit. Dial. Int. 2019, 39, 362–374. [Google Scholar] [CrossRef]
- Cho, M.E.; Hansen, J.L.; Peters, C.B.; Cheung, A.K.; Greene, T.; Sauer, B.C. An increased mortality risk is associated with abnormal iron status in diabetic and non-diabetic Veterans with predialysis chronic kidney disease. Kidney Int. 2019, 96, 750–760. [Google Scholar] [CrossRef]
- Mehta, R.C.; Cho, M.E.; Cai, X.; Lee, J.; Chen, J.; He, J.; Flack, J.; Shafi, T.; Saraf, S.L.; David, V.; et al. Iron status, fibroblast growth factor 23 and cardiovascular and kidney outcomes in chronic kidney disease. Kidney Int. 2021, 100, 1292–1302. [Google Scholar] [CrossRef]
- Li, P.K.; Szeto, C.C.; Piraino, B.; de Arteaga, J.; Fan, S.; Figueiredo, A.E.; Fish, D.N.; Goffin, E.; Kim, Y.L.; Salzer, W.; et al. ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit. Dial. Int. 2016, 36, 481–508. [Google Scholar] [CrossRef]
- Wu, H.; Ye, H.; Huang, R.; Yi, C.; Wu, J.; Yu, X.; Yang, X. Incidence and risk factors of peritoneal dialysis-related peritonitis in elderly patients: A retrospective clinical study. Perit. Dial. Int. 2020, 40, 26–33. [Google Scholar] [CrossRef] [PubMed]
- UK, N.C.G.C. Anaemia Management in Chronic Kidney Disease: Partial Update 2015; Royal College of Physicians: London, UK, 2015. [Google Scholar]
- Tsubakihara, Y.; Nishi, S.; Akiba, T.; Hirakata, H.; Iseki, K.; Kubota, M.; Kuriyama, S.; Komatsu, Y.; Suzuki, M.; Nakai, S.; et al. 2008 Japanese Society for Dialysis Therapy: Guidelines for renal anemia in chronic kidney disease. Ther. Apher. Dial. 2010, 14, 240–275. [Google Scholar] [CrossRef]
- KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease. Am. J. Kidney Dis. 2006, 47, S11–S145.
- Tansarli, G.S.; Karageorgopoulos, D.E.; Kapaskelis, A.; Gkegkes, I.; Falagas, M.E. Iron deficiency and susceptibility to infections: Evaluation of the clinical evidence. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 1253–1258. [Google Scholar] [CrossRef]
- Sato, M.; Hanafusa, N.; Tsuchiya, K.; Kawaguchi, H.; Nitta, K. Impact of Transferrin Saturation on All-Cause Mortality in Patients on Maintenance Hemodialysis. Blood Purif. 2019, 48, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Marx, J.J. Iron and infection: Competition between host and microbes for a precious element. Best Pract. Res. Clin. Haematol. 2002, 15, 411–426. [Google Scholar] [CrossRef]
- Nairz, M.; Dichtl, S.; Schroll, A.; Haschka, D.; Tymoszuk, P.; Theurl, I.; Weiss, G. Iron and innate antimicrobial immunity-Depriving the pathogen, defending the host. J. Trace Elem. Med. Biol. 2018, 48, 118–133. [Google Scholar] [CrossRef]
- Ekiz, C.; Agaoglu, L.; Karakas, Z.; Gurel, N.; Yalcin, I. The effect of iron deficiency anemia on the function of the immune system. Hematol. J. 2005, 5, 579–583. [Google Scholar] [CrossRef]
- Aly, S.S.; Fayed, H.M.; Ismail, A.M.; Abdel, H.G. Assessment of peripheral blood lymphocyte subsets in children with iron deficiency anemia. BMC Pediatr. 2018, 18, 49. [Google Scholar] [CrossRef]
- Guedes, M.; Muenz, D.G.; Zee, J.; Bieber, B.; Stengel, B.; Massy, Z.A.; Mansencal, N.; Wong, M.; Charytan, D.M.; Reichel, H.; et al. Serum Biomarkers of Iron Stores Are Associated with Increased Risk of All-Cause Mortality and Cardiovascular Events in Nondialysis CKD Patients, with or without Anemia. J. Am. Soc. Nephrol. 2021, 32, 2020–2030. [Google Scholar] [CrossRef]
- Luo, D.; Zhong, Z.; Qiu, Y.; Wang, Y.; Li, H.; Lin, J.; Chen, W.; Yang, X.; Mao, H. Abnormal iron status is associated with an increased risk of mortality in patients on peritoneal dialysis. Nutr. Metab. Cardiovasc Dis. 2021, 31, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Vandenesch, F.; Lina, G.; Henry, T. Staphylococcus aureus hemolysins, bi-component leukocidins, and cytolytic peptides: A redundant arsenal of membrane-damaging virulence factors? Front. Cell Infect. Microbiol. 2012, 2, 12. [Google Scholar] [CrossRef] [PubMed]
- May, A.K.; Gleason, T.G.; Sawyer, R.G.; Pruett, T.L. Contribution of Escherichia coli alpha-hemolysin to bacterial virulence and to intraperitoneal alterations in peritonitis. Infect. Immun. 2000, 68, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Pastor, M.T.; Puig, S. Adaptation to iron deficiency in human pathogenic fungi. Biochim. Biophys. Acta Mol. Cell Res. 2020, 1867, 118797. [Google Scholar] [CrossRef]
- Ueda, N.; Takasawa, K. Impact of Inflammation on Ferritin, Hepcidin and the Management of Iron Deficiency Anemia in Chronic Kidney Disease. Nutrients 2018, 10, 1173. [Google Scholar] [CrossRef]
- Galic, G.; Tomic, M.; Galesic, K.; Kvesic, A.; Soljic, M.; Londar, Z.; Valencic, M.; Martinovic, Z.; Vuckov, S. The etiological relation between serum iron level and infection incidence in hemodialysis uremic patients. Coll. Antropol. 2011, 35, 93–101. [Google Scholar] [PubMed]
- Teehan, G.S.; Bahdouch, D.; Ruthazer, R.; Balakrishnan, V.S.; Snydman, D.R.; Jaber, B.L. Iron storage indices: Novel predictors of bacteremia in hemodialysis patients initiating intravenous iron therapy. Clin. Infect. Dis. 2004, 38, 1090–1094. [Google Scholar] [CrossRef][Green Version]
- Teehan, G.S.; Ruthazer, R.; Balakrishnan, V.S.; Snydman, D.; Jaber, B.L. Iron storage indices and risk of bacterial infections in hemodialysis patients. Hemodial. Int. 2004, 8, 226–232. [Google Scholar] [CrossRef]
- Kuragano, T.; Matsumura, O.; Matsuda, A.; Hara, T.; Kiyomoto, H.; Murata, T.; Kitamura, K.; Fujimoto, S.; Hase, H.; Joki, N.; et al. Association between hemoglobin variability, serum ferritin levels, and adverse events/mortality in maintenance hemodialysis patients. Kidney Int. 2014, 86, 845–854. [Google Scholar] [CrossRef]
- Sirken, G.; Raja, R.; Rizkala, A.R. Association of different intravenous iron preparations with risk of bacteremia in maintenance hemodialysis patients. Clin. Nephrol. 2006, 66, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Hougen, I.; Collister, D.; Bourrier, M.; Ferguson, T.; Hochheim, L.; Komenda, P.; Rigatto, C.; Tangri, N. Safety of Intravenous Iron in Dialysis: A Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Macdougall, I.C.; Bhandari, S.; White, C.; Anker, S.D.; Farrington, K.; Kalra, P.A.; Mark, P.B.; McMurray, J.; Reid, C.; Robertson, M.; et al. Intravenous Iron Dosing and Infection Risk in Patients on Hemodialysis: A Prespecified Secondary Analysis of the PIVOTAL Trial. J. Am. Soc. Nephrol. 2020, 31, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Vychytil, A.; Haag-Weber, M. Iron status and iron supplementation in peritoneal dialysis patients. Kidney Int. Suppl. 1999, 69, S71–S78. [Google Scholar] [CrossRef]
- Allen, J.R.; Troidle, L.K.; Juergensen, P.H.; Kliger, A.S.; Finkelstein, F.O. Incidence of peritonitis in chronic peritoneal dialysis patients infused with intravenous iron dextran. Perit. Dial. Int. 2000, 20, 674–678. [Google Scholar] [CrossRef]
- Ganz, T.; Aronoff, G.R.; Gaillard, C.; Goodnough, L.T.; Macdougall, I.C.; Mayer, G.; Porto, G.; Winkelmayer, W.C.; Wish, J.B. Iron Administration, Infection, and Anemia Management in CKD: Untangling the Effects of Intravenous Iron Therapy on Immunity and Infection Risk. Kidney Med. 2020, 2, 341–353. [Google Scholar] [CrossRef]
- Handa, P.; Thomas, S.; Morgan-Stevenson, V.; Maliken, B.D.; Gochanour, E.; Boukhar, S.; Yeh, M.M.; Kowdley, K.V. Iron alters macrophage polarization status and leads to steatohepatitis and fibrogenesis. J. Leukoc. Biol. 2019, 105, 1015–1026. [Google Scholar] [CrossRef]
- Deicher, R.; Ziai, F.; Cohen, G.; Mullner, M.; Horl, W.H. High-dose parenteral iron sucrose depresses neutrophil intracellular killing capacity. Kidney Int. 2003, 64, 728–736. [Google Scholar] [CrossRef]
- Bonanni, A.; Mannucci, I.; Verzola, D.; Sofia, A.; Saffioti, S.; Gianetta, E.; Garibotto, G. Protein-energy wasting and mortality in chronic kidney disease. Int. J. Environ. Res. Public Health 2011, 8, 1631–1654. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, M.; Cobo, G.; Lindholm, B.; Stenvinkel, P. Inflammation and Protein-Energy Wasting in the Uremic Milieu. Contrib. Nephrol. 2017, 191, 58–71. [Google Scholar]
- Kalantar-Zadeh, K.; Kalantar-Zadeh, K.; Lee, G.H. The fascinating but deceptive ferritin: To measure it or not to measure it in chronic kidney disease? Clin. J. Am. Soc. Nephrol. 2006, 1 (Suppl. 1), S9–S18. [Google Scholar] [CrossRef] [PubMed]
- Gomme, P.T.; McCann, K.B.; Bertolini, J. Transferrin: Structure, function and potential therapeutic actions. Drug Discov. Today 2005, 10, 267–273. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Baseline Iron Status | p Value | |||
|---|---|---|---|---|---|
| RIS (n = 369) | AID (n = 148) | FID (n = 134) | HIS (n = 118) | ||
| Demographics | |||||
| Male, n (%) | 240 (65.0) | 45 (30.4) | 92 (68.7) | 90 (76.3) | <0.001 |
| Age (years) | 48.1 ± 14.8 | 46.8 ± 15.9 | 48.0 ± 15.6 | 44.1 ± 15.4 | 0.07 |
| BMI (kg/m2) | 21.8 ± 3.01 | 21.1 ± 3.35 | 21.6 ± 2.93 | 21.5 ± 2.98 | 0.04 |
| Diabetes, n (%) | 86 (23.3) | 32 (21.6) | 33 (24.6) | 29 (24.6) | 0.93 |
| Assisted PD | 101 (27.4) | 39 (26.4) | 40 (29.9) | 22 (18.6) | 0.19 |
| CCI | 3.53 ± 1.70 | 3.48 ± 1.846 | 3.56 ± 1.85 | 3.46 ± 1.81 | 0.76 |
| Primary kidney disease | 0.61 | ||||
| Chronic glomerulonephritis, n (%) | 225 (61.0) | 91 (61.5) | 68 (50.7) | 71 (60.2) | |
| Diabetic nephropathy, n (%) | 74 (20.1) | 28 (18.9) | 30 (22.4) | 27 (22.9) | |
| Hypertensive nephropathy, n (%) | 29 (7.9) | 11 (7.4) | 15 (11.2) | 10 (8.5) | |
| Other, n (%) | 41 (11.1) | 18 (12.2) | 21 (15.7) | 10 (8.5) | |
| Laboratory parameter | |||||
| Hemoglobin (g/dL) | 11.3 ± 1.54 | 10.8 ± 1.83 | 10.2 ± 1.98 | 10.6 ± 2.03 | <0.001 |
| Hs-CRP (mg/L) | 1.73 (0.68–5.64) | 1.47 (0.53–3.91) | 3.83 (1.03–10.8) | 1.62 (0.59–3.61) | <0.001 |
| Neutrophil/lymphocyte ratio | 2.63 (2.13–3.59) | 2.74 (2.22–3.80) | 3.11 (2.36–4.03) | 2.76 (2.09–3.70) | 0.01 |
| Albumin (g/L) | 37.5 ± 4.28 | 37.7 ± 4.83 | 36.8 ± 5.65 | 36.9 ± 4.83 | 0.36 |
| Serum creatinine (μmol/L) | 684 (563–889) | 671 (571–784) | 735 (558–984) | 768 (599–951) | 0.01 |
| Total cholesterol (mmol/L) | 5.00 (4.30–5.80) | 5.10 (4.40–5.90) | 5.10 (4.20–5.80) | 4.95 (4.20–5.70) | 0.68 |
| Urea acid (μmol/L) | 420 ± 92.6 | 398 ± 85.2 | 420 ± 107 | 435 ± 80.3 | 0.005 |
| Residual GFR (mL/min/1.73 m2) | 5.62 (4.13–7.15) | 4.63 (3.30–6.76) | 4.63 (3.87–6.14) | 5.48 (4.19–7.67) | 0.003 |
| Serum iron (μmol/L) | 10.7 ± 3.04 | 5.15 ± 2.25 | 5.54 ± 2.53 | 17.2 ± 5.15 | <0.001 |
| Transferrin saturation (%) | 19.0 (15.7–22.9) | 7.85 (5.66–10.2) | 9.42 (7.42–11.0) | 35.3 (30.5–43.0) | <0.001 |
| Ferritin (ng/mL) | 147 (110–209) | 26.5 (15.6–41.9) | 266 (199–461) | 458 (359–670) | <0.001 |
| Medications | |||||
| ESAs users, n (%) | 310 (87.3) | 141 (96.6) | 115 (91.3) | 87 (77.0) | <0.001 |
| Iron users, n (%) | 259 (73.0) | 113 (77.4) | 87 (69.0) | 72 (63.7) | 0.09 |
| Variables | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | AOR (95% CI) | p Value | |
| Age | 1.02 (1.01, 1.03) | <0.001 | 1.02 (1.00, 1.03) | 0.03 |
| Male gender | 0.80 (0.63, 1.03) | 0.08 | 0.90 (0.69, 1.16) | 0.39 |
| Diabetes | 1.02 (0.78, 1.33) | 0.88 | - | - |
| CCI | 1.13 (1.06, 1.21) | <0.001 | 0.92 (0.82, 1.04) | 0.18 |
| PD vintage (per 0.5 year) | 1.02 (0.99, 1.05) | 0.19 | 0.99 (0.96, 1.02) | 0.52 |
| ALB | 0.86 (0.84, 0.88) | <0.001 | 0.87 (0.84, 0.89) | <0.001 |
| Hb | 0.99 (0.98, 0.99) | <0.001 | 1.00 (0.99, 1.01) | 0.97 |
| Hs-CRP | 1.02 (1.01, 1.03) | <0.001 | 1.00 (0.99, 1.01) | 0.36 |
| N/L ratio | 1.13 (1.07, 1.19) | <0.001 | 1.06 (1.01, 1.11) | 0.02 |
| Iron status | ||||
| RIS | Ref. | Ref. | ||
| AID | 1.72 (1.22, 2.42) | 0.002 | 1.45 (1.06, 2.00) | 0.02 |
| FID | 1.93 (1.43, 2.60) | <0.001 | 1.33 (0.92, 1.91) | 0.13 |
| HIS | 1.22 (0.92, 1.63) | 0.17 | 1.25 (0.91, 1.71) | 0.17 |
| Variables | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | AHR (95% CI) | p Value | |
| Age | 1.00 (0.99, 1.02) | 0.81 | 0.99 (0.97, 1.01) | 0.26 |
| Male gender | 0.77 (0.49, 1.21) | 0.26 | 0.75 (0.46, 1.21) | 0.24 |
| Diabetes | 1.37 (0.84, 2.23) | 0.21 | 1.61 (0.92, 2.85) | 0.10 |
| CCI | 1.09 (0.96, 1.23) | 0.20 | - | - |
| ALB | 0.92 (0.88, 0.96) | <0.001 | 0.92 (0.87, 0.98) | 0.008 |
| Hb | 0.98 (0.97, 0.99) | 0.002 | 0.99 (0.98, 1.01) | 0.13 |
| Hs-CRP | 1.01 (1.00, 1.01) | 0.008 | 1.00 (0.99, 1.01) | 0.38 |
| N/L ratio | 1.05 (0.99, 1.11) | 0.07 | 1.01 (0.94, 1.08) | 0.80 |
| Iron status | ||||
| RIS | Ref. | Ref. | ||
| AID | 2.16 (1.17, 3.98) | 0.01 | 1.85 (1.01, 3.39) | 0.04 |
| FID | 2.14 (1.11, 4.14) | 0.02 | 1.89 (0.97, 3.69) | 0.06 |
| HIS | 2.33 (1.28, 4.24) | 0.005 | 2.70 (1.39, 5.25) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diao, X.; Zheng, Z.; Yi, C.; Cao, P.; Ye, H.; Liu, R.; Lin, J.; Chen, W.; Mao, H.; Huang, F.; et al. Association of Abnormal Iron Status with the Occurrence and Prognosis of Peritoneal Dialysis-Related Peritonitis: A Longitudinal Data-Based 10-Year Retrospective Study. Nutrients 2022, 14, 1613. https://doi.org/10.3390/nu14081613
Diao X, Zheng Z, Yi C, Cao P, Ye H, Liu R, Lin J, Chen W, Mao H, Huang F, et al. Association of Abnormal Iron Status with the Occurrence and Prognosis of Peritoneal Dialysis-Related Peritonitis: A Longitudinal Data-Based 10-Year Retrospective Study. Nutrients. 2022; 14(8):1613. https://doi.org/10.3390/nu14081613
Chicago/Turabian StyleDiao, Xiangwen, Zhiwei Zheng, Chunyan Yi, Peiyi Cao, Hongjian Ye, Ruihua Liu, Jianxiong Lin, Wei Chen, Haiping Mao, Fengxian Huang, and et al. 2022. "Association of Abnormal Iron Status with the Occurrence and Prognosis of Peritoneal Dialysis-Related Peritonitis: A Longitudinal Data-Based 10-Year Retrospective Study" Nutrients 14, no. 8: 1613. https://doi.org/10.3390/nu14081613
APA StyleDiao, X., Zheng, Z., Yi, C., Cao, P., Ye, H., Liu, R., Lin, J., Chen, W., Mao, H., Huang, F., & Yang, X. (2022). Association of Abnormal Iron Status with the Occurrence and Prognosis of Peritoneal Dialysis-Related Peritonitis: A Longitudinal Data-Based 10-Year Retrospective Study. Nutrients, 14(8), 1613. https://doi.org/10.3390/nu14081613