
A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms

 , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
2.1. Literature Search
2.2. Trial Selection
2.3. Data Extraction
2.4. Quality Assessment of the Included Studies
2.5. Statistical Analysis
3. Results
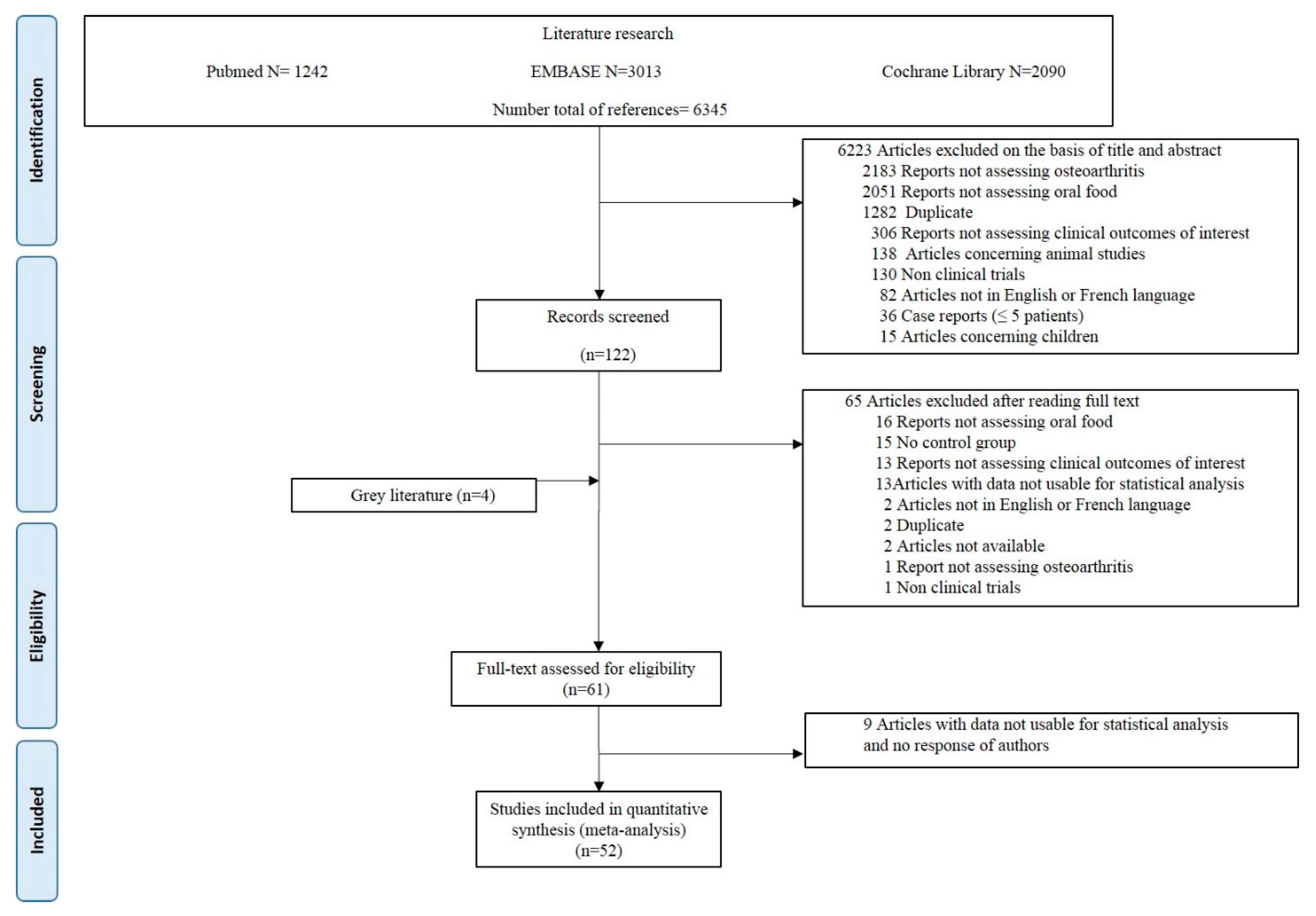
3.1. Literature Selection

3.2. Characteristics of the Included Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Disease | No. of Participants | Intervention | Dose | Duration (wks) | Control | Jadad Score | Measures | |
|---|---|---|---|---|---|---|---|---|---|
| Intervention | Total | ||||||||
| Atabaki [25] | KOA | 15 | 15 | Curcumin | 80 mg/d | 12 | Placebo | 5 | VAS pain, ESR, CRP |
| Haroyan [26] | KOA | 66 | 68 | Curcumin | 1500 mg/d | 12 | Placebo | 5 | Total WOMAC, VAS pain, ESR, CRP |
| Henrotin [27] | KOA | 49 | 45 | Curcumin | 380 mg/d | 12 | Placebo | 5 | KOOS, function, QoL |
| Khanna [28] | KOA | 40 | 40 | Curcumin | NA | 12 | Chondroitin | 3 | Total WOMAC, stiffness, VAS pain |
| Kuptniratsaikul 2014 [29] | KOA | 171 | 160 | Curcumin | 1500 mg/d | 4 | NSAID | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Kuptniratsaikul 2009 [30] | KOA | 52 | 55 | Curcumin | 2000 mg/d | 6 | NSAID | 4 | VAS pain |
| Madhu [31] | KOA | 29 | 29 | Curcumin | 1000 mg/d | 6 | Placebo | 4 | Total WOMAC, VAS pain |
| Panda [32] | KOA | 25 | 25 | Curcumin | 500 mg/d | 12 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Shep [33] | KOA | 71 | 69 | Curcumin | 500 mg/d | 4 | NSAID | 1 | VAS pain, function, QoL |
| Singhal [34] | KOA | 73 | 71 | Curcumin | 1000 mg/d | 6 | Paracetamol | 3 | Total WOMAC |
| Srivastava [35] | KOA | 78 | 82 | Curcumin | NA | 16 | Placebo | 5 | Stiffness, function, VAS pain |
| Wang [36] | KOA | 36 | 34 | Curcumin | 1000 mg/d | 12 | Placebo | 5 | Stiffness, function, VAS pain, QoL |
| Panahi [37] | KOA | 19 | 21 | Curcumin | 1500 mg/d | 6 | Placebo | 4 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Altman [38] | KOA | 247 | 124 | Ginger | NA | 6 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain, QoL |
| Wigler [39] | KOA | 29 | 14 | Ginger | 250 mg/d | 12 | Placebo | 4 | VAS pain, VAS activity |
| Bolognesi [40] | KOA | 54 | 28 | Ginger | NA | 24 | Placebo | 0 | VAS pain, stiffness, function, ESR, CRP |
| Jin [41] | KOA | 413 | 209 | Vitamin D3 | 50,000 IU/m | 96 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| MacAlindon [42] | KOA | 146 | 73 | Vitamin D3 | 2000 IU/d | 96 | Placebo | 5 | VAS pain, function |
| Sanghi [43] | KOA | 103 | 52 | Vitamin D3 | 60,000 IU/m | 48 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Medhi [44] | KOA | 50 | 50 | Vitamin E | 200 IU/d | 8 | Placebo | 2 | VAS pain |
| Dehghan [45] | KOA | 35 | 38 | Vitamin E | NA | 3 | Placebo | 2 | Stiffness, function, VAS pain |
| Tantavisut [46] | KOA | 31 | 35 | Vitamin E | 400 IU/d | 8 | Placebo | 5 | Stiffness, function, VAS pain |
| Wluka [47] | KOA | 67 | 69 | Vitamin E | 500 IU/d | 96 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Essouiri [48] | KOA | 51 | 49 | Vitamin E | NA | 8 | Placebo | 1 | Stiffness, function, VAS pain |
| Colker [49] | KOA | 16 | 15 | Multivitamin | NA | 6 | Placebo | 4 | Total WOMAC, VAS pain, KOOS for pain, KOOS for function, KOOS for QoL |
| Frestedt [50] | KOA | 20 | 16 | Multivitamin | NA | 12 | Placebo | 5 | Stiffness, function, VAS pain |
| Jacquet [51] | KOA | 41 | 40 | Omega-3 | NA | 12 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Stammers [52] | OA | 44 | 43 | Omega-3 | NA | 24 | Placebo | 3 | VAS pain |
| Chopra [53] | KOA | 45 | 45 | Herbal | NA | 32 | Placebo | 3 | Stiffness, VAS pain |
| Guo [54] | KOA | 21 | 21 | Herbal | NA | 2 | NSAID | abs | VAS pain |
| Tao [55] | KOA | 45 | 45 | Herbal | NA | 8 | Glucosamine | 1 | Total WOMAC, VAS pain, ESR, CRP |
| Wu [56] | KOA | 30 | 20 | Herbal | NA | 2 | NSAID | 1 | Stiffness, VAS pain |
| Farpour [57] | KOA | 18 | 20 | Herbal | NA | 8 | NSAID | 4 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Gupta [58] | KOA | 44 | 44 | Herbal | NA | 12 | Placebo | 3 | VAS pain |
| Hamblin [59] | KOA | 9 | 5 | Herbal | NA | 10 | Placebo | 4 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Karimifar [60] | KOA | 26 | 26 | Herbal | NA | 4 | NSAID | 3 | VAS pain, VAS activity |
| Karlapundi [61] | KOA | 34 | 32 | Herbal | NA | 12 | Placebo | 3 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Koonrungsesomboon [62] | KOA | 100 | 100 | Herbal | NA | 4 | NSAID | 5 | Stiffness, VAS pain, KOOS for pain, KOOS for function, KOOS for QoL |
| Moré [63] | KOA | 46 | 44 | Herbal | NA | 12 | Placebo | 3 | Total WOMAC, stiffness, VAS pain |
| Thomford [64] | OA | 44 | 11 | Herbal | NA | 8 | NSAID | 4 | VAS pain |
| Kakatum [65] | KOA | 32 | 31 | Herbal | NA | 4 | NSAID | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Pinsornsak [66] | KOA | 31 | 30 | Herbal | NA | 4 | NSAID | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Liu [67] | HOA | 52 | 54 | Herbal | NA | 12 | Placebo | 5 | VAS pain, VAS activity, function, QoL |
| Schumacher [68] | KOA | 26 | 22 | Cherry | NA | 6 | Placebo | 5 | Stiffness |
| Puente [69] | KOA | 30 | 30 | Beeswax | NA | 6 | Placebo | 4 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Shin [70] | KOA | 26 | 24 | Deer bone | NA | 12 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Salimzadeh [71] | KOA | 39 | 37 | Garlic | NA | 12 | Placebo | 5 | Total WOMAC, WOMAC function, stiffness, VAS pain |
| Lau [72] | KOA | 40 | 40 | Green mussel | NA | 24 | Placebo | 3 | VAS pain, VAS activity |
| Zawadzki [73] | KOA | 25 | 25 | Green mussel | NA | 12 | Fish oil | 5 | VAS pain, VAS activity |
| May [74] | KOA | 38 | 37 | Melon | NA | 12 | Placebo | 5 | KOOS for pain, KOOS for function, KOOS for QoL |
| Sadat [75] | KOA | 22 | 23 | Sesame | NA | 8 | Placebo | 1 | VAS pain |
| Schell [76] | KOA | 8 | 9 | Strawberries | NA | 12 | Placebo | 5 | VAS pain, CRP |
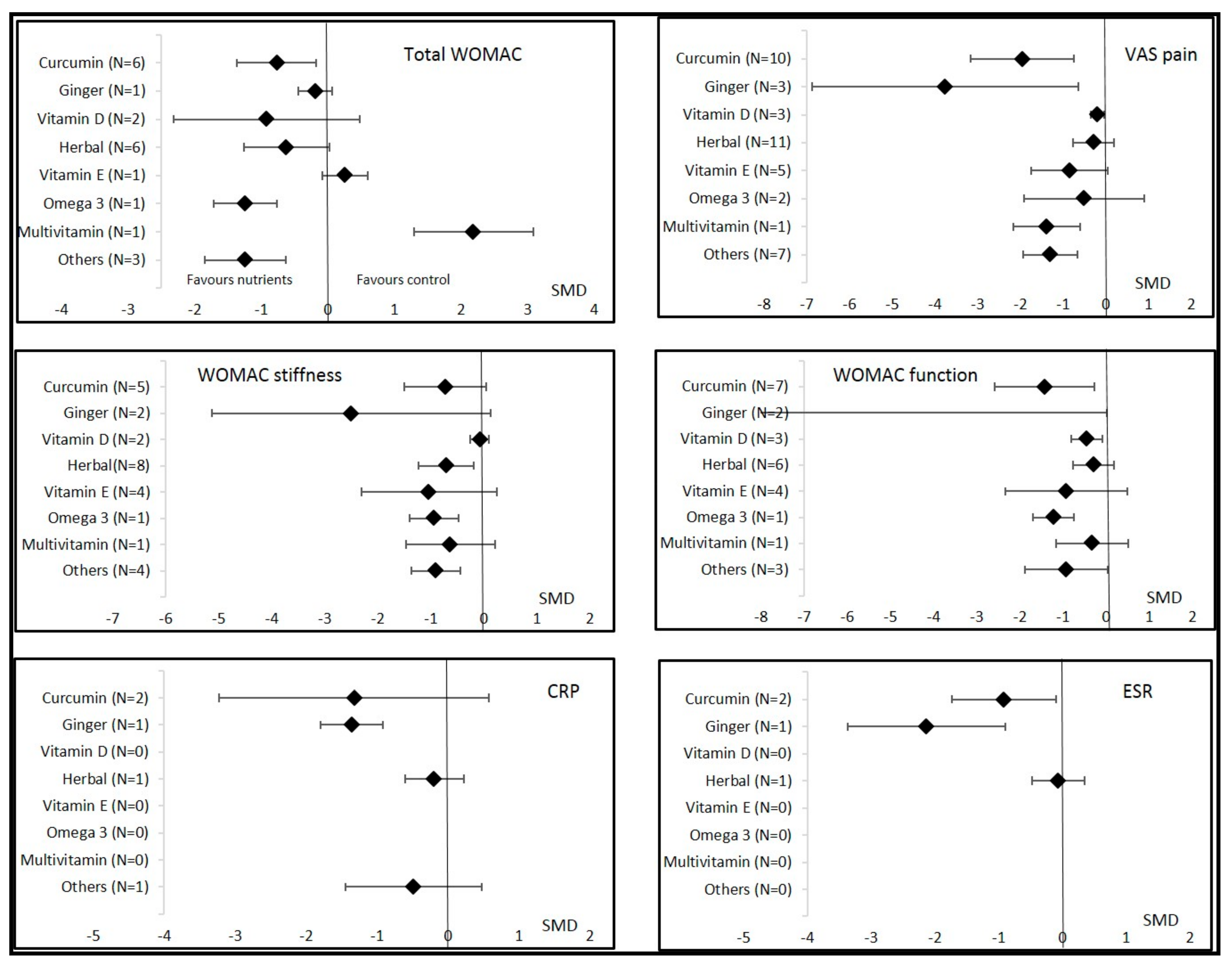
3.3. Overall Effects of Nutritional Supplements on OA Symptoms
3.3.1. Vitamin D
3.3.2. Curcumin
| Measure | Time Point | Vitamin D | Curcumin | Ginger | Vitamin E | Herbal | Multivitamin | Omega-3 | Others |
|---|---|---|---|---|---|---|---|---|---|
| WOMAC total | Overall 1 month 3 months 6 months 12 months 24 months | −0.92 (−2.32; 0.48) I2 = 97% −1.65 (−2.10; −1.20) −0.22 (−0.42; −0.03) | −0.78 (−1.31; −0.24) I2 = 92% −0.77 (−1.53; −0.01) −0.80 (−1.84; 0.24) | −0.19 (−0.44; 0.06) I2 = NA −0.19 (−0.44; 0.06) | 0.26 (−0.08; 0.60) I2 = NA 0.26 (−0.08; 0.60) | −0.62 (−1.26; 0.02) I2 = 88% −0.08 (−0.43; 0.27) −1.02 (−2.10; 0.07) | 2.19 (1.29; 3.09) I2 = NA 2.19 (1.29; 3.09) | −1.24 (−1.71; −0.76) I2 = NA −1.24 (−1.71; −0.76) | −1.24 (−1.85; −0.63) I2 = 78% −1.64 (−2.12; −1.17) −0.85 (−1.57; −0.13) |
| WOMAC stiffness | Overall 1 month 3 months 6 months 12 months 24 months | −0.07 (−0.25; 0.10) I2 = 0% 0.05 (−0.33; 0.44) −0.11 (−0.30; 0.09) | −0.61 (−1.29; 0.06) I2 = 94% −0.26 (−0.89; 0.38) −0.95 (−1.87; −0.03) | −2.50 (−5.13; 0.13) I2 = 98% −1.77 (−4.75; 1.20) −3.97 (−4.90; −3.04) | −1.04 (−2.31; 0.24) I2 = 97% 0.13 (−0.33; 0.59) −2.38 (−6.50; 1.74) 0.19 (−0.15; 0.53) | −0.71 (−1.23; −0.19) I2 = 89% −0.03 (−0.29; 0.23) −1.28 (−1.95; −0.62) −1.81 (−2.40; −1.21) | −0.63 (−1.47; 0.22) I2 = NA −0.63 (−1.47; 0.22) | −0.94 (−1.40; −0.48) I2 = NA −0.94 (−1.40; −0.48) | −0.90 (−1.37; −0.44) I2 = 71% −0.91 (−1.49; −0.33) −0.92 (−1.98; 0.14) |
| VAS pain | Overall 1 month 3 months 6 months 12 months 24 months | −0.20 (−0.35; −0.04) I2 = 0% −0.13 (−0.51; 0.26) −0.21 (0.38; −0.04) | −1.81 (−2.93; −0.69) I2 = 98% −0.10 (−1.34; 1.15) −4.5 (−6.85; −2.15) | −3.76 (−6.88; −0.65) I2 = 98% −3.64 (−10.47; 3.19) −0.28 (−1.09; 0.53) −7.79 (−9.38; −6.20) | −0.84 (−1.75; 0.05) I2 = 96% 0.23 (−0.07; 0.53) −2.06 (−3.91; −0.20) 0.22 (−0.11; 0.56) | −0.28 (−0.76; 0.19) I2 = 88% −0.02 (−0.61; 0.57) −0.04 (−0.42; 0.35) −2.78 (−3.49; −2.08) | −1.38 (−2.16; −0.59) I2 = NA −1.38 (−2.16; −0.59) | −0.51 (−1.92; 0.90) I2 = 94% −1.23 (−1.71; −0.75) 0.21 (−0.31; 0.73) | −1.30 (−1.93; −0.66) I2 = 92% −1.24 (−2.44; −0.05) −1.46 (−2.50; −0.41) −0.81 (−1.27; −0.35) |
| KOOS pain | Overall 1 month 3 months 6 months 12 months 24 months | 1.19 (0.42; 1.96) I2 = NA 1.19 (0.42; 1.96) | 0.33 (−0.13; 0.78) I2 = NA 0.33 (−0.13; 0.78) | ||||||
| VAS activity | Overall 1 month 3 months 6 months 12 months 24 months | −0.31 (−1.12; 0.50) I2 = NA −0.31 (−1.12; 0.50) | −0.02 (−0.40; 0.36) I2 = NA −0.02 (−0.40; 0.36) | −1.23 (−2.20; −0.26) I2 = 94% −1.24 (−4.01; 1.54) −1.61 (−3.68; 0.46) −0.61 (−1.06; −0.16) | |||||
| WOMAC function | Overall 1 month 3 months 6 months 12 months 24 months | −0.44 (−0.80; −0.09) I2 = 76% −0.90 (−1.31; −0.50) −0.44 (−0.80; −0.09) | −1.43 (−2.59; −0.27) I2 = 98% −0.47 (−1.18; 0.25) −2.76 (−6.31; 0.79) | −11.8(−23.57; 0.02) I2 = 99% −12.1(−35.87; 11.61) −11.5(−13.75; −9.21) | −0.92 (−2.33; 0.49) I2 = 97% 0.75 (0.27; 1.22) −2.41 (−5.36; 0.54) 0.25 (−0.08; 0.59) | −0.47 (−1.07; 0.12) I2 = 87% −0.11 (−0.42; 0.19) −0.71 (−1.88; 0.46) | −0.32 (−1.15; 0.51) I2 = NA −0.32 (−1.15; 0.51) | −1.21 (−1.69; −0.74) I2 = NA −1.21 (−1.69; −0.74) | −0.92 (−1.89; 0.04) I2 = 89% −1.83 (−2.43; −1.22) −0.47 (−1.13; 0.19) |
| KOOS function | Overall 1 month 3 months 6 months 12 months 24 months | 2.97 (1.93; 4.01) I2 = NA 2.97 (1.93; 4.01) | 0.52 (0.20; 0.85) I2 = 0% 0.41 (−0.05; 0.86) 0.64 (0.18; 1.10) | ||||||
| CRP | Overall 1 month 3 months 6 months 12 months 24 months | −1.32 (−3.23; 0.58) I2 = 93% −1.32 (−3.23; 0.58) | −1.36 (−1.80; −0.92) I2 = 38% −1.84 (−2.48; −1.20) −1.12 (−1.69; −0.54) −1.19 (−1.77; −0.61) | −0.19 (−0.60; 0.23) I2 = NA −0.19 (−0.60; 0.23) | −0.48 (−1.45; 0.48) I2 = NA −0.48 (−1.45; 0.48) | ||||
| ESR | Overall 1 month 3 months 6 months 12 months 24 months | −0.92 (−1.73; −0.10) I2 = 75% −0.92 (−1.73; −0.10) | −2.13 (−3.37; −0.89) I2 = 90% −2.63 (−3.37; −1.90) −0.98 (−1.55; −0.42) −2.84 (−3.60; −2.08) | −0.07 (−0.48; 0.35) I2 = NA −0.07 (−0.48; 0.35) | |||||
| SF12 | Overall 1 month 3 months 6 months 12 months 24 months | 0.54 (−0.25; 1.32) I2 = 91% 1.27 (0.91; 1.64) 0.17 (−0.14; 0.49) | 0.08 (−0.17; 0.33) I2 = NA 0.08 (−0.17; 0.33) | −0.01 (−0.39; 0.37) I2 = NA −0.01 (−0.39; 0.37) | |||||
| KOOS QoL | Overall 1 month 3 months 6 months 12 months 24 months | 0.61 (−0.11; 1.33) I2 = NA 0.61 (−0.11; 1.33) | 0.64 (0.26; 1.03) I2 = 26% 0.45 (−0.01; 0.91) 0.84 (0.37; 1.32) |


3.3.3. Ginger
3.3.4. Vitamin E and Multivitamin
3.3.5. Herbal Formulations
3.3.6. Omega-3
3.3.7. Other Nutritional Supplementations
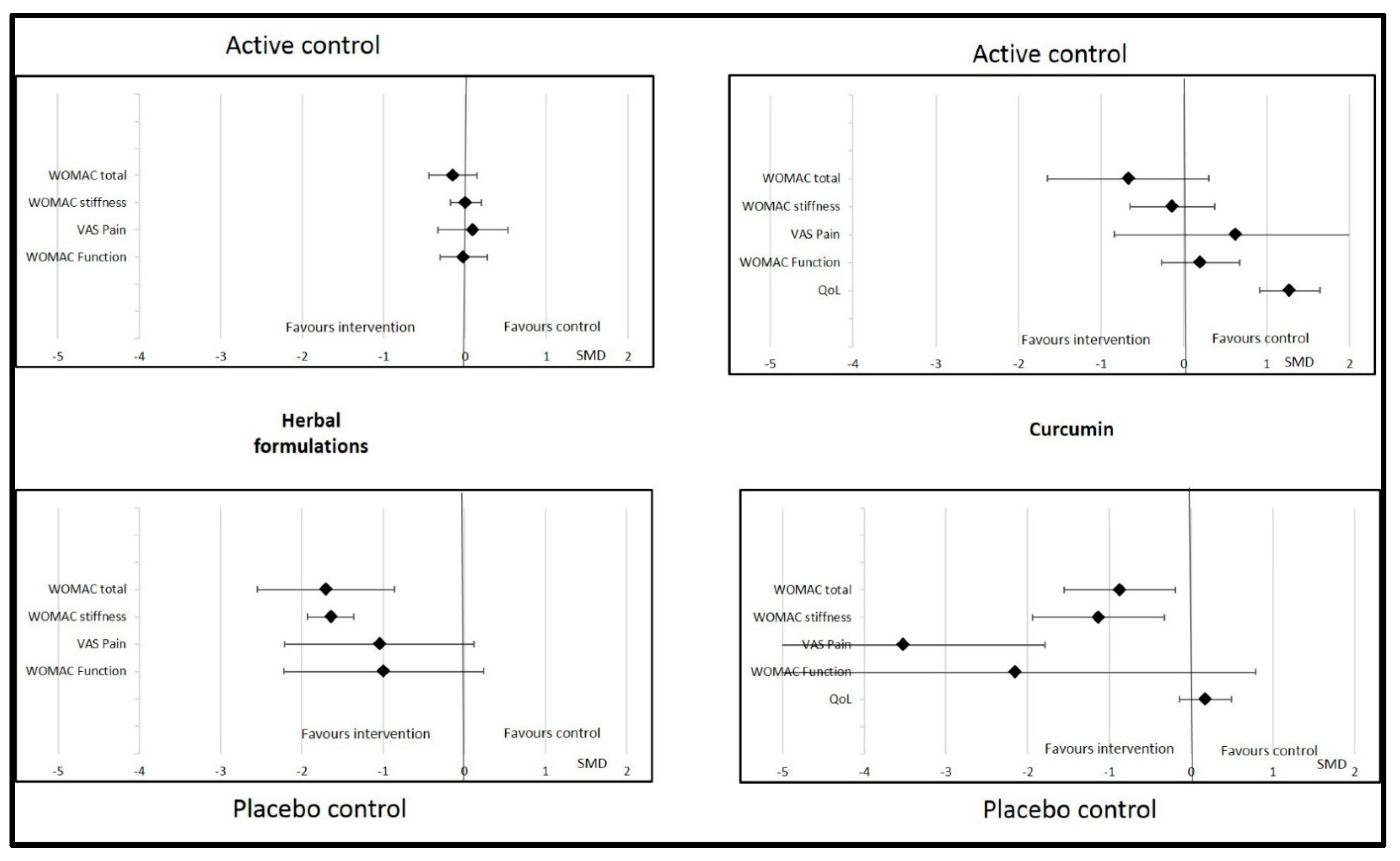
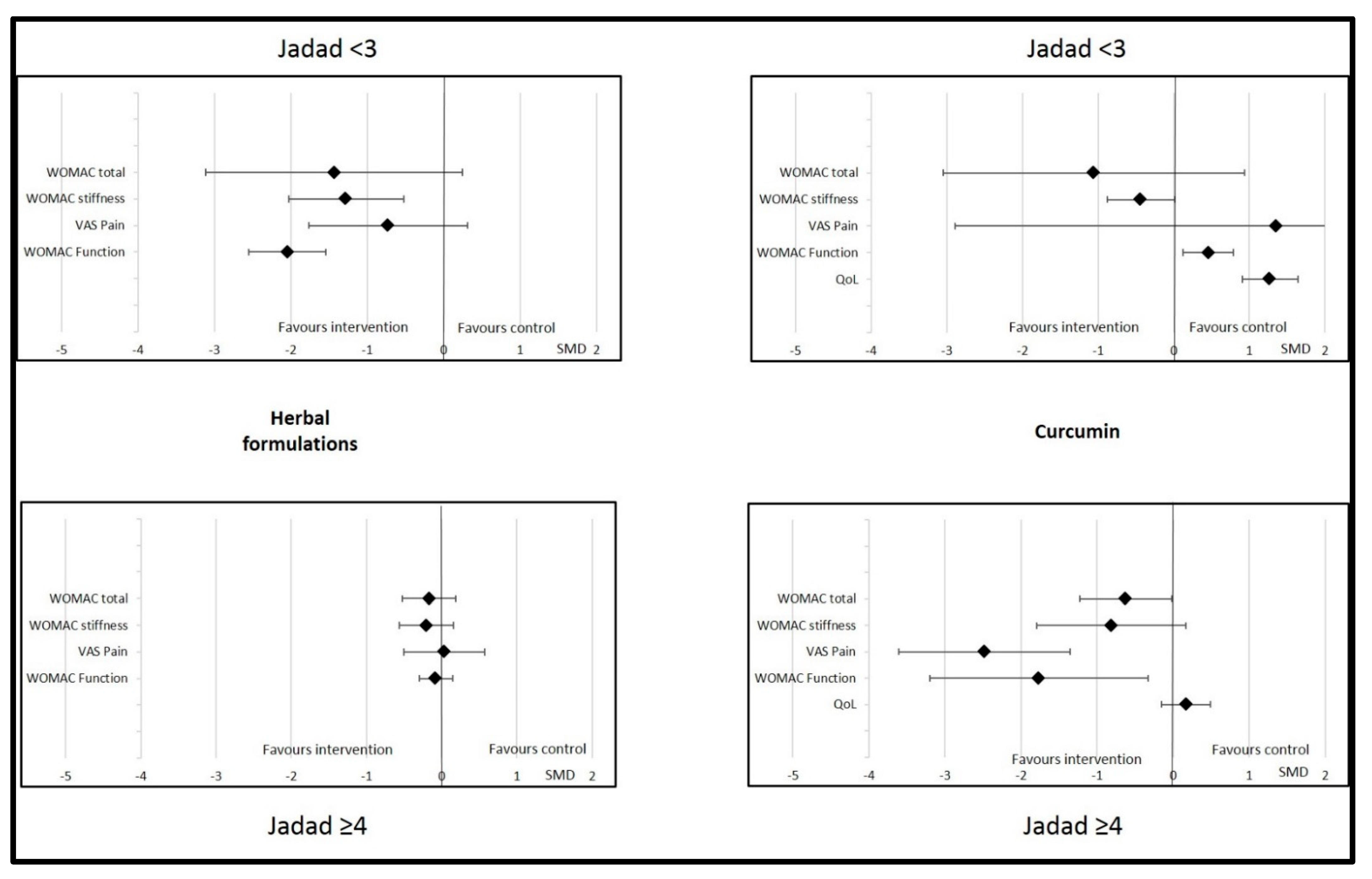
3.4. Effects of Nutritional Supplements Depending on Type of Controls and Jadad Score
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Binvignat, M.; Sokol, H.; Mariotti-Ferrandiz, E.; Berenbaum, F.; Sellam, J. Osteoarthritis and gut microbiome. Jt. Bone Spine 2021, 88, 105203. [Google Scholar] [CrossRef] [PubMed]
- Sellam, J.; Rat, A.-C.; Fellahi, S.; Bastard, J.-P.; Sime, W.N.; Ea, H.K.; Chevalier, X.; Richette, P.; Capeau, J.; Guillemin, F.; et al. Pain in women with knee and/or hip osteoarthritis is related to systemic inflammation and to adipose tissue dysfunction: Cross-sectional results of the KHOALA cohort. Semin Arthritis Rheum. Semin. Arthritis Rheum. 2020, 51, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Kloppenburg, M.; Berenbaum, F. Osteoarthritis year in review 2019: Epidemiology and therapy. Osteoarthr. Cartil. 2020, 28, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, S.; Wittoek, R.; Allado, E.; Cruzel, C.; Breuil, V.; Ziegler, L.E.; Louille, D.; Roux, C.; Kremer, J. Methotrexate in patients with hand erosive osteoarthritis refractory to usual treatments: A randomized, double-blind, placebo-controlled Trial. Arthritis Rheum. 2019, 71, 3149–3150. [Google Scholar] [CrossRef]
- Singh, A.; Kotlo, A.; Wang, Z.; Dissanayaka, T.; Das, S.; Antony, B. Efficacy and safety of hydroxychloroquine in osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Korean J. Intern. Med. 2022, 37, 210–221. [Google Scholar] [CrossRef]
- Aitken, D.; Laslett, L.L.; Pan, F.; Bellamy, N.; Bird, P.; Haugen, I.; Jones, G. A randomised double-blind place-bocontrolled crossover trial of adalimumab for erosive hand osteoarthritis: The humor trial. Osteoporos. Int. 2017, 28, S59. [Google Scholar] [CrossRef]
- Fuggle, N.R.; Cooper, C.; Oreffo, R.O.C.; Price, A.J.; Kaux, J.F.; Maheu, E.; Cutolo, M.; Honvo, G.; Conaghan, P.G.; Berenbaum, F.; et al. Alternative and complementary therapies in osteoarthritis and cartilage repair. Aging Clin. Exp. Res. 2020, 32, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Sellam, J.; Courties, A.; Eymard, F.; Ferrero, S.; Latourte, A.; Ornetti, P.; Bannwarth, B.; Baumann, L.; Berenbaum, F.; Chevalier, X.; et al. Recommendations of the French Society of Rheumatology on pharmacological treatment of knee osteoarthritis. Jt. Bone Spine 2020, 87, 548–555. [Google Scholar] [CrossRef]
- Daien, C.; Czernichow, S.; Letarouilly, J.-G.; Nguyen, Y.; Sanchez, P.; Sigaux, J.; Beauvais, C.; Desouches, S.; Le Puillandre, R.; Rigalleau, V.; et al. Dietary recommendations of the French Society for Rheumatology for patients with chronic inflammatory rheumatic diseases. Jt. Bone Spine 2021, 89, 105319. [Google Scholar] [CrossRef]
- Schönenberger, K.A.; Schüpfer, A.-C.; Gloy, V.L.; Hasler, P.; Stanga, Z.; Kaegi-Braun, N.; Reber, E. Effect of Anti-Inflammatory Diets on Pain in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4221. [Google Scholar] [CrossRef]
- Hahn, J.; Cook, N.R.; Alexander, E.K.; Friedman, S.; Walter, J.; Bubes, V.; Kotler, G.; Lee, I.-M.; Manson, J.E.; Costenbader, K.H. Vitamin D and marine omega 3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial. BMJ 2022, 376, e066452. [Google Scholar] [CrossRef] [PubMed]
- Raad, T.; Griffin, A.; George, E.S.; Larkin, L.; Fraser, A.; Kennedy, N.; Tierney, A.C. Dietary Interventions with or without Omega-3 Supplementation for the Management of Rheumatoid Arthritis: A Systematic Review. Nutrients 2021, 13, 3506. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-K.; Chen, P.-K.; Chen, C.-C.; Chang, S.-H.; Chen, C.-H.; Chen, D.-Y. Increased Levels of Omega-3 Fatty Acids and DHA Are Linked to Pain Reduction in Rheumatoid Arthritis Patients Treated with Janus Kinase Inhibitors. Nutrients 2021, 13, 3050. [Google Scholar] [CrossRef]
- Fatel, E.C.S.; Rosa, F.T.; Alfieri, D.F.; Flauzino, T.; Scavuzzi, B.M.; Lozovoy, M.A.B.; Iriyoda, T.M.V.; Simão, A.N.C.; Dichi, I. Beneficial effects of fish oil and cranberry juice on disease activity and inflammatory biomarkers in people with rheumatoid arthritis. Nutrition 2021, 86, 111183. [Google Scholar] [CrossRef]
- Ansari, M.Y.; Ahmad, N.; Haqqi, T.M. Oxidative stress and inflammation in osteoarthritis pathogenesis: Role of polyphenols. Biomed Pharm. 2020, 129, 110452. [Google Scholar] [CrossRef]
- Pincus, T.; Castrejon, I.; Yazici, Y.; Gibson, K.A.; Bergman, M.J.; Block, J.A. Osteoarthritis is as severe as rheumatoid arthritis: Evidence over 40 years according to the same measure in each disease. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S120), 7–17. [Google Scholar]
- Bannuru, R.R.; Osani, M.C.; Al-Eid, F.; Wang, C. Efficacy of curcumin and Boswellia for knee osteoarthritis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2018, 48, 416–429. [Google Scholar] [CrossRef]
- Zhao, Z.-X.; He, Y.; Peng, L.-H.; Luo, X.; Liu, M.; He, C.-S.; Chen, J. Does vitamin D improve symptomatic and structural outcomes in knee osteoarthritis? A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 2393–2403. [Google Scholar] [CrossRef]
- Yu, Y.; Liu, D.; Feng, D.; Zhao, J. Association between Vitamin D and Knee Osteoarthritis: A PRISMA-Compliant Meta-analysis. Z. Orthop. Unfall. 2021, 159, 281–287. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials. 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Atabaki, M.; Shariati-Sarabi, Z.; Tavakkol-Afshari, J.; Mohammadi, M. Significant immunomodulatory properties of curcumin in patients with osteoarthritis; a successful clinical trial in Iran. Int. Immunopharmacol. 2020, 85, 106607. [Google Scholar] [CrossRef]
- Haroyan, A.; Mukuchyan, V.; Mkrtchyan, N.; Minasyan, N.; Gasparyan, S.; Sargsyan, A.; Narimanyan, M.; Hovhannisyan, A. Efficacy and safety of curcumin and its combination with boswellic acid in osteoarthritis: A comparative, randomized, double-blind, placebo-controlled study. BMC Complement. Altern. Med. 2018, 18, 7. [Google Scholar] [CrossRef]
- Henrotin, Y.; Malaise, M.; Wittoek, R.; de Vlam, K.; Brasseur, J.; Luyten, F.; Jiangang, Q.; Van den Berghe, M.; Uhoda, R.; Bentin, J.; et al. Bio-optimized Curcuma longa extract is efficient on knee osteoarthritis pain: A double-blind multicenter randomized placebo controlled three-arm study. Arthritis Res. Ther. 2019, 21, 179. [Google Scholar] [CrossRef]
- Khanna, A.; Das, S.; Smina, T.; Thomas, J.; Kunnumakkara, A.; Maliakel, B.; Krishnakumar, I.; Mohanan, R. Curcumagalactomannoside/Glucosamine Combination Improved Joint Health Among Osteoarthritic Subjects as Compared to Chondroitin Sulfate/Glucosamine: Double-Blinded, Randomized Controlled Study. J. Altern. Complement. Med. 2020, 26, 945–955. [Google Scholar] [CrossRef]
- Kuptniratsaikul, V.; Dajpratham, P.; Taechaarpornkul, W.; Buntragulpoontawee, M.; Lukkanapichonchut, P.; Chootip, C.; Saengsuwan, J.; Tantayakom, K.; Laongpech, S. Efficacy and safety of Curcuma domestica extracts compared with ibuprofen in patients with knee osteoarthritis: A multicenter study. Clin. Interv. Aging 2014, 9, 451–458. [Google Scholar] [CrossRef]
- Kuptniratsaikul, V.; Thanakhumtorn, S.; Chinswangwatanakul, P.; Wattanamongkonsil, L.; Thamlikitkul, V. Efficacy and safety of Curcuma domestica extracts in patients with knee osteoarthritis. J. Altern. Complement. Med. 2009, 15, 891–897. [Google Scholar] [CrossRef]
- Madhu, K.; Chanda, K.; Saji, M. Safety and efficacy of Curcuma longa extract in the treatment of painful knee osteoarthritis: A randomized placebo-controlled trial. Inflammopharmacology 2013, 21, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.K.; Nirvanashetty, S.; Parachur, V.A.; Mohanty, N.; Swain, T. A Randomized, Double Blind, Placebo Controlled, Parallel-Group Study to Evaluate the Safety and Efficacy of Curene® versus Placebo in Reducing Symptoms of Knee OA. BioMed Res. Int. 2018, 2018, 5291945. [Google Scholar] [CrossRef] [PubMed]
- Shep, D.; Khanwelkar, C.; Gade, P.; Karad, S. Efficacy and safety of combination of curcuminoid complex and diclofenac versus diclofenac in knee osteoarthritis: A randomized trial. Medicine 2020, 99, e19723. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Hasan, N.; Nirmal, K.; Chawla, R.; Chawla, S.; Kalra, B.; Dhal, A. Bioavailable turmeric extract for knee osteoarthritis: A randomized, non-inferiority trial versus paracetamol. Trials 2021, 22, 105. [Google Scholar] [CrossRef]
- Srivastava, S.; Saksena, A.; Khattri, S.; Kumar, S.; Dagur, R. Curcuma longa extract reduces inflammatory and oxidative stress biomarkers in osteoarthritis of knee: A four-month, double-blind, randomized, placebo-controlled trial. Inflammopharmacology 2016, 24, 377–388. [Google Scholar] [CrossRef]
- Wang, Z.; Jones, G.; Winzenberg, T.; Cai, G.; Laslett, L.L.; Aitken, D.; Hopper, I.; Singh, A.; Jones, R.; Fripp, J.; et al. Effectiveness of Curcuma longa Extract for the Treatment of Symptoms and Effusion-Synovitis of Knee Osteoarthritis: A Randomized Trial. Ann. Intern. Med. 2020, 173, 861–869. [Google Scholar] [CrossRef]
- Panahi, Y.; Rahimnia, A.-R.; Sharafi, M.; Alishiri, G.; Saburi, A.; Sahebkar, A. Curcuminoid treatment for knee osteoarthritis: A randomized double-blind placebo-controlled trial. Phytother. Res. 2014, 28, 1625–1631. [Google Scholar] [CrossRef]
- Altman, R.D.; Marcussen, K.C. Effects of a ginger extract on knee pain in patients with osteoarthritis. Arthritis Rheum. 2001, 44, 2531–2538. [Google Scholar] [CrossRef]
- Wigler, I.; Grotto, I.; Caspi, D.; Yaron, M. The effects of Zintona EC (a ginger extract) on symptomatic gonarthritis. Osteoarthr. Cartil. 2003, 11, 783–789. [Google Scholar] [CrossRef]
- Bolognesi, G.; Belcaro, G.; Feragalli, B.; Cornelli, U.; Cotellese, R.; Hu, S.; Dugall, M. Movardol® (N-acetylglucosamine, Boswellia serrata, ginger) supplementation in the management of knee osteoarthritis: Preliminary results from a 6-month registry study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 5198–5204. [Google Scholar]
- Jin, X.; Cicuttini, F.; Wluka, A.; Zhu, Z.; Han, W.; Antony, B.; Wang, X.; Winzenberg, T.; Blizzard, L.; Jones, G.; et al. Vitamin d supplementation for the management of knee osteoarthritis: A two year double blind randomized controlled trial. Ann. Rheum. Dis. 2015, 74, 185. [Google Scholar] [CrossRef]
- McAlindon, T.; LaValley, M.; Schneider, E.; Nuite, M.; Lee, J.Y.; Price, L.L.; Lo, G.; Dawson-Hughes, B. Effect of vitamin D supplementation on progression of knee pain and cartilage volume loss in patients with symptomatic osteoarthritis: A randomized controlled trial. JAMA 2013, 309, 155–162. [Google Scholar] [CrossRef]
- Sanghi, D.; Srivastava, R.; Mishra, A.; Natu, S.; Mishra, R.; Agarwal, S. Role of vitamin d in osteoarthritis knee: A six month double blind, randomized, placebo control trial. Osteoarthr. Cartil. 2013, 21, S28–S29. [Google Scholar] [CrossRef][Green Version]
- Medhi, B.; Manpreet, S.; Deonis, X.; Aggarwal, S.; Pandhi, P.; Nagi, O. Comparative clinical trial of paracetamol alone and vitamin C and E as an add on therapy in patients suffering from primary knee osteoarthritis. JK Sci. 2011, 14, 38–42. [Google Scholar]
- Dehghan, M. Comparative effectiveness of B and e vitamins with diclofenac in reducing pain due to osteoarthritis of the knee. Med. Arch. 2015, 69, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Tantavisut, S.; Tanavalee, A.; Honsawek, S.; Suantawee, T.; Ngarmukos, S.; Adisakwatana, S.; Callaghan, J. Effect of vitamin E on oxidative stress level in blood, synovial fluid, and synovial tissue in severe knee osteoarthritis: A randomized controlled study. BMC Musculoskelet. Disord. 2017, 18, 281. [Google Scholar] [CrossRef] [PubMed]
- Wluka, A.; Stuckey, S.; Brand, C.; Cicuttini, F. Supplementary vitamin E does not affect the loss of cartilage volume in knee osteoarthritis: A 2 year double blind randomized placebo controlled study. J. Rheumatol. 2002, 29, 2585–2591. [Google Scholar]
- Essouiri, J.; Harzy, T.; Benaicha, N.; Errasfa, M.; Abourazzak, F.E. Effectiveness of Argan Oil Consumption on Knee Osteoarthritis Symptoms: A Randomized Controlled Clinical Trial. Curr. Rheumatol. Rev. 2017, 13, 231–235. [Google Scholar] [CrossRef][Green Version]
- Colker, C.; Swain, M.; Lynch, L.; Gingerich, D. Effects of a milk-based bioactive micronutrient beverage on pain symptoms and activity of adults with osteoarthritis: A double-blind, placebo-controlled clinical evaluation. Nutrition 2002, 18, 388–392. [Google Scholar] [CrossRef]
- Frestedt, J.; Walsh, M.; Kuskowski, M.; Zenk, J. A natural mineral supplement provides relief from knee osteoarthritis symptoms: A randomized controlled pilot trial. Nutr. J. 2008, 7, 9. [Google Scholar] [CrossRef]
- Jacquet, A.; Girodet, P.; Pariente, A.; Forest, K.; Mallet, L.; Moore, N. Phytalgic, a food supplement, vs placebo in patients with osteoarthritis of the knee or hip: A randomised double-blind placebo-controlled clinical trial. Arthritis Res. Ther. 2009, 11, R192. [Google Scholar] [CrossRef]
- Stammers, T.; Sibbald, B.; Freeling, P. Efficacy of cod liver oil as an adjunct to non-steroidal anti-inflammatory drug treatment in the management of osteoarthritis in general practice. Ann. Rheum. Dis. 1992, 51, 128–129. [Google Scholar] [CrossRef]
- Chopra, A.; Lavin, P.; Patwardhan, B.; Chitre, D. A 32-week randomized, placebo-controlled clinical evaluation of RA-11, an Ayurvedic drug, on osteoarthritis of the knees. J. Clin. Rheumatol. 2004, 10, 236–245. [Google Scholar] [CrossRef]
- Guo, Y.; Yao, J.; Liu, F.; Dong, B.; Wang, Z. Effect of Fuyuan Huoxue decoction on knee osteoarthritis. Osteoarthr. Cartil. 2021, 29, S416–S417. [Google Scholar] [CrossRef]
- Tao, Q.; Xu, Y.; Jin, D.; Yan, X. Clinical efficacy and safety of Gubitong Recipe (骨痹通方) in treating osteoarthritis of knee joint. Chin. J. Integr. Med. 2009, 15, 458–461. [Google Scholar] [CrossRef]
- Wu, X.; Zhou, Y. Observation on the therapeutic effect of Shu Feng Huo Luo Pian for treatment of osseous arthritis. J. Tradit. Chin. Med. 2002, 22, 12–14. [Google Scholar]
- Farpour, H.; Ashraf, A.; Hosseini, S. The Efficacy of Ozone Prolotherapy Compared to Intra-Articular Hypertonic Saline Injection in Reducing Pain and Improving the Function of Patients with Knee Osteoarthritis: A Randomized Clinical Trial. Evid.-Based Complement. Altern. Med. 2021, 2021, 5579944. [Google Scholar] [CrossRef]
- Gupta, A.K.; Acharya, K.; Sancheti, P.S.; Joshi, R.S. A double-blind, randomized, multicentric, placebo-controlled clinical trial of antarth, a phytomedicine, in the treatment of osteoarthritis. Indian J. Pharm. 2011, 43, 69–72. [Google Scholar] [CrossRef]
- Hamblin, L.; Laird, A.; Parkes, E.; Walker, A.F. Improved arthritic knee health in a pilot RCT of phytotherapy. J. R. Soc. Promot. Health 2008, 128, 255–262. [Google Scholar] [CrossRef]
- Karimifar, M.; Soltani, R.; Hajhashemi, V.; Sarrafchi, S. Evaluation of the effect of Elaeagnus angustifolia alone and combined with Boswellia thurifera compared with ibuprofen in patients with knee osteoarthritis: A randomized double-blind controlled clinical trial. Clin. Rheumatol. 2017, 36, 1849–1853. [Google Scholar] [CrossRef]
- Karlapudi, V.; Prasad Mungara, A.; Sengupta, K.; Davis, B.; Raychaudhuri, S. A Placebo-Controlled Double-Blind Study Demonstrates the Clinical Efficacy of a Novel Herbal Formulation for Relieving Joint Discomfort in Human Subjects with Osteoarthritis of Knee. J. Med. Food 2018, 21, 511–520. [Google Scholar] [CrossRef]
- Koonrungsesomboon, N.; Nopnithipat, S.; Teekachunhatean, S.; Chiranthanut, N.; Sangdee, C.; Chansakaow, S.; Tipduangta, P.; Hanprasertpong, N. Clinical Efficacy and Safety of Thai Herbal Formulation-6 in the Treatment of Symptomatic Osteoarthritis of the Knee: A Randomized-Controlled Trial. Evid.-Based Complement. Altern. Med. 2020, 2020, 8817374. [Google Scholar] [CrossRef]
- Moré, M.; Gruenwald, J.; Pohl, U.; Uebelhack, R. A Rosa canina-Urtica dioica-Harpagophytum procumbens/zeyheri Combination Significantly Reduces Gonarthritis Symptoms in a Randomized, Placebo-Controlled Double-Blind Study. Planta Med. 2017, 83, 1384–1391. [Google Scholar] [CrossRef]
- Thomford, K.P.; Yorke, J.; Thomford, A.K.; Amponsah, I.K. A formulation of Clausena anisata (Willd.) Hook. f. Ex Benth and Cassia sieberiana DC. alleviates the symptoms associated with osteoarthritis: A single-blind, randomised controlled trial of a traditional Ghanaian remedy. Clin. Phytoscience 2021, 7, 76. [Google Scholar] [CrossRef]
- Kakatum, N.; Pinsornsak, P.; Kanokkangsadal, P.; Ooraikul, B.; Itharat, A. Efficacy and Safety of Sahastara Remedy Extract Capsule in Primary Knee Osteoarthritis: A Randomized Double-Blinded Active-Controlled Trial. Evid.-Based Complement. Alternat. Med. 2021, 2021, 6635148. [Google Scholar] [CrossRef]
- Pinsornsak, P.; Kanokkangsadal, P.; Itharat, A. The clinical efficacy and safety of the sahastara remedy versus diclofenac in the treatment of osteoarthritis of the knee: A double-blind, randomized, and controlled trial. Evid.-Based Complement. Altern. Med. 2015, 2015, 103046. [Google Scholar] [CrossRef][Green Version]
- Liu, X.; Robbins, S.; Eyles, J.; Fedorova, T.; Virk, S.; Deveza, L.A.; McLachlan, A.J.; Hunter, D.J. Efficacy and safety of a supplement combination on hand pain among people with symptomatic hand osteoarthritis an internet-based, randomised clinical trial the RADIANT study. Osteoarthr. Cartil. 2021, 29, 667–677. [Google Scholar] [CrossRef]
- Schumacher, H.; Pullman-Mooar, S.; Gupta, S.; Dinnella, J.; Kim, R.; McHugh, M. Randomized double-blind crossover study of the efficacy of a tart cherry juice blend in treatment of osteoarthritis (OA) of the knee. Osteoarthr. Cartil. 2013, 21, 1035–1041. [Google Scholar] [CrossRef]
- Puente, R.; Illnait, J.; Mas, R.; Carbajal, D.; Mendoza, S.; Fernández, J.C.; Mesa, M.; Gámez, R.; Reyes, P. Evaluation of the effect of D-002, a mixture of beeswax alcohols, on osteoarthritis symptoms. Korean J. Intern. Med. 2014, 29, 191–202. [Google Scholar] [CrossRef]
- Shin, D.; Kim, E.; Kim, Y.; Kim, M.; Kim, J.; Ahn, C.; Park, S.; Lee, K.; Kim, J.; Kim, J. Deer Bone Extract Supplementation for Mild-to-Moderate Knee Osteoarthritis Symptoms: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Med. Food 2018, 21, 159–166. [Google Scholar] [CrossRef]
- Salimzadeh, A.; Alipoor, E.; Dehghani, S.; Yaseri, M.; Hosseini, M.; Feinle-Bisset, C.; Hosseinzadeh-Attar, M.J. The effect of 12-week garlic supplementation on symptom relief in overweight or obese women with knee osteoarthritis. Int. J. Clin. Pract. 2018, 72, e13208. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.; Chiu, P.; Chu, E.; Cheng, I.; Tang, W.; Man, R.; Halpern, G. Treatment of knee osteoarthritis with Lyprinol®, lipid extract of the green-lipped mussel-A double-blind placebo-controlled study. Prog. Nutr. 2004, 6, 17–31. [Google Scholar]
- Zawadzki, M.; Janosch, C.; Szechinski, J. Perna canaliculus lipid complex PCSO-524TM demonstrated pain relief for osteoarthritis patients benchmarked against fish oil, a randomized trial, without placebo control. Mar. Drugs 2013, 11, 1920–1935. [Google Scholar] [CrossRef]
- May, L.S.; Sanip, Z.; Shokri, A.A.; Kadir, A.A.; Lazin, M.M. The effects of Momordica charantia (bitter melon) supplementation in patients with primary knee osteoarthritis: A single-blinded, randomized controlled trial. Complement. Ther. Clin. Pract. 2018, 32, 181–186. [Google Scholar] [CrossRef]
- Sadat, B.E.; Haghighian, M.K.; Alipoor, B.; Mahdavi, A.M.; Jafarabadi, M.A.; Moghaddam, A. Effects of sesame seed supplementation on clinical signs and symptoms in patients with knee osteoarthritis. Int. J. Rheum. Dis. 2013, 16, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Schell, J.; Hal Scofield, R.; Barrett, J.; Kurien, B.; Betts, N.; Lyons, T.; Zhao, Y.; Basu, A. Strawberries improve pain and inflammation in obese adults with radiographic evidence of knee osteoarthritis. Nutrients 2017, 9, 949. [Google Scholar] [CrossRef]
- Gupta, S.C.; Sung, B.; Kim, J.H.; Prasad, S.; Li, S.; Aggarwal, B.B. Multitargeting by turmeric, the golden spice: From kitchen to clinic. Mol. Nutr. Food Res. 2012, 57, 1510–1528. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Hosseini, M.; Khalili, N.; Naimi, E.; Majeed, M.; Sahebkar, A. Antioxydant and anti-inflammatory effects of curcuminoid-piperine combination in subjects with metabolic syndrome: A randomized controlled trial and an updated meta-analysis. Clin. Nutr. 2015, 34, 1101–1108. [Google Scholar] [CrossRef]
- Hsiao, A.-F.; Lien, Y.-C.; Tzeng, I.-S.; Liu, C.-T.; Chou, S.-H.; Horng, Y.-S. The efficacy of high- and low-dose curcumin in knee osteoarthritis: A systematic review and meta-analysis. Complement. Ther. Med. 2021, 63, 102775. [Google Scholar] [CrossRef]
- Zeng, L.; Yu, G.; Hao, W.; Yang, K.; Chen, H. The efficacy and safety of Curcuma longa extract and curcumin supplements on osteoarthritis: A systematic review and meta-analysis. Biosci. Rep. 2021, 41, BSR20210817. [Google Scholar] [CrossRef]
- Kocaadam, B.; Şanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, V.; Sahebkar, A.; Hosseinzadeh, H. Turmeric (Curcuma longa) and its major constituent (curcumin) as nontoxic and safe substances: Review. Phyther. Res. 2018, 32, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.-Y. The spice for joint inflammation: Anti-inflammatory role of curcumin in treating osteoarthritis. Drug Des. Dev. Ther. 2016, 10, 3029–3042. [Google Scholar] [CrossRef]
- Mun, S.H.; Kim, H.S.; Kim, J.W.; Ko, N.Y.; Kim, D.K.; Lee, B.Y.; Kim, B.; Won, H.S.; Shin, H.-S.; Han, J.-W.; et al. Oral administration of curcumin suppresses production of matrix metalloproteinase (MMP)-1 and MMP-3 to ameliorate collagen-induced arthritis: Inhibition of the PKCdelta/JNK/c-Jun pathway. J. Pharmacol. Sci. 2009, 111, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Naderi, Z.; Mozaffari-Khosravi, H.; Dehghan, A.; Nadjarzadeh, A.; Huseini, H.F. Effect of ginger powder supplementation on nitric oxide and C-reactive protein in elderly knee osteoarthritis patients: A 12-week double-blind randomized placebo-controlled clinical trial. J. Tradit. Complement. Med. 2016, 6, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari-Khosravi, H.; Naderi, Z.; Dehghan, A.; Nadjarzadeh, A.; Huseini, H.F. Effect of ginger supplementation on proinflammatory cytokines in older patients with osteoarthritis: Outcomes of a randomized controlled clinical trial. J. Nutr. Gerontol. Geriatr. 2016, 35, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Babaahmadi-Rezaei, H.; Kheirollah, A.; Hesam, S.; Ayashi, S.; Aberumand, M.; Adel, M.H.; Zamanpour, M.; Alasvand, M.; Amozgari, Z.; Noor-Behbahani, M.; et al. Decreased lipoprotein (a) and serum high-sensitivity C-reactive protein levels in male patients with atherosclerosis after supplementation with ginger: A randomized controlled trial. ARYA Atheroscler. J. 2020, 16, 153–160. [Google Scholar] [CrossRef]
- Semwal, R.B.; Semwal, D.; Combrinck, S.; Viljoen, A.M. Gingerols and shogaols: Important nutraceutical principles from ginger. Phytochemistry 2015, 117, 554–568. [Google Scholar] [CrossRef]
- Rondanelli, M.; Fossari, F.; Vecchio, V.; Gasparri, C.; Peroni, G.; Spadaccini, D.; Riva, A.; Petrangolini, G.; Iannello, G.; Nichetti, M.; et al. Clinical trials on pain lowering effect of ginger: A narrative review. Phytother. Res. 2020, 34, 2843–2856. [Google Scholar] [CrossRef]
- Araya-Quintanilla, F.; Gutierrez-Espinoza, H.; Munoz-Yanez, M.J.; Sanchez-Montoya, U.; Lopez-Jeldes, J. Effectiveness of Ginger on Pain and Function in Knee Osteoarthritis: A PRISMA Systematic Review and Meta-Analysis. Pain Physician 2020, 23, E151–E161. [Google Scholar] [CrossRef]
- Boonstra, A.; Barrat, F.J.; Crain, C.; Heath, V.L.; Savelkoul, H.F.; O’Garra, A. 1alpha,25-Dihydroxyvitamin d3 has a direct effect on naive CD4(+) T cells to enhance the development of Th2 cells. J. Immunol. 2001, 167, 4974–4980. [Google Scholar] [CrossRef] [PubMed]
- Guillot, X.; Semerano, L.; Decker, P.; Falgarone, G.; Boissier, M.-C. Pain and immunity. Jt. Bone Spine 2012, 79, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Adorini, L.; Penna, G. Control of autoimmune diseases by the vitamin D endocrine system. Nat. Clin. Pract. Rheumatol. 2008, 4, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Soubrier, M.; Lambert, C.; Combe, B.; Gaudin, P.; Thomas, T.; Sibilia, J.; Dougados, M.; Dubost, J.-J. A randomised, double-blind, placebo-controlled study assessing the efficacy of high doses of vitamin D on functional disability in patients with rheumatoid arthritis. Clin. Exp. Rheumatol. 2018, 36, 1056–1060. [Google Scholar] [PubMed]
- Nguyen, Y.; Sigaux, J.; Letarouilly, J.-G.; Sanchez, P.; Czernichow, S.; Flipo, R.-M.; Soubrier, M.; Semerano, L.; Seror, R.; Sellam, J.; et al. Efficacy of Oral Vitamin Supplementation in Inflammatory Rheumatic Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Singh, A.; Akhtar, M.; Najmi, A.K. Vitamin D supplementation for the management of knee osteoarthritis: A systematic review of randomized controlled trials. Rheumatol. Int. 2017, 37, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Eftekharsadat, B.; Aghamohammadi, D.; Dolatkhah, N.; Hashemian, M.; Salami, H. Lower serum levels of alpha tocopherol and lycopene are associated with higher pain and physical disability in subjects with primary knee osteoarthritis: A case-control study. Int. J. Vitam. Nutr. Res. 2021, 91, 304–314. [Google Scholar] [CrossRef]
- Ryan, M.J.; Dudash, H.J.; Docherty, M.; Geronilla, K.B.; Baker, B.A.; Haff, G.G.; Cutlip, R.G.; Alway, S.E. Vitamin E and C supplementation reduces oxidative stress, improves antioxidant enzymes and positive muscle work in chronically loaded muscles of aged rats. Exp. Gerontol. 2010, 45, 882–895. [Google Scholar] [CrossRef]
- Alpsoy, L.; Yildirim, A.; Agar, G. The antioxidant effects of vitamin A, C, and E on aflatoxin B1-induced oxidative stress in human lymphocytes. Toxicol. Ind. Health 2009, 25, 121–127. [Google Scholar] [CrossRef]
- Gudivada, K.K.; Kumar, A.; Sriram, K.; Baby, J.; Shariff, M.; Sampath, S.; Sivakoti, S.; Krishna, B. Antioxidant micronutrient supplements for adult critically ill patients: A bayesian multiple treatment comparisons meta-analysis. Clin. Nutr. ESPEN 2022, 47, 78–88. [Google Scholar] [CrossRef]
- Hamedi-Kalajahi, F.; Zarezadeh, M.; Dehghani, A.; Musazadeh, V.; Kolahi, A.; Shabbidar, S.; Djafarian, K. A systematic review and meta-analysis on the impact of oral vitamin E supplementation on apolipoproteins A1 and B100. Clin. Nutr. ESPEN 2021, 46, 106–114. [Google Scholar] [CrossRef]
- Power, R.; Nolan, J.M.; Prado-Cabrero, A.; Roche, W.; Coen, R.; Power, T.; Mulcahy, R. Omega-3 fatty acid, carotenoid and vitamin E supplementation improves working memory in older adults: A randomised clinical trial. Clin. Nutr. 2021, 41, 405–414. [Google Scholar] [CrossRef]
- Jahromi, B.; Pirvulescu, I.; Candido, K.D.; Knezevic, N.N. Herbal Medicine for Pain Management: Efficacy and Drug Interactions. Pharmaceutics 2021, 13, 251. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathieu, S.; Soubrier, M.; Peirs, C.; Monfoulet, L.-E.; Boirie, Y.; Tournadre, A. A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms. Nutrients 2022, 14, 1607. https://doi.org/10.3390/nu14081607
Mathieu S, Soubrier M, Peirs C, Monfoulet L-E, Boirie Y, Tournadre A. A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms. Nutrients. 2022; 14(8):1607. https://doi.org/10.3390/nu14081607
Chicago/Turabian StyleMathieu, Sylvain, Martin Soubrier, Cedric Peirs, Laurent-Emmanuel Monfoulet, Yves Boirie, and Anne Tournadre. 2022. "A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms" Nutrients 14, no. 8: 1607. https://doi.org/10.3390/nu14081607
APA StyleMathieu, S., Soubrier, M., Peirs, C., Monfoulet, L.-E., Boirie, Y., & Tournadre, A. (2022). A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms. Nutrients, 14(8), 1607. https://doi.org/10.3390/nu14081607